
Meropenem Stability in Human Plasma at −20 °C: Detailed Assessment of Degradation

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
Data Availability
3. Discussion
4. Materials and Methods
4.1. Sample Preparation
4.2. Degradation Experiment Design
4.3. Degradation Modeling
4.4. Polynomial Regression
4.5. Artificial Neural Networks
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdul-Aziz, M.H.; Alffenaar, J.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.A.; Pea, F.; Sjovall, F.; et al. Infection Section of European Society of Intensive Care M, Pharmacokinetic/pharmacodynamic, Critically Ill Patient Study Groups of European Society of Clinical M, Infectious D, Infectious Diseases Group of International Association of Therapeutic Drug M, Clinical T, Infections in the ICU, Sepsis Working Group of International Society of Antimicrobial C, Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Societe Francaise de Pharmacologie et Therapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Societe Francaise d'Anesthesie et Reanimation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar]
- Wong, G.; Brinkman, A.; Benefield, R.J.; Carlier, M.; De Waele, J.J.; El Helali, N.; Frey, O.; Harbarth, S.; Huttner, A.; McWhinney, B.; et al. An international, multicentre survey of beta-lactam antibiotic therapeutic drug monitoring practice in intensive care units. J. Antimicrob. Chemother. 2014, 69, 1416–1423. [Google Scholar] [CrossRef] [Green Version]
- Denooz, R.; Charlier, C. Simultaneous determination of five beta-lactam antibiotics (cefepim, ceftazidim, cefuroxim, meropenem and piperacillin) in human plasma by high-performance liquid chromatography with ultraviolet detection. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2008, 864, 161–167. [Google Scholar] [CrossRef]
- D'Cunha, R.; Bach, T.; Young, B.A.; Li, P.; Nalbant, D.; Zhang, J.; Winokur, P.; An, G. Quantification of Cefepime, Meropenem, Piperacillin, and Tazobactam in Human Plasma Using a Sensitive and Robust Liquid Chromatography-Tandem Mass Spectrometry Method, Part 2: Stability Evaluation. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [Green Version]
- Pinder, N.; Brenner, T.; Swoboda, S.; Weigand, M.A.; Hoppe-Tichy, T. Therapeutic drug monitoring of beta-lactam antibiotics–Influence of sample stability on the analysis of piperacillin, meropenem, ceftazidime and flucloxacillin by HPLC-UV. J. Pharm. Biomed. Anal. 2017, 143, 86–93. [Google Scholar] [CrossRef]
- Mortensen, J.S.; Jensen, B.P.; Zhang, M.; Doogue, M. Preanalytical Stability of Piperacillin, Tazobactam, Meropenem, and Ceftazidime in Plasma and Whole Blood Using Liquid Chromatography-Tandem Mass Spectrometry. Ther. Drug Monit. 2019, 41, 538–543. [Google Scholar] [CrossRef]
- Zou, L.; Meng, F.; Hu, L.; Huang, Q.; Liu, M.; Yin, T. A novel reversed-phase high-performance liquid chromatographic assay for the simultaneous determination of imipenem and meropenem in human plasma and its application in TDM. J. Pharm. Biomed. Anal. 2019, 169, 142–150. [Google Scholar] [CrossRef]
- Lefeuvre, S.; Bois-Maublanc, J.; Hocqueloux, L.; Bret, L.; Francia, T.; Eleout-Da Violante, C.; Billaud, E.M.; Barbier, F.; Got, L. A simple ultra-high-performance liquid chromatography-high resolution mass spectrometry assay for the simultaneous quantification of 15 antibiotics in plasma. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2017, 1065-1066, 50–58. [Google Scholar] [CrossRef]
- Martens-Lobenhoffer, J.; Monastyrski, D.; Troger, U.; Bode-Boger, S.M. Stability of meropenem in plasma versus dried blood spots (DBS). J. Pharm. Biomed. Anal. 2019, 170, 279–284. [Google Scholar] [CrossRef]
- Zander, J.; Maier, B.; Zoller, M.; Dobbeler, G.; Frey, L.; Teupser, D.; Vogeser, M. Effects of biobanking conditions on six antibiotic substances in human serum assessed by a novel evaluation protocol. Clin. Chem. Lab. Med. 2016, 54, 265–274. [Google Scholar] [CrossRef]
- Kong, L.; Tang, Y.; Zhang, X.; Lu, G.; Yu, M.; Shi, Q.; Wu, X. Pharmacokinetic/Pharmacodynamic Analysis of Meropenem for the Treatment of Nosocomial Pneumonia in Intracerebral Hemorrhage Patients by Monte Carlo Simulation. Ann. Pharmacother. 2017, 51, 970–975. [Google Scholar] [CrossRef]
- Wenzler, E.; Gotfried, M.H.; Loutit, J.S.; Durso, S.; Griffith, D.C.; Dudley, M.N.; Rodvold, K.A. Meropenem-RPX7009 Concentrations in Plasma, Epithelial Lining Fluid, and Alveolar Macrophages of Healthy Adult Subjects. Antimicrob. Agents Chemother. 2015, 59, 7232–7239. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.A.; Kirkpatrick, C.M.; Roberts, M.S.; Robertson, T.A.; Dalley, A.J.; Lipman, J. Meropenem dosing in critically ill patients with sepsis and without renal dysfunction: Intermittent bolus versus continuous administration? Monte Carlo dosing simulations and subcutaneous tissue distribution. J. Antimicrob. Chemother. 2009, 64, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.Y.; Gu, J.; Lyu, J.; Liu, D.; Wang, Y.T.; Liu, F.; Zhu, F.X.; An, Y.Z. Pharmacokinetic and Pharmacodynamic Efficacies of Continuous versus Intermittent Administration of Meropenem in Patients with Severe Sepsis and Septic Shock: A Prospective Randomized Pilot Study. Chin. Med. J. (Engl.) 2017, 130, 1139–1145. [Google Scholar] [CrossRef]
- Jaruratanasirikul, S.; Sriwiriyajan, S.; Punyo, J. Comparison of the pharmacodynamics of meropenem in patients with ventilator-associated pneumonia following administration by 3-hour infusion or bolus injection. Antimicrob. Agents Chemother. 2005, 49, 1337–1339. [Google Scholar] [CrossRef] [Green Version]
- Afshartous, D.; Bauer, S.R.; Connor, M.J.; Aduroja, O.A.; Amde, M.; Salem, C.; Groszek, J.J.; Fissell, W.H. Pharmacokinetics and pharmacodynamics of imipenem and meropenem in critically ill patients treated with continuous venovenous hemodialysis. Am. J. Kidney Dis. 2014, 63, 170–171. [Google Scholar] [CrossRef] [Green Version]
- Kielstein, J.T.; Czock, D.; Schopke, T.; Hafer, C.; Bode-Boger, S.M.; Kuse, E.; Keller, F.; Fliser, D. Pharmacokinetics and total elimination of meropenem and vancomycin in intensive care unit patients undergoing extended daily dialysis. Crit. Care Med. 2006, 34, 51–56. [Google Scholar] [CrossRef]
- Rubino, C.M.; Bhavnani, S.M.; Loutit, J.S.; Morgan, E.E.; White, D.; Dudley, M.N.; Griffith, D.C. Phase 1 Study of the Safety, Tolerability, and Pharmacokinetics of Vaborbactam and Meropenem Alone and in Combination following Single and Multiple Doses in Healthy Adult Subjects. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [Green Version]
- ICH Expert Working Group. International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use. ICH Harmonised Tripartite Guideline. Evaluation for Stability Data. Q1E; ICH Expert Working Group: Geneva, Switzerland, 2003. [Google Scholar]
- FDA. Bioanalytical Method Validation Guidance for Industry. 2018. Available online: https://www.fda.gov/media/70858/download (accessed on 30 March 2021).
- Mendez, A.; Chagastelles, P.; Palma, E.; Nardi, N.; Schapoval, E. Thermal and alkaline stability of meropenem: Degradation products and cytotoxicity. Int. J. Pharm. 2008, 350, 95–102. [Google Scholar] [CrossRef]
- Bax, R.P.; Bastain, W.; Featherstone, A.; Wilkinson, D.M.; Hutchison, M.; Haworth, S.J. The pharmacokinetics of meropenem in volunteers. J. Antimicrob. Chemother. 1989, 24, 311–320. [Google Scholar] [CrossRef]
- Wallenburg, E.; Bruggemann, R.J.; Asouit, K.; Teulen, M.; de Haan, A.F.J.; Franssen, E.J.F.; Aarnoutse, R.E. First international quality control programme for laboratories measuring antimicrobial drugs to support dose individualization in critically ill patients. J. Antimicrob. Chemother. 2021, 76, 430–433. [Google Scholar] [CrossRef]
- Di, L.; Kerns, E.H.; Hong, Y.; Chen, H. Development and application of high throughput plasma stability assay for drug discovery. Int. J. Pharm. 2005, 297, 110–119. [Google Scholar] [CrossRef]
- Marquardt, D.W.; Snee, R.D. Ridge Regression in Practice. Am. Stat. 1975, 29, 3–20. [Google Scholar]
- Gelman, A. Scaling regression inputs by dividing by two standard deviations. Stat. Med. 2008, 27, 2865–2873. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.A.; Bottou, L.; Orr, G.B.; Müller, K.-R. Efficient BackProp. In Neural Networks: Tricks of the Trade: Second Edition, Montavon, G., Orr, G.B., Müller, K.-R., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 9–48. [Google Scholar]
- Box, G.E.P.; Behnken, D.W. Some New Three Level Designs for the Study of Quantitative Variables. Technometrics 1960, 2, 455–475. [Google Scholar] [CrossRef]
- Cybenko, G. Approximation by superpositions of a sigmoidal function. Math. Control Signals Syst. 1989, 2, 303–314. [Google Scholar] [CrossRef]
- Fletcher, R. Newton-Like Methods. In Practical Methods of Optimization; Springer: Berlin/Heidelberg, Germany, 2000; pp. 44–79. [Google Scholar]
- Cawley, G.; Talbot, N. On Over-fitting in Model Selection and Subsequent Selection Bias in Performance Evaluation. J. Mach. Learn. Res. 2010, 11, 2079–2107. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Seabold, S.; Perktold, J. Statsmodels: Econometric and Statistical Modeling with Python. In Proceedings of the Python in Science Conference, Austin, TX, USA, 6–12 July 2020. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
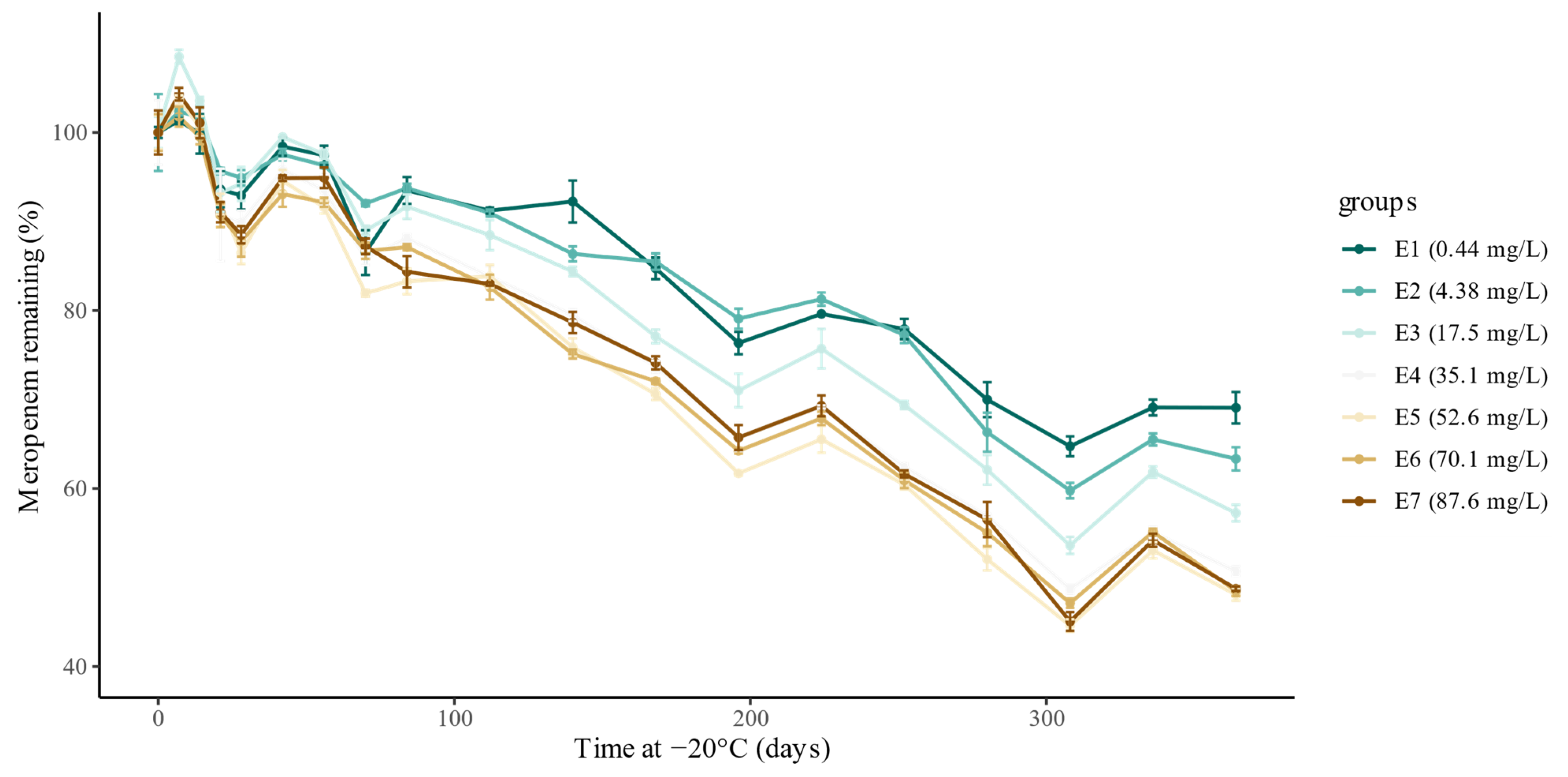
| Spiked Concentration (mg/L) | Time at −20 °C (Days) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 7 | 14 | 21 | 28 | 42 | 56 | 70 | 84 | 112 | 140 | 168 | 196 | 224 | 252 | 280 | 308 | 336 | 364 | |
| 0.44 (E1) | 0.46 | 0.46 | 0.46 | 0.43 | 0.43 | 0.45 | 0.45 | 0.40 | 0.43 | 0.42 | 0.42 | 0.39 | 0.35 | 0.37 | 0.36 | 0.32 | 0.30 | 0.32 | 0.32 |
| 4.38 (E2) | 4.37 | 4.47 | 4.44 | 4.18 | 4.15 | 4.26 | 4.21 | 4.02 | 4.10 | 3.97 | 3.77 | 3.74 | 3.46 | 3.55 | 3.38 | 2.90 | 2.61 | 2.86 | 2.77 |
| 17.5 (E3) | 16.4 | 17.8 | 17.0 | 15.3 | 15.5 | 16.3 | 16.0 | 14.6 | 15.0 | 14.5 | 13.8 | 12.6 | 11.6 | 12.4 | 11.4 | 10.2 | 8.8 | 10.1 | 9.4 |
| 35.1 (E4) | 33.2 | 34.5 | 33.5 | 30.2 | 29.9 | 31.8 | 31.1 | 28.5 | 29.3 | 27.9 | 26.4 | 24.5 | 21.8 | 23.0 | 20.7 | 18.9 | 16.2 | 18.3 | 16.9 |
| 52.6 (E5) | 50.3 | 52.1 | 50.6 | 46.2 | 43.5 | 47.5 | 46.1 | 41.2 | 41.9 | 42.1 | 38.1 | 35.5 | 31.0 | 32.9 | 30.4 | 26.2 | 22.4 | 26.7 | 24.2 |
| 70.1 (E6) | 67.5 | 68.7 | 67.2 | 61.2 | 59.3 | 62.8 | 62.2 | 58.5 | 58.8 | 55.8 | 50.7 | 48.6 | 43.4 | 45.8 | 41.1 | 37.1 | 31.8 | 37.2 | 32.7 |
| 87.6 (E7) | 83.3 | 86.9 | 84.2 | 75.8 | 73.7 | 79.0 | 79.0 | 72.6 | 70.2 | 69.1 | 65.5 | 61.7 | 54.7 | 57.7 | 51.3 | 47.1 | 37.5 | 45.1 | 40.6 |
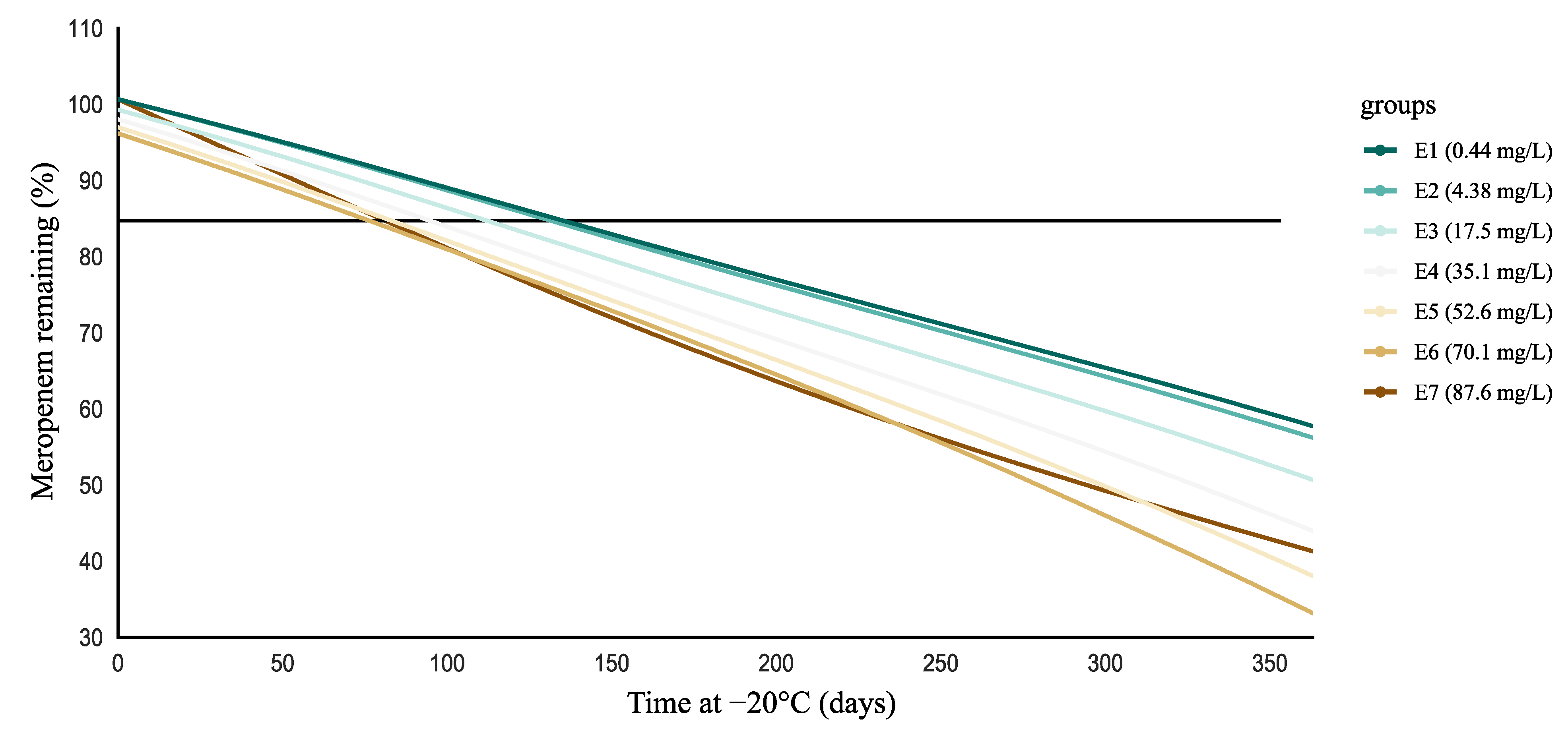
| POLY | ANN | |||
|---|---|---|---|---|
| Experiment Number | RMSE (%) | R2 | RMSE (%) | R2 |
| E1 (0.44 mg/L) | 5.68 | 0.868 | 3.60 | 0.909 |
| E2 (4.38 mg/L) | 3.03 | 0.948 | 2.91 | 0.949 |
| E3 (17.5 mg/L) | 4.24 | 0.922 | 4.15 | 0.926 |
| E4 (35.1 mg/L) | 3.89 | 0.950 | 3.75 | 0.953 |
| E5 (52.6 mg/L) | 4.49 | 0.928 | 4.25 | 0.941 |
| E6 (70.1 mg/L) | 3.43 | 0.962 | 3.14 | 0.967 |
| E7 (87.6 mg/L) | 3.93 | 0.945 | 3.03 | 0.970 |
| Mean ± SD | 4.10 ± 0.850 | 0.932 ± 0.031 | 3.55 ± 0.539 | 0.945 ± 0.022 |
| Coefficient (95% CI) | SD | t-Value | p-Value | |
|---|---|---|---|---|
| 0.779 (0.765–0.794) | 0.007 | 106 | 0.000 | |
| −0.166 (−0.176–−0.156) | 0.005 | −34.5 | 0.000 | |
| −0.046 (−0.054–−0.037) | 0.005 | −10.0 | 0.000 | |
| 0.004 (−0.006–0.013) | 0.005 | 0.736 | 0.463 | |
| −0.021 (−0.032–−0.010) | 0.005 | −3.90 | 0.000 | |
| 0.019 (0.010–0.028) | 0.005 | 4.04 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gijsen, M.; Filtjens, B.; Annaert, P.; Armoudjian, Y.; Debaveye, Y.; Wauters, J.; Slaets, P.; Spriet, I. Meropenem Stability in Human Plasma at −20 °C: Detailed Assessment of Degradation. Antibiotics 2021, 10, 449. https://doi.org/10.3390/antibiotics10040449
Gijsen M, Filtjens B, Annaert P, Armoudjian Y, Debaveye Y, Wauters J, Slaets P, Spriet I. Meropenem Stability in Human Plasma at −20 °C: Detailed Assessment of Degradation. Antibiotics. 2021; 10(4):449. https://doi.org/10.3390/antibiotics10040449
Chicago/Turabian StyleGijsen, Matthias, Benjamin Filtjens, Pieter Annaert, Yeghig Armoudjian, Yves Debaveye, Joost Wauters, Peter Slaets, and Isabel Spriet. 2021. "Meropenem Stability in Human Plasma at −20 °C: Detailed Assessment of Degradation" Antibiotics 10, no. 4: 449. https://doi.org/10.3390/antibiotics10040449
APA StyleGijsen, M., Filtjens, B., Annaert, P., Armoudjian, Y., Debaveye, Y., Wauters, J., Slaets, P., & Spriet, I. (2021). Meropenem Stability in Human Plasma at −20 °C: Detailed Assessment of Degradation. Antibiotics, 10(4), 449. https://doi.org/10.3390/antibiotics10040449