
Safety and Efficacy of Devices Delivering Inhaled Antibiotics among Adults with Non-Cystic Fibrosis Bronchiectasis: A Systematic Review and a Network Meta-Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
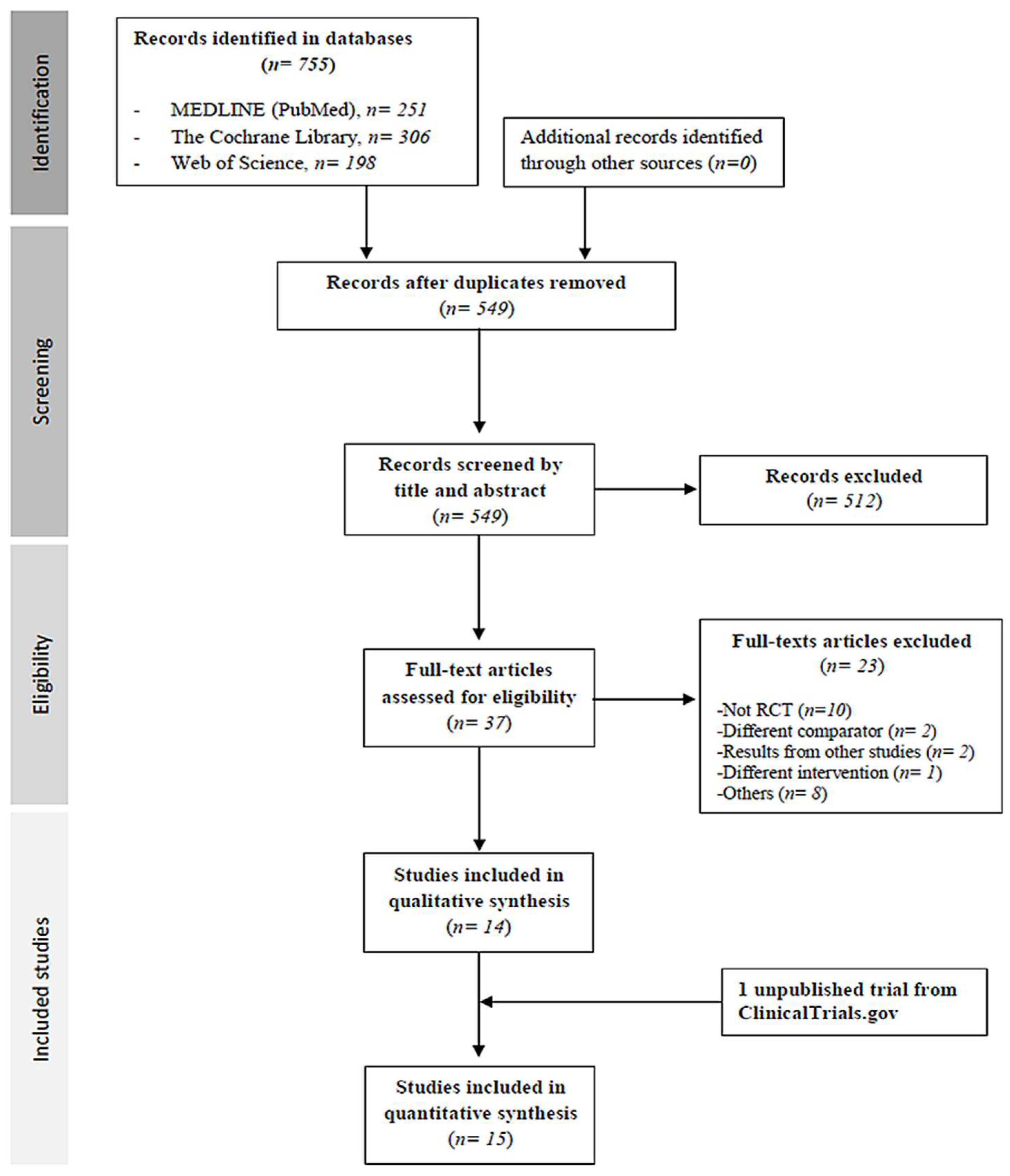
2.1. Study Selection
2.2. Study Characteristics
2.3. Risk of Bias Assessment
2.4. Outcomes
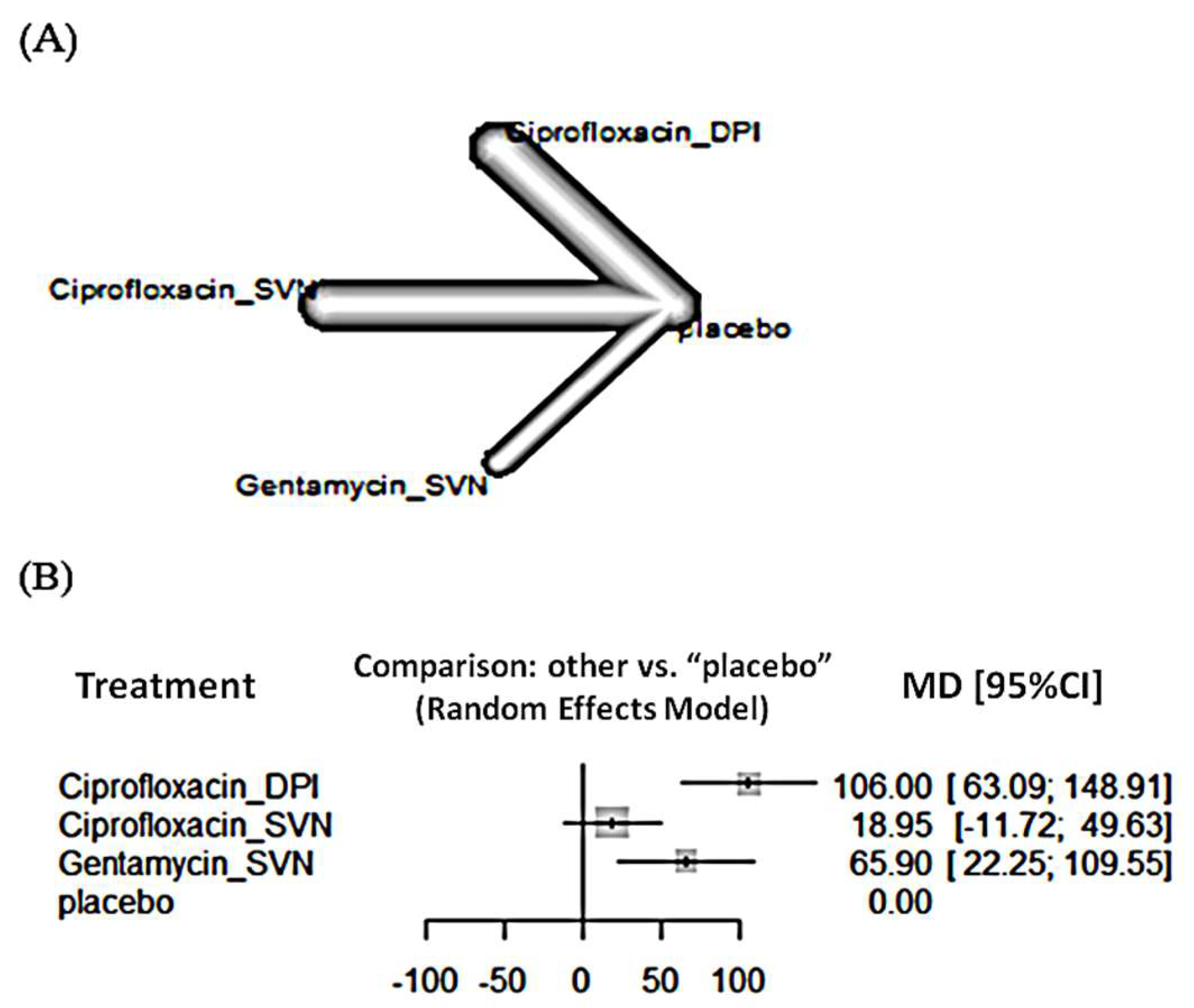
2.4.1. Efficacy
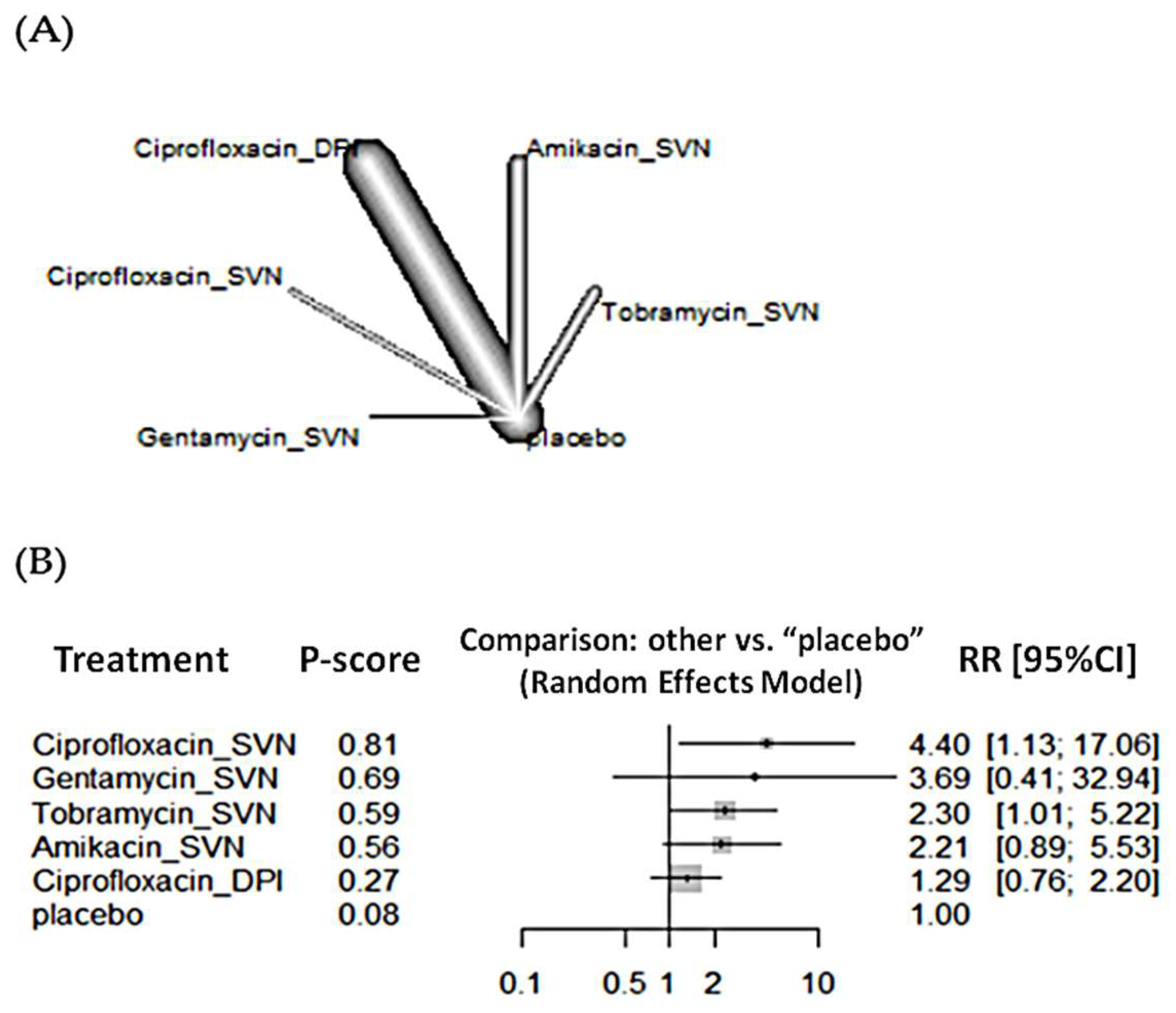
2.4.2. Microbiological Outcomes
2.4.3. Mortality
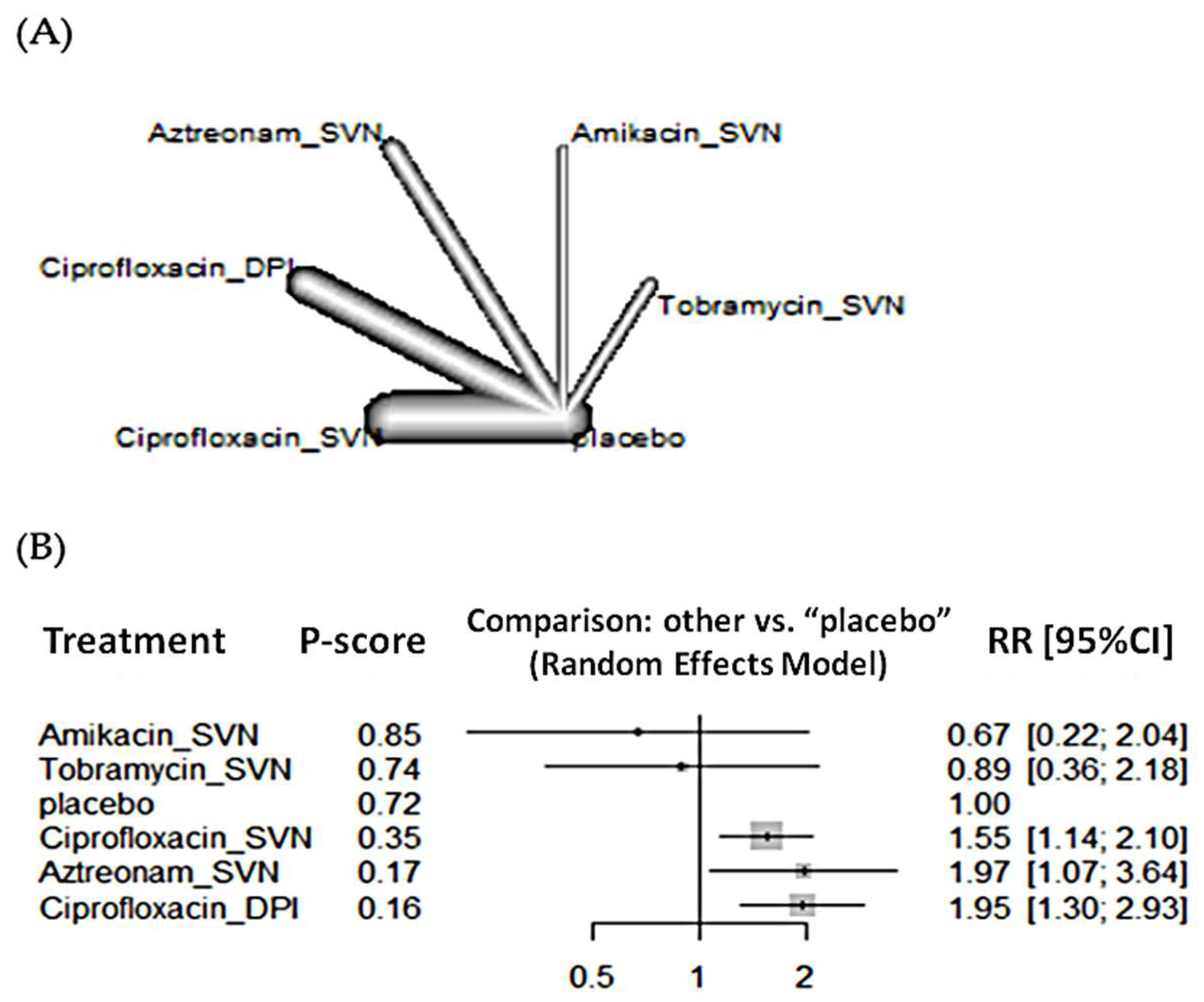
2.4.4. Safety Outcomes
3. Discussion
Strengths and Limitations
4. Methods
4.1. Registration and Protocol
4.2. Eligibility Criteria
- Clinical efficacy: time to fist exacerbation, number of patients at least one exacerbation, spirometry results as FEV1%, and quality of life measured by SGRQ. In this SGRQ questionnaire, higher scores indicate a poorer quality of life.
- Clinical outcomes: mortality.
- Microbiological outcomes: bacterial eradication, emergence of new potential respiratory pathogens, sputum bacterial density, and emergence of overall (and P. aeruginosa) antimicrobial resistance.
- Safety outcomes: adverse events related to study drug, serious adverse events, adverse events leading to study drug discontinuation, and bronchospasm episodes.
4.3. Search Strategy
4.4. Data Collection
4.5. Quality Assessment
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Castellani, C.; Duff, A.J.A.; Bell, S.C.; Heijerman, H.G.M.; Munck, A.; Ratjen, F.; Sermet-Gaudelus, I.; Southern, K.W.; Barben, J.; Flume, P.A.; et al. ECFS Best Practice Guidelines: The 2018 Revision. J. Cyst. Fibros. 2018, 17, 153–178. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.T.; Sullivan, A.L.; Chalmers, J.D.; De Soyza, A.; Elborn, S.J.; Floto, A.R.; Grillo, L.; Gruffydd-Jones, K.; Harvey, A.; Haworth, C.S.; et al. British Thoracic Society Guideline for Bronchiectasis in Adults. Thorax 2019, 74, 1–69. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.Á.; Máiz, L.; Olveira, C.; Girón, R.M.; de la Rosa, D.; Blanco, M.; Cantón, R.; Vendrell, M.; Polverino, E.; de Gracia, J.; et al. Spanish Guidelines on Treatment of Bronchiectasis in Adults. Arch. Bronconeumol. 2018, 54, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Polverino, E.; Goeminne, P.C.; McDonnell, M.J.; Aliberti, S.; Marshall, S.E.; Loebinger, M.R.; Murris, M.; Cantón, R.; Torres, A.; Dimakou, K.; et al. European Respiratory Society Guidelines for the Management of Adult Bronchiectasis. Eur. Respir. J. 2017, 50, 1700629. [Google Scholar] [CrossRef]
- Chang, A.B.; Bell, S.C.; Torzillo, P.J.; King, P.T.; Maguire, G.P.; Byrnes, C.A.; Holland, A.E.; O’Mara, P.; Grimwood, K. Extended voting group Chronic Suppurative Lung Disease and Bronchiectasis in Children and Adults in Australia and New Zealand Thoracic Society of Australia and New Zealand Guidelines. Med. J. Aust. 2015, 202, 21–23. [Google Scholar] [CrossRef]
- Tejada, S.; Campogiani, L.; Solé-Lleonart, C.; Gómez, A.; Gallego, M.; Vendrell, M.; Soriano, J.B.; Rello, J. Inhaled Antibiotics for Treatment of Adults with Non-Cystic Fibrosis Bronchiectasis: A Systematic Review and Meta-Analysis. Eur. J. Intern. Med. 2021, 90, 77–88. [Google Scholar] [CrossRef]
- Martínez-García, M.Á.; Oscullo, G.; Barreiro, E.; Cuenca, S.; Cervera, A.; Padilla-Galo, A.; de la Rosa, D.; Navarro, A.; Giron, R.; Carbonero, F.; et al. Inhaled Dry Powder Antibiotics in Patients with Non-Cystic Fibrosis Bronchiectasis: Efficacy and Safety in a Real-Life Study. J. Clin. Med. 2020, 9, 2317. [Google Scholar] [CrossRef]
- Rau, J.L. The Inhalation of Drugs: Advantages and Problems. Respir Care 2005, 50, 367–382. [Google Scholar]
- Dolovich, M.B.; Ahrens, R.C.; Hess, D.R.; Anderson, P.; Dhand, R.; Rau, J.L.; Smaldone, G.C.; Guyatt, G.; American College of Chest Physicians. American College of Asthma, Allergy, and Immunology Device Selection and Outcomes of Aerosol Therapy: Evidence-Based Guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest 2005, 127, 335–371. [Google Scholar] [CrossRef]
- Rello, J.; Rouby, J.J.; Sole-Lleonart, C.; Chastre, J.; Blot, S.; Luyt, C.E.; Riera, J.; Vos, M.C.; Monsel, A.; Dhanani, J.; et al. Key Considerations on Nebulization of Antimicrobial Agents to Mechanically Ventilated Patients. Clin. Microbiol. Infect. 2017, 23, 640–646. [Google Scholar] [CrossRef]
- Laska, I.F.; Crichton, M.L.; Shoemark, A.; Chalmers, J.D. The Efficacy and Safety of Inhaled Antibiotics for the Treatment of Bronchiectasis in Adults: A Systematic Review and Meta-Analysis. Lancet Respir. Med. 2019, 7, 855–869. [Google Scholar] [CrossRef]
- Xu, M.-J.; Dai, B. Inhaled Antibiotics Therapy for Stable Non-Cystic Fibrosis Bronchiectasis: A Meta-Analysis. Ther. Adv. Respir. Dis. 2020, 14, 1753466620936866. [Google Scholar] [CrossRef] [PubMed]
- Brodt, A.M.; Stovold, E.; Zhang, L. Inhaled Antibiotics for Stable Non-Cystic Fibrosis Bronchiectasis: A Systematic Review. Eur. Respir. J. 2014, 44, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Uttley, L.; Tappenden, P. Dry Powder Inhalers in Cystic Fibrosis: Same Old Drugs but Different Benefits? Curr. Opin. Pulm. Med. 2014, 20, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Baez-Pravia, O.V.; Montes-Andujar, L.; Menéndez, J.; Cardinal-Fernández, P. What Have We Learned from Network Meta-Analyses Applied to Critical Care? Minerva Anestesiol. 2019, 85, 433–442. [Google Scholar] [CrossRef]
- De Soyza, A.; Aksamit, T.; Bandel, T.-J.; Criollo, M.; Elborn, J.S.; Operschall, E.; Polverino, E.; Roth, K.; Winthrop, K.L.; Wilson, R. RESPIRE 1: A Phase III Placebo-Controlled Randomised Trial of Ciprofloxacin Dry Powder for Inhalation in Non-Cystic Fibrosis Bronchiectasis. Eur. Respir. J. 2018, 51, 1702052. [Google Scholar] [CrossRef]
- Aksamit, T.; De Soyza, A.; Bandel, T.-J.; Criollo, M.; Elborn, J.S.; Operschall, E.; Polverino, E.; Roth, K.; Winthrop, K.L.; Wilson, R. RESPIRE 2: A Phase III Placebo-Controlled Randomised Trial of Ciprofloxacin Dry Powder for Inhalation in Non-Cystic Fibrosis Bronchiectasis. Eur. Respir. J. 2018, 51, 1702053. [Google Scholar] [CrossRef]
- Wilson, R.; Welte, T.; Polverino, E.; De Soyza, A.; Greville, H.; O’Donnell, A.; Alder, J.; Reimnitz, P.; Hampel, B. Ciprofloxacin Dry Powder for Inhalation in Non-Cystic Fibrosis Bronchiectasis: A Phase II Randomised Study. Eur. Respir. J. 2013, 41, 1107–1115. [Google Scholar] [CrossRef]
- Haworth, C.S.; Bilton, D.; Chalmers, J.D.; Davis, A.M.; Froehlich, J.; Gonda, I.; Thompson, B.; Wanner, A.; O’Donnell, A.E. Inhaled Liposomal Ciprofloxacin in Patients with Non-Cystic Fibrosis Bronchiectasis and Chronic Lung Infection with Pseudomonas Aeruginosa (ORBIT-3 and ORBIT-4): Two Phase 3, Randomised Controlled Trials. Lancet Respir. Med. 2019, 7, 213–226. [Google Scholar] [CrossRef]
- Ailiyaer, Y.; Wang, X.; Zhang, Y.; Li, C.; Li, T.; Qi, Q.; Li, Y. A Prospective Trial of Nebulized Amikacin in the Treatment of Bronchiectasis Exacerbation. Respiration 2018, 95, 327–333. [Google Scholar] [CrossRef]
- Barker, A.F.; O’Donnell, A.E.; Flume, P.; Thompson, P.J.; Ruzi, J.D.; de Gracia, J.; Boersma, W.G.; De Soyza, A.; Shao, L.; Zhang, J.; et al. Aztreonam for Inhalation Solution in Patients with Non-Cystic Fibrosis Bronchiectasis (AIR-BX1 and AIR-BX2): Two Randomised Double-Blind, Placebo-Controlled Phase 3 Trials. Lancet Respir. Med. 2014, 2, 738–749. [Google Scholar] [CrossRef]
- Orriols, R.; Hernando, R.; Ferrer, A.; Terradas, S.; Montoro, B. Eradication Therapy against Pseudomonas Aeruginosa in Non-Cystic Fibrosis Bronchiectasis. Respiration 2015, 90, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Haworth, C.S.; Foweraker, J.E.; Wilkinson, P.; Kenyon, R.F.; Bilton, D. Inhaled Colistin in Patients with Bronchiectasis and Chronic Pseudomonas Aeruginosa Infection. Am. J. Respir. Crit. Care Med. 2014, 189, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Serisier, D.J.; Bilton, D.; De Soyza, A.; Thompson, P.J.; Kolbe, J.; Greville, H.W.; Cipolla, D.; Bruinenberg, P.; Gonda, I. ORBIT-2 investigators Inhaled, Dual Release Liposomal Ciprofloxacin in Non-Cystic Fibrosis Bronchiectasis (ORBIT-2): A Randomised, Double-Blind, Placebo-Controlled Trial. Thorax 2013, 68, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.P.; Govan, J.R.W.; Doherty, C.J.; Simpson, A.J.; Wilkinson, T.S.; Chalmers, J.D.; Greening, A.P.; Haslett, C.; Hill, A.T. A Randomized Controlled Trial of Nebulized Gentamicin in Non-Cystic Fibrosis Bronchiectasis. Am. J. Respir. Crit. Care Med. 2011, 183, 491–499. [Google Scholar] [CrossRef]
- Bilton, D.; Henig, N.; Morrissey, B.; Gotfried, M. Addition of Inhaled Tobramycin to Ciprofloxacin for Acute Exacerbations of Pseudomonas Aeruginosa Infection in Adult Bronchiectasis. Chest 2006, 130, 1503–1510. [Google Scholar] [CrossRef]
- Drobnic, M.E.; Suñé, P.; Montoro, J.B.; Ferrer, A.; Orriols, R. Inhaled Tobramycin in Non-Cystic Fibrosis Patients with Bronchiectasis and Chronic Bronchial Infection with Pseudomonas Aeruginosa. Ann. Pharmacother. 2005, 39, 39–44. [Google Scholar] [CrossRef]
- Couch, L.A. Treatment With Tobramycin Solution for Inhalation in Bronchiectasis Patients with Pseudomonas Aeruginosa. Chest 2001, 120, 114S–117S. [Google Scholar] [CrossRef]
- Barker, A.F.; Couch, L.; Fiel, S.B.; Gotfried, M.H.; Ilowite, J.; Meyer, K.C.; O’Donnell, A.; Sahn, S.A.; Smith, L.J.; Stewart, J.O.; et al. Tobramycin Solution for Inhalation Reduces Sputum Pseudomonas Aeruginosa Density in Bronchiectasis. Am. J. Respir. Crit. Care Med. 2000, 162, 481–485. [Google Scholar] [CrossRef]
- Insmed Incorporated. Safety and Tolerability Study of 2 Dose Level of ArikayceTM in Patients with Bronchiectasis and Chronic Infection Due to Pseudomonas Aeruginosa. 2019. Available online: https://clinicaltrials.gov/ct2/show/NCT00775138 (accessed on 8 March 2021).
- Tiddens, H.A.W.M.; Meerburg, J.J.; van der Eerden, M.M.; Ciet, P. The Radiological Diagnosis of Bronchiectasis: What’s in a Name? Eur. Respir. Rev. 2020, 29, 190120. [Google Scholar] [CrossRef]
- Kaplan, S.; Lee, A.; Caine, N.; Charman, S.C.; Bilton, D. Long-Term Safety Study of Colistimethate Sodium (Colobreathe®): Findings from the UK Cystic Fibrosis Registry. J. Cyst. Fibros. 2021, 20, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Konstan, M.W.; Flume, P.A.; Kappler, M.; Chiron, R.; Higgins, M.; Brockhaus, F.; Zhang, J.; Angyalosi, G.; He, E.; Geller, D.E. Safety, Efficacy and Convenience of Tobramycin Inhalation Powder in Cystic Fibrosis Patients: The EAGER Trial. J. Cyst. Fibros. 2011, 10, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Solé-Lleonart, C.; Rouby, J.-J.; Blot, S.; Poulakou, G.; Chastre, J.; Palmer, L.B.; Bassetti, M.; Luyt, C.-E.; Pereira, J.M.; Riera, J.; et al. Nebulization of Antiinfective Agents in Invasively Mechanically Ventilated Adults: A Systematic Review and Meta-Analysis. Anesthesiology 2017, 126, 890–908. [Google Scholar] [CrossRef] [PubMed]
- Boisson, M.; Bouglé, A.; Sole-Lleonart, C.; Dhanani, J.; Arvaniti, K.; Rello, J.; Rouby, J.-J.; Mimoz, O. European Investigator Network for Nebulized Antibiotics in Ventilator-Associated Pneumonia (ENAVAP). Nebulized Antibiotics for Healthcare- and Ventilator-Associated Pneumonia. Semin. Respir. Crit. Care Med. 2022; [Online ahead of print]. [Google Scholar] [CrossRef]
- Monsel, A.; Torres, A.; Zhu, Y.; Pugin, J.; Rello, J.; Rouby, J.-J. European Investigators Network for Nebulized Antibiotics in Ventilator-associated Pneumonia (ENAVAP) Nebulized Antibiotics for Ventilator-Associated Pneumonia: Methodological Framework for Future Multicenter Randomized Controlled Trials. Curr. Opin. Infect. Dis. 2021, 34, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Tejada, S.; Ramírez-Estrada, S.; Tejo, A.M.; Forero, C.G.; Pomares, X.; Gallego, M.; Soriano, J.B.; Chalmers, J.D.; Rello, J. Critical Appraisal of International Adult Bronchiectasis Guidelines Using the AGREE II Tool. Eur. J. Intern. Med. 2022; S0953-6205(22)00035-8, [Online ahead of print]. [Google Scholar] [CrossRef]
- Montón, C.; Prina, E.; Pomares, X.; Cugat, J.R.; Casabella, A.; Oliva, J.C.; Gallego, M.; Monsó, E. Nebulized Colistin And Continuous Cyclic Azithromycin In Severe COPD Patients With Chronic Bronchial Infection Due To Pseudomonas Aeruginosa: A Retrospective Cohort Study. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2365–2373. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Schrenzel, J.; Tejo, A.M. New Insights into Pneumonia in Patients on Prolonged Mechanical Ventilation: Need for a New Paradigm Addressing Dysbiosis. J. Bras. Pneumol. 2021, 47, e20210198. [Google Scholar] [CrossRef] [PubMed]
- Pomares, X.; Montón, C.; Bullich, M.; Cuevas, O.; Oliva, J.C.; Gallego, M.; Monsó, E. Clinical and Safety Outcomes of Long-Term Azithromycin Therapy in Severe COPD Beyond the First Year of Treatment. Chest 2018, 153, 1125–1133. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-Analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; ISBN 978-1-119-53661-1. [Google Scholar]
- Dolovich, M.B.; Dhand, R. Aerosol Drug Delivery: Developments in Device Design and Clinical Use. Lancet 2011, 377, 1032–1045. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Tonin, F.S.; Borba, H.H.; Mendes, A.M.; Wiens, A.; Fernandez-Llimos, F.; Pontarolo, R. Description of Network Meta-Analysis Geometry: A Metrics Design Study. PLoS ONE 2019, 14, e0212650. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Location | Age, Mean (SD) | Characteristics | N Patients | Intervention | Control | Doses | Frequency |
|---|---|---|---|---|---|---|---|---|---|
| DPI device | |||||||||
| deSoyza (RESPIRE-1) | 2018 | Israel, Australia, New Zealand, Spain, USA, UK, Germany, Japan, Italy, Latvia, France, Argentina, Slovakia, Denmark | Ciprofloxacin: 64.2 (12.1) Placebo: 64 (13.5) | RDBPCT, multicenter | 416 | Ciprofloxacin | Placebo | 32.5 mg | BID, 48 weeks of 14 or 28 days on/off via DPI |
| Aksamit (RESPIRE-2) | 2018 | Russia, Bulgaria, Latvia, Poland, South Korea, Serbia, Romania, Turkey, Australia, Germany, The Netherlands, USA, Brazil, Portugal, China, Austria, Argentina, Thailand, Taiwan, South Africa, Philippines, Lithuania, Czech Republic | Ciprofloxacin: 59.3 (14.2) Placebo: 60.6 (13.7) | RDBPCT, multicenter | 521 | Ciprofloxacin | Placebo | 32.5 mg | BID, 48 weeks of 14 or 28 days on/off via DPI |
| Wilson | 2013 | Australia, Germany, Spain, Sweden, UK, USA | Ciprofloxacin: 64.7 (11.8) Placebo: 61.4 (11.9) | RDBPCT, multicenter | 124 | Ciprofloxacin | Placebo | 32.5 mg | BID, 28 days on and 56 weeks off via DPI |
| SVN device | |||||||||
| Haworth (ORBIT 3) | 2019 | Australia, Canada, Germany, Hungary, Ireland, Israel, Italy, Latvia, Poland, UK, USA, Romania, South Africa, South Korea, Spain, Taiwan | Ciprofloxacin: 64.3 (13.6) Placebo: 66.7 (10.7) | RDBPCT, multicenter | 278 | Ciprofloxacin ARD-3150 | Placebo | 6 mL (3 mL liposome- encapsulated ciprofloxacin 135 mg + 3 mL free ciprofloxacin 54 mg) | QD, 48 weeks (6 cycles) of 28 day on/off via nebulizer (PARI LC sprint) |
| Haworth (ORBIT 4) | 2019 | Australia, Canada, France, Georgia, Hungary, Israel, Italy, New Zealand, Peru, Poland, Romania, Serbia, South Korea, Spain, UK, USA | Ciprofloxacin: 63.3 (13.5) Placebo: 64.2 (12.6) | RDBPCT, multicenter | 304 | Ciprofloxacin ARD-3150 | Placebo | 6 mL (3 mL liposome- encapsulated ciprofloxacin 135 mg + 3 mL free ciprofloxacin 54 mg) | QD, 48 weeks (6 cycles) of 28 day on/off via nebulizer (PARI LC sprint) |
| Serisier | 2013 | Australia, New Zealand | Ciprofloxacin: 70 (5.6) Placebo: 59.5 (13.2) | RDBPCT, multicenter | 42 | Ciprofloxacin | Placebo | 6 mL (liposome ciprofloxacin 150 mg + free ciprofloxacin 60 mg) | QD, 24 weeks (3 cycles) of 28 days on/off via nebulizer (PARI LC sprint) |
| Orriols | 2015 | Spain | Tobramycin: 69.3 (2.1) Placebo: 70.1 (1.9) | RSBPCT, single-center | 35 | Tobramycin | Placebo | 300 mg | BID, 12 weeks via a jet nebulizer |
| Bilton | 2006 | USA, UK | Tobramycin: 61.9 (11.4) Placebo: 63.7 (11.7) | RDBPCT, multicenter | 53 | Tobramycin | Placebo | 300 mg/5 mL + 750 mg | BID, 6 weeks via jet nebulizer (PARI LC PLUS) |
| Drobnic | 2005 | Spain | NR | RDBPCT, crossover, single-center | 60 | Tobramycin | Placebo | 8 mL | BID, 48 weeks (2 cycles each of 6 months) via a jet nebulizer |
| Couch and Barker | 2001 /2000 | US | NR | RDBPCT, multicenter | 74 | Tobramycin | Placebo | 300 mg | BID, 4 weeks via a jet nebulizer |
| Barker (AIR-BX1) | 2015 | Australia, Canada, USA | Aztreonam: 64.2 (12.9) Placebo: 64.9 (12.1) | RDBPCT, multicenter | 266 | Aztreonam | Placebo | 75 mg | TID, 16 weeks (2 cycles) of 28 days on/off via eFlow nebulizer |
| Barker (AIR-BX2) | 2015 | Australia, Belgium, Canada, France, Germany, Italy, The Netherlands, Spain, UK, USA | Aztreonam: 63.3 (14.2) Placebo: 62.7 (13.3) | RDBPCT, multicenter | 274 | Aztreonam | Placebo | 75 mg | TID, 16 weeks (2 cycles) of 28 days on/off via eFlow nebulizer |
| Ailiyaer | 2018 | China | Amikacin: 57.3 (13) Placebo: 56.5 (10.8) | RCT, open-label, multicenter | 152 | Amikacin | Placebo | 5 mL | BID, 2 weeks via a jet atomizer |
| TR02-107 | 2014 | Bulgaria, Greece, Hungary, India, Serbia, Ukraine | Amikacin: 49.9 (21.1) Placebo: 46.8 (15) | RDBPCT, multicenter | 62 | Amikacin | Placebo | 280 or 560 mg | QD, 4 weeks via eFlow nebulizer |
| Haworth | 2014 | United Kingdom, Russia, Ukraine | Colistin: 58.3 (15.3) Placebo: 60.3 (15.8) | RDBPCT, multicenter | 144 | Colistin | Placebo | 1 million IU | BID, 24 weeks via I-neb AAD system |
| Murray | 2011 | UK | * Gentamycin: 58 (53–67) Placebo: 64 (55.7–69) | RSBPCT, single-center | 65 | Gentamycin | Placebo | 80 mg | BID, 48 weeks via a jet nebulizer |
| Via DPI (Ciprofloxacin) n = 3 | Via SVN (Ciprofloxacin) n = 3 | ||||
|---|---|---|---|---|---|
| Outcomes | Trials | % (n/N) | Trials | % (n/N) | Risk Ratio (% CI) |
| Time to first pulmonary exacerbation, days | 2 | - | 5 | - | 87.05 (34.30; 139.79) |
| Patients with at least one exacerbation | 3 | 38.9 (266/683) | 8 | 42.4 (358/844) | 0.98 (0.74; 1.29) |
| Change in FEV1% | 3 | - | 3 | - | - |
| Change in SGRQ | 3 | - | 6 | - | −7.52 (−13.06; −1.98) |
| Overall mortality | 2 | 1.7 (11/623) | 6 | 2.1 (14/652) | 2.81 (0.39; 20.30) |
| Hospitalizations | 1 | 3.3 (2/60) | 5 | 8.5 (58/678) | - |
| Eradication pathogens | 3 | 34.3 (228/663) | 6 | 45 (73/162) | 0.29 (0.07; 1.26) |
| Emergence of new respiratory pathogens | 3 | 5.5 (38/683) | 2 | 36.6 (11/30) | 0.58 (0.27; 1.23) |
| Resistance in overall bacteria isolates | 2 | 20.8 (130/623) | 10 | 33.9 (174/513) | 1.26 (0.76; 2.09) |
| Resistance in P. aeruginosa isolates | - | - | 6 | 19.6 (75/382) | 3.15 (0.09; 109.40) |
| Change in bacterial density | 1 | - | 9 | - | 1.50 (−1.13; 4.13) |
| Drug-related AE | 3 | 19.9 (136/683) | 8 | 33.8 (283/837) | 0.99 (0.65; 1.51) |
| AE leading to drug discontinuation | 3 | 9.6 (66/683) | 10 | 10 (93/925) | 0.69 (0.35; 1.32) |
| Drug-related serious AE | 2 | 2.1 (7/338) | 4 | 2.9 (15/505) | 0.90 (0.11; 7.33) |
| Bronchospasm | 3 | 3.9 (27/683) | 5 | 3.3 (19/563) | 0.52 (0.08; 3.26) |
| 1. Device/drug availability |
| 2. Patient age and the ability to use the selected device correctly |
| 3. Clinical setting |
| 4. Device use with multiple medications |
| 5. Cost and reimbursement |
| 6. Convenience in both outpatient and inpatient settings |
| 7. Physician and patient preference |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tejada, S.; Ramírez-Estrada, S.; Forero, C.G.; Gallego, M.; Soriano, J.B.; Cardinal-Fernández, P.A.; Ehrmann, S.; Rello, J. Safety and Efficacy of Devices Delivering Inhaled Antibiotics among Adults with Non-Cystic Fibrosis Bronchiectasis: A Systematic Review and a Network Meta-Analysis. Antibiotics 2022, 11, 275. https://doi.org/10.3390/antibiotics11020275
Tejada S, Ramírez-Estrada S, Forero CG, Gallego M, Soriano JB, Cardinal-Fernández PA, Ehrmann S, Rello J. Safety and Efficacy of Devices Delivering Inhaled Antibiotics among Adults with Non-Cystic Fibrosis Bronchiectasis: A Systematic Review and a Network Meta-Analysis. Antibiotics. 2022; 11(2):275. https://doi.org/10.3390/antibiotics11020275
Chicago/Turabian StyleTejada, Sofia, Sergio Ramírez-Estrada, Carlos G. Forero, Miguel Gallego, Joan B. Soriano, Pablo A. Cardinal-Fernández, Stephan Ehrmann, and Jordi Rello. 2022. "Safety and Efficacy of Devices Delivering Inhaled Antibiotics among Adults with Non-Cystic Fibrosis Bronchiectasis: A Systematic Review and a Network Meta-Analysis" Antibiotics 11, no. 2: 275. https://doi.org/10.3390/antibiotics11020275
APA StyleTejada, S., Ramírez-Estrada, S., Forero, C. G., Gallego, M., Soriano, J. B., Cardinal-Fernández, P. A., Ehrmann, S., & Rello, J. (2022). Safety and Efficacy of Devices Delivering Inhaled Antibiotics among Adults with Non-Cystic Fibrosis Bronchiectasis: A Systematic Review and a Network Meta-Analysis. Antibiotics, 11(2), 275. https://doi.org/10.3390/antibiotics11020275