
The Prevalence and Factors Associated with Prophylactic Antibiotic Use during Delivery: A Hospital-Based Retrospective Study in Palembang, Indonesia

 and
and
Abstract
:1. Introduction
2. Results
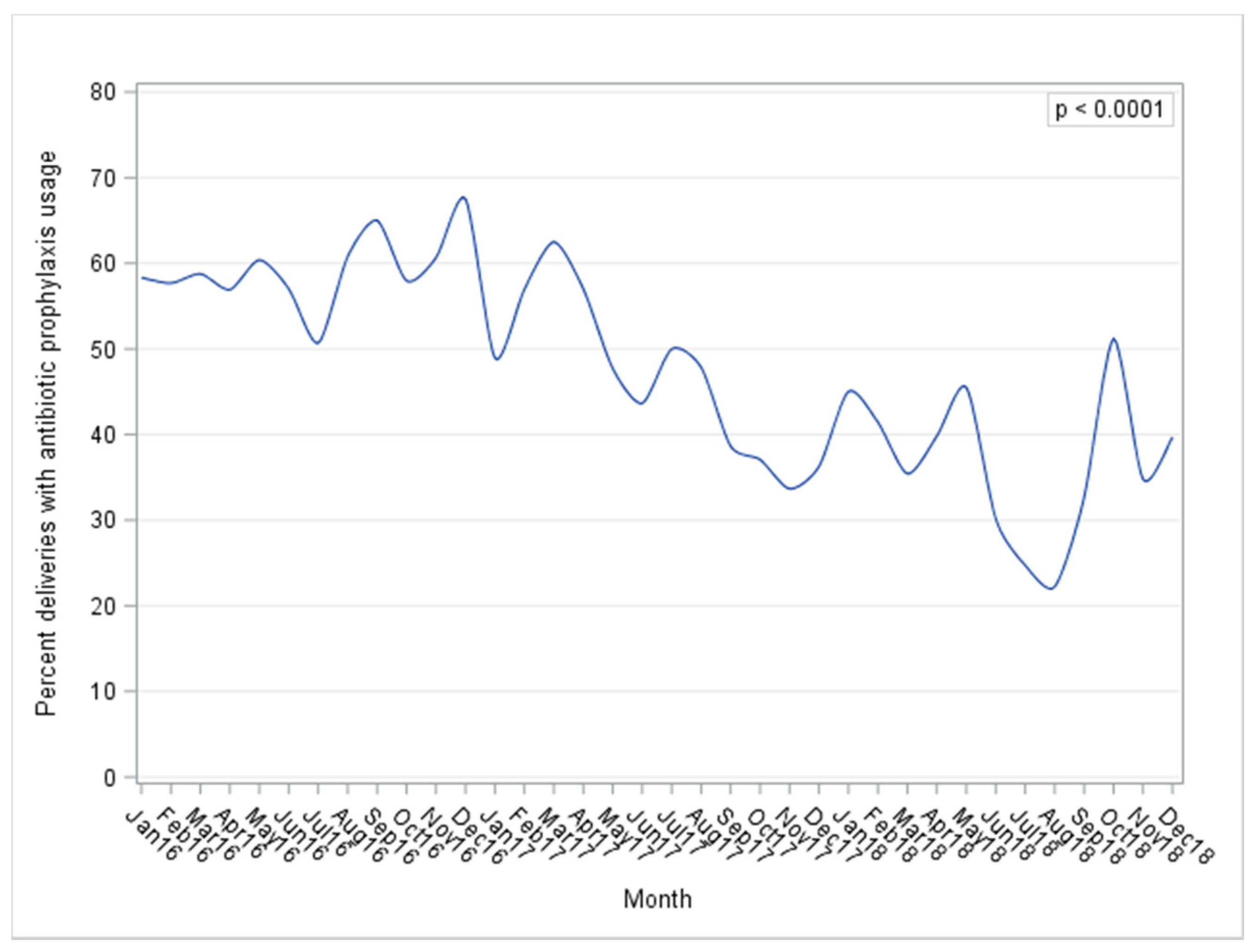
2.1. Prevalence of Prophylactic Antibiotic Usage
2.2. Adherence to Guidelines on Antibiotic Prophylaxis in Labor and Delivery
3. Discussion
4. Materials and Methods
4.1. Study Design and Study Population
4.2. Variables and Measurement
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, 323–333. [Google Scholar] [CrossRef] [Green Version]
- Hug, L.; Alexander, M.; You, D.; Alkema, L. National, regional, and global levels and trends in neonatal mortality between 1900 and 2017, with scenario-based projection to 2030; a systematic analysis. Lancet Glob. Health 2019, 7, e710–e720. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann-struzek, C.; Goldfarb, D.M.; Schlattmann, P.; Schlapbach, L.J.; Reinhart, K.; Kissoon, N. Review The global burden of paediatric and neonatal sepsis: A systematic review. Lancet 2018, 6, 223–230. [Google Scholar] [CrossRef]
- Van Dillen, J.; Zwart, J.; Schutte, J.; Van Roosmalen, J. Maternal sepsis: Epidemiology, etiology and outcome. Curr. Opin. Infect. Dis. 2010, 23, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Andergiorrgish, A.K.; Andemariam, M.; Temesghen, S.; Ogbai, L.; Ogbe, Z.; Zeng, L. Neonatal mortality and associated factors in the specialized neonatal care unit Asmara, Ertrea. BMC Public Health 2020, 20, 10. [Google Scholar]
- Brizuela, V.; Cuesta, C.; Bartolelli, G.; Abdosh, A.A.; Abou Malham, S.; Assarag, B.; Banegas, R.C.; Díaz, V.; El-Kak, F.; El Sheikh, M.; et al. Availibility of facility resources and services and infection-related maternal outcomes in the WHO Global Maternal Sepsis Study: A cross sectional study. Lancet Glob. Health 2021, 9, e1252–e1261. [Google Scholar] [CrossRef]
- National Population and Family Planning Board (BKKBN); Statistics Indonesia (BPS); Ministry of Health (Kemenkes); ICF. Indonesia Demographic and Health Survey 2017; BKKBN; BPS; Kemenkes; ICF: Jakarta, Indonesia, 2018.
- Soedarmono, Y.S.M. The Indonesian approach to reduce maternal mortality. ISBT Sci. Ser. 2017, 12, 272–280. [Google Scholar] [CrossRef]
- Sulistyono, A.; Joewono, H.T.; Mita, A. Maternal death at Dr. Soetomo general hospital surabaya—Indonesia accroding to McCarthy and Maine’s model 2013–2015. Eur. Asian J. Biosci. 2020, 14, 24231–24236. [Google Scholar]
- Schrag, S.; Gorwitz, R.; Fultz-Butts, K.; Schuchat, A. Prevention of perinatal group B streptococcal disease. Revised guidelines from CDC. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2010, 51, 1–53. [Google Scholar]
- Schrag, S.J.; Zywicki, S.S.; Farley, M.M.; Reingold, A.; Harrison, L.H.; Lefkowitz, L.B.; Hadler, J.L.; Danila, R.; Ciselak, P.R.; Schuchat, A. Group B Streptococcal Disease in the era of intrapartum antibiotic prophylaxis. N. Engl. J. Med. 2000, 342, 15–20. [Google Scholar] [CrossRef]
- Smaill, F.M.; Grivell, R.M. Antibiotic prophylaxis versus no prophylaxis for preventing infection after cesarean section. Cochrane Database Syst. Rev. 2014, 10, CD007482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenyon, S.; Boulvain, M.; Neilson, J.P. Antibiotics for preterm rupture of membranes. Cochrane Database Syst. Rev. 2013, 12, CD001058. [Google Scholar] [CrossRef] [PubMed]
- Le Doare, K.; O’Driscoll, M.; Turner, K.; Seedat, F.; Russell, N.J.; Seale, A.C.; Heath, P.T.; Lawn, J.E.; Baker, C.J.; Bartlett, L.; et al. Intrapartum Antibiotic Chemoprophylaxis Policies for the Prevention of Group B Streptococcal Disease Worldwide: Systematic Review. Clin. Infect. Dis. 2017, 65, S143–S151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, R.; Hasselquist, M.; Cardenas, V.; Zerr, D.M.; Kramer, J.; Zavitkovsky, A.; Schuchat, A. Introduction of the new Centers for Disease Control and Prevention group B streptococcal prevention guideline at a large West Coast health maintenance organization. Am. J. Obs. Gynecol. 2001, 184, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Sanneving, L.; Mahadik, K.; Santacatterina, M.; Dhaneria, S.; Stålsby Lundborg, C. Antibiotic prescribing in women during and after delivery in a non-teaching, tertiary care hospital in Ujjain, India: A prospective cross-sectional study. J. Pharm. Policy Pract. 2013, 6, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Mensah, K.B.; Opoku-Agyeman, K.; Ansah, C. Antibiotic use during pregnancy: A retrospective study of prescription patterns and birth outcomes at an antenatal clinic in rural Ghana. J. Pharm. Policy Pract. 2017, 10, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Jury, I.; Thompson, K.; Hirst, J.E. A scoping review of maternal antibiotic prophylaxis in low-and middle-income countries: Comparison to WHO recommendations for prevention and treatment of maternal peripartum infection. Int. J. Gynecol. Obs. 2021, 1–12. [Google Scholar] [CrossRef]
- Seedat, F.; Stinton, C.; Patterson, J.; Geppert, J.; Tan, B.; Robinson, E.R.; McCarthy, N.D.; Uthman, O.A.; Freeman, K.; Johnson, S.A.; et al. Adverse events in women and children who have received intrapartum antibiotic prophylaxis treatment: A systematic review. BMC Pregnancy Childbirth 2017, 17, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tejada, B.M. Antibiotic use and misuse during pregnancy and delivery: Benefits and risks. Int. J. Environ. Res. Public Health 2014, 11, 7993–8009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, A.; Kohli, J.K. Antibiotic prophylaxis in cesarean section causing anaphylaxis and intrauterine fetal death. J. Obstet. Gynaecol. Res. 2008, 34, 252–254. [Google Scholar] [CrossRef]
- Kenyon, S.; Pike, K.; Jones, D.R.; Brocklehurst, P.; Marlow, N.; Salt, A.; Taylor, D.J. Childhood outcomes after prescription of antibiotics to pregnant women with spontaneous preterm labour: 7-year follow-up of the ORACLE II trial. Lancet 2008, 372, 1319–1327. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists Use of prophylactic antibioitcs in labor adn delivery. Obstet. Gynecol. 2018, 132, 103–119.
- World Health Organziation. WHO Recommendations for Prevention and Treatment of Maternal Peripartum Infections; World Health Organization: Geneva, Switzerland, 2015; ISBN 9789241549363. [Google Scholar]
- Kotwani, A.; Holloway, K. Trends in antibiotic use among outpatients in New Delhi, India. BMC Infect. Dis. 2011, 11, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [Green Version]
- Stokholm, J.; Schjørring, S.; Pedersen, L.; Bischoff, A.L.; Følsgaard, N.; Carson, C.G.; Chawes, B.L.K.; Bønnelykke, K.; Mølgaard, A.; Krogfelt, K.A.; et al. Prevalence and predictors of antibiotic administration during pregnancy and birth. PLoS ONE 2013, 8, e82932. [Google Scholar] [CrossRef] [PubMed]
- Koebnick, C.; Tartof, S.Y.; Sidell, M.A.; Rozema, E.; Chung, J.; Chiu, V.Y.; Taylor, Z.W.; Xiang, A.H.; Getahun, D. Effect of In-Utero Antibiotic Exposure on Childhood Outcomes: Methods and Baseline Data of the Fetal Antibiotic EXposure (FAX) Cohort Study. JMIR Res. Protoc. 2019, 8, e12065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Persaud, R.R.; Azad, M.B.; Chari, R.S.; Sears, M.R.; Becker, A.B.; Kozyrskyj, A.L.; the CHILD Study Investigators. Perinatal antibiotic exposure of neonates in Canada and associated risk factors: A population-based study. J. Matern. Fetal Neonatal Med. 2015, 28, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Quinn, G.P.; Block, R.G.; Clayman, M.L.; Kelvin, J.; Arvey, S.R.; Lee, J.H.; Reinecke, J.; Sehovic, I.; Jacobsen, P.B.; Reed, D.; et al. If you did not document it, it did not happen: Rates of documentation of discussion of infertility risk in adolescent and young adult oncology patients’ medical records. J. Oncol. Pract. 2015, 11, 137–144. [Google Scholar] [CrossRef]
- Mishra, A.K.; Bhattarai, S.; Bhurtel, P.; Bista, N.R.; Shrestha, P.; Thakali, K.; Banthia, P.; Pathak, S.R. Need for improvement of medical records. J. Nepal Med. Assoc. 2009, 48, 103–106. [Google Scholar] [CrossRef]
- Arnold, L.B.; Usery, J.B.; Finch, C.K.; Wallace, J.L.; Deaton, P.R.; Self, T.H. Inadequate Documentation of Asthma Management in Hospitalized Adult Patients. South. Med. J. 2009, 102, 510–514. [Google Scholar] [CrossRef]
- Adane, K.; Muluye, D.; Abebe, M. Processing medical data: A systematic review. Arch. Public Health 2013, 71, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Departemen Kebidanan & Penyakit Kandungan. Panduan Pelayanan Klinis Kebidanan dan Penyakit Kandungan; RSUP dr. Mohammad Hoesin Palembang: Palembang, Indonesia, 2012. [Google Scholar]
- Departemen/SMF Keshatan Anak; Panduan Praktik Klinik (PPK): Palembang, Indonesia, 2014.
- Perkumpulan Obstetri Ginekologi Indonesia Panduan Antibiotika. Profilaksis Pada Pembedahan Obstetri dan Ginekologi; Paraton, H., Ed.; Perkumpulan Obstetri Ginekologi Indonesia: Jakarta, Indonesia, 2013. [Google Scholar]
- Perkumpulan Obstetri Ginekologi Indonesia. Pedoman Nasional Pelayanan Kedokteran KETUBAN PECAH DINI; Perkumpulan Obstetri dan Ginekologi Indonesia, Himpunan Kedokteran Fetomaternal: Jakarta, Indonesia, 2016. [Google Scholar]
- National Clinic Training Network, Indonesian Pediatric Society IS of O and G. Pelayanan Obstetri Dan Neonatal Emergensi Komprehensif Ponek; The Republic of Indonesia Ministry of Health: Jakarta, Indonesia, 2008.
- Thomson, A.J.; Ramsay, J.E. Antepartum haemorrhage. R. Coll. Obstet. Gynecol. 2011, 63, 1–23. [Google Scholar]
- Thomson, A.J. Care of Women Presenting with Suspected Preterm Prelabour Rupture of Membranes from 24+0 Weeks of Gestation. BJOG Int. J. Obstet. Gynaecol. 2019, 126, e152–e166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organizaiton. Pocket Book of Hospital Care for Children, 2nd ed.; World Health Organization: Geneva, Switzerland, 2013; ISBN 9789241548373. [Google Scholar]
- Homer, C.S.E.; Scarf, V.; Catling, C.; Davis, D. Culture-based versus risk-based screening for the prevention of group B streptococcal disease in newborns: A review of national guidelines. Women Birth 2014, 27, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Kurz, E.; Davis, D. Routine culture-based screening versus risk-based management for the prevention of early-onset group B streptococcus disease in the neonate: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 206–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kardana, I.M. Incidence and factors associated with mortality of neonatal sepsis. Paediatr. Indones. 2017, 51, 144. [Google Scholar] [CrossRef] [Green Version]
- Hasibuan, B.S. Comparison of microbial pattern in early and late onset neonatal sepsis in referral center Haji Adam Malik hospital Medan Indonesia. IOP Conf. Ser. Earth Environ. Sci. 2018, 125, 3–8. [Google Scholar] [CrossRef]
- Tan, K.W.; Tay, L.; Lin, R.; Daniel, M.; Bhavani, S.; Lim, S.H. Group B Streptococcal Septicaemia/Meningitis in Neonates in a Singapore Teaching Hospital. Aust. N. Z. J. Obstet. Gynaecol. 1998, 38, 418–423. [Google Scholar] [CrossRef]
- Subramaniam, A.; Abramovici, A.; Andrews, W.W.; Tita, A.T. Antimicrobials for Preterm Birth Prevention: An Overview. Infect. Dis. Obstet. Gynecol. 2012, 2012, 157159. [Google Scholar] [CrossRef]
- Flenady, V.; Hawley, G.; Stock, O.M.; Kenyon, S.; Badawi, N. Prophylactic antibiotics for inhibiting preterm labour with intact membranes. Cochrane Database Syst. Rev. 2013, 12, CD000246. [Google Scholar] [CrossRef] [Green Version]
- Gnann, J.W.; Goetter, W.E.; Elliott, A.M.; Cobbs, C.G. Ceftriaxone: In Vitro Studies and Clinical Evaluation. Antimicrob. AGENTS Chemother. 1982, 22, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paccione, K.A.; Wiesenfeld, H.C. Guideline Adherence for Intrapartum Group B Streptococci Prophylaxis in Penicillin-Allergic Patients. Infect. Dis. Obstet. Gynecol. 2013, 2013, 917304. [Google Scholar] [CrossRef] [PubMed]
- Abdel Jalil, M.H.; Abu Hammour, K.; Alsous, M.; Hadadden, R.; Awad, W.; Bakri, F.; Fram, K. Noncompliance with surgical antimicrobial prophylaxis guidelines: A Jordanian experience in cesarean deliveries. Am. J. Infect. Control 2018, 46, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Radyowijati, A.; Haak, H. Improving antibiotic use in low-income countries: An overview of evidence on determinants. Soc. Sci. Med. 2003, 57, 733–744. [Google Scholar] [CrossRef]
- Mol, P.G.M.; Wieringa, J.E.; NannanPanday, P.V.; Gans, R.O.B.; Degener, J.E.; Laseur, M.; Haaijer-Ruskamp, F.M. Improving compliance with hospital antibiotic guidelines: A time-series intervention analysis. J. Antimicrob. Chemother. 2005, 55, 550–557. [Google Scholar] [CrossRef] [Green Version]
- Mol, P.G.M.; Rutten, W.J.M.J.; Gans, R.O.B.; Degener, J.E.; Haaijer-Ruskamp, F.M. Adherence Barriers to Antimicrobial Treatment Guidelines in Teaching Hospital, the Netherlands. Emerg. Infect. Dis. 2004, 10, 522. [Google Scholar] [CrossRef] [Green Version]
- Epstein, A.M.; Begg, C.B.; Mcneil, B.J. The Effects of Physicians’ Training and Personality on Test Ordering for Ambulatory Patients. AJPH 1984, 74, 271. [Google Scholar] [CrossRef] [Green Version]
- Henriet, L.; Kaminski, M. Impact of induced abortions on subsequent pregnancy outcome: The 1995 French national perinatal survey. Br. J. Obstet. Gynaecol. 2001, 108, 1036–1042. [Google Scholar]
- Thom, D.H.; Nelson, L.M.; Vaughan, T.L. Spontaneous abortion and subsequent adverse birth outcomes. Am. J. Obstet. Gynecol. 1992, 166, 111–116. [Google Scholar] [CrossRef]
- Yang, J.; Wang, Y.; Wang, X.Y.; Zhao, Y.Y.; Wang, J.; Zhao, Y.Y. Adverse Pregnancy Outcomes of Patients with History of First-Trimester Recurrent Spontaneous Abortion. Biol. Med. Res. Int. 2017, 2017, 4359424. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | 2016 | 2017 | 2018 | Total | p a |
|---|---|---|---|---|---|
| n = 1087 | n = 1227 | n = 1343 | n = 3657 | ||
| Maternal age group | |||||
| <17 years old | 5 (0.5) | 6 (0.5) | 12(0.9) | 23 (0.6) | 0.21 |
| 17–35 years old | 851 (78.3) | 979 (79.8) | 1027 (76.5) | 2857 (78.1) | |
| >35 years old | 231 (21.3) | 242 (19.7) | 304 (22.6) | 777 (21.3) | |
| Mother Education | |||||
| No formal education | 3 (0.3) | 23 (1.9) | 7 (0.5) | 33 (0.9) | <0.0001 |
| Less than high school | 72 (6.7) | 120 (9.8) | 193 (14.4) | 385 (10.5) | |
| High school graduate | 895 (83.2) | 898 (73.2) | 871 (64.9) | 2664 (72.9) | |
| College or higher | 106 (9.8) | 130 (10.6) | 192 (14.3) | 428 (11.7) | |
| Missing b | 11 (1.0) | 56 (4.6) | 80 (5.9) | 147 (4.0) | |
| Mother’s place of residence | |||||
| Resident | 693 (63.8) | 770 (62.6) | 870 (64.8) | 2333 (63.8) | 0.54 |
| Non-resident | 393 (36.2) | 456 (37.2) | 470 (35.0) | 1319 (36.1) | |
| Missing b | 1(0.1) | 1 (0.1) | 3 (0.2) | 5 (0.1) | |
| Birth attendant | |||||
| Ob/Gyn | 193 (17.8) | 177 (14.4) | 172 (12.8) | 542 (14.8) | 0.003 |
| Resident | 894 (82.2) | 1050 (85.6) | 1171 (87.2) | 3115 (85.2) | |
| Obstetric factors | |||||
| Parity ≥ 5 | 15 (1.4) | 30 (2.4) | 25 (1.9) | 70 (1.9) | 0.17 |
| Previous abortion > 1 | 34 (3.1) | 43 (3.5) | 23 (1.7) | 100 (2.7) | 0.01 |
| Gestational age < 37 weeks | 297 (27.3) | 239 (19.5) | 300 (22.3) | 836 (22.9) | <0.0001 |
| Multiple birth | 33 (3.0) | 21 (1.7) | 32 (2.4) | 86 (2.4) | 0.11 |
| Mode of delivery | |||||
| C-section | 486 (44.7) | 491 (40.02) | 658 (49.0) | 1635 (44.7) | 0.0004 |
| Spontaneous vaginal delivery | 575 (52.9) | 699 (57.0) | 648 (48.3) | 1922 (52.6) | |
| Vacuum extraction | 11 (1.0) | 14 (1.1) | 21 (1.6) | 46 (1.3) | |
| Forceps extraction | 15 (1.4) | 23 (1.9) | 16 (1.2) | 54 (1.5) | |
| Intrapartum temperature ≥ 38 °C | 20 (1.8) | 17 (1.4) | 67 (5.0) | 104 (2.8) | <0.0001 |
| PROM | 374 (34.4) | 349 (28.4) | 312 (23.2) | 1035 (28.3) | <0.0001 |
| Maternal leukocyte count | |||||
| >15,000/mm3 | 316 (29.1) | 333 (27.1) | 354 (21.2) | 1003 (27.4) | 0.25 |
| <15,000/mm3 | 674 (62.0) | 753 (61.4) | 852 (58.3) | 2279 (62.3) | |
| Missing b | 97 (8.9) | 141 (11.5) | 137 (20.6) | 375 (10.3) | |
| Antepartum hemorrhage | 22 (2.0) | 24 (2.0) | 16 (1.2) | 62 (1.7) | 0.2 |
| Foul-smelling amnion fluid | 7 (0.6) | 17 (1.4) | 11 (0.8) | 35 (1.0) | 0.15 |
| Variables | Antibiotic Prophylaxis | OR (95% CI) | p a | aOR (95%CI) † | p a | |
|---|---|---|---|---|---|---|
| Yes | No | |||||
| (n = 1721) | (n = 1936) | |||||
| Maternal age group | ||||||
| <17 years old | 9 (0.5) | 14 (0.7) | 0.75 (0.32–1.72) | 0.13 | 1.04 (0.32–3.35) | 0.34 |
| 17–35 years old | 1323 (76.9) | 1534 (79.2) | Ref | Ref | ||
| >35 years old | 389 (22.6) | 388 (20.0) | 1.16 (1.00–1.36) | 1.17 (0.94–1.48) | ||
| Mother Education b | ||||||
| No formal education | 13 (0.8) | 20 (1.1) | 0.84 (0.41–1.75) | 0.009 | 0.83 (0.30–2.36) | 0.01 |
| Less than high school | 159 (9.6) | 226 (12.2) | 0.92 (0.68–1.22) | 0.91 (0.61–1.37) | ||
| High school graduate | 1298 (78.5) | 1366 (73.6) | 1.23 (0.99–1.54) | 1.39 (1.04–1.86) | ||
| College or higher | 184 (11.1) | 244 (13.2) | Ref | Ref | ||
| Mother’s place of residence c | ||||||
| Resident | 1055 (61.3) | 654 (33.9) | Ref | 0.003 | Ref | 0.08 |
| Non-resident | 666 (38.7) | 1278 (66.2) | 1.23 (1.08–1.41) | 1.19 (0.98–1.45) | ||
| Birth attendant | ||||||
| Ob/Gyn | 298 (17.3) | 244 (12.6) | 1.45 (1.21–1.75) | <0.0001 | 1.29 (1.001–1.66) | 0.049 |
| Resident | 1423 (82.7) | 1692 (87.4) | Ref | |||
| Parity | ||||||
| <5 | 1691 (98.3) | 1896 (98.0) | Ref | 0.48 | -- | -- |
| ≥5 | 30 (1.7) | 40 (2.1) | 0.84 (0.52–1.36) | |||
| Previous abortion | ||||||
| ≤1 | 1663 (96.6) | 1894 (97.8) | Ref | 0.03 | Ref | 0.02 |
| >1 | 58 (3.4) | 42 (2.2) | 1.57 (1.05–2.35) | 1.88 (1.11–3.17) | ||
| Gestational age < 37 weeks | 450 (26.2) | 384 (19.9) | 1.42 (1.21–1.66) | <0.0001 | 1.13 (0.89–1.41) | 0.31 |
| Multiple birth | 41 (2.4) | 45 (2.3) | 1.03 (0.69–1.57) | 0.91 | -- | -- |
| Mode of delivery | ||||||
| C-section | 1040 (60.4) | 595 (30.7) | 3.45 (3.01–3.96) | <0.0001 | 7.96 (6.40–9.91) | <0.0001 |
| Spontaneous vaginal delivery | 646 (37.5) | 1276 (65.9) | Ref | Ref | ||
| Vacuum extraction | 16 (0.9) | 30 (1.6) | 1.05 (0.57–1.95) | 1.54 (0.60–3.92) | ||
| Forceps extraction | 19 (1.1) | 35 (1.8) | 1.07 (0.61–1.89) | 2.21 (1.00–4.85) | ||
| Intrapartum temperature ≥ 38 °C | 48 (2.8) | 56 (2.9) | 0.96 (0.65–1.42) | 0.85 | 0.71 (0.43–1.17) | 0.18 |
| PROM | 991 (57.6) | 44 (2.3) | 58.37 (42.65–79.89) | <0.0001 | 117.78 (83.28–166.58) | <0.0001 |
| Maternal leukocyte count | 474 (28.0) d | 528 (28.1) e | 0.99 (0.84–1.17) | 0.93 | -- | -- |
| >15,000/mm3 | ||||||
| Antepartum hemorrhage | 62 (3.6) | 0 (0) | 145.87 (8.82–>999) | 0.0005 | 309.93 (18.17–>999) | <0.0001 |
| Foul-smelling amnion fluid | 17 (1.0) | 18 (0.9) | 1.06 (0.54–2.07) | 0.86 | -- | -- |
| Variables | Adherence | Non-Adherence | OR (95% CI) | p a | aOR (95% CI) † |
|---|---|---|---|---|---|
| (n = 2519) | (n = 1138) | ||||
| Year of admission | |||||
| 2016 | 839 (33.3) | 248 (21.8) | Ref | <0.0001 | Ref |
| 2017 | 873 (34.7) | 354 (31.1) | 0.73 (0.60–0.88) | 0.57 (0.45–0.74) | |
| 2018 | 807 (32.0) | 536 (47.1) | 0.45 (0.37–0.55) | 0.39 (0.31–0.50) | |
| Maternal age group | |||||
| <17 years old | 13 (0.5) | 10 (0.9) | 0.58 (0.25–1.33) | 0.39 | -- |
| 17–35 years old | 1976 (78.4) | 881 (77.4) | Ref | ||
| >35 years old | 530 (21.1) | 247 (21.7) | 0.96 (0.81–1.14) | ||
| Mother Education b | |||||
| No formal education | 23 (1.0) | 10 (0.9) | 1.15 (0.54–2.49) | 0.04 | 1.04 (0.34–3.11) |
| Less than high school | 244 (10.1) | 141 (12.9) | 0.87 (0.65–1.16) | 0.94 (0.63–1.39) | |
| High school graduate | 1867 (77.2) | 796 (73.0) | 1.18 (0.95–1.46) | 1.19 (0.89–1.58) | |
| College or higher | 285 (11.8) | 143 (13.1) | Ref | Ref | |
| Mother’s place of residence c | |||||
| Resident | 1628 (64.8) | 705 (62.0) | Ref | 0.1 | 0.95 (0.78–112) |
| Non-resident | 886 (35.2) | 433 (38.0) | 0.89 (0.77–1.02) | Ref | |
| Birth attendant | |||||
| Ob/Gyn | 375 (14.9) | 167 (14.7) | 1.02 (0.84–1.24) | 0.87 | -- |
| Resident | 2144 (85.1) | 971 (85.3) | Ref | ||
| Parity | |||||
| <5 | 2467 (98.1) | 1116 (98.1) | Ref | 0.95 | -- |
| ≥5 | 48 (1.9) | 22 (1.9) | 0.99 (0.59–1.64) | ||
| Previous abortion | |||||
| ≤1 | 2449 (97.2) | 1082 (97.4) | Ref | 0.81 | -- |
| >1 | 70 (2.8) | 30 (2.6) | 1.06 (0.68–1.63) | ||
| Gestational age < 37 weeks | 450 (17.9) | 386 (33.9) | 0.42 (0.36–0.50) | <0.0001 | 0.37 (0.25–0.54) |
| Multiple birth | 52 (2.1) | 33 (3.5) | 0.68 (0.44–1.06) | 0.09 | 1.66 (0.90–3.03) |
| Mode of delivery | |||||
| C-section | 1040 (41.3) | 595 (52.3) | 0.63 (0.54–0.72) | <0.0001 | 1.34 (0.09–2.00) |
| Spontaneous vaginal delivery | 1414 (56.1) | 508 (44.6) | Ref | Ref | |
| Vacuum extraction | 33 (1.3) | 13 (1.1) | 0.91 (0.48–1.75) | 0.88 (0.37–2.05) | |
| Forceps extraction | 32 (1.3) | 22 (1.9) | 0.52 (0.30–0.91) | 0.41 (0.19–0.87) | |
| Intrapartum temperature ≥ 38 °C | 48 (1.9) | 56 (4.9) | 0.38 (0.25–0.56) | <0.0001 | 0.52 (0.29–0.95) |
| PROM | 991 (39.3) | 44 (3.9) | 16.13 (11.81–22.03) | <0.0001 | 27.88 (17.17–45.26) |
| Maternal leukocyte count > 15,000/mm3 | 549 (20.9) d | 482 (28.0) e | 0.34 (0.29–0.41) | <0.0001 | 0.23 (0.18–0.28) |
| Antepartum hemorrhage | 62 (2.5) | 0 (0) | 3.31 (1.42–7.70) | 0.006 | 194.81 (11.46–>999.99) |
| Foul-smelling amnion fluid | 28 (1.0) | 7 (0.6) | 57.92 (3.50–958.43) | 0.005 | 3.65 (1.26–10.58) |
| Numbers of indications | |||||
| for antibiotic prophylaxis in a patient | |||||
| None | 873 (34.7) | 312 (33.3) | Ref | <0.0001 | Ref |
| One indication | 924 (36.7) | 638 (56.1) | 0.52 (0.44–0.61) | 0.36 (0.24–0.54) | |
| Two indications | 612 (24.3) | 180 (15.8) | 1.22 (0.98–1.50) | 0.64 (0.31–1.29) | |
| Three or more indications | 110 (4.4) | 8 (0.7) | 4.91 (2.37–10.19) | 0.63 (0.17–2.29) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karmila, A.; Zulkarnain, M.; Martadiansyah, A.; Mirani, P.; Bernolian, N.; Gardiner, J.C.; Zhang, L. The Prevalence and Factors Associated with Prophylactic Antibiotic Use during Delivery: A Hospital-Based Retrospective Study in Palembang, Indonesia. Antibiotics 2021, 10, 1004. https://doi.org/10.3390/antibiotics10081004
Karmila A, Zulkarnain M, Martadiansyah A, Mirani P, Bernolian N, Gardiner JC, Zhang L. The Prevalence and Factors Associated with Prophylactic Antibiotic Use during Delivery: A Hospital-Based Retrospective Study in Palembang, Indonesia. Antibiotics. 2021; 10(8):1004. https://doi.org/10.3390/antibiotics10081004
Chicago/Turabian StyleKarmila, Ariesti, Mohammad Zulkarnain, Abarham Martadiansyah, Putri Mirani, Nuswil Bernolian, Joseph C. Gardiner, and Lixin Zhang. 2021. "The Prevalence and Factors Associated with Prophylactic Antibiotic Use during Delivery: A Hospital-Based Retrospective Study in Palembang, Indonesia" Antibiotics 10, no. 8: 1004. https://doi.org/10.3390/antibiotics10081004
APA StyleKarmila, A., Zulkarnain, M., Martadiansyah, A., Mirani, P., Bernolian, N., Gardiner, J. C., & Zhang, L. (2021). The Prevalence and Factors Associated with Prophylactic Antibiotic Use during Delivery: A Hospital-Based Retrospective Study in Palembang, Indonesia. Antibiotics, 10(8), 1004. https://doi.org/10.3390/antibiotics10081004