

Combination Regimens with Colistin Sulfate versus Colistin Sulfate Monotherapy in the Treatment of Infections Caused by Carbapenem-Resistant Gram-Negative Bacilli



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval of the Study Protocol
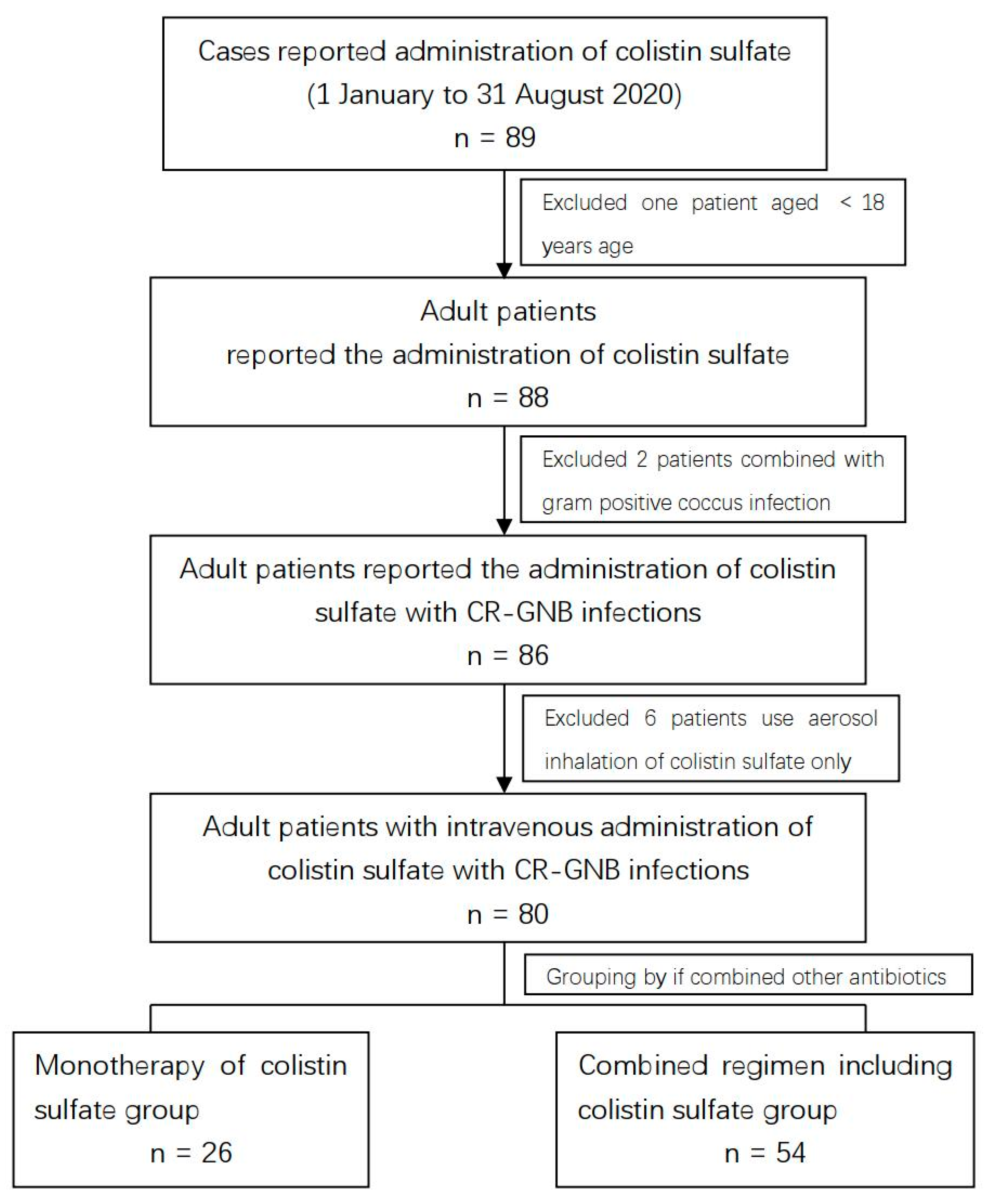
2.2. Patients
2.3. Data Collection
2.4. Clinical Efficiency Evaluation
2.5. Safety Evaluation
2.6. Microbiology
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Clinical Efficiency Evaluation
3.3. Safety Evaluation
3.4. Susceptibility Testing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CR-GNB | carbapenem-resistant Gram-negative bacilli |
| CRO | carbapenem-resistant organisms |
| CRKP | carbapenem-resistant Klebsiella pneumoniae |
| CRAB | carbapenem-resistant Acinetobacter baumannii |
| CRPA | carbapenem-resistant Pseudomonas aeruginosa |
| CMS | colistin methanesulfonate |
| CHINET | China Antimicrobial Surveillance Network |
| CRP | C-reactive protein |
| PCT | procalcitonin |
| CLSI | Clinical and Laboratory Standards Institute |
| MIC | minimal inhibitory concentration |
References
- Karakonstantis, S.; Kritsotakis, E.I.; Gikas, A. Treatment options for K. pneumoniae, P. aeruginosa and A. baumannii co-resistant to carbapenems, aminoglycosides, polymyxins and tigecycline: An approach based on the mechanisms of resistance to carbapenems. Infection 2020, 48, 835–851. [Google Scholar] [CrossRef]
- Guan, X.; He, L.; Hu, B.; Hu, J.; Huang, X.; Lai, G.; Li, Y.; Liu, Y.; Ni, Y.; Qiu, H.; et al. Laboratory diagnosis, clinical management and infection control of the infections caused by extensively drug-resistant Gram-negative bacilli: A Chinese consensus statement. Clin. Microbiol. Infect. 2016, 22 (Suppl. S1), S15–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Sayed Ahmed, M.A.E.; Zhong, L.L.; Shen, C.; Yang, Y.; Doi, Y.; Tian, G.B. Colistin and its role in the Era of antibiotic resistance: An extended review (2000–2019). Emerg. Microbes. Infect. 2020, 9, 868–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nation, R.L.; Li, J.; Cars, O.; Couet, W.; Dudley, M.N.; Kaye, K.S.; Mouton, J.W.; Paterson, D.L.; Tam, V.H.; Theuretzbacher, U.; et al. Framework for optimisation of the clinical use of colistin and polymyxin B: The Prato polymyxin consensus. Lancet Infect. Dis. 2015, 15, 225–234. [Google Scholar] [CrossRef]
- Ni, M.; Zhao, L.; Zhang, W.J.; Ma, J.W.; Zhang, G.Y.; Cui, D.M.; Wang, K.; Fei, Y.B.; Gao, L.; Shen, F.M. Pharmacokinetics of colistin in cerebrospinal fluid after intraventricular administration alone in intracranial infections. Int. J. Antimicrob. Agents 2021, 57, 106281. [Google Scholar] [CrossRef] [PubMed]
- Mizuyachi, K.; Hara, K.; Wakamatsu, A.; Nohda, S.; Hirama, T. Safety and pharmacokinetic evaluation of intravenous colistin methanesulfonate sodium in Japanese healthy male subjects. Curr. Med. Res. Opin. 2011, 27, 2261–2270. [Google Scholar] [CrossRef] [PubMed]
- Hanafin, P.O.; Nation, R.L.; Scheetz, M.H.; Zavascki, A.P.; Sandri, A.M.; Kwa, A.L.; Cherng, B.P.Z.; Kubin, C.J.; Yin, M.T.; Wang, J.; et al. Assessing the predictive performance of population pharmacokinetic models for intravenous polymyxin B in critically ill patients. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 1525–1537. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.L.; Liu, P.; Zhang, Q.W.; Yuan, W.H.; Wang, D.; Zhang, X.J.; Yang, J. Population pharmacokinetics and clinical outcomes of polymyxin B in paediatric patients with multidrug-resistant Gram-negative bacterial infections. J. Antimicrob. Chemother. 2022, dkac265. [Google Scholar] [CrossRef] [PubMed]
- Scudeller, L.; Righi, E.; Chiamenti, M.; Bragantini, D.; Menchinelli, G.; Cattaneo, P.; Giske, C.G.; Lodise, T.; Sanguinetti, M.; Piddock, L.J.V.; et al. Systematic review and meta-analysis of in vitro efficacy of antibiotic combination therapy against carbapenem-resistant Gram-negative bacilli. Int. J. Antimicrob. Agents 2021, 57, 106344. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Zhu, H.H.; Li, G.H.; Qi, T.T.; Ye, L.J.; Teng, X.Q.; Qu, Q.; He, G.F.; Qu, J. A Comparative Study of the Microbiological Efficacy of Polymyxin B on Different Carbapenem-Resistant Gram-Negative Bacteria Infections. Front Med. 2021, 8, 620885. [Google Scholar] [CrossRef] [PubMed]
- Qu, J.; Qi, T.T.; Qu, Q.; Long, W.M.; Chen, Y.; Luo, Y.; Wang, Y. Polymyxin B-Based Regimens for Patients Infected with Carbapenem-Resistant Gram-Negative Bacteria: Clinical and Microbiological Efficacy, Mortality, and Safety. Infect. Drug. Resist. 2022, 15, 1205–1218. [Google Scholar] [CrossRef] [PubMed]
- Cisneros, J.M.; Rosso-Fernández, C.M.; Roca-Oporto, C.; De Pascale, G.; Jiménez-Jorge, S.; Fernández-Hinojosa, E.; Matthaiou, D.K.; Ramírez, P.; Díaz-Miguel, R.O.; Estella, A.; et al. Colistin versus meropenem in the empirical treatment of ventilator-associated pneumonia (Magic Bullet study): An investigator-driven, open-label, randomized, noninferiority controlled trial. Crit. Care 2019, 23, 383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, S.H.; Chao, C.M.; Chang, S.P.; Lu, L.C.; Lai, C.C. Clinical Efficacy and Safety of Cefoperazone-Sulbactam in Treatment of Intra-Abdominal Infections: A Systematic Review and Meta-Analysis. Surg. Infect. 2021, 22, 763–770. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 32nd ed.; CLSI supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2022. [Google Scholar]
- Pogue, J.M.; Jones, R.N.; Bradley, J.S.; Andes, D.R.; Bhavnani, S.M.; Drusano, G.L.; Dudley, M.N.; Flamm, R.K.; Rodvold, K.A.; Ambrose, P.G. Polymyxin Susceptibility Testing and Interpretive Breakpoints: Recommendations from the United States Committee on Antimicrobial Susceptibility Testing (USCAST). Antimicrob. Agents Chemother. 2020, 64, e01495-19. [Google Scholar] [CrossRef] [PubMed]
- Perez, F.; El Chakhtoura, N.G.; Yasmin, M.; Bonomo, R.A. Polymyxins: To Combine or Not to Combine? Antibiotics 2019, 8, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doi, Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin. Infect Dis. 2019, 69 (Suppl. S7), S565–S575. [Google Scholar] [CrossRef] [Green Version]
- Vardakas, K.Z.; Mavroudis, A.D.; Georgiou, M.; Falagas, M.E. Intravenous colistin combination antimicrobial treatment vs. monotherapy: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2018, 51, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Zusman, O.; Altunin, S.; Koppel, F.; Dishon Benattar, Y.; Gedik, H.; Paul, M. Polymyxin monotherapy or in combination against carbapenem-resistant bacteria: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2017, 72, 29–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horcajada, J.P.; Montero, M.; Oliver, A.; Sorlí, L.; Luque, S.; Gómez-Zorrilla, S.; Benito, N.; Grau, S. Epidemiology and Treatment of Multidrug-Resistant and Extensively Drug-Resistant Pseudomonas aeruginosa Infections. Clin. Microbiol. Rev. 2019, 32, e00031-19. [Google Scholar] [CrossRef]
- Daikos, G.L.; Tsaousi, S.; Tzouvelekis, L.S.; Anyfantis, I.; Psichogiou, M.; Argyropoulou, A.; Stefanou, I.; Sypsa, V.; Miriagou, V.; Nepka, M.; et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections: Lowering mortality by antibiotic combination schemes and the role of carbapenems. Antimicrob. Agents Chemother. 2014, 58, 2322–2328. [Google Scholar] [CrossRef]
- Abdelsalam, M.F.A.; Abdalla, M.S.; El-Abhar, H.S.E. Prospective, comparative clinical study between high-dose colistin monotherapy and colistin-meropenem combination therapy for treatment of hospital-acquired pneumonia and ventilator-associated pneumonia caused by multidrug-resistant Klebsiella pneumoniae. J. Glob Antimicrob. Resist. 2018, 15, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Daikos, G.L.; Durante-Mangoni, E.; Yahav, D.; Carmeli, Y.; Benattar, Y.D.; Skiada, A.; Andini, R.; Eliakim-Raz, N.; Nutman, A.; et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant Gram-negative bacteria: An open-label, randomised controlled trial. Lancet Infect. Dis. 2018, 18, 391–400. [Google Scholar] [CrossRef]
- Yin, D.; Wu, S.; Yang, Y.; Shi, Q.; Dong, D.; Zhu, D.; Hu, F. Results from the China Antimicrobial Surveillance Network (CHINET) in 2017 of the In Vitro Activities of Ceftazidime-Avibactam and Ceftolozane-Tazobactam against Clinical Isolates of Enterobacteriaceae and Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2019, 63, e02431-18. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Monotherapy of Colistin Sulfate (n = 26) | Combined Regimen including Colistin Sulfate (n = 54) | t/χ2 Value | p-Value | |
|---|---|---|---|---|
| Age(years) Average ± SD | 60.5 ± 21.9 | 59.9 ± 19.2 | 0.14 | 0.893 |
| Sex (Male) | 19 (73.1) | 40 (74.1) | 0.01 | 0.924 |
| Comorbidities | ||||
| Diabetes | 3 (11.5) | 8 (14.8) | 0.16 | 0.690 |
| Malignant Tumor | 3 (11.5) | 15 (27.8) | 2.65 | 0.103 |
| Cardiovascular Disease | 4 (15.4) | 9 (16.7) | 0.66 | 0.884 |
| Transplant Recipient | 0 (0) | 5 (9.3) | - | 0.168 |
| Respiratory Comorbidities | 4 (15.4) | 13 (25.0) | 0.79 | 0.332 |
| Chronic Liver Diseases | 2 (7.7) | 5 (9.3) | - | 0.816 |
| Others | 5 (19.2) | 11 (20.4) | 0.01 | 0.905 |
| History of glucocorticoids | 5 (19.2) | 19 (35.2) | - | 0.145 |
| History of immunosuppressants | 1 (3.9) | 11 (20.4) | 3.76 | 0.053 |
| Invasive procedures one week before Infections | ||||
| Deep-vein catheterization | 14 (53.9) | 19 (35.2) | 2.52 | 0.112 |
| Indwell gastric tube | 9 (34.6) | 19 (35.2) | <0.001 | 0.960 |
| Indwell urethral catheter | 11 (42.3) | 16 (29.6) | 1.26 | 0.261 |
| Indwell tracheal intubation | 10 (38.5) | 24 (44.4) | 0.26 | 0.612 |
| Tracheotomy | 8 (30.8) | 7 (13.0) | 3.65 | 0.056 |
| Bronchoscopy | 11 (42.3) | 12 (22.2) | 3.46 | 0.063 |
| Operation with general anesthetics | 5 (19.2) | 12 (22.2) | 0.09 | 0.759 |
| Infectious Diseases | - | - | ||
| Hospital-acquired pneumoniae HAP | 17 (65.4) | 37 (68.5) | 0.08 | 0.779 |
| Bloodstream infection, BSI | 6 (23.1) | 6 (11.1) | 1.97 | 0.160 |
| Acute suppurative peritonitis | 0 (0) | 5 (9.3) | - | 0.168 |
| Urinary tract infection | 3 (11.5) | 1 (1.9) | - | 0.063 |
| Acute meningitis | 0 (0) | 3 (5.6) | - | 0.237 |
| Pathogenic Bacteria | Monotherapy of Colistin Sulfate (n = 26) | Combined Regimen including Colistin Sulfate (n = 54) | t/χ2 Value | p-Value |
|---|---|---|---|---|
| Acinetobacter baumannii | 11 (42.3) | 23 (42.6) | <0.001 | 0.981 |
| Pseudomonas aeruginosa | 8 (30.8) | 12 (22.2) | 0.68 | 0.408 |
| Klebsiella pneumoniae | 6 (23.1) | 11 (20.4) | 0.08 | 0.782 |
| Stenotrophomonas maltophilia | 1 (3.9) | 2 (3.7) | - | 0.975 |
| Citrobacter freudii | 0 (0) | 1 (1.9) | - | 0.989 |
| ≥two species of bacteria | 0 (0) | 5 (9.3) | - | 0.168 |
| Monotherapy with Colistin Sulfate (n = 26) | Combined Regimen including Colistin Sulfate (n = 54) | t/χ2/Z Value | p-Value | |
|---|---|---|---|---|
| Time from the positive outcome of culture to the initiation of antimicrobial treatment (d) Average ± SD | 2.0 ± 1.4 | 2.2 ± 1.4 | −0.38 | 0.704 |
| Treatment course (d) Average ± SD | 11.7 ± 4.9 | 11.3 ± 4.1 | 0.37 | 0.708 |
| Treatment course of HAP (d) Average ± SD | 12.0 ± 4.8 | 10.6 ± 4.3 | 1.05 | 0.260 |
| Treatment course of BSI (d) Average ± SD | 9.7 ± 4.3 | 14.5 ± 2.1 | −3.09 | 0.01 |
| No. of cases in which temperature (T) returned to normal | 22 (84.6) | 48 (88.9) | 0.29 | 0.588 |
| Time taken for T cases to return to normal (d) Average ± SD | 4.0 ± 3.2 | 5.4 ± 4.4 | −1.30 | 0.196 |
| Length of hospital stay (d) Average ± SD | 47.2 ± 32.4 | 49.8 ± 35.0 | −0.31 | 0.755 |
| No. of cases in which WBC count returned to normal within seven days b | 11 (42.3) | 37 (72.6) | 6.71 | 0.001 |
| No. of cases with decreased neutrophilic granulocyte percentage within seven days b | 10 (38.5) | 36 (70.6) | 7.39 | 0.007 |
| No. of cases with decreased CRP within seven days | 15 (57.7) | 50 (92.6) | 14.03 | 0.002 |
| No. of cases with decreased PCT within seven days | 14 (53.9) | 47 (87.0) | 10.68 | 0.001 |
| Variation range of the WBC count (*109/L) ab Median (Q1, Q3) | −1 (−5, 1.8) | −2.7 (−6.1, −1) | 2.12 | 0.034 |
| Variation range of neutrophilic granulocyte percentage ab Median (Q1, Q3) | 1 (−5.5, 5.5) | −5.95 (−15, −3) | 3.26 | 0.001 |
| Variation range of CRP (mg/dL) a Median (Q1, Q3) | 2 (−33, 16) | −21 (−54, −7) | 1.96 | 0.051 |
| Variation range of PCT (ng/mL) a Median (Q1, Q3) | 0.0 (−0.4, 2) | −0.28 (−2.1, −0.1) | 3.18 | 0.002 |
| Clinical efficacy | 19 (73.1) | 51 (94.4) | 7.33 | 0.007 |
| Microbial clearance rate | 13 (50.0) | 40 (74.1) | 4.55 | 0.033 |
| 28-day mortality | 3 (11.5) | 3 (5.6) | - | 0.341 |
| Total mortality | 5 (19.2) | 5 (9.3) | 1.60 | 0.207 |
| Monotherapy of Colistin Sulfate (n = 26) | Combined Regimen including Colistin Sulfate (n = 54) | χ2 Value | p-Value | |
|---|---|---|---|---|
| No. of cases with elevated serum creatinine | 6 (23.1) | 11 (20.4) | 0.08 | 0.782 |
| No. of cases with elevated ALT | 3 (11.5) | 5 (9.3) | - | 0.750 |
| No. of cases with elevated AST | 5 (19.2) | 7 (13.0) | 0.54 | 0.462 |
| No. of cases with elevated TBil | 4 (15.3) | 10 (18.5) | 0.12 | 0.730 |
| No. of cases with decreased platelet count * | 1 (4.0) | 3 (5.9) | - | 0.703 |
| Acinetobacter baumannii (n = 23) | Klebsiella pneumoniae (n = 11) | Pseudomonas aeruginosa (n = 13) | ||||
|---|---|---|---|---|---|---|
| MIC50 | R% | MIC50 | R% | MIC50 | R% | |
| Piperacillin/Tazobactam | ≥128 | 100 | ≥128 | 100 | ≥128 | 92 |
| Ceftazidime | ≥64 | 100 | ≥64 | 100 | ≥64 | 69 |
| Cefoperazone/Sulbactam | ≥64 | 100 | ≥64 | 100 | ≥64 | 100 |
| Cefepime | ≥64 | 100 | ≥64 | 100 | ≥64 | 77 |
| Imipenem | ≥16 | 100 | ≥16 | 100 | ≥16 | 92 |
| Meropenem | ≥16 | 100 | ≥16 | 100 | ≥16 | 92 |
| Ciprofloxacin | ≥4 | 100 | ≥4 | 82 | ≥4 | 85 |
| Levofloxacin | ≥8 | 100 | ≥8 | 82 | ≥4 | 85 |
| Amikacin | 16 | 96 | 2 | 36 | 4 | 31 |
| Minocycline | 4 | 43 | 8 | 73 | - | - |
| Doxycycline | ≥16 | 100 | ≥16 | 91 | - | - |
| Sulfamethoxazole/Trimethoprim | ≥320 | 83 | ≥320 | 91 | - | - |
| Tigecycline | 1 | 9 | 2 | 0 | - | - |
| Colistin | ≤0.5 | 0 | ≤0.5 | 0 | ≤0.5 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hao, M.; Yang, Y.; Guo, Y.; Wu, S.; Hu, F.; Qin, X. Combination Regimens with Colistin Sulfate versus Colistin Sulfate Monotherapy in the Treatment of Infections Caused by Carbapenem-Resistant Gram-Negative Bacilli. Antibiotics 2022, 11, 1440. https://doi.org/10.3390/antibiotics11101440
Hao M, Yang Y, Guo Y, Wu S, Hu F, Qin X. Combination Regimens with Colistin Sulfate versus Colistin Sulfate Monotherapy in the Treatment of Infections Caused by Carbapenem-Resistant Gram-Negative Bacilli. Antibiotics. 2022; 11(10):1440. https://doi.org/10.3390/antibiotics11101440
Chicago/Turabian StyleHao, Min, Yang Yang, Yan Guo, Shi Wu, Fupin Hu, and Xiaohua Qin. 2022. "Combination Regimens with Colistin Sulfate versus Colistin Sulfate Monotherapy in the Treatment of Infections Caused by Carbapenem-Resistant Gram-Negative Bacilli" Antibiotics 11, no. 10: 1440. https://doi.org/10.3390/antibiotics11101440
APA StyleHao, M., Yang, Y., Guo, Y., Wu, S., Hu, F., & Qin, X. (2022). Combination Regimens with Colistin Sulfate versus Colistin Sulfate Monotherapy in the Treatment of Infections Caused by Carbapenem-Resistant Gram-Negative Bacilli. Antibiotics, 11(10), 1440. https://doi.org/10.3390/antibiotics11101440