3. Results
3.1. Five Factor Model-Only (FFM-Only) Profiles
In a latent profile analysis of the FFM-Only domains, a four-profile model yielded the best fit to the data as suggested by theoretical considerations and profile interpretability shown in
Table 2. One profile for the five-profile solution yielded a profile with <5% of participants. Close examination of the five-profile solution suggests that a fifth profile did not enhance interpretability or create a distinct profile with varying level and shape compared to others.
The FFM-only four-profile solution was named descriptively consistent with profiles, as previously labeled by
Yin et al. (
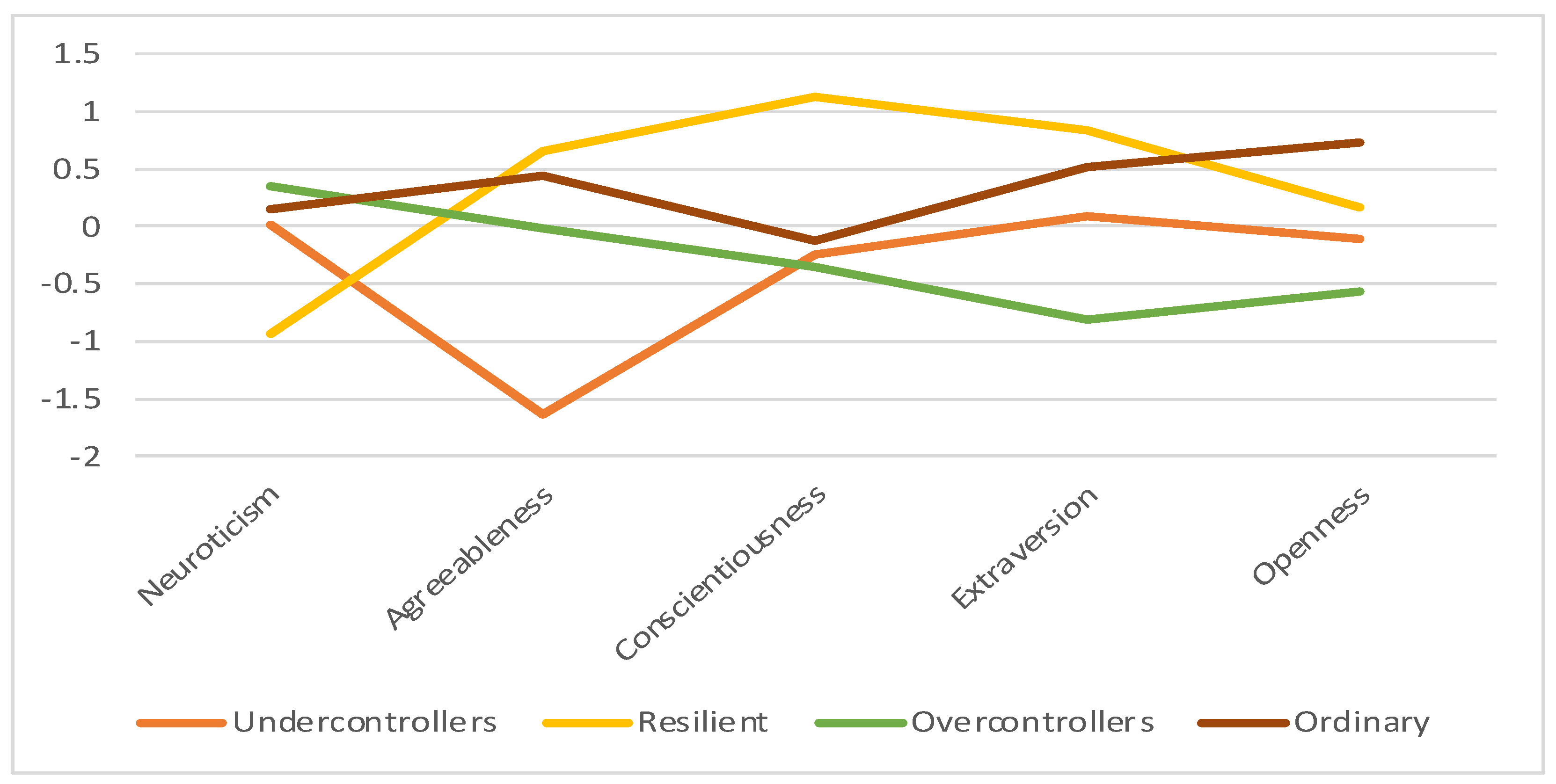
2021) as (1) Undercontroller, (2) Resilient, (3) Overcontroller, and (4) Ordinary (
Figure 1). The Undercontroller profile members (14.4% of participants; 55.6% male, 44.4% female) were between the ages of 20 and 56 (M = 33.54, SD = 12.09). This group was labeled following the lowest scores on agreeableness, low scores on conscientiousness, and mid-ranged scores on neuroticism, extraversion, and openness to experience compared to other profiles. The Resilient profile members (18.5% of participants; 41.7% male, 58.3% female) were between the ages of 22 and 71 (M = 43.58, SD = 13.39) and demonstrated the lowest scores in neuroticism, highest scores in agreeableness, conscientiousness, and extraversion, and mid-ranged scores in openness to experience compared to other profiles. The Overcontrollers group (39.5% of participants; 57.1% male, 42.9% female) between the ages of 18 to 87 (M = 42.12, SD = 14.28) consists of high scores on neuroticism and low scores in conscientiousness, extraversion, and openness to experience. This profile is also characterized by mid-ranged agreeableness. The Ordinary profile (27.7% of respondents; 49.5% male; 50.5% females) were between ages 18 to 62 (M = 36.17, SD = 11.99) and exhibited mid-ranged neuroticism, agreeableness, conscientiousness, and extraversion. This term was amongst those most commonly used when profiles demonstrate mid-range responses on traits (
Yin et al. 2021). This profile has the highest openness to experience score compared to other profiles. The most critical variable in determining profiles was agreeableness, as evinced with the largest effect size and VS-MPR (ηp
2 = 0.58; VS-MPR = 1.31 × 1032), reflecting more significant differences between profiles. The least essential variable is openness to experience, as apparent with the smallest effect size and VS-MPR (ηp
2 = 0.33; VS-MPR = 1.48 × 1013). Details are found in
Appendix A.
Demographic effects on profile membership were assessed and no gender differences were found (χ
2[3, N = 201] = 4.74,
p = 0.19, BF
10 Independent Multinomial = 0.14). Age predicted profile membership (P[M] = 0.50, P[M|data] = 0.93, BF
M = 14.14, error % = 0.02). With posterior odds corrected for multiple testing with prior odds set as 0.41 (
Westfall et al. 1997), there was strong evidence that the Undercontroller profile (M = 33.54, SD = 12.09) was younger than the Resilient profile (M = 43.58, SD = 13.39; Posterior Odds = 5.31; BF
10 = 12.83, error% < 0.001). There was moderate evidence that the Undercontroller profile members were younger than Overcontroller profile members (M = 42.12, SD = 14.28; Posterior Odds = 2.93, BF
10 = 7.08, errors% < 0.001), Ordinary profile (M = 36.17, SD = 11.99) was younger than the Resilient profile (Posterior Odds = 2.33, BF
10 = 5.63, error% < 0.001), and the Ordinary profile was younger than the Overcontroller profile (Posterior Odds = 1.30, BF
10 = 3.14, error% < 0.01). No evidence was found for other age differences between profiles.
3.2. Associations of FFM Only Profiles with Clinical Symptoms and Cognitive Ability Measures
When accounting for the error variance and the effects of gender and age, profile membership was associated with problematic gambling. In particular, the model with profile, gender, and age (P[M] = 0.13, P[M|Data] = 0.59, BFM = 9.97, BF10 = 422.62, error% = 0.88) compared to the gender and age model (P[M] = 0.13, P[M|data] = 0.05, BFM = 0.34, BF10 = 33.00, error% < 0.01) was a better fit for the data. The model with profile membership with covariates was preferred to the covariates only model by a factor of 13 (422.62/33 ≃ 12.80). Post hoc comparisons suggested that the Undercontroller profile (M = 3.64; SD = 5.90) was more likely to engage in problematic gambling than the Resilient (M = 1.11, SD = 3.65; Posterior Odds = 82.81, BF10,U = 199.91, error% < 0.001) and Ordinary profiles (M = 1.00, SD = 2.35; Posterior Odds = 19.95, BF10,U = 48.17, error% < 0.001). When using established cut-offs (PGSI ≥ 3) for problematic gambling, a Chi-Square Test of Independence showed a significant relationship between profile membership and problematic gambling with medium effect sizes, χ2(3, N = 199) = 9.79, p < 0.05, VS-MPR = 4.62, Cramer’s V = 0.22, BF10 = 0.45. The number of individuals who engaged in problematic gambling was greater than expected in the Undercontroller profile (z = 2.72).
FFM profile membership did not appear to predict problematic alcohol use, matrix reasoning, or verbal abilities. When gender, age, and profile membership were entered to predict problematic alcohol use, the age-only model (P[M] = 0.13, P[M|Data] = 0.47, BFM = 6.14, BF10 = 2.04, error% < 0.01) outperformed other models containing profile membership. Chi-square tests were consistent with these findings, with no association between profile membership and problematic alcohol use (AUDIT ≥ 5), χ2[3, N = 199] = 5.21, p = 0.16, BF10 = 0.18). For matrix reasoning, there was no evidence that the profiles model (P[M] = 0.50, P[M|Data] = 0.45, BFM = 0.83, BF10 = 0.83, error% < 0.001) is a better fit than the null model (P[M] = 0.50, P[M|Data] = 0.55, BFM = 1.21, BF10 = 1.00). Similarly, there was no evidence that the profiles model (P[M] = 0.50, P[M|Data] = 0.48, BFM = 0.91, BF10 = 0.91, error% < 0.001) outperforms the null model (P[M] = 0.50, P[M|Data] = 0.52, BFM = 1.10, BF10 = 1.00) for verbal reasoning.
Table 3 shows counts and standardized residuals of profile membership and diagnosis. There was no association between lifetime anxiety disorder diagnosis and profile membership (χ
2[3, N = 200] = 0.45,
p = 0.93, BF
10 Independent Multinomial = 0.02). However, profile membership was significantly associated with current anxiety disorder (χ
2[3, N = 200] = 7.90,
p = 0.05, BF
10 Independent Multinomial = 0.82). The Resilient group was less likely than expected to meet criteria for a current anxiety disorder (z = −2.28) and the Overcontroller group was more likely to meet criteria for a current anxiety disorder (z = 2.39). No significant relationships were found between profiles membership and lifetime substance use disorder (χ
2[3, N = 201] = 0.35,
p = 0.95, BF
10 Independent Multinomial = 0.01) and current substance use disorder (χ
2[3, N = 199] = 5.95,
p = 0.11, BF
10 Independent Multinomial = 0.12). No significant associations were found between profile membership and lifetime mood disorder (χ
2[3, N = 200] = 2.97,
p = 0.40, BF
10 Independent Multinomial = 0.08) and current mood disorder (χ
2 [3, N = 200] = 5.48,
p = 0.14, BF
10 Independent Multinomial = 0.21).
3.3. AMPD Profiles
Like the extraction with FFM-only profiles, the optimal number of profiles was selected based on theoretical considerations, profile interpretability, and the comparison of alternative profile solutions (see
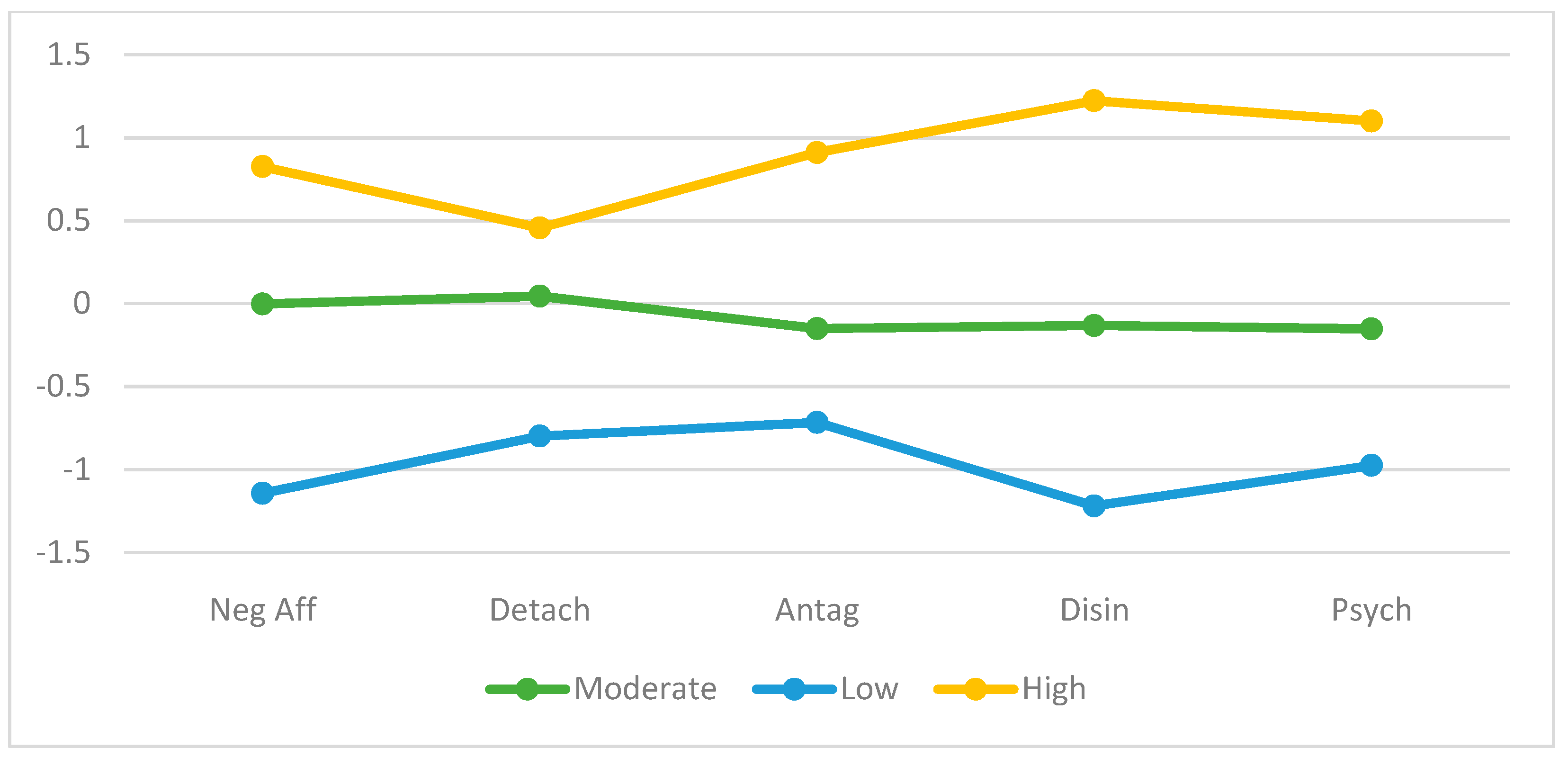
Table 4). The three-profile solution was the most suitable given theoretical considerations and it demonstrated the highest classification accuracy as the BIC reaches a minimum and entropy a maximum at three profiles (see
Figure 2). The High Psychopathology group (22.1% of respondents; 39.5% male, 60.46% female) was between the ages of 20 to 56 (M = 30.73; SD = 8.89) and consisted of the highest scores across all pathological personality domains compared to the other two profiles. The Moderate Psychopathology group (62.3% of respondents; 54.5% male, 45.5% female) was between the ages of 18 to 87 (M = 41.23; SD = 13.71) and revealed moderate scores across all personality domains compared to the other two profiles. The Low Psychopathology group (n = 30, 43.33% male, 56.67% female) was between the ages of 19 and 71 (M = 45.43; SD = 13.52) and showed the lowest scores across all personality domains compared to the other two profiles. The most critical variable was disinhibition as evinced by the largest effect size estimates VS-MPR (ηp
2 = 0.60; VS-MPR = 3.46 × 1035). The least essential variables were detachment (ηp
2 = 0.24; VS-MPR = 2.02 × 10 + 9) and antagonism (ηp
2 = 0.24; VS-MPR = 2.85 × 10 + 9), with the smallest effect size and VS-MPR.
Profiles did not differ based on gender (χ
2[3, N = 194] = 5.92,
p = 0.21, BF
10 Independent Multinomial = 0.28). Age predicted profile membership (P[M] = 0.50, P[M|data] = 1.00, BF
M = 12,364, error % = 0.02). With posterior odds corrected for multiple testing and prior odds set as 0.59 (
Westfall et al. 1997), there was extreme evidence that the High Psychopathology group were younger than the Moderate Psychopathology group (Posterior Odds = 1910; BF
10 = 3251, error% < 0.001) and Low Psychopathology group (Posterior Odds = 24,011, BF
10 = 40,877, errors% < 0.001). No evidence was found for other age differences between Moderate and Low Psychopathology profiles.
3.4. Associations of AMPD-Only Profiles with Clinical Symptoms and Cognitive Ability Measures
After explaining the error variance attributable to gender and age, profile membership was associated with enhanced problematic gambling. As such, the model with profile and gender (P[M] = 0.13, P[M|Data] = 0.53, BFM = 7.89, BF10 = 1359, error% = 1.78) outperformed other combinations of the profile, gender, and age. Post hoc tests indicated that High Psychopathology (M = 3.32, SD = 5.29) scored higher than Moderate Psychopathology (M = 1.05, SD = 2.20; Posterior Odds = 42.07, BF10,U = 71.63, error% < 0.001) and Low Psychopathology on the PGSI (M = 1.55, SD = 4.41; Posterior Odds = 12.19, BF10,U = 20.75, error% < 0.001). There was a significant relationship between profile membership and problematic gambling with medium to large effect sizes, χ2(3, N = 199) = 13.92, p < 0.001, VS-MPR = 55.62, Cramer’s V = 0.26, BF10 = 25.13. The High Psychopathology group (z = 3.71) were likelier than expected to meet the cut-off for problematic gambling.
When accounting for the error variance and the effects of gender and age, profile membership was associated with problematic alcohol use. Specifically, the model with profile (P[M] = 0.13, P[M|Data] = 0.49, BFM = 6.63, BF10 = 9.69, error% = 0.01) was more probable than other combinations of gender, age, and profile. Post hoc comparisons suggested that the High Psychopathology profile (M = 10.77, SD = 8.27) scored higher than Moderate (M = 7.17, SD = 8.57; Posterior Odds = 14.05, BF10,U = 23.91, error% < 0.001) and Low Psychopathology profiles (M = 4.55, SD = 5.51; Posterior Odds = 221, BF10,U = 376, error% < 0.001) on the AUDIT. When using cut-offs (AUDIT ≥ 5), a Chi-Square Test of Independence showed a significant link between profile membership and alcohol use, χ2(3, N = 199) = 10.89, p < 0.01, VS-MPR = 15.65, Cramer’s V = 0.23, BF10 = 11.87. The High Psychopathology group (z = 3.26) was more likely to meet the cut-off for problematic alcohol use than expected.
AMPD-only profile membership did not predict matrix reasoning or verbal abilities. For matrix reasoning, the null model (P[M] = 0.50, P[M|Data] = 0.91, BFM = 9.83, BF10 = 0.10) outperforms the profiles model (P[M] = 0.50, P[M|Data] = 0.09, BFM = 0.10, BF10 = 0.10, error% = 0.02). Similarly, the null model (P[M] = 0.50, P[M|Data] = 0.92, BFM = 11.92, BF10 = 1.00) for verbal reasoning outperforms the profiles model (P[M] = 0.50, P[M|Data] = 0.08, BFM = 0.08, BF10 = 0.08, error% = 0.02).
There was no significant relationship between profile membership and lifetime anxiety disorder diagnosis, χ
2(2, N = 200) = 7.15,
p = 0.38, BF
10 = 0.13. There was a significant association between AMPD-only profile membership and current anxiety disorder diagnosis, χ
2(2, N = 200) = 13.00,
p < 0.01, VS-MPR = 37.57, Cramer’s V = 0.25, BF
10 = 28.89. As expected, the High Psychopathology group was more likely than expected to meet criteria for an anxiety disorder (z = 3.04), whereas the Low Psychopathology group was less likely than expected to meet criteria for an anxiety disorder (z = −2.58). There was a significant association between profile membership and lifetime substance use disorder, χ
2(2, N = 201) = 8.38,
p < 0.05, VS-MPR = 5.79, Cramer’s V = 0.20, BF
10 = 2.32, and current substance use disorder, χ
2(3, N = 199) = 8.17,
p < 0.05, VS-MPR = 5.35 Cramer’s V = 0.20, BF
10 = 4.63. In both cases, the High Psychopathology group was more likely to meet the criteria, whereas the Low Psychopathology group were less likely to meet the criteria for substance use disorder (
Table 3). There was no evidence that AMPD profile membership was associated with lifetime mood disorder, χ
2(2, N = 200) = 1.91,
p = 0.38, BF
10 = 0.11, or current mood disorder, χ
2(2, N = 200) = 4.28,
p = 0.12, BF
10 = 0.36.
3.5. FFM–AMPD Profiles
The five factors from the BFAS and PID-5 were finally entered in a latent profile analysis (
Table 5). The five-profile solution had lowest BIC of all profiles and the highest entropy. However, examination of the profiles produced by the five-profile solutions suggested the “adaptive profile” from the four-profile solution was split into two separate profiles based on severity (i.e., one endorsing more psychopathology, one endorsing less). Thus, the more parsimonious four-profile solution was the most suitable given that it created distinct, practically meaningful profiles, yet showed a better fit for the data than the three-profile solution (
Spurk et al. 2020).
FFM-only and AMPD-only profiles extracted earlier in our samples were named according to profiles extracted in previous investigations. The profiles extracted from the combination of FFM and AMPD traits required a different naming system given that these present profiles have not been previously extracted (i.e., previous studies used a different and narrower set of traits from which profiles were extracted). The profiles were labelled adhering to naming practices specific to a theoretical framework (
Weller et al. 2020). The Hierarchical Taxonomy of Psychopathology (HiTOP) consortium outlines significant psychopathology dimensions at the higher-order spectra: internalizing, somatoform, disinhibited externalizing, antagonistic externalizing, thought disorder, and detachment. The spectra can be combined into larger superspectra: emotional dysfunction (internalizing and somatoform), externalizing (disinhibited and antagonistic), and psychosis (thought disorder and detachment;
Kotov et al. 2017,
2020;
Markon et al. 2011).
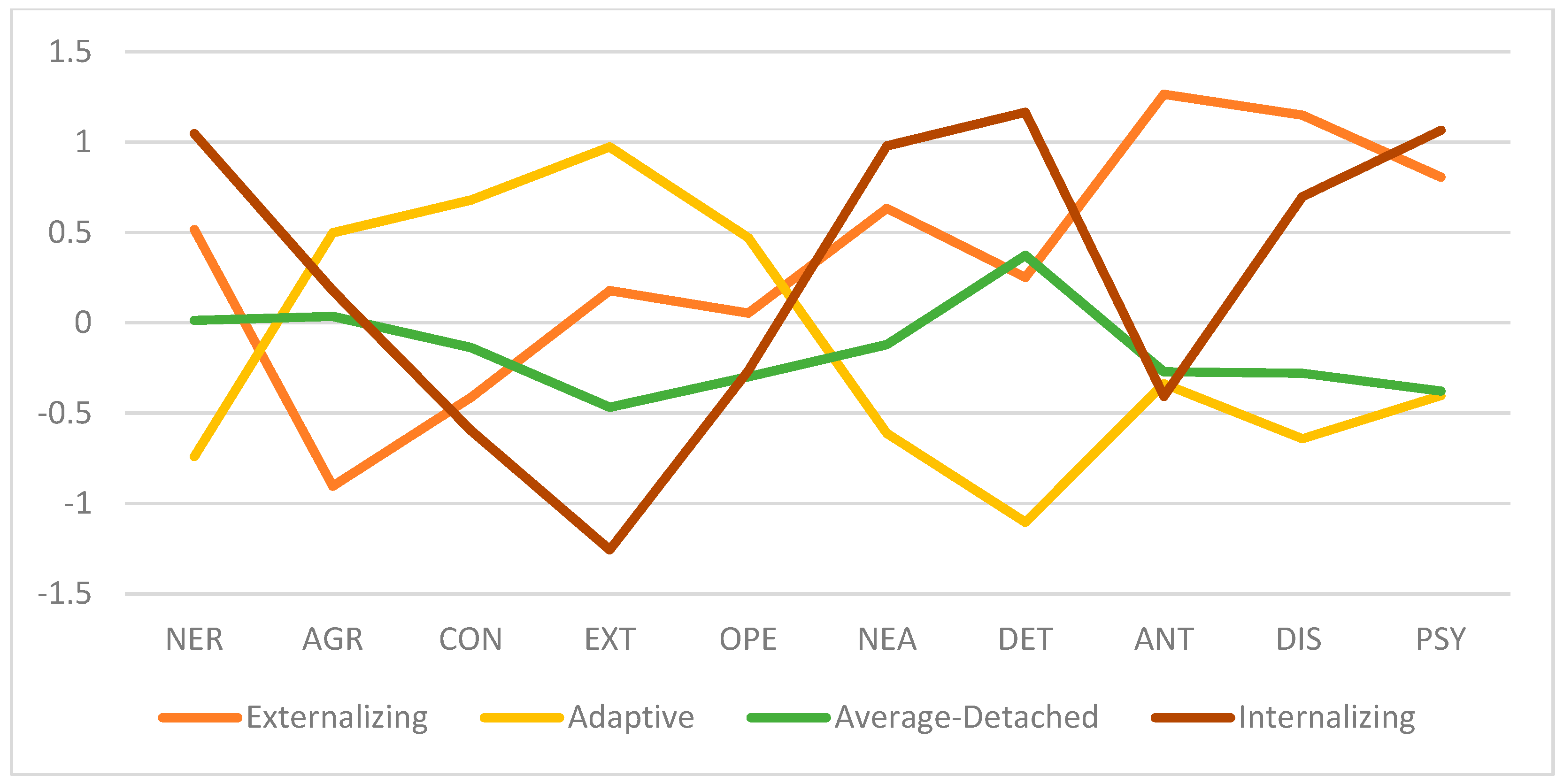
Figure 3 shows a visual depiction of the means across profiles. The Externalizing profile members (21.5% of respondents; 46.3% male, 53.7% female) were between the ages of 20 to 56 (M = 32.31; SD = 10.37) and labeled accordingly based on the lowest scores in agreeableness and highest scores in antagonism and disinhibition. The Adaptive profile (28.2% of respondents, 45.5% male, 54.5% female) between the ages of 19 and 71 (M = 39.67; SD = 12.86) has the lowest neuroticism, negative affectivity, detachment, antagonism, disinhibition, and psychoticism while exhibiting the highest agreeableness, conscientiousness, extraversion, and openness to experience compared to its counterparts. The Average-Detached profile (40% of respondents, 57.7% male, 42.3% female) was between the ages of 18 to 73 (M = 43.27; SD = 13.99) and shows moderate scores across all domains with the lowest scores in openness to experience (tied with Internalizing-Thought disorder profile) and psychoticism (tied with the Adaptive profile). The Average-Detached profile was labelled as such given its maxima is in the detachment domain. The Internalizing-Thought disorder profile (10.3% of respondents, 35% male, 65% female) between the ages of 18 to 73 (M = 43.27; SD = 13.99) had the lowest extraversion and openness to experience and highest neuroticism, negative affectivity, detachment, and psychoticism compared to other profiles. In this latent profile analysis, the most important variable is detachment as evinced with the largest effect size and VS-MPR (ηp
2 = 0.61; VS-MPR = 4.55 × 10 + 34), reflecting larger differences between profile memberships. The least important variable is openness-to-experience, with the smallest effect size and VS-MPR (ηp
2 = 0.09; VS-MPR = 88.35).
Appendix A shows details of these analyses.
Similar to previous findings, profiles did not differ based on gender (χ
2[3, N = 194] = 4.30,
p = 0.23, BF
10 Independent Multinomial = 0.11). Age predicted profile membership (P[M] = 0.50, P[M|data] = 0.99, BF
M = 77.31, error % < 0.01). With posterior odds corrected for multiple testing and prior odds set as 0.41 (
Westfall et al. 1997), there was extreme evidence that the Externalizing profile was younger than the Average-Detached profile (Posterior Odds = 395; BF
10 = 955, error% < 0.001) and strong evidence that the Externalizing group was younger than the Adaptive profile (Posterior Odds = 4.66, BF
10 = 11.26, errors% < 0.001). No evidence was found for other age differences for other profiles.
3.6. Associations of FFM–AMPD Profiles with Clinical Symptoms
When accounting for the error variance and the effects of gender and age, profile membership was associated with problematic gambling (
Table 6). The model with profile, gender, and age (P[M] = 0.13, P[M|Data] = 0.51, BF
M = 7.25, BF
10 = 389.21, error% = 1.33) was compared to the gender and age model (P[M] = 0.13, P[M|data] = 0.04, BF
M = 0.32, BF
10 = 33.00, error% < 0.01). The model with profile group was preferred in predicting problematic gambling to the covariates only model by a factor of 12 (389/33 ≃ 11.79). Post hoc tests show that the Externalizing profile (M = 3.19; SD = 5.23) scored higher than Average-Detached (M = 0.96, SD = 2.20; Posterior Odds = 30.37, BF
10, U = 73.33, error% < 0.001) and Adaptive (M = 1.26, SD = 3.31; Posterior Odds = 13.02, BF
10, U = 31.43, error% < 0.001) profiles. When using cut-offs for problematic gambling (PGSI ≥3), a Chi-Square Test of Independence revealed a significant relationship between the profile memberships and problematic gambling with medium effect sizes, χ
2(3, N = 199) = 12.21,
p < 0.01, VS-MPR = 10.96, Cramer’s V = 0.25, BF
10 = 1.20. The Externalizing profile members (z = 3.47) were more likely to meet the cut-off for problematic gambling compared to the other groups.
There was only anecdotal evidence that profile membership was linked with problematic alcohol use (P[M] = 0.13, P[M|Data] = 0.28, BFM = 2.74, BF10 = 2.57, error% < 0.001). However, there was a significant relationship between problematic alcohol use and profile membership with medium effect sizes when using categorical cut-offs (AUDIT ≥ 5), χ2(3, N = 199) = 11.80, p < 0.01, VS-MPR = 9.41, Cramer’s V = 0.24, BF10 = 4.91. The Externalizing profile was more likely (z = 2.64) to meet the criteria than expected.
Based on Bayesian ANOVA, there was no evidence that the FFM–AMPD profile membership was associated with matrix reasoning and verbal abilities. For verbal comprehension, there was no evidence that the profiles model (P[M] = 0.50, P[M|Data] = 0.04, BFM = 0.04, BF10 = 0.04, error% < 0.01) outperforms the null model (P[M] = 0.50, P[M|Data] = 0.96, BFM = 25.52, BF10 = 1.00). Similarly, there was no evidence that the profiles model (P[M] = 0.50, P[M|Data] = 0.04, BFM = 0.04, BF10 = 0.04, error% < 0.01) outperforms the null model (P[M] = 0.50, P[M|Data] = 0.96, BFM = 25.24, BF10 = 1.00) for matrix reasoning.
There were no significant associations between profile membership and lifetime DSM diagnosis, including lifetime anxiety disorder (χ2[3, N = 200] = 3.97, p = 0.26, BF10 Independent Multinomial = 0.09), lifetime substance use disorder (χ2[3, N = 201] = 6.92, p = 0.07, BF10 Independent Multinomial = 0.37), and lifetime mood disorder (χ2[3, N = 200] = 3.96, p = 0.27, BF10 Independent Multinomial = 0.12).
Profile membership was associated with current anxiety disorder diagnosis (χ2[3, N = 200] = 18.58, p < 0.001, Cramer’s V = 0.30, VS-MPR > 100, BF10 Independent Multinomial = 236.93). The Internalizing-Thought disorder profile was more likely than expected to meet the criteria for an anxiety disorder (z = 2.83), whereas the Adaptive group were less likely to meet the criteria for a current anxiety disorder (z = 3.77). Profile membership was also significantly associated with current substance use disorder (χ2[3, N = 199] = 8.29, p < 0.05 Cramer’s V = 0.20, VS-MPR = 2.84, BF10 Independent Multinomial = 1.10). The Externalizing profile was more likely than expected to meet the criteria for a current substance use disorder (z = 2.64). Profile membership was associated with current mood disorder (χ2 [3, N = 200] = 8.57, p < 0.05, Cramer’s V = 0.21, VS-MPR = 3.09, BF10 Independent Multinomial = 0.98). The Internalizing group were more likely (z = 2.21) and the Adaptive group were less likely (z = −2.27) to meet the criteria for a current mood disorder.
3.7. Comparisons of Profiles
Significant overlaps existed between the FFM-only and the FFM–AMPD combined profiles, χ
2 [9, N = 201] = 160.58,
p < 0.001, Cramer’s V = 0.52, VS-MPR > 100, BF
10 Independent Multinomial > 100 (
Table 6). Specifically, the FFM-only Undercontroller profile overlaps largely with the FFM–AMPD Externalizing profile, whereas the FFM-only Resilient profile corresponds with the FFM–AMPD combined Adaptive profile. The FFM-only Overcontrollers profile resembles both the FFM–AMPD combined Average-Withdrawn and Internalizing-Thought disorder profiles. The FFM-only Ordinary profile is more widely dispersed compared to the other profiles but shows the most overlap (non-significant) with the Adaptive profile.
When comparing AMPD-only and the FFM–AMPD combined profiles, there were significant connections between the profiles χ2 [6, N = 201] = 172.32, p < 0.001, Cramer’s V = 0.65, VS-MPR > 100, BF10 Independent Multinomial > 100). Specifically, the FFM–AMPD Externalizing and Internalizing profiles overlap largely with the AMPD-only High Psychopathology group. The FFM–AMPD Adaptive profile corresponds with the AMPD-only Low Psychopathology group whereas the FFM–AMPD Average-Withdrawn profile intersects with the AMPD-only Moderate Psychopathology group.
Finally, there were significant associations between the FFM-only and AMPD-only profiles, χ2 [6, N = 201] = 86.43, p < 0.001, Cramer’s V = 0.46 VS-MPR > 100, BF10 Independent Multinomial > 100. The FFM-only Undercontroller profile largely overlaps with the AMPD-only High Psychopathology group whereas the FFM-only Resilient profile overlaps with Low Psychopathology. The FFM-only Overcontroller and Ordinary profiles demonstrate significant overlap with the AMPD-only Moderate Psychopathology group.
4. Discussion
Our main goal for this investigation was to attempt to extract latent profiles from FFM and AMPD both together and separately to determine whether the additional construct coverage of AMPD personality traits may add additional information to the FFM. In the past decade, the AMPD has gained considerable attention as it provides information on personality psychopathology with practical and significant clinical implications (
Clark and Watson 2022). Using best practices with latent profile analyses, four profiles (i.e., Undercontroller, Overcontroller, Ordinary, and Resilient) were extracted when only the FFM was used, and AMPD-only profiles uncovered three profiles of High, Moderate, and Low Psychopathology. When considering both the FFM and AMPD, four profiles were revealed as Internalizing-Thought disorder, Externalizing, Average-Detached, and Adaptive profiles. Notably, entropy, as a measure of how accurately the model defines profiles (
Celeux and Soromenho 1996;
Wang et al. 2017), was the highest in the FFM–AMPD combined profiles (entropy = 0.84) compared to FFM-only (entropy = 0.66) and AMPD-only (entropy = 0.79). The minimal value of the diagonal of the average latent class probabilities for the most probable profile was also highest in FFM–AMPD profiles. These results suggest a better fit of the model with the data when using FFM–AMPD profiles. Given that entropy indicates the mixture model’s ability to return well-separated profiles, the FFM-only profiles may not provide distinguished separation between profiles. Hence, future studies should investigate whether FFM traits may be combined with other indicators for profile formation to enhance entropy.
Our first research objective was to evaluate whether a four-profile solution of the FFM would emerge in a clinical sample as it did previously in community and clinical samples. The characteristics of the four profiles extracted from the FFM-only profiles were broadly consistent with the average level and shape compared to other community and university samples with
Yin et al.’s (
2021) systematic review. The Undercontroller profile members demonstrated low agreeableness and conscientiousness, whereas the Overcontrollers group exhibited high neuroticism and low extraversion and openness-to-experience. The Resilient group emerged with low neuroticism and high agreeableness, openness to experience, extraversion, and conscientiousness. Consistent with other latent profiles extracted with the FFM, an Ordinary group also emerged with mid-ranged symptoms across all domains compared to other profiles (
Kinnunen et al. 2012;
Zhang et al. 2015;
Min and Su 2020). Given the dimensional nature of these constructs, individuals classified under these symptom profiles with mid-ranged symptoms may not be experiencing significant personality psychopathology but are also not free of symptoms.
Latent profile analyses with only AMPD traits revealed three AMPD profiles with identical shapes of varying levels of psychopathology (i.e., high, moderate, and low). These findings reflect other latent profiles that found similar high and low personality psychopathology with similar shapes (e.g.,
Ahmed et al. 2021;
Li et al. 2019;
Tabak and Weisman de Mamani 2013). Like the p factor in psychopathology (
Caspi et al. 2014;
Caspi and Moffitt 2018), the p factor in personality disorders as an integrated personality trait may explain why all five pathological personality traits are highly comorbid (
Asadi et al. 2021). Of note, these results differ from that of
Hanegraaf et al. (
2022), who extracted four profiles using the AMPD. Notably,
Hanegraaf et al. (
2022) utilized the short version of the PID-5 and recruited an MTURK sample as opposed to a treatment-seeking clinical sample in the present study. In the present study, four profiles were not extracted given the increase in BIC and a large decrease in entropy. Based on sample characteristics (i.e., age, gender, clinical status), the number and type of profiles may differ. Future studies should replicate findings to reveal whether community or clinical samples may differ based on the number of profiles extracted.
The second research objective was to extract profiles from both FFM and AMPD and compare them to FFM-only and AMPD-only profiles. This is the first study to assess personality profiles that both the FFM and AMPD provided. Results corroborate that the sample size and characteristics of the FFM–AMPD profiles were different from FFM-only and AMPD-only. Within the FFM-only profiles, the present study found that agreeableness and openness to experience were the most and least important variables, respectively, when distinguishing between profiles. Likewise,
Yin et al. (
2021) found across 34 studies that openness to experience is the least important for the profile classification but found neuroticism as the most important dimension. For AMPD, the most important variable is disinhibition while the least important variables were detachment and antagonism. In contrast, the most important variable is detachment while the least important is openness to experience in the FFM–AMPD profiles. Remarkably, the detachment dimension showed high scores in the Externalizing and Internalizing-Thought disorder profiles, moderate scores with the Average-Detached profile, and low scores in the Adaptive profile. For AMPD, detachment was high, moderate, and low in the High Psychopathology, Moderate Psychopathology, and Low Psychopathology group, respectively. The distribution of trait scores differs more substantively across profiles in the FFM–AMPD combined profiles. These findings speak to the differential results in latent profiles when FFM and AMPD measures are combined, despite the substantive conceptual overlap in four of five traits between the FFM and AMPD. Importantly, 19 of 42 (45.2%) individuals classified as Externalizing were Undercontrollers while 19 of 28 (67.86%) individuals classified as Undercontrollers were part of the Externalizing group. Moreover, 18 of 20 (90%) Internalizing-Thought disorder members were classified as Overcontrollers, yet 18 of 79 Overcontrollers (22.78%) were classified as Internalizing-Thought disorder. In other words, almost all members of the Internalizing group are Overcontrollers, but only a quarter of Overcontrollers have Internalizing-Thought disorder membership. Combined with the findings of higher neuroticism scores in the Internalizing-Thought disorder group and that this group was associated with current mood disorder diagnosis, the Internalizing-Thought disorder profile may be extracted as a group with more severe psychopathology within the Overcontrollers.
No gender differences were found across all profiles, which is contrary to expectations that males and females are overrepresented among Undercontrollers and Overcontrollers, respectively (e.g.,
Akse et al. 2004;
Asendorpf et al. 2001;
Dubas et al. 2002). Moreover, verbal and matrix reasoning scores did not differ even though lower IQ in childhood and adulthood were associated with enhanced risk of psychopathology (
Koenen et al. 2009;
Melby et al. 2020). Executive function and cognitive reserve are implicated across psychiatric disorders and may, therefore, not discriminate well at this level of resolution. Specifically, this study recruited a treatment-seeking clinical sample in a mental health hospital, suggesting that almost all patients are expected to be experiencing significant internalizing or externalizing psychopathology. Perhaps the addition of a community-based sample who completed the questionnaires and cognitive tasks into the analyses may indicate substantive differences across cognitive ability between groups. Future studies should uncover whether these profiles may be associated with differential scores with the full WAIS battery in a mixed community and clinical sample (
Wechsler 1997).
Our third goal was to examine to whether profiles showed differential patterns of association with a set of external criterion variables. In the FFM-only profiles, Undercontrollers were more likely to report problematic gambling and Overcontrollers were more likely to be diagnosed with an anxiety disorder. Results were consistent with findings that classification as an undercontroller at age 3 predicted future problematic gambling habits in adulthood, even when controlling for socio-economic status and childhood IQ (
Slutske et al. 2012). For AMPD-only profiles, the High Psychopathology profile was more likely to engage in problematic gambling and alcohol use than other groups. Members of the High Psychopathology group were also more likely diagnosed with a current anxiety disorder and substance use disorder, but not a mood disorder. For FFM–AMPD, the Internalizing-Thought disorder profile was more likely to meet the criteria for a current mood and anxiety disorder. The Externalizing profile was more likely to meet the criteria for a current substance use disorder and engage in problem gambling and alcohol use.
In contrast to FFM-only profiles that were not associated with current substance use disorder and mood disorder, the FFM–AMPD combined profiles may have better convergent and discriminant validity for DSM-relevant psychopathology. Notably, the profiles were only associated with current, but not lifetime, diagnosis, suggesting that these profiles reflected current symptoms, difficulties, and impairments experienced. Profiles may be associated with current diagnoses, but not lifetime diagnoses, because the PID-5 assesses significant personality dysfunction at present and personality may change over the course of the lifetime and throughout treatment (
Roberts et al. 2006,
2017). Lifetime diagnoses may be indicative of acute symptom changes at a specific time, which may not be reflective of the individual‘s current disposition. The combined profiles may be meaningful and clinically useful for the clinical population under investigation.
Limitations and Future Directions
The present study is not without some limitations. First, the study used self-report measures as indicators for latent profiles, which may be predisposed to social desirability or degree of insight for the individual. Future studies should evaluate whether informant reports of the five-factor model of personality and alternative model of personality disorder traits produce similar profiles found in this study (
Markon et al. 2013). Second, the cross-sectional nature of this study limits any causal extrapolations regarding the influences of these profile characteristics on clinical symptoms and mental health disorder diagnoses. Of note, the individuals falling in the High Psychopathology, Undercontrollers, and Externalizing profiles were younger than others, which was consistent with previous findings (
Specht et al. 2014). Undercontrollers tend to experience increased agreeableness over time, which may suggest improvements with poor behavioural control with age (
Klimstra et al. 2010;
Morizot and Le Blanc 2005). Furthermore, externalizing psychopathology in youth is linked with developing mood disorders in adulthood (
Loth et al. 2014). Future studies may assess whether heterotypic continuity occurs in personality profiles, such as that of psychiatric disorders across the lifespan (
Lavigne et al. 2014;
Lahey et al. 2014). Of note, the present study excluded patients with current or lifetime history of psychotic disorder. Samples with patients who have or are currently experiencing psychosis may have a broader range of psychoticism in AMPD-based profile formation. Third, the associated measures evaluated in the present study were limited to cognitive ability, problematic gambling, problematic alcohol use, and DSM diagnoses. Future studies should explore whether these profiles may be able to distinguish other behavioural addictions, such as problematic gaming (e.g.,
Richard et al. 2020), which are associated with both internalizing and externalizing symptoms (
Lau et al. 2018). Future studies should also investigate whether self-reported profiles align with specific neurodevelopmental processes and mechanisms (
Casey et al. 2014). Fourth, the stability of the latent profile solutions needs to be replicated, as previous findings revealed unstable or unreliable latent class solutions across individuals (
Freudenstein et al. 2019). Future studies should replicate these findings and utilize both raw and age-corrected scores for intelligence measures. Lastly, the present study utilized the classification scheme of personality disorder consistent with the PID-5 aligned with DSM-5 classification. Using the International Classification of Disease (11th ed.; ICD-11) personality disorder (PD) conceptualization of psychopathology,
Sellbom et al. (
2020) proposed five trait domains that may be measured with the PID-5: Negative Affectivity, Detachment, Dissociality, Disinhibition, and Anankastia. Future findings should consider whether similar or conceptually distinct personality profiles emerge using these different classifications of pathological personality traits.



{kind=link}
{kind=link}
{kind=link}


