
Outcomes and Risk Factors in Prosthetic Joint Infections by multidrug-resistant Gram-negative Bacteria: A Retrospective Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions
2.3. Investigated Variables
2.4. Microbiological Analysis
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Microbial Identification
3.3. Potential Predisposing Factors for PJI Caused by MDR-GNB and Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Presence of a major criteria |
| 1. Sinus tract with evidence of communication of the joint or visualization of the prosthesis |
| or |
| 2. Identification of the same phenotypically similar pathogen in two or more different periprosthetic tissue samples or in joint fluid |
| Presence of four or more minor criteria |
| 1. Presence of purulent periprosthetic secretion |
| 2. Identification of acute inflammatory reaction in histopathologic tests of periprosthetic tissue |
| 3. A single culture with the identification of a microorganism |
| 4. High leukocyte cellularity in the synovial fluid |
| 5. High percentage of neutrophils in the synovial fluid |
| 6. Increased serum levels of C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) |
Appendix B

{kind=link}
{kind=link}
| Variables | PJI a | ||
|---|---|---|---|
| MDR/XDR GNB b | Other Bacteria | p-Value c | |
| No. (%) | No. (%) | ||
| N = 56 | N = 42 | ||
| Demographic data | |||
| Males | 29 (70.7) | 12 (29.3) | 0.021 * |
| Females | 27 (47.4) | 30 (52.6) | |
| Age (years) | F | ||
| Mean ± Standard deviation | 68.2 ± 13.8 | 66.0 ± 1.4 | 0.415 *** |
| Age group | |||
| up to 50 | 7 (70.0) | 3 (30.0) | 0.126 ** |
| 51–60 years | 13 (56.5) | 10 (43.5) | |
| 61–70 years | 7 (35.0) | 13 (65.0) | |
| 71–80 years | 18 (58.1) | 13 (41.9) | |
| above 80 years | 11 (78.6) | 3 (21.4) | |
| Variables related to the patient | |||
| Presence of comorbidities | 41 (73.2) | 30 (71.4) | 0.845 * |
| SAH d | 33 (58.9) | 27 (64.3) | 0.590 * |
| DM e | 12 (21.4) | 8 (19.0) | 0.772 * |
| Malnutrition | 7 (12.5) | 1 (2.4) | 0.133 ** |
| Anemia | 2 (3.6) | 0 (0) | 0.505 ** |
| Neoplasm | 0 (0) | 1 (2.4) | 0.429 ** |
| Lung disease | 0 (0) | 5 (9) | 0.013 ** |
| Metabolic syndrome | 6 (10.7) | 12 (28.6) | 0.024 * |
| Cardiovascular disease | 4 (7.1) | 1 (2.4) | 0.388 ** |
| Other comorbidities f | 4 (7.1) | 7 (16.7) | 0.197 ** |
| Alcoholism | 12 (21.4) | 2 (4.8) | 0.020 * |
| Smoking | 9 (16.1) | 4 (9.5) | 0.344 * |
| ASA classification g | |||
| 1 | 8 (14.3) | 13 (31.0) | 0.114 * |
| 2 | 28 (50.0) | 19 (45.2) | |
| 3 or 4 | 20 (35.7) | 10 (23.8) | |
| Previous orthopedic infection | 20 (35.7) | 0 (0) | 0.000 * |
| Previous use of antimicrobials (last three months) | |||
| Yes | 31 (55.4) | 6 (14.3) | 0.000 * |
| Quinolones | 12 (21.4) | 3 (7.1) | 0.052 * |
| β-Lactam Antibiotics | 20 (35.7) | 4 (9.5) | 0.003 * |
| Antimicrobial combination | 10 (17.9) | 1 (2.4) | 0.000 ** |
| Variables related to the surgical procedure | |||
| Arthroplasty | |||
| Total | 41 (73.2) | 34 (81.0) | 0.371 * |
| Revision | 66.1 (37) | 11.9 (5) | 0.000 * |
| Non-elective | 31 (55.4) | 8 (19.0) | 0.000 * |
| Hip | 56 (100) | 26 (61.9) | 0.000 * |
| Duration of the procedure > 2.5 h | 8 (14.3) | 7 (16.7) | 0.746 * |
| Blood transfusion | 16 (28.6) | 3 (7.1) | 0.008 * |
| Variables related to the postoperative period | |||
| Concomitant non-orthopedic infection | 11 (19.6) | 2 (4.8) | 0.032 * |
| Previous orthopedic infection | 20 (35.7) | 0 (0) | 0.000 * |
| Polymicrobial infection | 4 (7.1) | 4 (9.5) | 0.721 ** |
| Early infection | 32 (57.1) | 37 (88.1) | 0.001 * |
| Postoperative hematoma | 29 (51.8) | 1 (2.4) | 0.000 * |
| Sepsis associated with infection | 2 (3.6) | 0 (0) | 0.505 ** |
| Variable | PJI by MDR-GNB | Descriptive Measures | p * | ||
|---|---|---|---|---|---|
| Min-Max | Median (P25–P75) | Mean ± SD | |||
| Time elapsed between prosthesis and diagnosis (days) | Yes | 7.0–5.040.0 | 37.0 (20.3–472.5) | 453.1 ± 934.7 | 0.066 |
| No | 7.0–1.825.0 | 30.0 (20.0–39.3) | 95.4 ± 285.4 | ||
| Time to failure (days) | Yes | 1.0–179.0 | 68.0 (37.0–102.3) | 77.1 ± 50.1 | 0.063 |
| No | 34.0–225.0 | 105.0 (72.0–181.0) | 119.1 ± 62.9 | ||
| Variables | Univariate Analysis | Prevalence Ratio 95% CI | p-Value a |
|---|---|---|---|
| PJI b by GNB c | 0.087 | - | - |
| PJI by MDR-GNB d | 1.0 (0.4; 2.5) | 0.991 | |
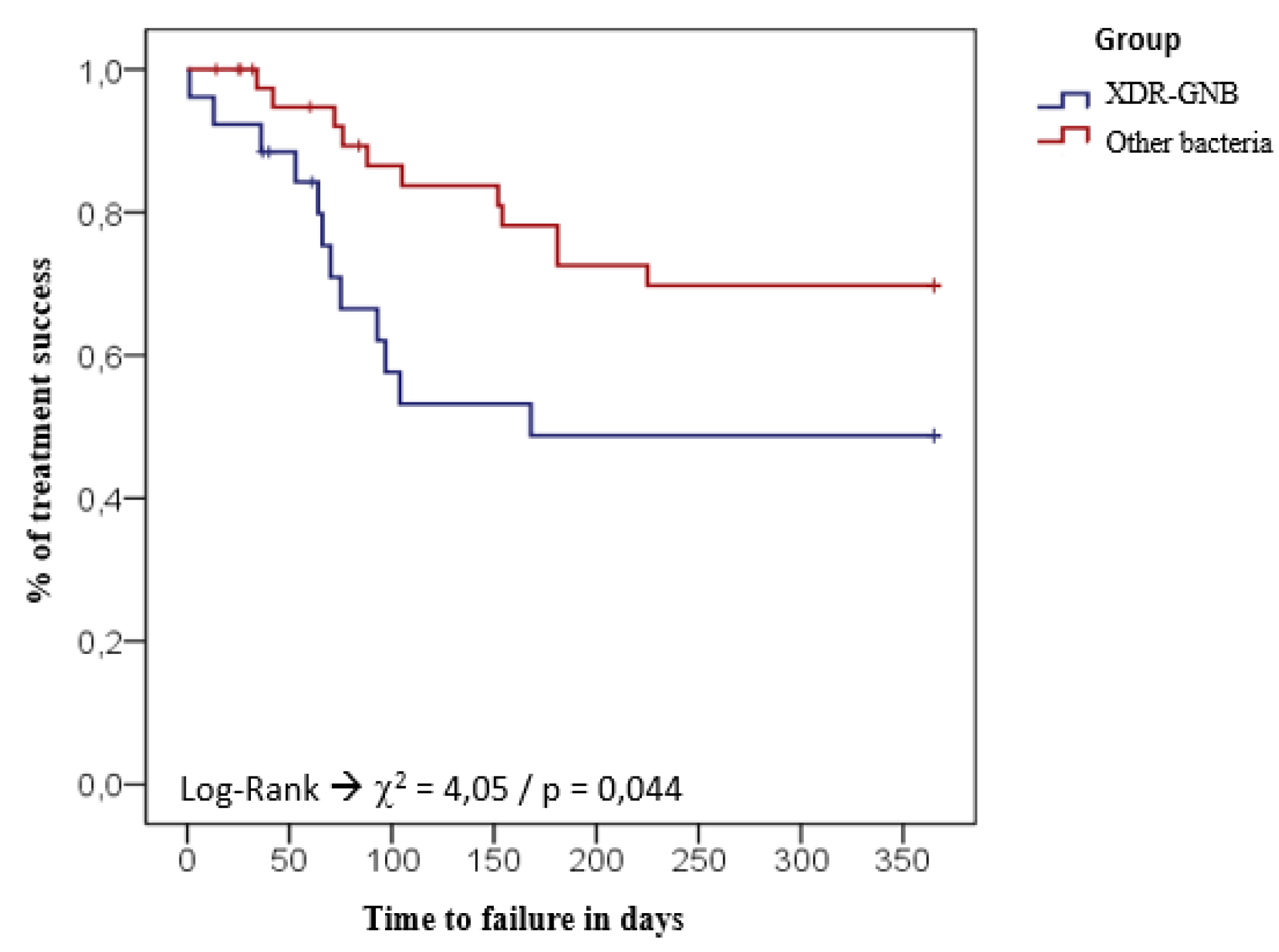
| PJI by XDR-GNB e | 2.3 (1.0; 5.2) | 0.044 | |
| DAIR f surgical strategy | 0.842 | - | - |
| Presence of comorbidities | 0.038 | 2.9 (1.0; 8.4) | 0.044 |
References
- Kozak, L.J.; DeFrances, C.J.; Hall, M.J. National Hospital Discharge Survey: 2004 Annual Summary with Detailed Diagnosis and Procedure Data. Vital. Health Stat. 2006, 13, 1–209. [Google Scholar]
- Corvec, S.; Portillo, M.E.; Pasticci, B.M.; Borens, O.; Trampuz, A. Epidemiology and New Developments in the Diagnosis of Prosthetic Joint Infection. Int. J. Artif. Organs 2012, 35, 923–934. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.L.; Kurtz, S.M.; Lau, E.; Bozic, K.J.; Berry, D.J.; Parvizi, J. Prosthetic Joint Infection Risk After Total Hip Arthroplasty in the Medicare Population. J. Arthroplast. 2009, 24 (Suppl. 6), 105–109. [Google Scholar] [CrossRef]
- Martínez-Pastor, J.C.; Muñoz-Mahamud, E.; Vilchez, F.; García-Ramiro, S.; Bori, G.; Sierra, J.; Martínez, J.A.; Font, L.; Mensa, J.; Soriano, A. Outcome of Acute Prosthetic Joint Infections Due to Gram-Negative Bacilli Treated with Open Debridement and Retention of the Prosthesis. Antimicrob. Agents Chemother. 2009, 53, 4772–4777. [Google Scholar] [CrossRef] [Green Version]
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [Green Version]
- Nagaya, L.H.; Salles, M.J.C.; Takikawa, L.S.C.; Fregoneze, M.; Doneux, P.; Da Silva, L.A.; Sella, G.D.V.; Miyazaki, A.N.; Checchia, S.L. Infections after shoulder arthroplasty are correlated with higher anesthetic risk score: A case-control study in Brazil. Braz. J. Infect. Dis. 2017, 21, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, P.; Lee, M.S.; Hsu, K.; Chang, Y.; Shih, H.; Ueng, S.W. Gram-Negative Prosthetic Joint Infections: Risk Factors and Outcome of Treatment. Clin. Infect. Dis. 2009, 49, 1036–1043. [Google Scholar] [CrossRef]
- Namba, R.S.; Inacio, M.C.; Paxton, E.W. Risk Factors Associated with Deep Surgical Site Infections After Primary Total Knee Arthroplasty: An Analysis of 56,216 Knees. J. Bone Jt. Surg. Am. Vol. 2013, 95, 775–782. [Google Scholar] [CrossRef] [Green Version]
- Malinzak, R.A.; Ritter, M.A.; Berend, M.E.; Meding, J.B.; Olberding, E.M.; Davis, K.E. Morbidly Obese, Diabetic, Younger, and Unilateral Joint Arthroplasty Patients Have Elevated Total Joint Arthroplasty Infection Rates. J. Arthroplast. 2009, 24 (Suppl. 6), 84–88. [Google Scholar] [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [Green Version]
- Pradella, J.G.D.P.; Bovo, M.; Salles, M.J.C.; Klautau, G.B.; De Camargo, O.A.P.; Cury, R.D.P.L. Infected primary knee arthroplasty: Risk factors for surgical treatment failure. Rev. Bras. Ortop. 2013, 48, 432–437. [Google Scholar] [CrossRef] [Green Version]
- Benito, N.; Franco, M.; Ribera, A.; Soriano, A.; Rodriguez-Pardo, D.; Sorlí, L.; Fresco, G.; Fernández-Sampedro, M.; Del Toro, M.D.; Guío, L.; et al. Time trends in the aetiology of prosthetic joint infections: A multicentre cohort study. Clin. Microbiol. Infect. 2016, 22, 732.e1–732.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fantoni, M.; Borrè, S.; Rostagno, R.; Riccio, G.; Carrega, G.; Giovannenze, F.; Taccari, F. Epidemiological and clinical features of prosthetic joint infections caused by gram-negative bacteria. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 187–194. [Google Scholar]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New Definition for Periprosthetic Joint Infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandel, C.E.; Jenkinson, R.; Daneman, N.; Backstein, D.; Hansen, B.E.; Muller, M.P.; Katz, K.C.; Widdifield, J.; Bogoch, E.; Ward, S.; et al. Predictors of Treatment Failure for Hip and Knee Prosthetic Joint Infections in the Setting of 1- and 2-Stage Exchange Arthroplasty: A Multicenter Retrospective Cohort. Open Forum Infect. Dis. 2019, 6, ofz452. [Google Scholar] [CrossRef] [Green Version]
- Shohat, N.; Goswami, K.; Tan, T.L.; Fillingham, Y.; Parvizi, J. Increased Failure after Irrigation and Debridement for Acute Hematogenous Periprosthetic Joint Infection. J. Bone Jt. Surg. Am. Vol. 2019, 101, 696–703. [Google Scholar] [CrossRef]
- Leclercq, R.; Cantón, R.; Brown, D.; Giske, C.; Heisig, P.; MacGowan, A.; Mouton, J.; Nordmann, P.; Rodloff, A.; Rossolini, G.; et al. EUCAST expert rules in antimicrobial susceptibility testing. Clin. Microbiol. Infect. 2013, 19, 141–160. [Google Scholar] [CrossRef] [Green Version]
- Villegas, M.V.; Blanco, M.G.; Sifuentes-Osornio, J.; Rossi, F. Increasing prevalence of extended-spectrum-betalactamase among Gram-negative bacilli in Latin America: 2008 update from the Study for Monitoring Antimicrobial Resistance Trends (SMART). Braz. J. Infect. Dis. 2011, 15, 34–39. [Google Scholar] [CrossRef] [Green Version]
- Gales, A.C.; Castanheira, M.; Jones, R.N.; Sader, H.S. Antimicrobial resistance among Gram-negative bacilli isolated from Latin America: Results from SENTRY Antimicrobial Surveillance Program (Latin America, 2008–2010). Diagn. Microbiol. Infect. Dis. 2012, 73, 354–360. [Google Scholar] [CrossRef]
- Vega, S.; Dowzicky, M.J. Antimicrobial susceptibility among Gram-positive and Gram-negative organisms collected from the Latin American region between 2004 and 2015 as part of the Tigecycline Evaluation and Surveillance Trial. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 1–16. [Google Scholar] [CrossRef]
- Kim, Y.A.; Kim, J.J.; Won, D.J.; Lee, K. Seasonal and Temperature-Associated Increase in Community-Onset Acinetobacter baumannii Complex Colonization or Infection. Ann. Lab. Med. 2018, 38, 266–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perencevich, E.N.; McGregor, J.C.; Shardell, M.; Furuno, J.P.; Harris, A.D.; Morris, J.G.; Fisman, D.N.; Johnson, J.A. Summer Peaks in the Incidences of Gram-Negative Bacterial Infection Among Hospitalized Patients. Infect. Control. Hosp. Epidemiol. 2008, 29, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, A.M.E.; Bénard, M.; Meis, J.F.; Van Hellemondt, G.; Goosen, J.H.M. The unsuspected prosthetic joint infection. Bone Jt. J. 2017, 99-B, 1482–1489. [Google Scholar] [CrossRef] [PubMed]
- Hoell, S.; Moeller, A.; Gosheger, G.; Hardes, J.; Dieckmann, R.; Schulz, D. Two-stage revision arthroplasty for periprosthetic joint infections: What is the value of cultures and white cell count in synovial fluid and CRP in serum before second stage reimplantation? Arch. Orthop. Trauma Surg. 2016, 136, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Whitehouse, M.R.; Blom, A.W.; Beswick, A.D.; Team, I. Patient-Related Risk Factors for Periprosthetic Joint Infection after Total Joint Arthroplasty: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0150866. [Google Scholar] [CrossRef]
- Liu, P.; Li, X.; Luo, M.; Xu, X.; Su, K.; Chen, S.; Qing, Y.; Li, Y.; Qiu, J. Risk Factors for Carbapenem-Resistant Klebsiella pneumoniaeInfection: A Meta-Analysis. Microb. Drug Resist. 2018, 24, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Raman, G.; Avendano, E.E.; Chan, J.; Merchant, S.; Puzniak, L. Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control. 2018, 7, 79. [Google Scholar] [CrossRef] [Green Version]
- Benito, N.; Mur, I.; Ribera, A.; Soriano, A.; Rodríguez-Pardo, D.; Sorlí, L.; Cobo, J.; Fernández-Sampedro, M.; Del Toro, M.D.; Guío, L.; et al. The Different Microbial Etiology of Prosthetic Joint Infections according to Route of Acquisition and Time after Prosthesis Implantation, Including the Role of Multidrug-Resistant Organisms. J. Clin. Med. 2019, 8, 673. [Google Scholar] [CrossRef] [Green Version]
- Saleh, K.; Olson, M.; Resig, S.; Bershadsky, B.; Kuskowski, M.; Gioe, T.; Robinson, H.; Schmidt, R.; McElfresh, E. Predictors of wound infection in hip and knee joint replacement: Results from a 20 year surveillance program. J. Orthop. Res. 2002, 20, 506–515. [Google Scholar] [CrossRef]
- Cheung, E.V.; Sperling, J.W.; Cofield, R.H. Infection Associated With Hematoma Formation After Shoulder Arthroplasty. Clin. Orthop. Relat. Res. 2008, 466, 1363–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uçkay, I.; Bernard, L. Gram-Negative versus Gram-Positive Prosthetic Joint Infections. Clin. Infect. Dis. 2010, 50, 795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulos, A.; Ribera, A.; Mavrogenis, A.F.; Rodriguez-Pardo, L.; Bonnet, E.; Josésalles, M.; Del Toro, M.D.; Nguyen, S.; Blanco-García, A.; Skaliczki, G.; et al. Corrigendum to “Multidrug-resistant and extensively drug-resistant Gram-negative prosthetic joint infections: Role of surgery and impact of colistin administration”. Int. J. Antimicrob. Agents 2019, 53, 538–539. [Google Scholar] [CrossRef] [PubMed]
- Cobo, J.; Miguel, L.G.S.; Euba, G.; Rodríguez, D.; García-Lechuz, J.; Riera, M.; Falgueras, L.; Palomino, J.; Benito, N.; Del Toro, M.; et al. Early prosthetic joint infection: Outcomes with debridement and implant retention followed by antibiotic therapy. Clin. Microbiol. Infect. 2011, 17, 1632–1637. [Google Scholar] [CrossRef] [Green Version]


| Characteristics | Number of Patients No. (%) Total = 98 |
|---|---|
| Age (years) (mean ± S.D.) | 67.3 ± 13.2 |
| P50 (P25–P75) | 69.5 (58.7–77) |
| Age group | |
| up to 50 | 10 (1.2) |
| 51–60 | 23 (23.5) |
| 61–70 | 20 (20.4) |
| 71–80 | 31 (31.6) |
| over 80 | 14 (14.3) |
| Time between prosthesis and diagnosis (days) P50 (P25–P 75) | 32 (20–242) |
| Variables related to the patient | |
| Comorbidities (yes) | 71 (72.4) |
| SAH a | 60 (61.2) |
| DM b | 20 (20.4) |
| Malnutrition | 8 (8.2) |
| Anemia | 2 (2.0) |
| Neoplasm | 1 (1.0) |
| Lung disease | 5 (5.1) |
| Metabolic syndrome | 18 (18.4) |
| Cardiovascular disease | 5 (5.1) |
| Other comorbidities c | 11 (11.3) |
| Previous use of an antimicrobial | 37 (37.8) |
| Variables related to the surgical procedure | |
| Arthroplasty | |
| Total | 75 (76.5) |
| Primary | 56 (57.2) |
| Elective | 59 (60.2) |
| Hip | 82 (83.7) |
| DAIR d | 69 (70.4) |
| Procedure duration greater than 2.5 h | 5 (5.1) |
| Blood transfusion | 16 (16.3) |
| Variables related to the postoperative period | |
| Concomitant non-orthopedic infection | 11 (11.2) |
| Previous ortopedic infection | 19 (19.4) |
| Early infection | 68 (69.4) |
| Sepsis | 2 (2.0) |
| Microbial isolates in 56 episodes ofMDR/XDR GNB a PJIb | 60 (100) |
| Acinetobacter baumannii | 31 (51.7) |
| Enterobacter aerogenes | 8 (13.3) |
| Klebsiella pneumoniae | 6 (10.0) |
| Escherichia coli | 5 (8.3) |
| Proteus mirabilis | 4 (6.7) |
| Pseudomonas aeruginosa | 3 (5.0) |
| Others GNB-MDR | 3 (5.0) |
| Microbial isolates in 42 episodes of others bacterias PJI b | 44 (100) |
| MSSA c | 16 (36.4) |
| Pseudomonas aeruginosa | 6 (13.6) |
| MRSA d | 5 (11.4) |
| Enterobacter aerogenes | 4 (9.1) |
| Proteus mirabilis | 3 (6.8) |
| Proteus vulgaris | 2 (4.5) |
| Acinetobacter baumannii | 2 (4.5) |
| Klebsiella pneumoniae | 2 (4.5) |
| Morganella morganii | 1 (2.3) |
| Enterobacter sakazakii | 1 (2.3) |
| Enterobacter cloacae | 1 (2.3) |
| Escherichia coli | 1 (2.3) |
| Variables | Prevalence Ratio 95% CI | p-Value c |
|---|---|---|
| Revision arthroplasty | 1.7 (1.2; 2.4) | 0.002 |
| Previous orthopedic infection | 1.5 (1.1; 2.1) | 0.020 |
| Postoperative hematoma | 2.6 (1.7; 4.0) | <0.001 |
| Early infection | 2.2 (1.4; 3.5) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Silva, R.B.; Salles, M.J. Outcomes and Risk Factors in Prosthetic Joint Infections by multidrug-resistant Gram-negative Bacteria: A Retrospective Cohort Study. Antibiotics 2021, 10, 340. https://doi.org/10.3390/antibiotics10030340
da Silva RB, Salles MJ. Outcomes and Risk Factors in Prosthetic Joint Infections by multidrug-resistant Gram-negative Bacteria: A Retrospective Cohort Study. Antibiotics. 2021; 10(3):340. https://doi.org/10.3390/antibiotics10030340
Chicago/Turabian Styleda Silva, Raquel Bandeira, and Mauro José Salles. 2021. "Outcomes and Risk Factors in Prosthetic Joint Infections by multidrug-resistant Gram-negative Bacteria: A Retrospective Cohort Study" Antibiotics 10, no. 3: 340. https://doi.org/10.3390/antibiotics10030340
APA Styleda Silva, R. B., & Salles, M. J. (2021). Outcomes and Risk Factors in Prosthetic Joint Infections by multidrug-resistant Gram-negative Bacteria: A Retrospective Cohort Study. Antibiotics, 10(3), 340. https://doi.org/10.3390/antibiotics10030340