
NDM Production as a Dominant Feature in Carbapenem-Resistant Enterobacteriaceae Isolates from a Tertiary Care Hospital

 , ,
, ,
Abstract
:1. Introduction
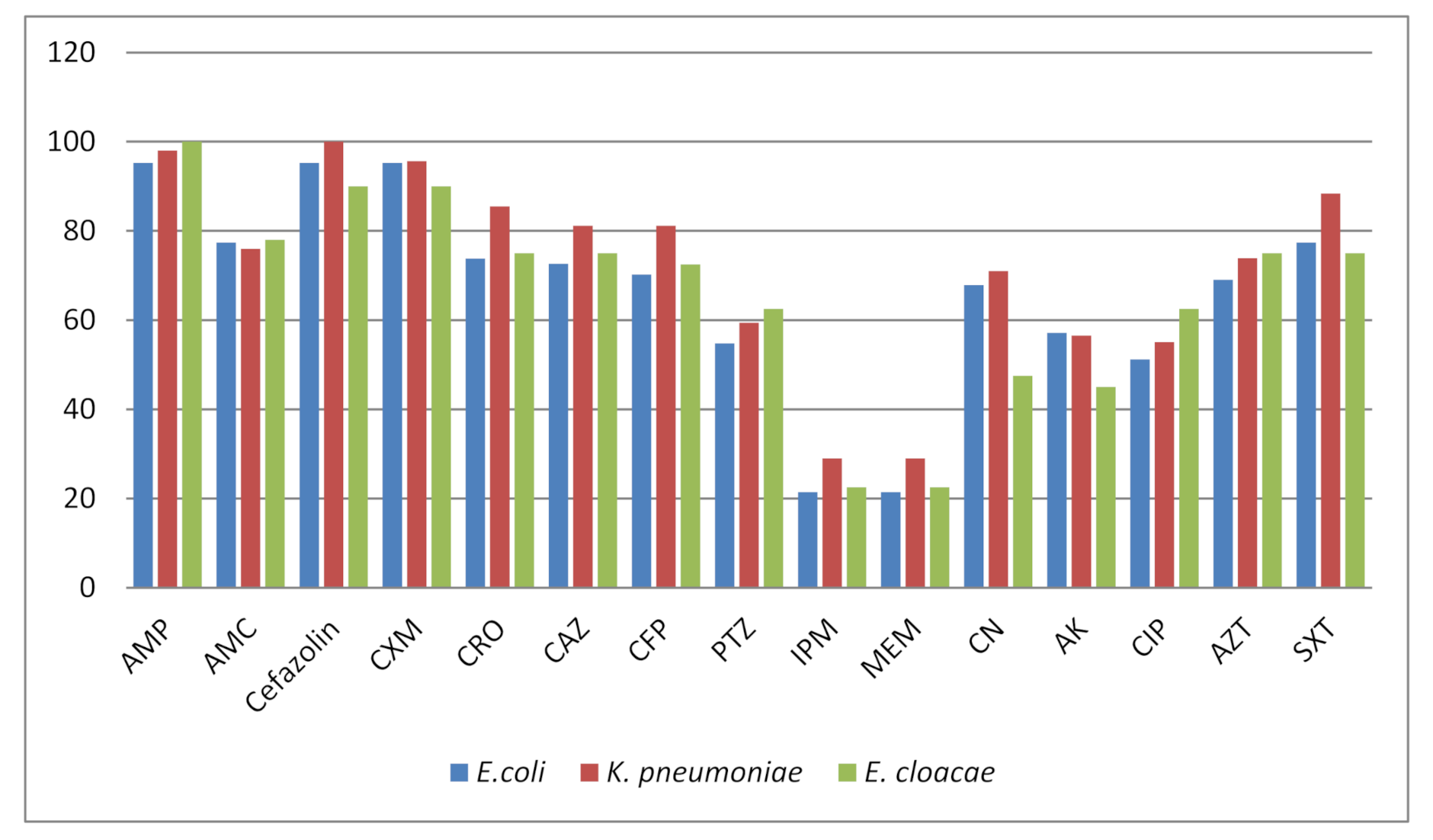
2. Results
3. Discussion
4. Materials and Methods
4.1. Setting
4.2. Sample Size and Collection
4.3. Identification of the Isolates
4.4. Manual PCR Method
4.5. Plasmid Extraction and Conjugation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, M.H.; Chan, E.W.; Chen, S. Isolation of carbapenem-resistant Pseudomonas spp. from food. J. Glob. Antimicrob. Resist. 2015, 5, 109–114. [Google Scholar] [CrossRef]
- Doi, Y. Treatment options for carbapenem-resistant gram-negative bacterial infections treatment options for carbapenem-resistant gram-negative bacterial infections. Clin. Infect. Dis. 2018, 69, S565–S575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marco, C.; Alberto, A.; Tommaso, G.; Teresa, S.; Marzia, L.F.; Carla, F.; Mirandola, W.; Gargiulo, R.; Barozzi, A.; Mauri, C.; et al. Multicenter evaluation of the RAPIDEC! CARBA NP test for rapid screening of carbapenemase-producing Enterobacteriaceae and Gram-negative nonfermenters from clinical specimens. Diagn. Microbiol. Infect. Dis. 2017, 88, 207–213. [Google Scholar] [CrossRef]
- Nordmann, P.; Poirel, L.; Walsh, T.R.; Livermore, D.M. The emerging NDM carbapenemases. Trends. Microbiol. 2011, 19, 588–595. [Google Scholar] [CrossRef]
- Rossolini, G.M. Extensively drug-resistant carbapenemase-producing Enterobacteriaceae: An emerging challenge for clinicians and healthcare systems. J. Intern. Med. 2015, 277, 528–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suwantarat, N.; Carroll, K.C. Epidemiology and molecular characterization of multidrug-resistant Gram-negative bacteria in Southeast Asia. Antimicrob. Resist. Infect. Control 2016, 4, 15. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Poirel, L. Epidemiology and diagnostics of carbapenem resistance in gram-negative bacteria. Clin. Infect. Dis. 2019, 69, S521–S528. [Google Scholar] [CrossRef] [Green Version]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of carbapenem-resistant Enterobacteriaceae: The impact and evolution of a global menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Ye, H. Clinical and mortality risk factors in bloodstream infections with carbapenem-resistant Enterobacteriaceae. Can. J. Infect. Dis. Med. Microbiol. 2017, 6212910. [Google Scholar] [CrossRef] [Green Version]
- Mitra, S.; Mukherjee, S.; Naha, S.; Chattopadhyay, P.; Dutta, S.; Basu, S. Evaluation of co-transfer of plasmid-mediated fluoroquinolone resistance genes and blaNDM gene in Enterobacteriaceae causing neonatal septicaemia. Antimicrob. Resist. Infect. Control 2019, 8. [Google Scholar] [CrossRef]
- Rao, M.R.; Chandrashaker, P.; Mahale, R.P.; Shivappa, S.G.; Gowda, R.S.; Chitharagi, V.B. Detection of carbapenemase production in Enterobacteriaceae and Pseudomonas species by carbapenemase Nordmann–Poirel test. J. Lab. Physicians 2019, 11, 107–110. [Google Scholar] [CrossRef]
- Clinical & Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing; 28th Informational Supplement. M100-S28; CLSI: Wayne, PA, USA, 2018. [Google Scholar]
- Zhang, Y.; Wang, Q.; Yin, Y.; Chen, H.; Jin, L.; Gu, B.; Xie, L.; Yang, C.; Ma, X.; Li, H.; et al. Epidemiology of carbapenem-resistant Enterobacteriaceae infections: Report from the China CRE Network. Antimicrob. Agents Chemother. 2018, 62, e01882-17. [Google Scholar] [CrossRef] [Green Version]
- Dortet, L.; Poirel, L.; Nordmann, P. Worldwide dissemination of the NDM-type carbapenemases in Gram-negative bacteria. BioMed Res. Int. 2014, 2014, 249856. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Fang, L.; Fu, Y.; Du, X.; Shen, Y.; Yu, Y. Dissemination of NDM-1-producing Enterobacteriaceae mediated by the IncX3-type plasmid. PLoS ONE 2012, 5, e0129454. [Google Scholar] [CrossRef] [Green Version]
- Abrar, S.; Hussain, S.; Khan, R.A.; Ul-Ain, N.; Haider, H.; Riaz, S. Prevalence of extended-spectrum-β-lactamase-producing Enterobacteriaceae: First systematic meta-analysis report from Pakistan. Antimicrob. Resist. Infect. Control 2018, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Garg, A.; Garg, J.; Upadhyay, G.C.; Agarwal, A.; Bhattacharjee, A. Evaluation of the Rapidec Carba NP test kit for detection of carbapenemase-producing Gram-Negative Bacteria. Antimicrob. Agents Chemother. 2015, 59, 7870–7872. [Google Scholar] [CrossRef] [Green Version]
- Masseron, A.; Poirel, L.; Ali, B.J.; Syed, M.A.; Nordmann, P. Molecular characterization of multidrug-resistance in Gram-negative bacteria from the Peshawar teaching hospital, Pakistan. New Microbes New Infect. 2019, 32, 100605. [Google Scholar] [CrossRef]
- Kaase, M.; Nordmann, P.; Wichelhaus, T.A.; Gatermann, S.G.; Bonnin, R.A.; Poirel, L. NDM-2 carbapenemase in Acinetobacter baumannii from Egypt. J. Antimicrob. Chemother. 2011, 66, 1260–1262. [Google Scholar] [CrossRef] [Green Version]
- Manenzhe, R.I.; Zar, H.J.; Nicol, M.P.; Kaba, M. The spread of carbapenemase-producing bacteria in Africa: A systematic review. J. Antimicrob. Chemother. 2015, 70, 23–40. [Google Scholar] [CrossRef] [Green Version]
- Pandya, N.P.; Prajapati, S.B.; Mehta, S.J.; Kikani, K.M.; Joshi, P.J. Evaluation of various methods for detection of metallo-β-lactamase (MBL) production in gram-negative bacilli. Int. J. Biol. Med. Res. 2011, 2, 775–777. [Google Scholar]
- Wolter, D.J.; Khalaf, N.; Robledo, I.E.; Vázquez, G.J.; Santé, M.I.; Aquino, E.E.; Goering, R.V.; Hanson, N.D. Surveillance of carbapenem-resistant Pseudomonas aeruginosa isolates from Puerto Rican Medical Center Hospitals: Dissemination of KPC and IMP-18 ß-lactamases. Antimicrob. Agents Chemother. 2009, 53, 1660–1664. [Google Scholar] [CrossRef] [Green Version]
- Borgia, S.; Lastovetska, O.; Richardson, D.; Eshaghi, A.; Xiong, J.; Chung, C.; Baqi, M.; McGeer, A.; Ricci, G.; Sawicki, R.; et al. Outbreak of carbapenem-resistant Enterobacteriaceae containing blaNDM-1, Ontario, Canada. Clin. Infect. Dis. 2012, 55, e109–e117. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Species | Number (%) of CR * | Number (%) of CS ** | Total No. of Isolates (%) |
|---|---|---|---|
| E. coli | 18 (21.42) | 66 (78.57) | 84 (35.29) |
| K. pneumoniae | 20 (28.98) | 49 (71.01) | 69 (28.99) |
| Enterobacter cloacae | 9 (22.50) | 31 (77.50) | 40 (16.80) |
| Klebsiella aerogenes | 3 (23.07) | 10 (76.92) | 13 (5.46) |
| S. typhi | - | 10 (100) | 10 (4.20) |
| P. mirabilis | 2 (20.0) | 8 (80.00) | 10 (4.20) |
| K. oxytoca | - | 6 (100) | 6 (2.52) |
| P. vulgaris | - | 4 (100) | 4 (1.68) |
| S. marcescens | - | 2 (100) | 2 (0.84) |
| Total | 52 (21.84) | 186 (78.15) | 238 (100) |
| Carbapenem-Resistant (CR) Species | Rapedic CARBA NP Positive No. (%), n = 52 | MBL Positive No. (%), n = 52 | PCR blaNDM No. (%), n = 52 |
|---|---|---|---|
| E. coli | 16 (30.76) | 15 (28.84) | 15 (28.84) |
| K. pneumoniae | 19 (36.53) | 17 (32.69) | 16 (30.76) |
| E. cloacae | 8 (15.38) | 8 (15.38) | 7 (13.46) |
| Klebsiella aerogenes | 3 (5.76) | 3 (5.76) | 3 (5.76) |
| Total No. (%) | 46 (88.46) | 43 (82.69) | 41 (78.84) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uddin, F.; Imam, S.H.; Khan, S.; Khan, T.A.; Ahmed, Z.; Sohail, M.; Elnaggar, A.Y.; Fallatah, A.M.; El-Bahy, Z.M. NDM Production as a Dominant Feature in Carbapenem-Resistant Enterobacteriaceae Isolates from a Tertiary Care Hospital. Antibiotics 2022, 11, 48. https://doi.org/10.3390/antibiotics11010048
Uddin F, Imam SH, Khan S, Khan TA, Ahmed Z, Sohail M, Elnaggar AY, Fallatah AM, El-Bahy ZM. NDM Production as a Dominant Feature in Carbapenem-Resistant Enterobacteriaceae Isolates from a Tertiary Care Hospital. Antibiotics. 2022; 11(1):48. https://doi.org/10.3390/antibiotics11010048
Chicago/Turabian StyleUddin, Fakhur, Syed Hadi Imam, Saeed Khan, Taseer Ahmed Khan, Zulfiqar Ahmed, Muhammad Sohail, Ashraf Y. Elnaggar, Ahmed M. Fallatah, and Zeinhom M. El-Bahy. 2022. "NDM Production as a Dominant Feature in Carbapenem-Resistant Enterobacteriaceae Isolates from a Tertiary Care Hospital" Antibiotics 11, no. 1: 48. https://doi.org/10.3390/antibiotics11010048
APA StyleUddin, F., Imam, S. H., Khan, S., Khan, T. A., Ahmed, Z., Sohail, M., Elnaggar, A. Y., Fallatah, A. M., & El-Bahy, Z. M. (2022). NDM Production as a Dominant Feature in Carbapenem-Resistant Enterobacteriaceae Isolates from a Tertiary Care Hospital. Antibiotics, 11(1), 48. https://doi.org/10.3390/antibiotics11010048