
Clinical Impact of Revised Ciprofloxacin Breakpoint in Patients with Urinary Tract Infections by Enterobacteriaceae

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
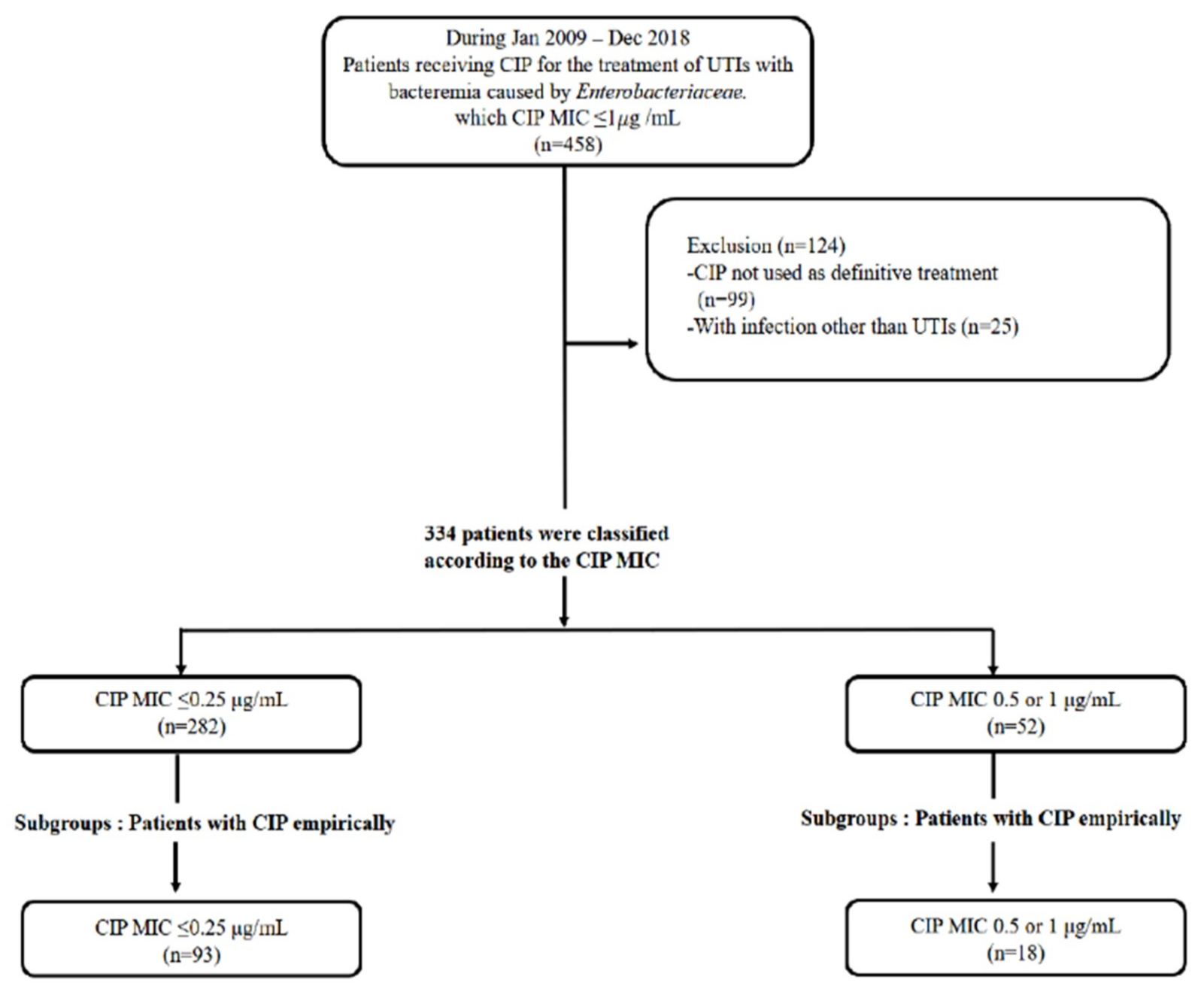
2.1. Study Populations, Baseline Characteristics, and Severity of Infections
2.2. Clinical Outcomes of Patients with Enterobacteriaceae Bacteremic UTIs
2.3. Multivariate Analysis of Relapse within 4 Weeks and 90 Days Recurrence
2.4. A Subgroup of 111 Patients Treated with CIP Empirically as Well as Definitively
3. Discussion
4. Method
4.1. Study Designs and Patients
4.2. Antimicrobial Susceptibility Testing
4.3. Clinical Evaluation and Outcomes
4.4. Definitions
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hooton, T.M. Uncomplicated Urinary Tract Infection. N. Engl. J. Med. 2012, 366, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.; Lyman, A.; Gupta, K.; Mahoney, M.V.; Snyder, G.M.; Hirsch, E.B. Clinical Management of an Increasing Threat: Outpatient Urinary Tract Infections Due to Multidrug-Resistant Uropathogens. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, 960–965. [Google Scholar] [CrossRef]
- Foxman, B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am. J. Med. 2002, 5s–13s. [Google Scholar] [CrossRef]
- Wayne, P. CLSI. Fluoroquinolone Breakpoints for Enterobacteriaceae and Pseudomonas Aeruginosa. 1st ed. CLSI Ratinale Document MR02. Available online: www.clsi.org (accessed on 20 February 2021).
- Lettieri, J.T.; Rogge, M.C.; Kaiser, L.; Echols, R.M.; Heller, A.H. Pharmacokinetic profiles of ciprofloxacin after single intravenous and oral doses. Antimicrob. Agents Chemother. 1992, 36, 993–996. [Google Scholar] [CrossRef]
- Kim, E.S.; Hooper, D.C. Clinical Importance and Epidemiology of Quinolone Resistance. Infect. Chemother. 2014, 46, 226–238. [Google Scholar] [CrossRef] [PubMed]
- Hooper, D.C.; Jacoby, G.A. Mechanisms of drug resistance: Quinolone resistance. Ann. N. Y. Acad. Sci. 2015, 1354, 12–31. [Google Scholar] [CrossRef] [PubMed]
- Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; CLSI Supplement M100; The Clinical Laboratory Standards Institute: Wayne, PA, USA, 2018.
- Humphries, R.M.; Abbott, A.N.; Hindler, J.A. Understanding and Addressing CLSI Breakpoint Revisions: A Primer for Clinical Laboratories. J. Clin. Microbiol. 2019, 57. [Google Scholar] [CrossRef]
- Performance Standards for Antimicrobial Susceptibility Testing, 29th ed; CLSI Supplement M100; The Clinical Laboratory Standards Institute: Wayne, PA, USA, 2019.
- Forrest, A.; Nix, D.E.; Ballow, C.H.; Goss, T.F.; Birmingham, M.C.; Schentag, J.J. Pharmacodynamics of intravenous ciprofloxacin in seriously ill patients. Antimicrob. Agents Chemother. 1993, 37, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Drusano, G.L.; Preston, S.L.; Fowler, C.; Corrado, M.; Weisinger, B.; Kahn, J. Relationship between fluoroquinolone area under the curve: Minimum inhibitory concentration ratio and the probability of eradication of the infecting pathogen, in patients with nosocomial pneumonia. J. Infect. Dis. 2004, 189, 1590–1597. [Google Scholar] [CrossRef]
- Ebbing, L.; Metlay, J.P.; Bilker, W.B.; Edelstein, P.H.; Fishman, N.O. Association between Fluoroquinolone Resistance and Mortality in Escherichia coli and Klebsiella pneumoniae Infections: The Role of Inadequate Empirical Antimicrobial Therapy. Clin. Infect. Dis. 2005, 41, 923–929. [Google Scholar] [CrossRef]
- Peralta, G.; Sánchez, M.B.; Garrido, J.C.; De Benito, I.; Cano, M.E.; Martínez-Martínez, L.; Roiz, M.P. Impact of antibiotic resistance and of adequate empirical antibiotic treatment in the prognosis of patients with Escherichia coli bacteraemia. J. Antimicrob. Chemother. 2007, 60, 855–863. [Google Scholar] [CrossRef]
- Lee, S.S.; Kim, Y.; Chung, D.R. Impact of discordant empirical therapy on outcome of community-acquired bacteremic acute pyelonephritis. J. Infect. 2011, 62, 159–164. [Google Scholar] [CrossRef]
- Jeon, J.H.; Kim, K.; Han, W.D.; Song, S.H.; Park, K.U.; Rhee, J.E.; Song, K.H.; Park, W.B.; Kim, E.S.; Park, S.W.; et al. Empirical use of ciprofloxacin for acute uncomplicated pyelonephritis caused by Escherichia coli in communities where the prevalence of fluoroquinolone resistance is high. Antimicrob. Agents Chemother. 2012, 56, 3043–3046. [Google Scholar] [CrossRef]
- Gupta, K.; Hooton, T.M.; Stamm, W.E. Increasing antimicrobial resistance and the management of uncomplicated community-acquired urinary tract infections. Ann. Intern. Med. 2001, 135, 41–50. [Google Scholar] [CrossRef]
- Chen, Y.H.; Ko, W.C.; Hsueh, P.R. The role of fluoroquinolones in the management of urinary tract infections in areas with high rates of fluoroquinolone-resistant uropathogens. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 1699–1704. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, Y.; Liu, C.; Kudinha, T.; Liu, X.; Luo, Y.; Yang, Q.; Sun, H.; Hu, J.; Xu, Y.C. Comparison of five commonly used automated susceptibility testing methods for accuracy in the China Antimicrobial Resistance Surveillance System (CARSS) hospitals. Infect. Drug Resist. 2018, 11, 1347–1358. [Google Scholar] [CrossRef] [PubMed]
- Gales, A.C.; Gordon, K.A.; Wilke, W.W.; Pfaller, M.A.; Jones, R.N. Occurrence of single-point gyrA mutations among ciprofloxacin-susceptible Escherichia coli isolates causing urinary tract infections in Latin America. Diagn. Microbiol. Infect. Dis. 2000, 36, 61–64. [Google Scholar] [CrossRef]
- Pourahmad Jaktaji, R.; Mohiti, E. Study of Mutations in the DNA gyrase gyrA Gene of Escherichia coli. Iran J. Pharm Res. 2010, 9, 43–48. [Google Scholar]
- Kim, H.B.; Park, C.H.; Kim, C.J.; Kim, E.C.; Jacoby, G.A.; Hooper, D.C. Prevalence of plasmid-mediated quinolone resistance determinants over a 9-year period. Antimicrob. Agents Chemother. 2009, 53, 639–645. [Google Scholar] [CrossRef]
- Yang, H.Y.; Nam, Y.S.; Lee, H.J. Prevalence of plasmid-mediated quinolone resistance genes among ciprofloxacin-nonsusceptible Escherichia coli and Klebsiella pneumoniae isolated from blood cultures in Korea. Can. J. Infect. Dis. Med Microbiol. 2014, 25, 163–169. [Google Scholar] [CrossRef]
- Kotb, D.N.; Mahdy, W.K.; Mahmoud, M.S.; Khairy, R.M.M. Impact of co-existence of PMQR genes and QRDR mutations on fluoroquinolones resistance in Enterobacteriaceae strains isolated from community and hospital acquired UTIs. BMC Infect. Dis. 2019, 19, 979. [Google Scholar] [CrossRef] [PubMed]
- Ranjbar, R.; Tolon, S.S.; Sami, M.; Golmohammadi, R. Detection of Plasmid-Mediated qnr Genes Among the Clinical Quinolone-Resistant Escherichia coli Strains Isolated in Tehran, Iran. Open Microbiol. J. 2018, 12, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.J.; Tan, M.X.; Chen, M.I.; Tan, T.Y.; Koo, S.H.; Koong, A.Y.L.; Ng, L.P.; Hu, P.L.; Tan, K.T.; Moey, P.K.S.; et al. Interaction between Antibiotic Resistance, Resistance Genes, and Treatment Response for Urinary Tract Infections in Primary Care. J. Clin. Microbiol. 2019, 57. [Google Scholar] [CrossRef] [PubMed]
- Salah, F.D.; Soubeiga, S.T.; Ouattara, A.K.; Sadji, A.Y.; Metuor-Dabire, A.; Obiri-Yeboah, D.; Banla-Kere, A.; Karou, S.; Simpore, J. Distribution of quinolone resistance gene (qnr) in ESBL-producing Escherichia coli and Klebsiella spp. in Lomé, Togo. Antimicrob. Resist. Infect. Control. 2019, 8, 104. [Google Scholar] [CrossRef]
- Esmaeel, N.E.; Gerges, M.A.; Hosny, T.A.; Ali, A.R.; Gebriel, M.G. Detection of Chromosomal and Plasmid-Mediated Quinolone Resistance Among Escherichia coli Isolated from Urinary Tract Infection Cases; Zagazig University Hospitals, Egypt. Infect. Drug Resist. 2020, 13, 413–421. [Google Scholar] [CrossRef]
- Komp Lindgren, P.; Karlsson, A.; Hughes, D. Mutation rate and evolution of fluoroquinolone resistance in Escherichia coli isolates from patients with urinary tract infections. Antimicrob. Agents Chemother. 2003, 47, 3222–3232. [Google Scholar] [CrossRef]
- Seok, H.; Cha, M.K.; Kang, C.I.; Cho, S.Y.; Kim, S.H.; Ha, Y.E.; Chung, D.R.; Peck, K.R.; Song, J.H. Failure of Ciprofloxacin Therapy in the Treatment of Community-Acquired Acute Pyelonephritis caused by In-Vitro Susceptible Escherichia coli Strain Producing CTX-Type Extended-Spectrum β-Lactamase. Infect. Chemother. 2018, 50, 357–361. [Google Scholar] [CrossRef]
- Kang, C.I.; Kim, S.H.; Park, W.B.; Lee, K.D.; Kim, H.B.; Kim, E.C.; Oh, M.D.; Choe, K.W. Bloodstream infections due to extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae: Risk factors for mortality and treatment outcome, with special emphasis on antimicrobial therapy. Antimicrob. Agents Chemother. 2004, 48, 4574–4581. [Google Scholar] [CrossRef]
- Rhee, J.Y.; Kwon, K.T.; Ki, H.K.; Shin, S.Y.; Jung, D.S.; Chung, D.R.; Ha, B.C.; Peck, K.R.; Song, J.H. Scoring systems for prediction of mortality in patients with intensive care unit-acquired sepsis: A comparison of the Pitt bacteremia score and the Acute Physiology and Chronic Health Evaluation II scoring systems. Shock 2009, 31, 146–150. [Google Scholar] [CrossRef]


{kind=link}
| Variables | CIP-Susceptible MIC ≤ 0.25 (n = 282) | CIP-Non-Susceptible MIC = 0.5 or 1 (n = 52) | p Value |
|---|---|---|---|
| Sex, female | 227 (80.5) | 49 (94.2) | 0.016 |
| Age (years) | 69 (55–78) | 68.5 (51–77) | 0.363 |
| Patients with any comorbidity | |||
| Diabetes mellitus | 79 (28) | 15 (28.8) | 0.902 |
| Cardiovascular disease | 113 (40.1) | 18 (34.6) | 0.459 |
| Respiratory disease | 6 (2.1) | 0 (0) | 0.359 |
| Liver disease | 27 (9.6) | 10 (19.2) | 0.041 |
| Renal disease | 12 (4.3) | 6 (11.5) | 0.033 |
| Neurologic disease | 34 (12.1) | 6 (11.5) | 0.916 |
| Solid cancer | 46 (16.3) | 3 (5.8) | 0.048 |
| Connective tissue disease | 10 (3.5) | 2 (3.8) | 0.915 |
| Hematologic disease | 4 (1.4) | 1 (1.9) | 0.573 |
| Solid organ transplantation | 15 (5.3) | 6 (11.5) | 0.090 |
| CWI score | 1 (0–2) | 1 (0–2) | 0.558 |
| Pitt bacteremia score | 1 (0–2) | 1 (0–1) | 0.006 |
| Identified pathogen | |||
| Escherichia coli | 256 (90.8) | 48 (92.3) | 0.723 |
| Klebsiella pneumoniae | 26 (9.2) | 4 (7.7) | 0.723 |
| ESBL Producing organism | 10 (3.5) | 2 (3.8) | 0.915 |
| Empirical antibiotics | |||
| Appropriate antibiotics | 278 (98.6) | 33 (63.5) | <0.001 |
| Ciprofloxacin | 93 (33) | 18 (34.6) | 0.818 |
| Ceftriaxone | 114 (40.3) | 21 (40.4) | 0.996 |
| Piperacillin/tazobactam | 47 (16.7) | 9 (17.3) | 0.909 |
| Ertapenem | 5 (1.8) | 1 (1.9) | 0.940 |
| Others | 23 (8.2) | 3 (5.8) | 0.399 |
| Treatment duration | 13 (11–17) | 13 (10–15) | 0.119 |
| Follow up duration | 107 (63–141.50) | 100 (43.25–131.25) | 0.401 |
| Risk factors for recurrence | 75 (26.6) | 14 (26.9) | 0.961 |
| Previous UTIs history | 36 (12.8) | 8 (15.4) | 0.608 |
| Foreign body insertion | 14 (5) | 0 (0) | 0.101 |
| Urinary stone | 12 (4.3) | 0 (0) | 0.130 |
| Polycystic kidney disease | 1 (0.4) | 0 (0) | 0.844 |
| Urinary dysfunction | 12 (4.3) | 3 (5.8) | 0.628 |
| Kidney transplantation | 13 (4.6) | 6 (11.5) | 0.047 |
| Variables | CIP-Susceptible MIC ≤ 0.25 (n = 282) | CIP-Non-Susceptible MIC = 0.5 or 1 (n = 52) | p Value |
|---|---|---|---|
| Length of Hospital days | 6 (4–8) | 5 (4–6.75) | 0.055 |
| Recurrence within 4 weeks | 7 (2.5) | 2 (3.8) | 0.577 |
| Recurrence within 90 days | 23 (8.2) | 3 (5.8) | 0.399 |
| All-cause mortality | 3 (1.1) | 1 (1.9) | 0.494 |
| Prolonged bacteremia more than 1 week | 0 (0) | 0 (0) | 1 |
| Time to defervescence | 3 (2–4) | 2 (1–3) | 0.003 |
| Variables | HR (95% CI) | p Value |
|---|---|---|
| Sex, female | 1.391 (0.164–11.827) | 0.763 |
| Age | 1.025 (0.979–1.073) | 0.298 |
| CIP, non-susceptible | 0.888 (0.091–8.698) | 0.918 |
| ESBL producing organism | 1.488 (0.099–22.392) | 0.774 |
| CWI score | 0.904 (0.585–1.397) | 0.649 |
| Appropriate antibiotics | 0.235 (0.017–3.240) | 0.279 |
| Pitt bacteremia score | 1.267 (0.828–1.937) | 0.275 |
| Risk factors for recurrence | 0.356 (0.044–2.886) | 0.334 |
| Variables | HR (95% CI) | p Value |
|---|---|---|
| Sex, female | 0.910 (0.331–2.504) | 0.855 |
| Age | 0.979 (0.957–1.001) | 0.066 |
| CIP, non-susceptible | 0.365 (0.075–1.791) | 0.214 |
| ESBL producing organism | 1.538 (0.251–9.432) | 0.642 |
| CWI score | 1.030 (0.854–1.241) | 0.760 |
| Appropriate antibiotics | 0.316 (0.052–1.918) | 0.211 |
| Pitt bacteremia score | 0.847 (0.578–1.242) | 0.395 |
| Risk factors for recurrence | 2.370 (1.050–5.351) | 0.038 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, G.E.; Ko, J.-H.; Cho, S.Y.; Huh, H.J.; Baek, J.Y.; Ko, K.S.; Kang, C.-I.; Chung, D.R.; Peck, K.R. Clinical Impact of Revised Ciprofloxacin Breakpoint in Patients with Urinary Tract Infections by Enterobacteriaceae. Antibiotics 2021, 10, 469. https://doi.org/10.3390/antibiotics10040469
Park GE, Ko J-H, Cho SY, Huh HJ, Baek JY, Ko KS, Kang C-I, Chung DR, Peck KR. Clinical Impact of Revised Ciprofloxacin Breakpoint in Patients with Urinary Tract Infections by Enterobacteriaceae. Antibiotics. 2021; 10(4):469. https://doi.org/10.3390/antibiotics10040469
Chicago/Turabian StylePark, Ga Eun, Jae-Hoon Ko, Sun Young Cho, Hee Jae Huh, Jin Yang Baek, Kwan Soo Ko, Cheol-In Kang, Doo Ryeon Chung, and Kyong Ran Peck. 2021. "Clinical Impact of Revised Ciprofloxacin Breakpoint in Patients with Urinary Tract Infections by Enterobacteriaceae" Antibiotics 10, no. 4: 469. https://doi.org/10.3390/antibiotics10040469
APA StylePark, G. E., Ko, J. -H., Cho, S. Y., Huh, H. J., Baek, J. Y., Ko, K. S., Kang, C. -I., Chung, D. R., & Peck, K. R. (2021). Clinical Impact of Revised Ciprofloxacin Breakpoint in Patients with Urinary Tract Infections by Enterobacteriaceae. Antibiotics, 10(4), 469. https://doi.org/10.3390/antibiotics10040469