Intraoperative Bacterial Contamination and Activity of Different Antimicrobial Prophylaxis Regimens in Primary Knee and Hip Replacement

 , ,
, , 
 and
and 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Setting and Patients
2.2. Surgical Antimicrobial Prophylaxis Regimens
2.3. Sample Collection
2.4. Determination of Antibiotic Levels
2.5. Microbiological Methods
2.6. Statistical Methods
3. Results
3.1. Patients and Surgical Antimicrobial Prophylaxis
3.2. Intraoperative Cultures
3.3. Susceptibility of Bacterial Isolates and ATCC Strains, Antibiotic Plasma Levels and Serum Bactericidal Titers
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owens, C.D.; Stoessel, K. Surgical site infections: Epidemiology, microbiology and prevention. J. Hosp. Infect. 2008, 70, 3–10. [Google Scholar] [CrossRef]
- Batty, L.M.; Lanting, B. Contemporary Strategies to Prevent Infection in Hip and Knee Arthroplasty. Curr. Rev. Musculoskelet. Med. 2020, 13, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Gallo, J.; Nieslanikova, E. Prevention of Prosthetic Joint Infection: From Traditional Approaches towards Quality Improvement and Data Mining. J. Clin. Med. 2020, 9, 2190. [Google Scholar] [CrossRef]
- Aboltins, C.A.; Berdal, J.E.; Casas, F.; Corona, P.S.; Cuellar, D.; Ferrari, M.C.; Hendershot, E.; Huang, W.; Kuo, F.; Malkani, A.; et al. Hip and Knee Section, Prevention, Antimicrobials (Systemic): Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S279–S288. [Google Scholar] [CrossRef]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am. J. Heal. Pharm. 2013, 70, 195–283. [Google Scholar] [CrossRef] [Green Version]
- Talbot, T.R. Surgical Site Infections and Antimicrobial Prophylaxis. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases; Elsevier: New York, NY, USA, 2019; pp. 3891–3904. [Google Scholar] [CrossRef]
- Benito, N.; Franco, M.; Ribera, A.; Soriano, A.; Rodriguez-Pardo, D.; Sorli, L.; Fresco, G.; Fernandez-Sampedro, M.; del Toro, M.D.; Guio, L.; et al. Time trends in the aetiology of prosthetic joint infections: A multicentre cohort study. Clin. Microbiol. Infect. 2016, 22, 732. [Google Scholar] [CrossRef] [Green Version]
- Peel, T.N.; Cheng, A.C.; Buising, K.L.; Choong, P.F.M. Microbiological aetiology, epidemiology, and clinical profile of prosthetic joint infections: Are current antibiotic prophylaxis guidelines effective? Antimicrob. Agents Chemother. 2012, 56, 2386–2391. [Google Scholar] [CrossRef] [Green Version]
- Siljander, M.P.; Sobh, A.H.; Baker, K.C.; Baker, E.A.; Kaplan, L.M. Multidrug-Resistant Organisms in the Setting of Periprosthetic Joint Infection—Diagnosis, Prevention, and Treatment. J. Arthroplast. 2018, 33, 185–194. [Google Scholar] [CrossRef]
- Berríos-Torres, S.I.; Yi, S.H.; Bratzler, D.W.; Ma, A.; Mu, Y.; Zhu, L.; Jernigan, J.A. Activity of commonly used antimicrobial prophylaxis regimens against pathogens causing coronary artery bypass graft and arthroplasty surgical site infections in the United States, 2006–2009. Infect. Control. Hosp. Epidemiol. 2014, 35, 231–239. [Google Scholar] [CrossRef]
- Sewick, A.; Makani, A.; Wu, C.; O’Donnell, J.; Baldwin, K.D.; Lee, G.-C. Does dual antibiotic prophylaxis better prevent surgical site infections in total joint arthroplasty? Clin. Orthop. Relat. Res. 2012, 470, 2702–2707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tornero, E.; García-Ramiro, S.; Martínez-Pastor, J.C.; Bori, G.; Bosch, J.; Morata, L.; Sala, M.; Basora, M.; Mensa, J.; Soriano, A. Prophylaxis with Teicoplanin and Cefuroxime Reduces the Rate of Prosthetic Joint Infection after Primary Arthroplasty. Antimicrob. Agents Chemother. 2015, 59, 831–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtney, P.M.; Melnic, C.M.; Zimmer, Z.; Anari, J.; Lee, G.-C. Addition of Vancomycin to Cefazolin Prophylaxis Is Associated with Acute Kidney Injury After Primary Joint Arthroplasty. Clin. Orthop. Relat. Res. 2015, 473, 2197–2203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosco, J.A.; Tejada, P.R.R.; Catanzano, A.J.; Stachel, A.G.; Phillips, M.S. Expanded Gram-Negative Antimicrobial Prophylaxis Reduces Surgical Site Infections in Hip Arthroplasty. J. Arthroplast. 2016, 31, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Tucker, A.; Hegarty, P.; Magill, P.J.; Blaney, J.; Armstrong, L.V.; McCaffrey, J.E.; Beverland, D.E. Acute Kidney Injury After Prophylactic Cefuroxime and Gentamicin in Patients Undergoing Primary Hip and Knee Arthroplasty—A Propensity Score–Matched Study. J. Arthroplast. 2018, 33, 3009–3015. [Google Scholar] [CrossRef] [PubMed]
- Barbero-Allende, J.M.; García-Sánchez, M.; Montero-Ruiz, E.; Vallés-Purroy, A.; Plasencia-Arriba, M.Á.; Sanz-Moreno, J. Dual prophylaxis with teicoplanin and cefazolin in the prevention of prosthetic joint infection. Enferm. Infecc. Microbiol. Clin. 2019, 37, 588–591. [Google Scholar] [CrossRef]
- Parvizi, J.; Ghazavi, M. Committee of the Consensus Meeting M of PA. Optimal Timing and Antibiotic Prophylaxis in Periprosthetic Joint Infection (PJI): Literature Review and World Consensus (Part Three). Shafa Orthop. J. 2015, 2, e2355. [Google Scholar]
- Yusuf, E.; Croughs, P. Vancomycin prophylaxis in prosthetic joint surgery? Clin. Microbiol. Infect. 2020, 26, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Rybak, M.; Lomaestro, B.; Rotschafer, J.C.; Moellering, R.; Craig, W.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am. J. Heal. Pharm. 2009, 66, 82–98. [Google Scholar] [CrossRef]
- Ulldemolins, M.; Roberts, J.A.; Rello, J.; Paterson, D.L.; Lipman, J. The effects of hypoalbuminaemia on optimizing antibacterial dosing in critically ill patients. Clin. Pharmacokinet. 2011, 50, 99–110. [Google Scholar] [CrossRef]
- Bailey, D.N.; Briggs, J.R. Gentamicin and Tobramycin Binding to Human Serum in Vitro. J. Anal. Toxicol. 2004, 28, 187–189. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 9.0. 2019. Available online: http://www.eucast.org. (accessed on 23 December 2020).
- National Committee for Clinical and Laboratory Standards. Methodology for the Serum Bactericidal Test.; Approved Guideline; NCCLS document M21-A: Wayne, PA, USA, 1999.
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R. Model-building strategies and methods for logistic regression. In Applied Logistic Regression; Hosmer, D.W., Lemeshow, S., Sturdivant, R., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; pp. 89–152. [Google Scholar]
- Siddiqi, A.; Forte, S.A.; Docter, S.; Bryant, D.; Sheth, N.P.; Chen, A.F. Perioperative antibiotic prophylaxis in total joint arthroplasty. J. Bone Jt. Surg. 2019, 101, 828–842. [Google Scholar] [CrossRef] [PubMed]
- Babu, S.; Al-Obaidi, B.; Jardine, A.; Jonas, S.; Al-Hadithy, N.; Satish, V. A comparative study of 5 different antibiotic prophylaxis regimes in 4500 total knee replacements. J. Clin. Orthop. Trauma 2020, 11, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Wyles, C.C.; Hevesi, M.; Osmon, D.R.; Park, M.A.; Habermann, E.B.; Lewallen, D.G.; Berry, D.J.; Sierra, R.J. 2019 John Charnley Award: Increased risk of prosthetic joint infection following primary total knee and hip arthroplasty with the use of alternative antibiotics to cefazolin: The value of allergy testing for antibiotic prophylaxis. Bone Jt. J. 2019, 101-B, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Bitkover, C.Y.; Marcusson, E.; Ransjö, U. Spread of coagulase-negative staphylococci during cardiac operations in a modern operating room. Ann. Thorac. Surg. 2000, 69, 1110–1115. [Google Scholar] [CrossRef]
- Parvizi, J.; Barnes, S.; Shohat, N.; Edmiston, C.E. Environment of care: Is it time to reassess microbial contamination of the operating room air as a risk factor for surgical site infection in total joint arthroplasty? Am. J. Infect. Control. 2017, 45, 1267–1272. [Google Scholar] [CrossRef]
- Wildeman, P.; Tevell, S.; Eriksson, C.; Lagos, A.C.; Söderquist, B.; Stenmark, B. Genomic characterization and outcome of prosthetic joint infections caused by Staphylococcus aureus. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Font-Vizcarra, L.; Tornero, E.; Bori, G.; Bosch, J.; Mensa, J.; Soriano, A. Relationship between intraoperative cultures during hip arthroplasty, obesity, and the risk of early prosthetic joint infection: A prospective study of 428 patients. Int. J. Artif. Organs 2011, 34, 870–875. [Google Scholar] [CrossRef]
- Frank, C.B.; Adams, M.; Kroeber, M.; Wentzensen, A.; Heppert, V.; Schulte-Bockholt, D.; Guehring, T. Intraoperative subcutaneous wound closing culture sample: A predicting factor for periprosthetic infection after hip- and knee-replacement? Arch. Orthop. Trauma Surg. 2011, 131, 1389–1396. [Google Scholar] [CrossRef]
- Haenle, M.; Podbielski, A.; Ellenrieder, M.; Mundt, A.; Krentz, H.; Mittelmeier, W.; Skripitz, R. Bacteriology swabs in primary total knee arthroplasty. GMS Hyg. Infect. Control. 2013, 8. [Google Scholar] [CrossRef]
- Jonsson, E.Ö.; Johannesdottir, H.; Robertsson, O.; Mogensen, B. Bacterial contamination of the wound during primary total hip and knee replacement. Median 13 years of follow-up of 90 replacements. Acta Orthop. 2014, 85, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knobben, B.A.S.; Engelsma, Y.; Neut, D.; Van Der Mei, H.C.; Busscher, H.J.; Van Horn, J.R. Intraoperative contamination influences wound discharge and periprosthetic infection. Clin. Orthop. Relat. Res. 2006, 452, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.K.; Higuera, C.; Deirmengian, G.; Parvizi, J.; Austin, M.S. Swab cultures are not as effective as tissue cultures for diagnosis of periprosthetic joint infection. Clin. Orthop. Relat. Res. 2013, 471, 3196–3203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benito, N.; Mur, I.; Ribera, A.; Soriano, A.; Rodriguez-Pardo, D.; Sorli, L.; Cobo, J.; Fernandez-Sampedro, M.; del Toro, M.D.; Guio, L.; et al. The Different Microbial Etiology of Prosthetic Joint Infections according to Route of Acquisition and Time after Prosthesis Implantation, Including the Role of Multidrug-Resistant Organisms. J. Clin. Med. 2019, 8, 673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheidt, S.; Walter, S.; Randau, T.M.; Köpf, U.S.; Jordan, M.C.; Hischebeth, G.T.R. The Influence of Iodine-Impregnated Incision Drapes on the Bacterial Contamination of Scalpel Blades in Joint Arthroplasty. J. Arthroplast. 2020, 35, 2595–2600. [Google Scholar] [CrossRef]
- Alverdy, J.C.; Hyman, N.; Gilbert, J. Re-examining causes of surgical site infections following elective surgery in the era of asepsis. Lancet Infect. Dis. 2020, 20, e38–e43. [Google Scholar] [CrossRef]
- Stratton, C.W. The usefulness of the serum bactericidal test in orthopedic infections. Orthopedics 1984, 7, 1579–1580. [Google Scholar]
- Harley, W.B.; Stratton, C.W. The serum bactericidal test revisited. Infect. Dis. Newsl. 1993, 12, 61–64. [Google Scholar] [CrossRef]
- Gaibani, P.; Lombardo, D.; Bartoletti, M.; Ambretti, S.; Campoli, C.; Giannella, M.; Tedeschi, S.; Conti, M.; Mancini, R.; Landini, M.P.; et al. Comparative serum bactericidal activity of meropenem-based combination regimens against extended-spectrum beta-lactamase and KPC-producing Klebsiella pneumoniae. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1925–1931. [Google Scholar] [CrossRef]
- Spaziante, M.; Franchi, C.; Taliani, G.; d’Avolio, A.; Pietropaolo, V.; Biliotti, E.; Esvan, R.; Venditti, M. Serum bactericidal activity levels monitor to guide intravenous dalbavancin chronic suppressive therapy of inoperable staphylococcal prosthetic valve endocarditis: A case report. Open. Forum Infect. Dis. 2019, 6, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Zaghi, I.; Gaibani, P.; Campoli, C.; Bartoletti, M.; Giannella, M.; Ambretti, S.; Viale, P.; Lewis, R.E. Serum bactericidal titres for monitoring antimicrobial therapy: Current status and potential role in the management of multidrug-resistant Gram-negative infections. Clin. Microbiol. Infect. 2020, 26, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Ravi, S.; Zhu, M.; Luey, C.; Young, S.W. Antibiotic resistance in early periprosthetic joint infection. ANZ J. Surg. 2016, 86, 1014–1018. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Intraoperative Cultures | p-Value | Multivariate Analysis | p-Value | |
|---|---|---|---|---|---|
| Positive (n = 57) | Negative (n = 75) | OR (CI 95%) | |||
| Sex—number of males or females with positive cultures/total number of males or females, respectively (%) | 0.023 | 2.412 (1.170–4.973) | 0.017 | ||
| 31/57 (54.4) | ||||
| 26/75 (37.7) | ||||
| Age, years—mean (SD) | 71 (9.6) | 72 (7.9) | 0.615 | ||
| BMI—mean (SD) | 29.9 (5.1) | 29.1 (4.9) | 0.393 | ||
| Antimicrobial prophylaxis—number of culture-positive patients with each type of prophylaxis/total of patients receiving each type of prophylaxis (%) | |||||
| 9/22 (40.9) 13/20 (65) 6/11 (54.5) | 0.293 | |||
| 9/22 (40.9) 14/39 (35.9) | 0.698 | |||
| 13/20 (65) 9/20 (45) | 0.204 | |||
| 6/11 (54.5) 6/20 (30) | 0.180 | |||
| 29/79 (36.7) 28/53 (52.8) | 0.067 | 0.475 (0.229–0.987) | 0.046 | |
Prosthesis location—number of patients with a hip or knee prosthesis and positive cultures/total number of patients with hip or knee prostheses, respectively (%)
| 30/64 (46.9) 27/68 (39.7) | 0.406 | |||
| Surgery duration, minutes—mean (SD) | 75 (18.8) | 78 (20.2) | 0.363 | ||
| Bacterial Species | Surgical Procedures (n = 57) | THA (n = 30) | TKA (n = 27) | p-Value * |
|---|---|---|---|---|
| Cutibacterium species—n (%) | 34 (59.6) | 22 (73.3) | 12 (44.4) | 0.026 |
| 33 | 21 | 12 | 0.051 |
| 1 | 1 | 0 | |
| Coagulase-negative staphylococci—n (%) | 30 (52.6) | 15 (50) | 15 (55.6) | 0.675 |
| 19 (33.3) | 8 (26.7) | 11 (40.7) | 0.399 |
| 12 (21.1) | 8 (26.7) | 4 (14.8) | 0.441 |
| 3 2 1 1 1 1 1 | 1 2 1 1 0 0 1 | 2 0 0 0 1 1 0 | |
| Micrococcus luteus—n (%) | 8 (14.0) | 4 (13.3) | 4 (14.8) | |
| Corynebacterium species—n (%) | 4 (7.0) | 3 | 1 | |
| 1 1 1 1 1 1 | 0 1 1 1 1 0 | 1 0 0 0 0 1 | |
| Paenibacillus lautus | 1 | 1 | 0 | |
| Actinomyces neuii | 1 | 1 | 0 | |
| Dermabacter hominis | 1 | 0 | 1 | |
| Kocuria rhizophila | 1 | 1 | 0 |
| Antimicrobial Used as Prophylaxis | Free Plasma Concentration (mg/L), Median (Range) | Free Plasma Concentration (mg/L)/ MIC (mg/L), Median (Range) |
|---|---|---|
| Cefazolin | 17.3 (11.2–33.2) | 44.4 (0.3–1037.5) |
| Cefuroxime | 24.2 (11–44.2) | 81.6 (1.1–1833.5) |
| Gentamicin | 12.3 (8.5–19.4) | 9.01(0.6–323.4) |
| Vancomycin | 7.8 (4.6–19.05) | 25.6(3.5–152.4) |
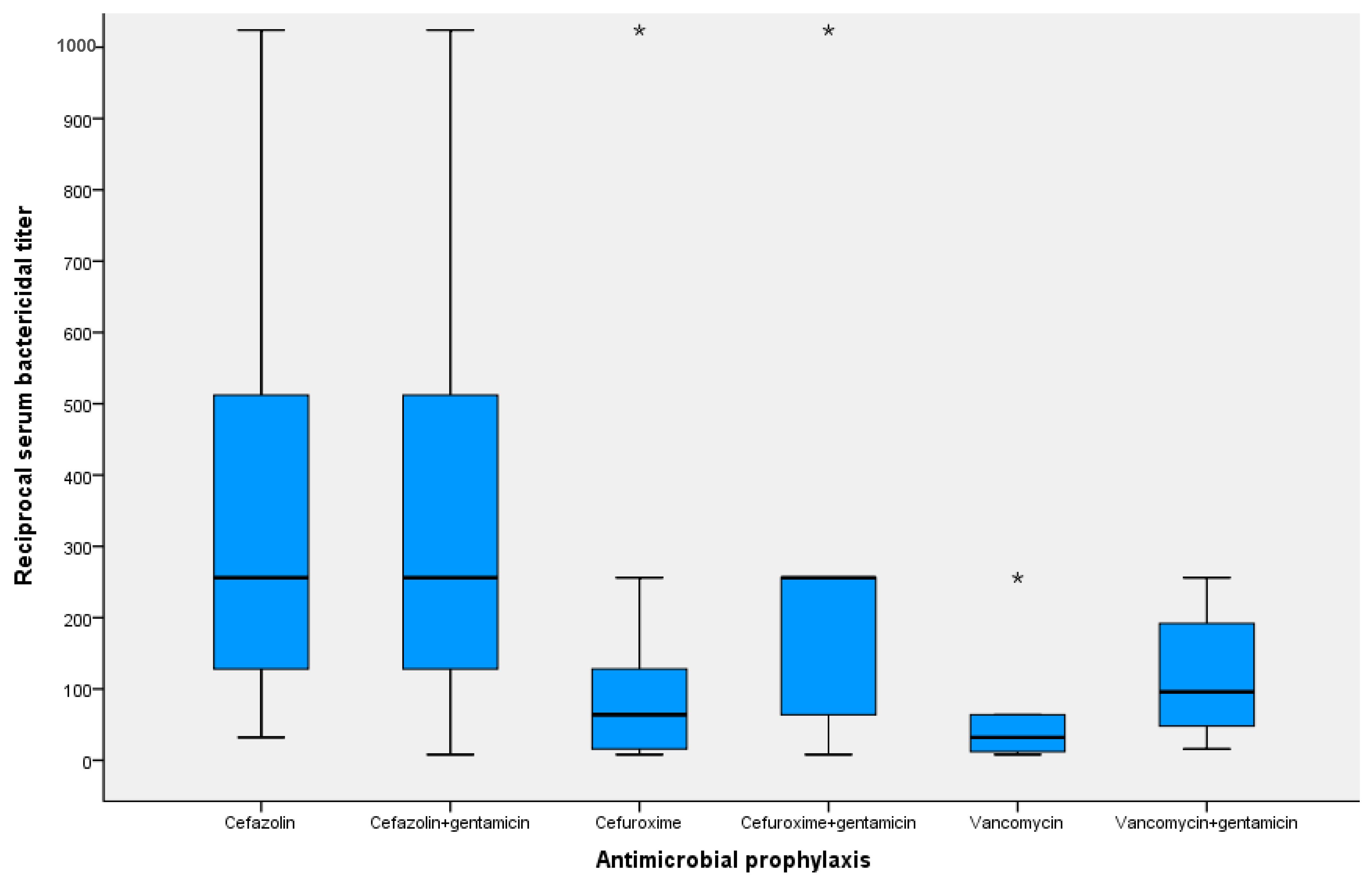
| Antimicrobial Prophylaxis | Reciprocal Serum Bactericidal Titer—Median (Range) | ||||
|---|---|---|---|---|---|
| Isolates from the Surgical Field | Staphylococcus epidermidis ATCC 12228 | Staphylococcus aureus ATCC 25923 | Escherichia coli ATCC 25922 | Pseudomonas aeruginosa ATCC 27853 | |
| Cefazolin | 256 (32–1024) | 256 (32–512) | 256 (64–1024) | 64 (16–256) | <2 (<2) |
| Cefazolin+Gentamicin | 256 (8–1024) | 512 (32–1024) | 256 (32–1024) | 64 (16–256) | 8 (<2–16) |
| Cefuroxime | 64 (8–1024) | 64 (16–512) | 32 (8–64) | 8 (2–32) | <2 (<2) |
| Cefuroxime+Gentamicin | 256 (8–1024) | 256 (64–512) | 128 (8–128) | 32 (16–32) | 4 (<2–4) |
| Vancomycin | 32 (8–256) | 12 (8–32) | 12 (8–16) | <2 (<2–2) | <2 (<2) |
| Vancomycin+Gentamicin | 64 (16–256) | 256 (256–512) | 128 (32–256) | 32 (16–64) | 4 (4–8) |
| Antimicrobial (n) | Free Plasma Concentration (mg/L), Median (Range) | MIC (mg/L) | |||
|---|---|---|---|---|---|
| Staphylococcus epidermidis ATCC 12228 | Staphylococcus aureus ATCC 25923 | Escherichia coli ATCC 25922 | Pseudomonas aeruginosa ATCC 27853 | ||
| Cefazolin (56) | 17.3 (6.5–35.4) | 0.5 | 0.5 | 3 | >256 |
| Cefuroxime (21) | 25.7 (11–44.2) | 0.75 | 0.5 | 6 | >256 |
| Gentamicin (54) | 12.55 (8.5–19.4) | 0.125 | 0.38 | 0.75 | 1.5 |
| Vancomycin (16) | 7.65 (4.6–19.05) | 1.5 | 1 | >256 | >256 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera, A.; Sánchez, A.; Luque, S.; Mur, I.; Puig, L.; Crusi, X.; González, J.C.; Sorlí, L.; González, A.; Horcajada, J.P.; et al. Intraoperative Bacterial Contamination and Activity of Different Antimicrobial Prophylaxis Regimens in Primary Knee and Hip Replacement. Antibiotics 2021, 10, 18. https://doi.org/10.3390/antibiotics10010018
Rivera A, Sánchez A, Luque S, Mur I, Puig L, Crusi X, González JC, Sorlí L, González A, Horcajada JP, et al. Intraoperative Bacterial Contamination and Activity of Different Antimicrobial Prophylaxis Regimens in Primary Knee and Hip Replacement. Antibiotics. 2021; 10(1):18. https://doi.org/10.3390/antibiotics10010018
Chicago/Turabian StyleRivera, Alba, Alba Sánchez, Sonia Luque, Isabel Mur, Lluís Puig, Xavier Crusi, José Carlos González, Luisa Sorlí, Aránzazu González, Juan Pablo Horcajada, and et al. 2021. "Intraoperative Bacterial Contamination and Activity of Different Antimicrobial Prophylaxis Regimens in Primary Knee and Hip Replacement" Antibiotics 10, no. 1: 18. https://doi.org/10.3390/antibiotics10010018
APA StyleRivera, A., Sánchez, A., Luque, S., Mur, I., Puig, L., Crusi, X., González, J. C., Sorlí, L., González, A., Horcajada, J. P., Navarro, F., & Benito, N. (2021). Intraoperative Bacterial Contamination and Activity of Different Antimicrobial Prophylaxis Regimens in Primary Knee and Hip Replacement. Antibiotics, 10(1), 18. https://doi.org/10.3390/antibiotics10010018