
Predictor of Early Administration of Antibiotics and a Volume Resuscitation for Young Infants with Septic Shock

 , ,
, ,
Abstract
:1. Introduction
2. Results
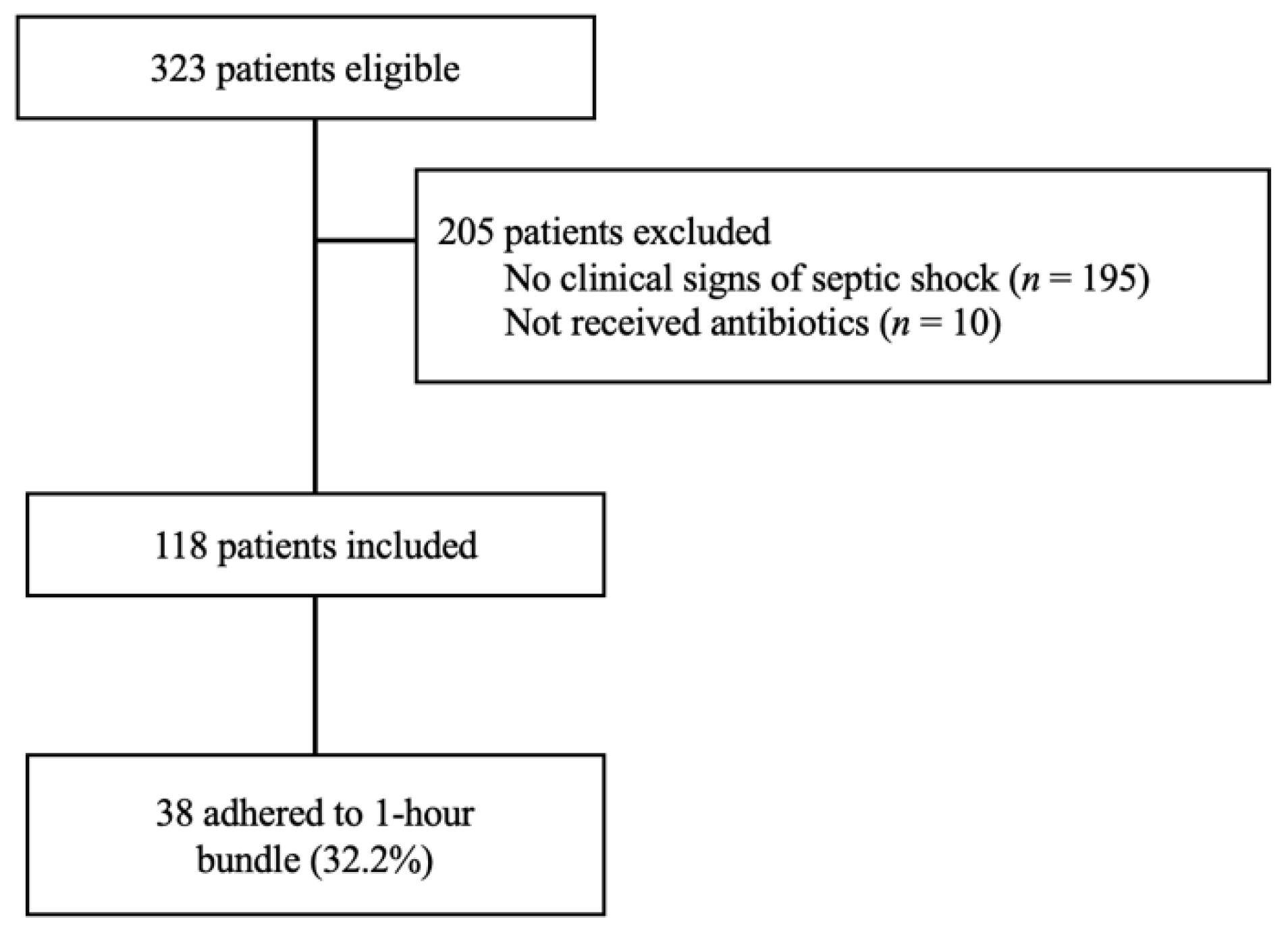
2.1. Demographics
2.2. Comparison between the Patient Group with Bundle Completion and without Bundle Completion
2.3. Predictor (s) of the 1 h Bundle Completion
3. Discussion
4. Materials and Methods
4.1. Study Design and Setting
4.2. Participants
4.3. Data Collection
4.4. Statistical Analysis
4.5. Ethics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pantell, R.H.; Roberts, K.B.; Adams, W.G.; Dreyer, B.P.; Kuppermann, N.; O’Leary, S.T.; Okechukwu, K.; Woods, C.R. Evaluation and management of well-appearing febrile infants 8 to 60 days old. Pediatrics 2021, 148, e2021052228. [Google Scholar] [CrossRef] [PubMed]
- Bonadio, W.A.; Hagen, E.; Rucka, J.; Shallow, K.; Stommel, P.; Smith, U. Efficacy of a protocol to distinguish risk of serious bacterial infection in the outpatient evaluation of febrile young infants. Clin. Pediatr. 1993, 32, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Baskin, M.N.; Fleisher, G.R.; O’Rourke, E.J. Identifying febrile infants at risk for a serious bacterial infection. J. Pediatr. 1993, 123, 489–490. [Google Scholar] [CrossRef]
- Baraff, L.J.; Bass, J.W.; Fleisher, G.R.; Klei, J.O.; McCracken, G.H.; Powell, K.R.; Schriger, D.L. Practice guideline for the management of infants and children 0 to 36 months of age with fever without source. Pediatrics 1993, 92, 1–12. [Google Scholar] [CrossRef]
- Ramgopal, S.; Horvat, C.M.; Yanamala, N.; Alpern, E.R. Machine learning to predict serious bacterial infections in young febrile infants. Pediatrics 2020, 146, e20194096. [Google Scholar] [CrossRef] [PubMed]
- Chiu, I.M.; Cheng, C.Y.; Zeng, W.H.; Huang, Y.H.; Lin, C.H.R. Using machine learning to predict invasive bacterial infections in young febrile infants visiting the emergency department. J. Clin. Med. 2021, 10, 1875. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.-M.; Lin, C.-H.R.; Zhang, H.; Chiu, I.-M.; Cheng, C.-Y.; Yu, H.-R.; Huang, Y.-H. Using machine learning to predict bacteremia in febrile children presented to the emergency department. Diagnostics 2020, 10, 307. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.L.; Peters, M.J.; Alhazzani, W.; Agus, M.S.D.; Flori, H.R.; Inwald, D.P.; Nadel, S.; Schlapbach, L.J.; Tasker, R.C.; Argent, A.C.; et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Pediatr. Crit. Care Med. 2020, 21, e52–e106. [Google Scholar] [CrossRef] [PubMed]
- Evans, I.V.R.; Phillips, G.S.; Alpern, E.R.; Angus, D.C.; Friedrich, M.E.; Kissoon, N.; Lemeshow, S.; Levy, M.M.; Parker, M.M.; Terry, K.N. Association between the New York sepsis care mandate and in-hospital mortality for pediatric sepsis. JAMA 2018, 320, 358–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lane, R.D.; Funai, T.; Reeder, R.; Larsen, G.Y. High reliability pediatric septic shock quality improvement initiative and decreasing mortality. Pediatrics 2016, 138, e20154153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, Y.; Sankar, J.; Dhochak, N.; Gupta, S.; Lodha, R.; Kabra, S.K. Decreasing the time to administration of first dose of antibiotics in children with severe sepsis. J. Healthc. Qual. 2019, 41, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Sankar, J.; Garg, M.; Ghimire, J.J.; Sankar, M.J.; Lodha, R.; Kabra, S.K. Delayed administration of antibiotics beyond the first hour of recognition is associated with increased mortality rates in children with sepsis/severe sepsis and septic shock. J. Pediatr. 2021, 233, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Balamuth, F.; Alpern, E.R.; Abbadessa, M.K.; Hayes, K.; Schast, A.; Lavelle, J.; Fitzgerals, J.C.; Weiss, S.L.; Zorc, J.J. Improving recognition of pediatric severe sepsis in the emergency department: Contributions of a vital sign–based electronic alert and bedside clinician identification. Ann. Emerg. Med. 2017, 70, 759–768. [Google Scholar] [CrossRef] [PubMed]
- Nomura, O.; Morikawa, Y.; Mori, T.; Hagiwara, Y.; Sakakibara, S.; Horikoshi, Y.; Inoie, N. Limited utility of SIRS criteria in septic young infants. Children 2021, 8, 1003. [Google Scholar] [CrossRef]
- Hayakawa, I.; Nomura, O.; Uda, K.; Funakoshi, Y.; Sakakibara, H.; Horikoshi, Y. Incidence and aetiology of serious viral infections in young febrile infants. J. Paediatr. Child Health 2019, 56, 586–589. [Google Scholar] [CrossRef] [PubMed]
- Nomura, O.; Ihara, T.; Sakakibara, H.; Horikoshi, Y.; Inoue, N. Predicting serious bacterial infection in febrile young infants utilizing body temperature. Pediatr. Int. 2019, 61, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, B.; Giroir, B.; Randolph, A. International consensus conference on pediatric sepsis international pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr. Crit. Care Med. 2005, 6, 2–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Dellinger, R.P.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock, 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Lane, R.D.; Olson, J.; Reeder, R.; Miller, B.; Workman, J.K.; Thorell, E.A.; Larsen, G.Y. Antibiotic timing in pediatric septic shock. Hosp. Pediatr. 2020, 10, 311–317. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | |
|---|---|
| Demographics | |
| Age, median (IQR), Days | 37.0 (21–65) |
| Wt, median (IQR), kg | 4.3 (3.6–5.3) |
| Male, % (n) | 53.4 (63) |
| Vital signs | |
| Core body temperature, median (IQR), °C | 38.6 (38.3–38.9) |
| Heart rate, median (IQR), beats per minute | 178.0 (164.0–192.2) |
| Respiratory rate, median (IQR), breaths per minute | 38.5 (31.0–47.3) |
| Pulse oximetry, median (IQR), % | 99 (97–100) |
| Glasgow Coma Scale lower than 15, % (n) | 16.1 (19) |
| Physical examinations | |
| Cool extremities, % (n) | 71.2 (84) |
| Prolonged Capillary Refilling Time, % (n) | 50.0 (59) |
| Hypotension, % (n) | 8.5 (10) |
| Laboratory examinations | |
| WBC count, median (IQR), ×103 | 9.0 (6.5–12.6) |
| Neutrophils, median (IQR), % | 48.8 (34.1–62.1) |
| Lactate, median (IQR), mmol/L | 2.6 (1.9–3.3) |
| CRP, median (IQR), mmol/L | 0.5 (0.2–1.3) |
| Platelet count, median (IQR), ×103 | 38.6 (28.6–48.6) |
| Bilirubin, median (IQR), mg/dl | 3.5 (1.8–10.1) |
| Creatinine, median (IQR), mg/dl | 0.24 (0.21–0.27) |
| Clinical diagnosis | |
| Serious bacterial infections, % (n) | 11.9 (14) |
| Serious viral infections, % (n) | 24.6 (29) |
| Pediatric SOFA score, median (IQR) | 2 (1–3) |
| Treatment | |
| Hospitalization inwards, % (n) | 93.2 (110) |
| Intensive care unit admission, % (n) | 6.8 (8) |
| Day of stay, median (IQR), days | 6.0 (5.0–7.0) |
| Bundle completions, % (n) | 32.2 (38) |
| Total-infusion amount, median (IQR), mL/kg | 19.8 (9.8–37.6) |
| Variables | Bundle Completion (n = 38) | Bundle Incompletion (n = 80) | p-Value |
|---|---|---|---|
| Demographics | |||
| Bodyweight, median (IQR), kg | 4.8 (3.7–5.3) | 4.2 (3.5–5.3) | 0.48 |
| Age, median (IQR), days | 40.0 (28.3–60.3) | 31.0 (20.0–65.8) | 0.24 |
| Male, % (n) | 65.8 (25) | 48.8 (39) | 0.11 |
| Vital signs | |||
| Core body temperature, median (IQR), °C | 38.9 (38.4–39.0) | 38.5 (38.2–38.9) | 0.05 |
| Heart rate, median (IQR), beats per minute | 187.5 (169.0–198.5) | 173.0 (158.0–188.8) | <0.01 |
| Respiratory rate, median (IQR), breaths per minute | 39.0 (29.8–51.0) | 38.5 (32.0–45.8) | 0.72 |
| Pulse oximetry, median (IQR), % | 99.0 (97.8–100) | 99.0 (97.0–100) | 0.26 |
| Physical examinations | |||
| Cool extremities, % (n) | 31 (81.6) | 53 (66.3) | 0.13 |
| Prolonged Capillary Refilling Time, % (n) | 28 (73.7) | 31 (38.8) | <0.01 |
| Hypotension, % (n) | 3 (7.9) | 7 (8.8) | 1.00 |
| Glasgow Coma Scale lower than 15, % (n) | 23.7 (9) | 12.5 (10) | 0.18 |
| Laboratory examinations | |||
| WBC count, median (IQR), ×103 | 6.9 (5.5–10.2) | 9.9 (7.5–13.6) | <0.01 |
| Neutrophils, median (IQR), % | 46.1(30.6–59.2) | 50.4 (35.5–62.4) | 0.29 |
| Lactate, median (IQR), mmol/L | 2.4 (1.9–3.1) | 2.7 (1.9–3.4) | 0.36 |
| CRP, median (IQR), mg/dl | 0.5 (0.2–1.1) | 0.5 (0.2–1.6) | 0.86 |
| Platelet count, median (IQR), ×103 | 35.8 (27.5–47.8) | 39.5 (30.2–51.0) | 0.47 |
| Bilirubin, median (IQR), mg/dl | 2.8 (1.5–7.2) | 3.8 (1.1–10.7) | 0.92 |
| Creatinine, median (IQR), mg/dl | 0.24 (0.20–0.26) | 0.24 (0.21–0.27) | 0.57 |
| Clinical diagnosis | |||
| pSOFA score, median (IQR) | 2 (1–3) | 2 (0–3) | 0.71 |
| Serious bacterial infections, % (n) | 13.2 (5) | 11.3 (9) | 0.77 |
| Serious viral infections, % (n) | 31.6 (12) | 21.3 (17) | 0.26 |
| Treatment | |||
| Intensive care unit admission, % (n) | 13.2 (5) | 3.8 (2) | 0.11 |
| Total-infusion amount, median (IQR), mL/kg | 49.5 (33.2–57.0) | 11.2 (7.6–20.2) | <0.01 |
| Length of stay, median (IQR), days | 5.5 (5.0–8.3) | 6.0 (5.0–6.0) | 0.61 |
| Characteristics | Odds Ratio | 95% CI | p |
|---|---|---|---|
| Heart rate | 1.02 | 1.00–1.04 | 0.04 |
| Male sex | 2.00 | 0.87–4.60 | 0.11 |
| Age | 1.00 | 0.99–1.02 | 0.68 |
| Respiratory rate | 1.00 | 0.96–1.03 | 0.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomura, O.; Ihara, T.; Morikawa, Y.; Sakakibara, H.; Horikoshi, Y.; Inoue, N. Predictor of Early Administration of Antibiotics and a Volume Resuscitation for Young Infants with Septic Shock. Antibiotics 2021, 10, 1414. https://doi.org/10.3390/antibiotics10111414
Nomura O, Ihara T, Morikawa Y, Sakakibara H, Horikoshi Y, Inoue N. Predictor of Early Administration of Antibiotics and a Volume Resuscitation for Young Infants with Septic Shock. Antibiotics. 2021; 10(11):1414. https://doi.org/10.3390/antibiotics10111414
Chicago/Turabian StyleNomura, Osamu, Takateru Ihara, Yoshihiko Morikawa, Hiroshi Sakakibara, Yuho Horikoshi, and Nobuaki Inoue. 2021. "Predictor of Early Administration of Antibiotics and a Volume Resuscitation for Young Infants with Septic Shock" Antibiotics 10, no. 11: 1414. https://doi.org/10.3390/antibiotics10111414
APA StyleNomura, O., Ihara, T., Morikawa, Y., Sakakibara, H., Horikoshi, Y., & Inoue, N. (2021). Predictor of Early Administration of Antibiotics and a Volume Resuscitation for Young Infants with Septic Shock. Antibiotics, 10(11), 1414. https://doi.org/10.3390/antibiotics10111414