
Availability of Physical Activity Tracking Data from Wearable Devices for Glaucoma Patients

 , and
, and 
Abstract
:1. Introduction
2. Methods
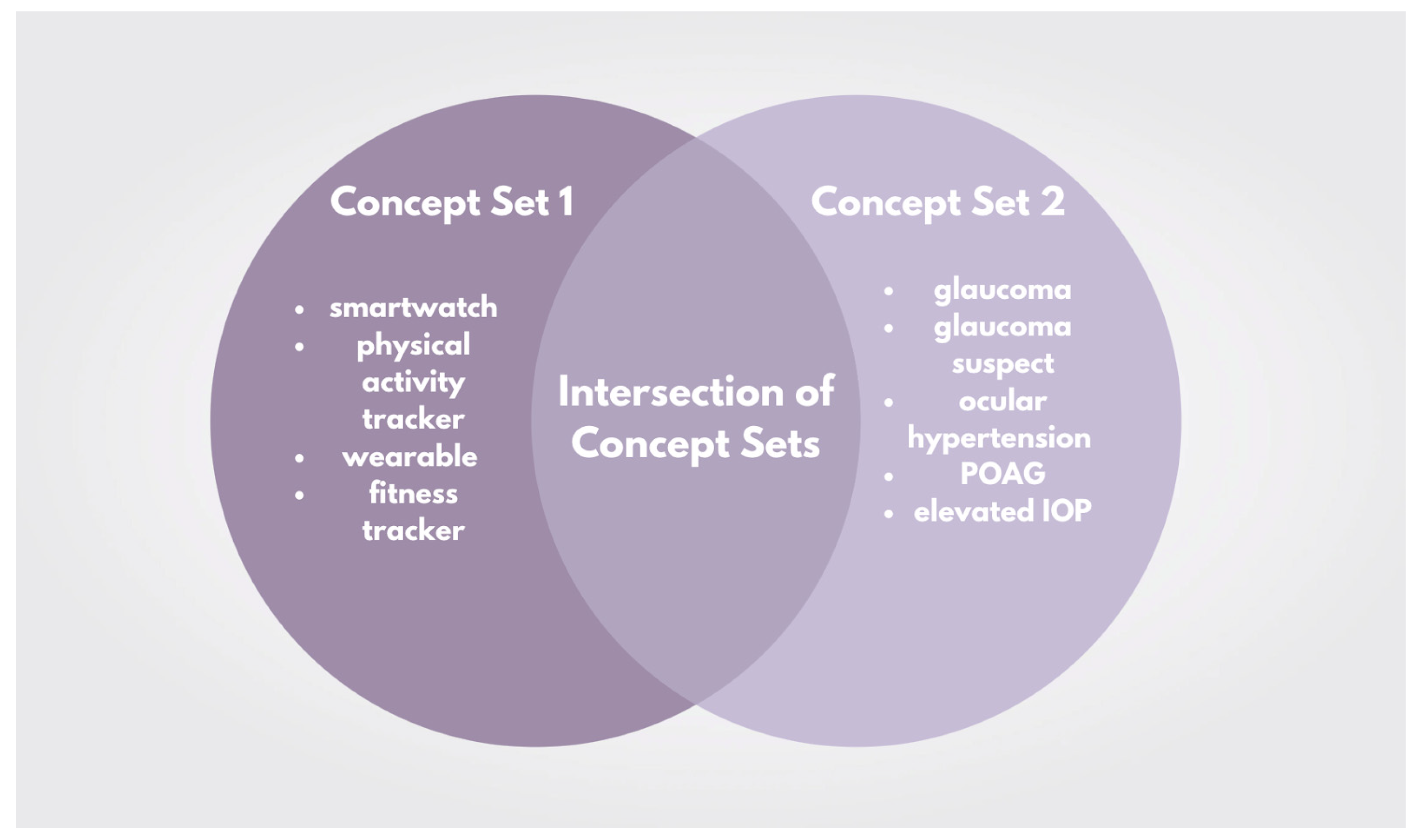
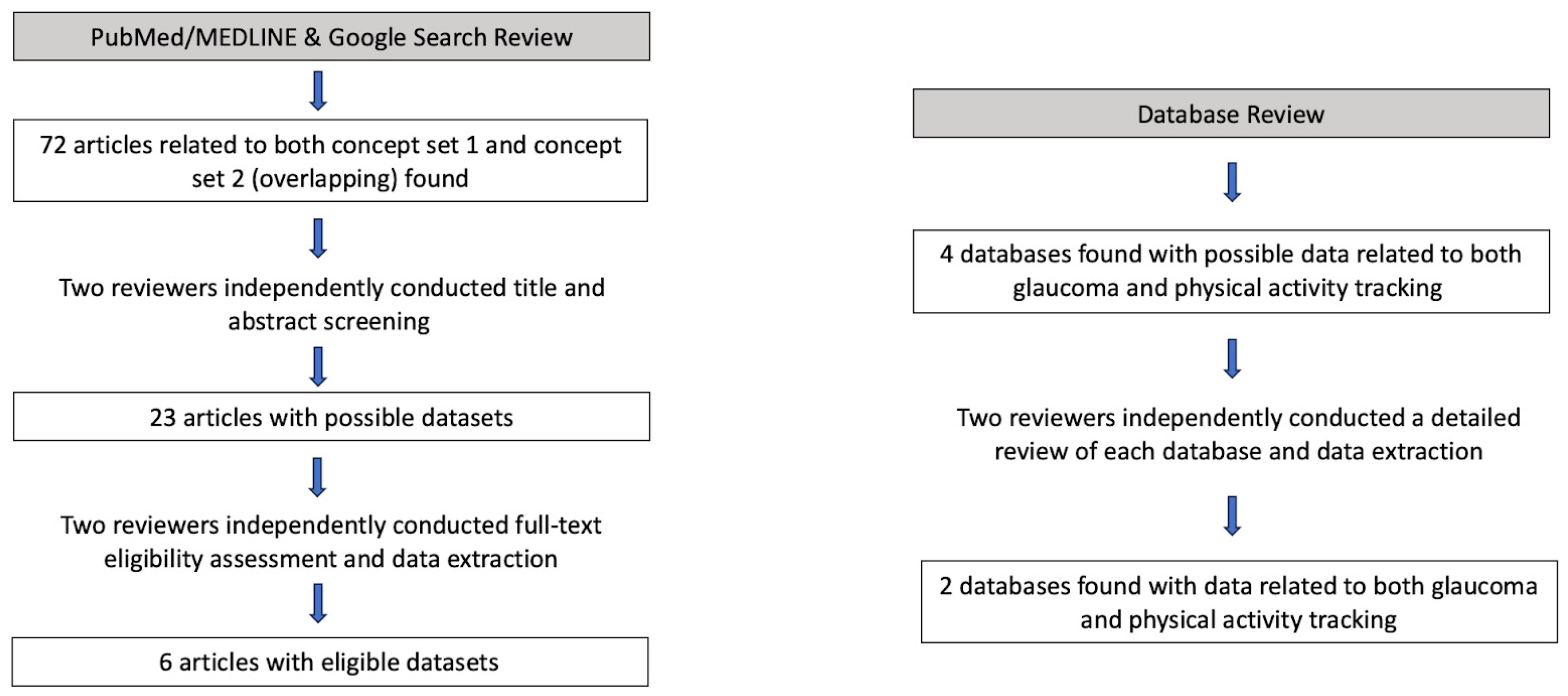
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Query and Extraction
3. Results
3.1. Overview of Available Datasets
3.2. Cohort Sizes
3.3. Main Findings from Journal Articles
3.4. Ophthalmological Data Available among Datasets with Physical Activity Tracking
3.5. Features of Physical Activity Tracking Data
3.6. Diversity of Data

{kind=link}
{kind=link}
| Dataset | Number of Glaucoma Patients | Number of Patients (Any Diagnosis) with Physical Activity Tracking Data Available | Number of Glaucoma Patients with Physical Activity Tracking Data Available | Access Details | Glaucoma-Related Data Available in Dataset | Fitness Device Used | Overall Race/Ethnicity Composition of Dataset |
|---|---|---|---|---|---|---|---|
| National Institutes of Health All of Us Research Program [22] | 15,578 | 12,844 | 437 | Restricted access by registration and approval, must be a U.S. resident, training required, requires institutional data use agreement | Epidemiological analysis including glaucoma status, family history, and genetics. Diagnosis codes and procedure codes are also available | FitBit | 244,540 (52.0%) White, 82,020 (17.4%) Black/African American/African, 75,420 (16%) Hispanic/Latino, 14,800 (3.1%) Asian, and Other (11.5%) |
| United Kingdom BioBank (UKBB a) [23] | 7550 * | 37,641 | 429 | Restricted by registration and requires payment, requires affiliation with research/university, must have an established research profile | Visual acuity, autorefraction and keratometry, IOP b, corneal hysteresis, corneal resistance factor, retinal photography, spectral domain optical coherence tomography | Accelerometer data (various devices possible) | 511,441 (94.4%) White, 10,253 (1.89%) Asian/British Asian, 8290 (1.53%) Black/British Black, Other (2.13%) |
| Ma QY et al. (2022) [16] | 123 | 61 | 61 | Journal article, data available upon request to the authors | IOP b, ocular perfusion pressure | Unspecified sports watch | 123 (100%) Asian (Chinese) |
| E et al. (2021) [17] | 229 | 229 | 229 | Journal article, data available upon request to the authors | Visual acuity, visual field damage, integrated visual field sensitivity | Waist-bound physical tracking device with GPS tracking | 63 (27.5%) African American |
| Ramulu et al. (2012) [18] | 83 | 141 | 83 | Journal article, data available upon request to the authors | Better-eye visual field mean deviation | Omnidirectional accelerometer | 40 (28.4%) African American |
| Lee et al. (2019) [19] | 83 | 141 | 83 | Journal article, data available upon request to the authors | Eye Mean deviation, visual field loss | Omnidirectional accelerometer | 46 (32%) Non-Caucasian |
| Berry et al. (2023) [20] | 512 (PROGRESSA c) N/A (UK BB) | 465 (PROGRESSA) 96,679 (UK BB) | 465 (PROGRESSA) N/A (UK BB) | Journal article, data accessible via UKBB a and available upon request to the PROGRESSA study group | Visual acuity, IOP, ultrasound central corneal pachymetry, vertical cup to disc ratio (PROGRESSA) Described above (UKBB) | FitBit (PROGRESSA) Triaxial accelerometer (UKBB) | Not reported by authors, available upon request to the PROGRESSA study group and under UKBB. |
| Madjedi et al. (2023) [21] | Refer to UKBB a data above | Refer to UKBB a data above | Refer to UKBB a data above | Journal article, data accessible via UKBB a | Refer to UKBB a data above | Refer to UKBB a data above | Refer to UKBB a data above |
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA J. Am. Med. Assoc. 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Zhang, N.; Wang, J.; Li, Y.; Jiang, B. Prevalence of primary open angle glaucoma in the last 20 years: A meta-analysis and systematic review. Sci. Rep. 2021, 11, 13762. [Google Scholar] [CrossRef]
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Coleman, A.L.; Miglior, S. Risk factors for glaucoma onset and progression. Surv. Ophthalmol. 2008, 53 (Suppl. 1), S3–S10. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, H. Intraocular pressure reduction in glaucoma: Does every mmHg count? Taiwan J. Ophthalmol. 2020, 10, 255–258. [Google Scholar] [CrossRef]
- Coleman, A.L.; Kodjebacheva, G. Risk factors for glaucoma needing more attention. Open Ophthalmol. J. 2009, 3, 38–42. [Google Scholar] [CrossRef]
- Detry-Morel, M. Currents on target intraocular pressure and intraocular pressure fluctuations in glaucoma management. Bull. De La Soc. Belg. D’ophtalmologie 2008, 308, 35–43. [Google Scholar]
- Nie, L.; Cheng, D.; Cen, J.; Ye, Y.; Qiao, Y.; Fang, J.; Zhu, X.; Wu, M.; Xu, J.; Liang, Y.; et al. Effects of Exercise on Optic Nerve and Macular Perfusion in Glaucoma and Normal Subjects. J. Glaucoma 2022, 31, 804–811. [Google Scholar] [CrossRef]
- Yeak Dieu Siang, J.; Mohamed MN, A.B.; Mohd Ramli, N.B.; Zahari, M.B. Effects of regular exercise on intraocular pressure. Eur. J. Ophthalmol. 2022, 32, 2265–2273. [Google Scholar] [CrossRef]
- McMonnies, C.W. Intraocular pressure and glaucoma: Is physical exercise beneficial or a risk? J. Optom. 2016, 9, 139–147. [Google Scholar] [CrossRef]
- Vaghefi, E.; Shon, C.; Reading, S.; Sutherland, T.; Borges, V.; Phillips, G.; Niederer, R.L.; Danesh-Meyer, H. Intraocular pressure fluctuation during resistance exercise. BMJ Open Ophthalmol. 2021, 6, e000723. [Google Scholar] [CrossRef]
- Vieira, G.M.; Oliveira, H.B.; de Andrade, D.T.; Bottaro, M.; Ritch, R. Intraocular pressure variation during weight lifting. Arch. Ophthalmol. 2006, 124, 1251–1254. [Google Scholar] [CrossRef]
- Ferguson, T.; Olds, T.; Curtis, R.; Blake, H.; Crozier, A.J.; Dankiw, K.; Dumuid, D.; Kasai, D.; O’Connor, E.; Virgara, R.; et al. Effectiveness of wearable activity trackers to increase physical activity and improve health: A systematic review of systematic reviews and meta-analyses. Lancet. Digit. Health 2022, 4, e615–e626. [Google Scholar] [CrossRef]
- National Institutes of Health All of Us Research Program Investigators. Survey Explorer. Available online: https://www.researchallofus.org/data-tools/survey-explorer/ (accessed on 5 December 2022).
- United Kingdom BioBank. Showcase. Available online: https://biobank.ndph.ox.ac.uk/showcase/ (accessed on 9 December 2022).
- Ma, Q.-Y.; Zhou, J.; Xue, Y.-X.; Xia, Y.-T.; Wu, J.-G.; Yang, Y.-X. Analysis of aerobic exercise influence on intraocular pressure and ocular perfusion pressure in patients with primary open-angle glaucoma: A randomized clinical trial. Indian J. Ophthalmol. 2022, 70, 4228–4234. [Google Scholar] [CrossRef]
- E, J.-Y.; Mihailovic, A.; Garzon, C.; Schrack, J.A.; Li, T.; West, S.K.; Friedman, D.S.; Gitlin, L.N.; Ramulu, P.Y. Importance and Severity Dependence of Physical Activity by GPS-Tracked Location in Glaucoma Patients. Am. J. Ophthalmol. 2021, 230, 276–284. [Google Scholar] [CrossRef]
- Ramulu, P.Y.; Maul, E.; Hochberg, C.; Chan, E.S.; Ferrucci, L.; Friedman, D.S. Real-world assessment of physical activity in glaucoma using an accelerometer. Ophthalmology 2012, 119, 1159–1166. [Google Scholar] [CrossRef]
- Lee, M.J.; Wang, J.; Friedman, D.S.; Boland, M.V.; De Moraes, C.G.; Ramulu, P.Y. Greater Physical Activity Is Associated with Slower Visual Field Loss in Glaucoma. Ophthalmology 2019, 126, 958–964. [Google Scholar] [CrossRef]
- Berry, E.C.; Marshall, H.N.; Mullany, S.; Torres, S.D.; Schmidt, J.; Thomson, D.; Knight LS, W.; Hollitt, G.L.; Qassim, A.; Ridge, B.; et al. Physical Activity Is Associated with Macular Thickness: A Multi-Cohort Observational Study. Investig. Ophthalmol. Vis. Sci. 2023, 64, 11. [Google Scholar] [CrossRef]
- Madjedi, K.M.; Stuart, K.V.; Chua, S.Y.; Ramulu, P.Y.; Warwick, A.; Luben, R.N.; Sun, Z.; Chia, M.A.; Aschard, H.; Wiggs, J.L.; et al. The association of physical activity with glaucoma and related traits in the UK Biobank. Ophthalmology 2023, in press. [Google Scholar] [CrossRef]
- National Institutes of Health All of Us Research Program Investigators. Data Snapshots. Available online: https://www.researchallofus.org/data-tools/data-snapshots/ (accessed on 15 July 2023).
- United Kingdom BioBank. Data Field. Available online: https://biobank.ctsu.ox.ac.uk/crystal/field.cgi?id=21000 (accessed on 15 July 2023).
- Baxter, S.L.; Saseendrakumar, B.R.; Paul, P.; Kim, J.; Bonomi, L.; Kuo, T.-T.; Loperena, R.; Ratsimbazafy, F.; Boerwinkle, E.; Cicek, M.; et al. Predictive Analytics for Glaucoma Using Data From the All of Us Research Program. Am. J. Ophthalmol. 2021, 227, 74–86. [Google Scholar] [CrossRef]
- Natsis, K.; Asouhidou, I.; Nousios, G.; Chatzibalis, T.; Vlasis, K.; Karabatakis, V. Aerobic exercise and intraocular pressure in normotensive and glaucoma patients. BMC Ophthalmol. 2009, 9, 6. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Lin TP, H.; Gao, K.; Zhou, R.; Radke, N.V.; Lam DS, C.; Zhang, X. Aerobic exercise reduces intraocular pressure and expands Schlemm’s canal dimensions in healthy and primary open-angle glaucoma eyes. Indian J. Ophthalmol. 2021, 69, 1127–1134. [Google Scholar] [CrossRef]
- Jiménez, R.; Molina, R.; García, J.A.; Redondo, B.; Vera, J. Wearing Swimming Goggles Reduces Central Corneal Thickness and Anterior Chamber Angle, and Increases Intraocular Pressure. Curr. Eye Res. 2020, 45, 535–541. [Google Scholar] [CrossRef]
- Ma, K.T.; Chung, W.S.; Seo, K.Y.; Seong, G.J.; Kim, C.Y. The effect of swimming goggles on intraocular pressure and blood flow within the optic nerve head. Yonsei Med. J. 2007, 48, 807–809. [Google Scholar] [CrossRef]
- Jasien, J.V.; Jonas, J.B.; de Moraes, C.G.; Ritch, R. Intraocular Pressure Rise in Subjects with and without Glaucoma during Four Common Yoga Positions. PLoS ONE 2015, 10, e0144505. [Google Scholar] [CrossRef]
- Roberts-Lewis, S.F.; White, C.M.; Ashworth, M.; Rose, M.R. Validity of Fitbit activity monitoring for adults with progressive muscle diseases. Disabil. Rehabil. 2022, 44, 7543–7553. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Kim, Y.; Bai, Y.; Burns, R.D.; Brusseau, T.A.; Byun, W. Validation of the Apple Watch for Estimating Moderate-to-Vigorous Physical Activity and Activity Energy Expenditure in School-Aged Children. Sensors 2021, 21, 6413. [Google Scholar] [CrossRef] [PubMed]
- Germini, F.; Noronha, N.; Borg Debono, V.; Abraham Philip, B.; Pete, D.; Navarro, T.; Keepanasseril, A.; Parpia, S.; de Wit, K.; Iorio, A. Accuracy and Acceptability of Wrist-Wearable Activity-Tracking Devices: Systematic Review of the Literature. J. Med. Internet Res. 2022, 24, e30791. [Google Scholar] [CrossRef]
- Leung, W.; Case, L.; Sung, M.C.; Jung, J. A meta-analysis of Fitbit devices: Same company, different models, different validity evidence. J. Med. Eng. Technol. 2022, 46, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.A.; Quante, M.; Godbole, S.; James, P.; Hipp, J.A.; Marinac, C.R.; Mariani, S.; Feliciano, E.M.C.; Glanz, K.; Laden, F.; et al. Variation in actigraphy-estimated rest-activity patterns by demographic factors. Chronobiol Int. 2017, 34, 1042–1056. [Google Scholar] [CrossRef] [PubMed]
- Weinert, D.; Gubin, D. The Impact of Physical Activity on the Circadian System: Benefits for Health, Performance and Wellbeing. Appl. Sci. 2022, 12, 9220. [Google Scholar] [CrossRef]
- Lanzani, M.F.; de Zavalía, N.; Fontana, H.; Sarmiento, M.I.K.; Golombek, D.; Rosenstein, R.E. Alterations of locomotor activity rhythm and sleep parameters in patients with advanced glaucoma. Chronobiol Int. 2012, 29, 911–919. [Google Scholar] [CrossRef]
- Reutrakul, S.; Crowley, S.J.; Park, J.C.; Chau, F.Y.; Priyadarshini, M.; Hanlon, E.C.; Danielson, K.K.; Gerber, B.S.; Baynard, T.; Yeh, J.J.; et al. Relationship between Intrinsically Photosensitive Ganglion Cell Function and Circadian Regulation in Diabetic Retinopathy. Sci. Rep. 2020, 10, 1560. [Google Scholar] [CrossRef]
- Danilenko, K.V.; Stefani, O.; Voronin, K.A.; Mezhakova, M.S.; Petrov, I.M.; Borisenkov, M.F.; Markov, A.A.; Gubin, D.G. Wearable Light-and-Motion Dataloggers for Sleep/Wake Research: A Review. Appl. Sci. 2022, 12, 11794. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhanvadia, S.B.; Meller, L.; Madjedi, K.; Weinreb, R.N.; Baxter, S.L. Availability of Physical Activity Tracking Data from Wearable Devices for Glaucoma Patients. Information 2023, 14, 493. https://doi.org/10.3390/info14090493
Bhanvadia SB, Meller L, Madjedi K, Weinreb RN, Baxter SL. Availability of Physical Activity Tracking Data from Wearable Devices for Glaucoma Patients. Information. 2023; 14(9):493. https://doi.org/10.3390/info14090493
Chicago/Turabian StyleBhanvadia, Sonali B., Leo Meller, Kian Madjedi, Robert N. Weinreb, and Sally L. Baxter. 2023. "Availability of Physical Activity Tracking Data from Wearable Devices for Glaucoma Patients" Information 14, no. 9: 493. https://doi.org/10.3390/info14090493
APA StyleBhanvadia, S. B., Meller, L., Madjedi, K., Weinreb, R. N., & Baxter, S. L. (2023). Availability of Physical Activity Tracking Data from Wearable Devices for Glaucoma Patients. Information, 14(9), 493. https://doi.org/10.3390/info14090493