
Clinical Efficacy of Hydroxychloroquine in Patients with COVID-19: Findings from an Observational Comparative Study in Saudi Arabia

 , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
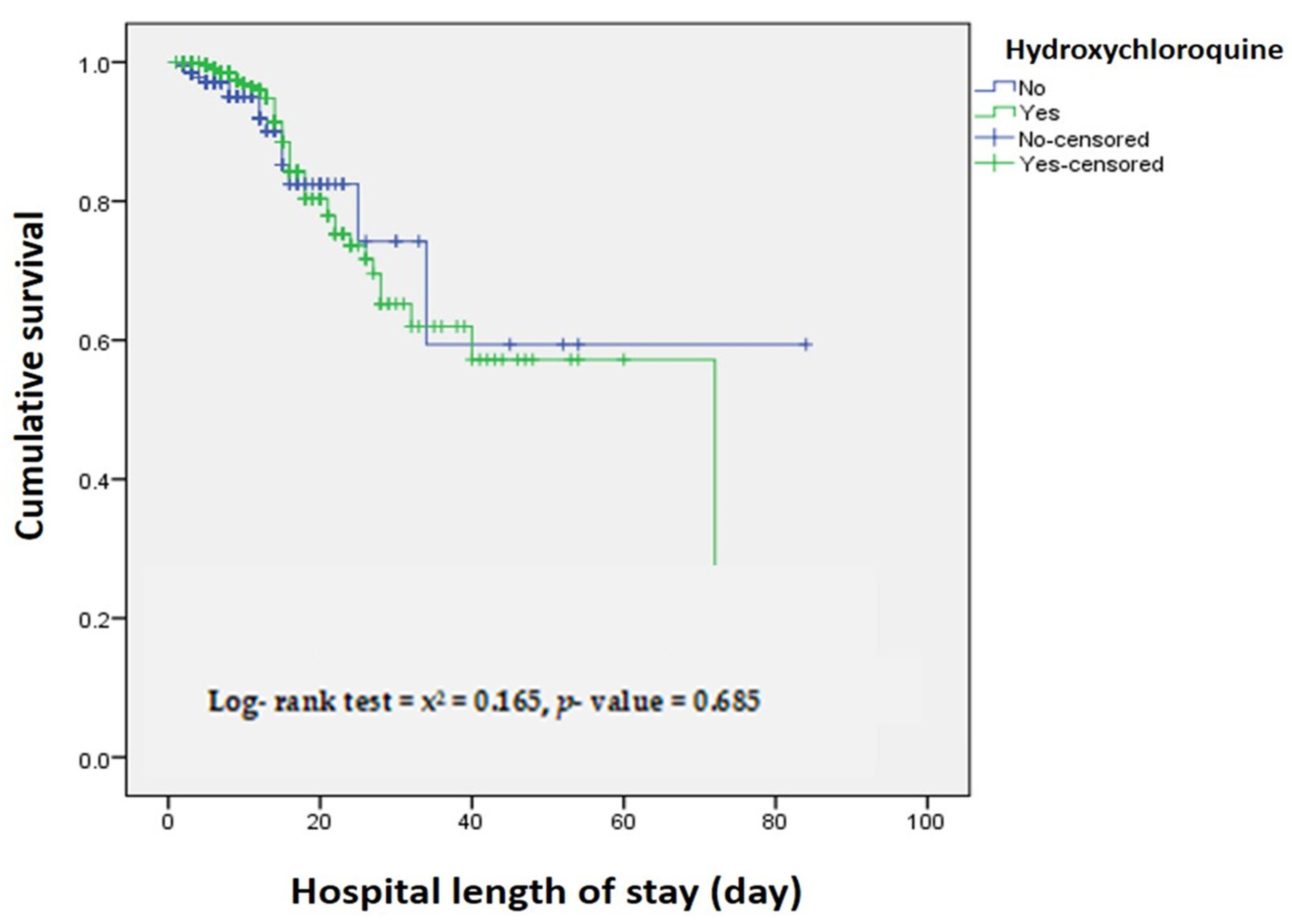
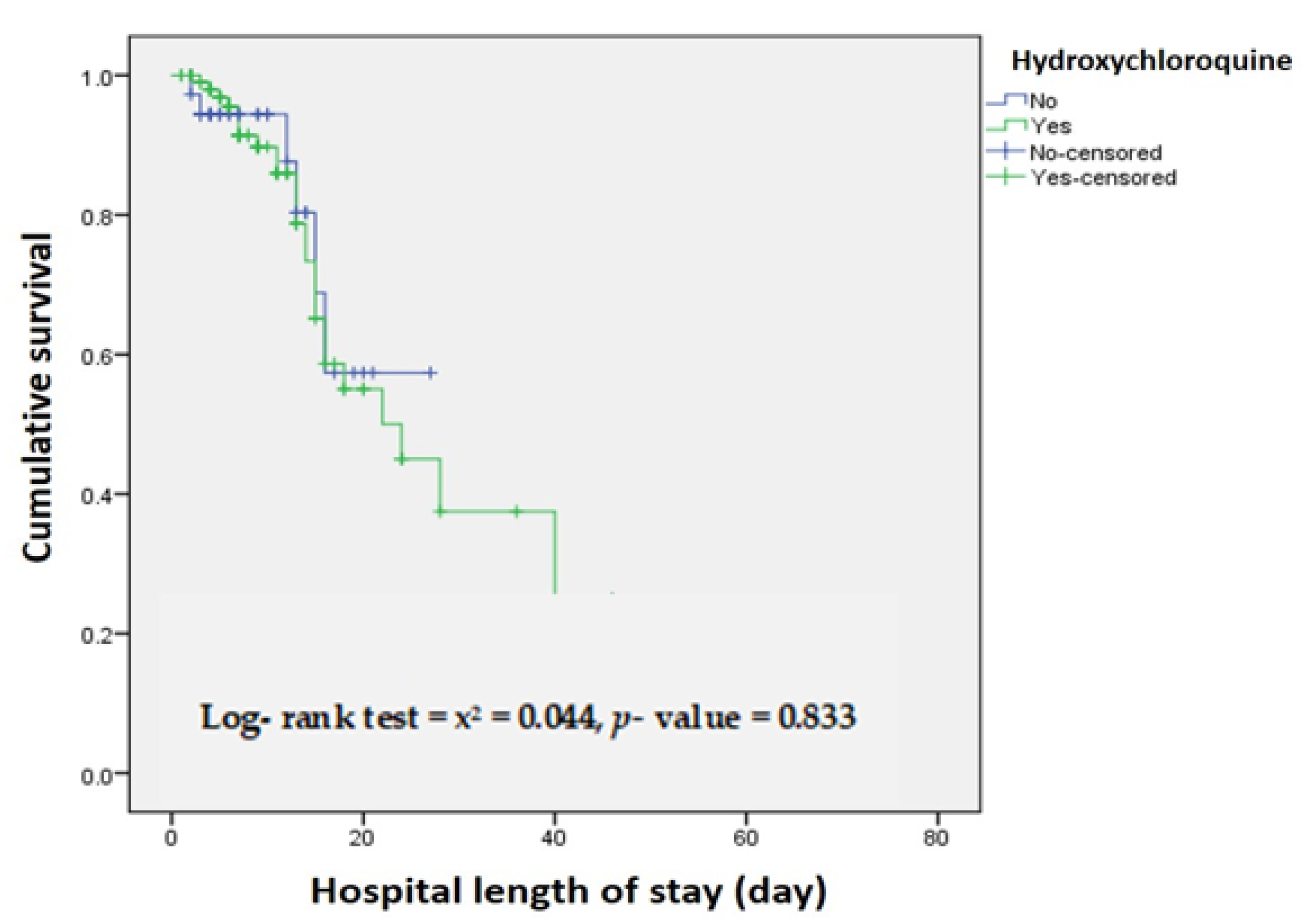
2. Results
3. Discussion
Strengths and Limitations
4. Materials and Methods
4.1. Study Design and Population
4.2. Baseline Information Collection
4.3. Outcomes
4.4. Statistical Analysis
4.5. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McIntosh, K.; Dees, J.H.; Becker, W.B.; Kapikian, A.Z.; Chanock, R.M. Recovery in tracheal organ cultures of novel viruses from patients with respiratory disease. Proc. Natl. Acad. Sci. USA 1967, 57, 933–940. [Google Scholar] [CrossRef] [Green Version]
- Esper, F.; Weibel, C.; Ferguson, D.; Landry, M.L.; Kahn, J.S. Evidence of a Novel Human Coronavirus That is Associated with Respiratory Tract Disease in Infants and Young Children. J. Infect. Dis. 2005, 191, 492–498. [Google Scholar] [CrossRef] [Green Version]
- Stöhr, K.A. A multicentre collaboration to investigate the cause of severe acute respiratory syndrome. Lancet 2003, 361, 1730–1733. [Google Scholar] [CrossRef] [Green Version]
- Peiris, J.S.M.; Lai, S.T.; Poon, L.L.M.; Guan, Y.; Yam, L.Y.C.; Lim, W.; Nicholls, J.; Yee, W.K.S.; Yan, W.W.; Cheung, M.T.; et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet 2003, 361, 1319–1325. [Google Scholar] [CrossRef] [Green Version]
- Zumla, A.; Hui, D.S.; Perlman, S. Middle East respiratory syndrome. Lancet 2015, 386, 995–1007. [Google Scholar] [CrossRef] [Green Version]
- Zaki, A.M.; van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.M.E.; Fouchier, R.A.M. Isolation of a Novel Coronavirus from a Man with Pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef]
- AlTakarli, N.S. Emergence of COVID-19 Infection: What Is Known and What Is to Be Expected–Narrative Review Article. Dubai Med. J. 2020, 3, 13–18. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease-2019 (COVID-19) Situation Report–100; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- European Centre for Disease Prevention and Control. Novel Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK-Sixth Update; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2020.
- Pak, A.; Adegboye, O.A.; Adekunle, A.I.; Rahman, K.M.; McBryde, E.S.; Eisen, D.P. Economic Consequences of the COVID-19 Outbreak: The Need for Epidemic Preparedness. Front. Public Heath 2020, 8, 1–4. [Google Scholar] [CrossRef]
- Casadevall, A.; Pirofski, L.A. The convalescent sera option for containing COVID-19. J. Clin. Investig. 2020, 130, 1545–1548. [Google Scholar] [CrossRef] [Green Version]
- U.S. National Library of Medicine COVID-19. Available online: https://www.clinicaltrials.gov/ct2/results?cond=COVID-19&term=& (accessed on 12 January 2021).
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 1–15. [Google Scholar] [CrossRef]
- Shah, R.R.; Stonier, P.D. Repurposing old drugs in oncology: Opportunities with clinical and regulatory challenges ahead. J. Clin. Pharm. Ther. 2018, 44, 6–22. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Hu, J.; Zhang, Z.; Jiang, S.; Han, S.; Yan, D.; Zhuang, R.; Hu, B.; Zhang, Z. Efficacy of hydroxychloroquine in patients with COVID-19: Results of a randomized clinical trial. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Geleris, J.; Sun, Y.; Platt, J.; Zucker, J.; Baldwin, M.; Hripcsak, G.; Labella, A.; Manson, D.K.; Kubin, C.; Barr, R.G.; et al. Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 382, 2411–2418. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Dufort, E.M.; Udo, T.; Wilberschied, L.A.; Kumar, J.; Tesoriero, J.; Weinberg, P.; Kirkwood, J.; Muse, A.; Dehovitz, J.; et al. Association of Treatment with Hydroxychloroquine or Azithromycin with In-Hospital Mortality in Patients with COVID-19 in New York State. J. Am. Med. Assoc. 2020, 323, 2493–2502. [Google Scholar] [CrossRef]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; Wang, F.; Li, D.; Yang, M.; Xing, L.; et al. Treatment of 5 Critically Ill Patients with COVID-19 with Convalescent Plasma. J. Am. Med. Assoc. 2020, 323, 1582–1589. [Google Scholar] [CrossRef]
- Tripathy, S.; Dassarma, B.; Roy, S.; Chabalala, H. A review on possible modes of action of chloroquine/hydroxychloroquine: Repurposing against SAR-CoV-2 (COVID-19) pandemic. Int. J. Antimicrob. Agents 2020, 56, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Picot, S.; Marty, A.; Bienvenu, A.L.; Blumberg, L.H.; Dupouy-Camet, J.; Carnevale, P.; Kano, S.; Jones, M.K.; Daniel-Ribeiro, C.T.; Mas-Coma, S. Coalition: Advocacy for prospective clinical trials to test the post-exposure potential of hydroxychloroquine against COVID-19. One Health 2020, 9, 1–5. [Google Scholar] [CrossRef]
- Shah, R.R. Chloroquine and hydroxychloroquine for COVID-19: Perspectives on their failure in repurposing. J. Clin. Pharm. Ther. 2020, 46, 17–27. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.; Parola, P.; Hoang, V.T. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Coronavirus (COVID-19) Update: Daily Roundup 30 March 2020. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-daily-roundup-march-30-2020 (accessed on 1 January 2021).
- Juurlink, D.N. Safety considerations with chloroquine, hydroxychloroquine and azithromycin in the management of SARS-CoV-2 infection. Can. Med. Assoc. J. 2020, 192, E450–E453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandvuillemin, A.; Fresse, A.; Cholle, C.; Yamani, S.; Dautriche, A. Adverse drug reactions of hydroxychloroquine: Analysis of French pre-pandemic SARS-CoV2 pharmacovigilance data. Therapie 2020, 75, 385–387. [Google Scholar] [CrossRef]
- Food and Drug Administration. Aralen Chloroquine Phosphate, USP Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/006002s044lbl.pdf (accessed on 1 January 2021).
- Hancox, J.C.; Hasnain, M.; Vieweg, W.V.R.; Crouse, E.L.B.; Baranchuk, A. Azithromycin, cardiovascular risks, QTc interval prolongation, torsade de pointes, and regulatory issues: A narrative review based on the study of case reports. Ther. Adv. Infect. Dis. 2013, 1, 155–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chorin, E.; Dai, M.; Shulman, E.; Wadhwani, L.; Bar-Cohen, R.; Barbhaiya, C.; Aizer, A.; Holmes, D.; Bernstein, S.; Spinelli, M.; et al. The QT interval in patients with COVID-19 treated with hydroxychloroquine and azithromycin. Nat. Med. 2020, 26, 808–809. [Google Scholar] [CrossRef] [PubMed]
- Drew, B.J.; Ackerman, M.J.; Funk, M.; Gibler, W.B.; Kligfield, P.; Menon, V.; Philippides, G.J.; Roden, D.M.; Zareba, W. Prevention of Torsade de Pointes in Hospital Settings: A Scientific Statement from the American Heart Association and the American College of Cardiology Foundation. J. Am. Coll. Cardiol. 2010, 55, 934–947. [Google Scholar] [CrossRef] [Green Version]
- Etchegoyen, C.V.; Keller, G.A.; Mrad, S.; Cheng, S.; Girolamo, G. Di Drug-induced QT Interval Prolongation in the Intensive Care Unit. Curr. Clin. Pharmacol. 2017, 12, 210–222. [Google Scholar] [CrossRef]
- Saudi Ministry of Health. COVID-19 Guidelines. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Pages/covid19.aspx (accessed on 1 January 2021).
- Almazrou, S.H.; Almalki, Z.S.; Alanazi, A.S.; Alqahtani, A.M.; Alghamd, S.M. Comparing the impact of Hydroxychloroquine based regimens and standard treatment on COVID-19 patient outcomes: A retrospective cohort study. Saudi Pharm. J. 2020, 28, 1877–1882. [Google Scholar] [CrossRef] [PubMed]
- Mahevas, M.; Tran, V.-T.; Roumier, M.; Chabrol, A.; Paule, R.; Guillaud, C.; Fois, E.; Lepeule, R.; Szwebel, T.-A.; Lescure, F.-X.; et al. Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: Observational comparative study using routine care data. BMJ 2020. [Google Scholar] [CrossRef] [PubMed]
- Sarma, P.; Kaur, H.; Kumar, H.; Mahendru, D.; Avti, P.; Bhattacharyya, A.; Prajapat, M.; Shekhar, N.; Kumar, S.; Singh, R.; et al. Virological and clinical cure in COVID-19 patients treated with hydroxychloroquine: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Mega, T.A.; Feyissa, T.M.; Bosho, D.D.; Goro, K.K.; Negera, G.Z. The Outcome of Hydroxychloroquine in Patients Treated for COVID-19: Systematic Review and Meta-Analysis. Can. Respir. J. 2020, 2020, 1–16. [Google Scholar] [CrossRef]
- Ip, A.; Ahn, J.; Zhou, Y.; Goy, A.; Hansen, E.; Pecora, A.; Sinclaire, B.; Bednarz, U.; Marafelias, M.; Sawczuk, I.; et al. Hydroxychloroquine in the treatment of outpatients with mildly symptomatic COVID-19: A multi-center observational study. BMC Infect. Dis. 2021, 21, 72. [Google Scholar] [CrossRef]
- Almaghlouth, I.; Islam, T.; Alamro, N.; Alsultan, A.; Alfadda, A.; Al-Muhsen, S.; Almasry, A.; Almadi, M.A.; Hersi, A.; BaHammam, A. Mapping COVID-19 related research from Saudi Arabia, a scoping review: Between reality and dreams. Saudi Med. J. 2020, 41, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Elfiky, A.A. Anti-HCV, nucleotide inhibitors, repurposing against COVID-19. Life Sci. 2020, 248. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Total Patients (n = 775) | G1 (n = 568) | G2 (n = 207) | p-Value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age | |||||||
| Less than 30 | 119 | 15.4% | 84 | 14.8% | 35 | 16.9% | 0.731 |
| 30–50 | 264 | 34.1% | 193 | 34% | 71 | 34.2% | |
| <50 | 392 | 50.6% | 291 | 51.2% | 101 | 48.8% | |
| Gender | |||||||
| Female | 368 | 47.5% | 252 | 44.4% | 116 | 56% | 0.004 |
| Male | 407 | 52.5% | 316 | 55.6% | 91 | 44% | |
| Nationality | |||||||
| Saudi | 640 | 82.6% | 463 | 81.5% | 177 | 85.5% | 0.195 |
| Non-Saudi | 135 | 17.4% | 105 | 18.5% | 30 | 14.5% | |
| Treatment Regimens | Number of Patients | % |
|---|---|---|
| Group 1 (n = 568) | ||
| Hydroxychloroquine | 147 | 25.9 |
| Hydroxychloroquine + Ceftriaxone | 137 | 24.1 |
| Hydroxychloroquine + Ceftriaxone + azithromycin | 76 | 13.4 |
| Hydroxychloroquine + azithromycin + Tamiflu | 50 | 8.8 |
| Hydroxychloroquine + azithromycin | 37 | 6.5 |
| Hydroxychloroquine + ceftriaxone + favipiravir | 21 | 3.7 |
| Hydroxychloroquine + ceftriaxone + azithromycin + favipiravir | 19 | 3.3 |
| Hydroxychloroquine + ceftriaxone + azithromycin + Tamiflu | 18 | 3.2 |
| Hydroxychloroquine + ceftriaxone + Tamiflu | 11 | 1.9 |
| Hydroxychloroquine + Tamiflu | 6 | 1.1 |
| Hydroxychloroquine + azithromycin + favipiravir | 6 | 1.1 |
| Hydroxychloroquine + azithromycin + Lopinavir/Ritonavir + Tamiflu | 5 | 0.9 |
| Hydroxychloroquine + favipiravir | 5 | 0.9 |
| Hydroxychloroquine + ceftriaxone + azithromycin + favipiravir + Tamiflu | 4 | 0.7 |
| Hydroxychloroquine + ceftriaxone + azithromycin + Lopinavir/Ritonavir + Tamiflu | 3 | 0.5 |
| Hydroxychloroquine + ceftriaxone + Ribavirin + Lopinavir/Ritonavir | 3 | 0.5 |
| Hydroxychloroquine + ceftriaxone + azithromycin + Lopinavir/Ritonavir | 3 | 0.5 |
| Hydroxychloroquine + ceftriaxone + azithromycin + Ribavirin + Lopinavir/Ritonavir | 2 | 0.4 |
| Hydroxychloroquine + ceftriaxone + azithromycin + Ribavirin + Lopinavir/Ritonavir + Tamiflu | 2 | 0.4 |
| Hydroxychloroquine + azithromycin + Ribavirin + Tamiflu | 2 | 0.4 |
| Hydroxychloroquine + Ribavirin | 2 | 0.4 |
| Hydroxychloroquine + azithromycin + favipiravir + Tamiflu | 2 | 0.4 |
| Hydroxychloroquine + ceftriaxone + azithromycin + favipiravir + Tocilizumab + Tamiflu | 2 | 0.4 |
| Hydroxychloroquine + Ribavirin + Lopinavir/Ritonavir + Tamiflu | 1 | 0.2 |
| Hydroxychloroquine + favipiravir + Tocilizumab | 1 | 0.2 |
| Hydroxychloroquine + azithromycin + Lopinavir/Ritonavir | 1 | 0.2 |
| Hydroxychloroquine + ceftriaxone + azithromycin + Tocilizumab | 1 | 0.2 |
| Hydroxychloroquine + ceftriaxone + Ribavirin | 1 | 0.2 |
| Group 2 (n = 207) | ||
| Ceftriaxone | 56 | 27.1 |
| Ceftriaxone + azithromycin | 56 | 27.1 |
| Azithromycin | 46 | 22.2 |
| Ceftriaxone + azithromycin + favipiravir | 10 | 4.8 |
| Ceftriaxone + favipiravir | 8 | 3.9 |
| Azithromycin + Tamiflu | 7 | 3.4 |
| Ceftriaxone + Tamiflu | 6 | 2.9 |
| Ceftriaxone + azithromycin + Tamiflu | 4 | 1.9 |
| Favipiravir | 4 | 1.9 |
| Azithromycin + favipiravir | 2 | 1.0 |
| Ribavirin | 2 | 1.0 |
| Ceftriaxone + azithromycin + Tocilizumab | 1 | 0.5 |
| Ceftriaxone + azithromycin + Ribavirin | 1 | 0.5 |
| Ceftriaxone + azithromycin + favipiravir + Tamiflu | 1 | 0.5 |
| Azithromycin + Ribavirin | 1 | 0.5 |
| Tamiflu | 1 | 0.5 |
| Ceftriaxone + Ribavirin + Lopinavir/Ritonavir | 1 | 0.5 |
| G1 (n = 568) | G2 (n = 207) | |||||||
|---|---|---|---|---|---|---|---|---|
| Outcome | Mean | SD | Median | IQR | Mean | SD | Median | IQR |
| Hospital length of stay | 14.01 | 11.74 | 11 | 7–17 | 11.36 | 9.73 | 9.5 | 4–15.7 |
| Time in ICU | 11.48 | 10 | 9 | 5-15 | 9.44 | 6.32 | 8 | 4–13.7 |
| N | % | N | % | |||||
| ICU admission | 104 | 18.3% | 36 | 17.4% | ||||
| Mechanical ventilator | 63 | 26.8% | 21 | 31.3% | ||||
| Mortality rate | 44 | 7.7% | 15 | 7.2% | ||||
| Outcome | Estimates | SE | p-Value |
|---|---|---|---|
| Hospital length of stay | 0.028 | 0.04 | 0.451 |
| ICU admission | −0.063 | 0.21 | 0.769 |
| Time in ICU | 0.002 | 0.04 | 0.972 |
| Mechanical ventilator | −0.599 | 0.48 | 0.211 |
| Mortality rate | 0.756 | 0.58 | 0.191 |
| No of Patients at Risk N (%) | ||||
|---|---|---|---|---|
| Day 1 (Admission) | Day 7 | Day 14 | Day 28 | |
| Hydroxychloroquine | 566 (100) | 346 (61) | 141 (24.9) | 31 (5.5) |
| Non-Hydroxychloroquine | 206 (100) | 104 (50.5) | 41 (20) | 7 (3.4) |
| No of Patients at Risk N (%) | ||||
|---|---|---|---|---|
| Day 1 (Admission) | Day 7 | Day 14 | Day 28 | |
| Hydroxychloroquine | 103 (100) | 68 (66) | 28 (27) | 5 (4.8) |
| Non-Hydroxychloroquine | 35 (100) | 19 (54.3) | 8 (22.9) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alghamdi, S.; Barakat, B.; Berrou, I.; Alzahrani, A.; Haseeb, A.; Hammad, M.A.; Anwar, S.; Sindi, A.A.A.; Almasmoum, H.A.; Albanghali, M. Clinical Efficacy of Hydroxychloroquine in Patients with COVID-19: Findings from an Observational Comparative Study in Saudi Arabia. Antibiotics 2021, 10, 365. https://doi.org/10.3390/antibiotics10040365
Alghamdi S, Barakat B, Berrou I, Alzahrani A, Haseeb A, Hammad MA, Anwar S, Sindi AAA, Almasmoum HA, Albanghali M. Clinical Efficacy of Hydroxychloroquine in Patients with COVID-19: Findings from an Observational Comparative Study in Saudi Arabia. Antibiotics. 2021; 10(4):365. https://doi.org/10.3390/antibiotics10040365
Chicago/Turabian StyleAlghamdi, Saleh, Bassant Barakat, Ilhem Berrou, Abdulhakim Alzahrani, Abdul Haseeb, Mohamed Anwar Hammad, Sirajudheen Anwar, Abdulmajeed Abdulghani A. Sindi, Hussain A. Almasmoum, and Mohammad Albanghali. 2021. "Clinical Efficacy of Hydroxychloroquine in Patients with COVID-19: Findings from an Observational Comparative Study in Saudi Arabia" Antibiotics 10, no. 4: 365. https://doi.org/10.3390/antibiotics10040365
APA StyleAlghamdi, S., Barakat, B., Berrou, I., Alzahrani, A., Haseeb, A., Hammad, M. A., Anwar, S., Sindi, A. A. A., Almasmoum, H. A., & Albanghali, M. (2021). Clinical Efficacy of Hydroxychloroquine in Patients with COVID-19: Findings from an Observational Comparative Study in Saudi Arabia. Antibiotics, 10(4), 365. https://doi.org/10.3390/antibiotics10040365