
Outpatient Antibiotic Prescriptions in France: Patients and Providers Characteristics and Impact of the COVID-19 Pandemic


Abstract
:1. Introduction
2. Results
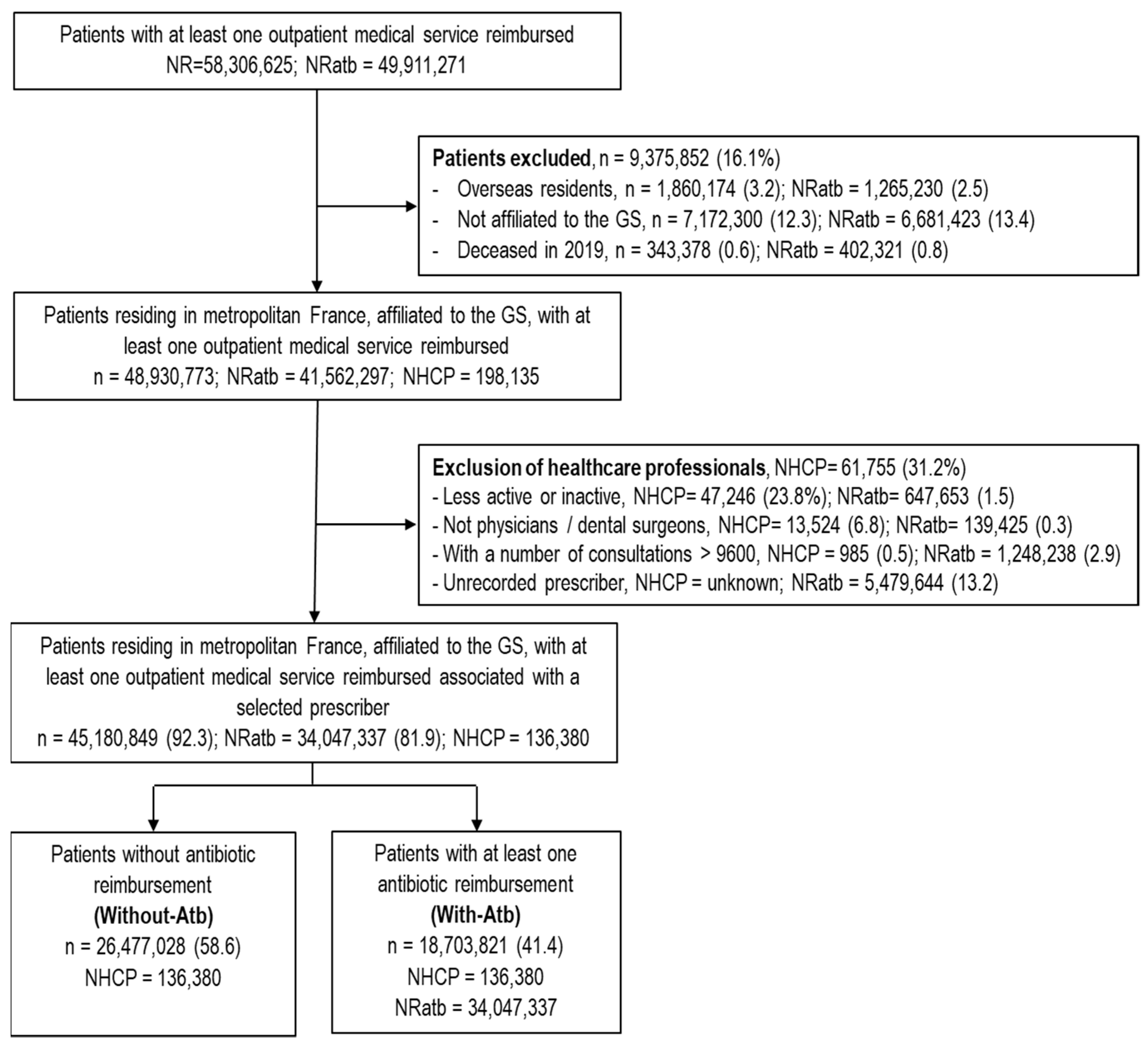
2.1. Patients
2.2. Prescribers
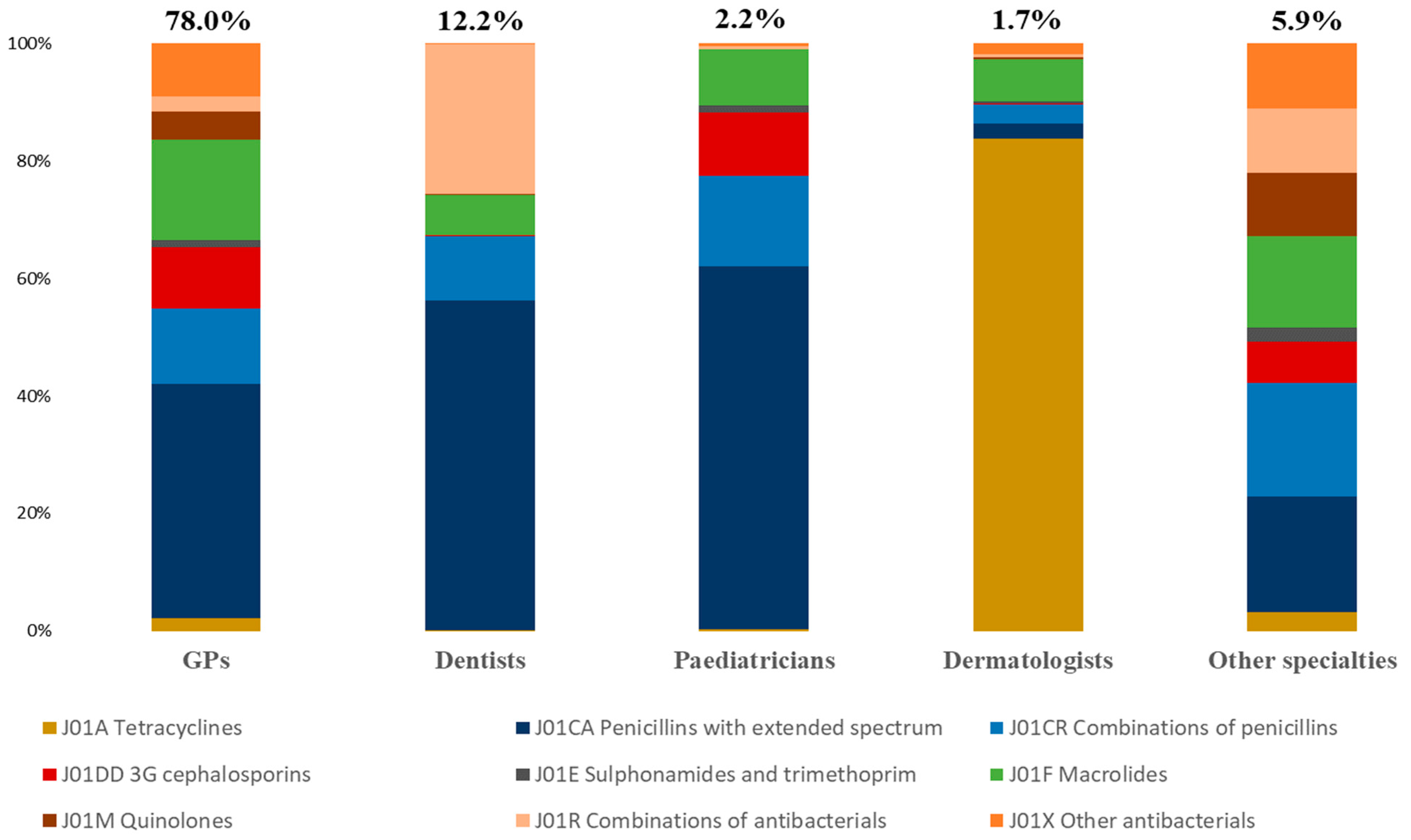
2.3. Antibiotic Prescriptions
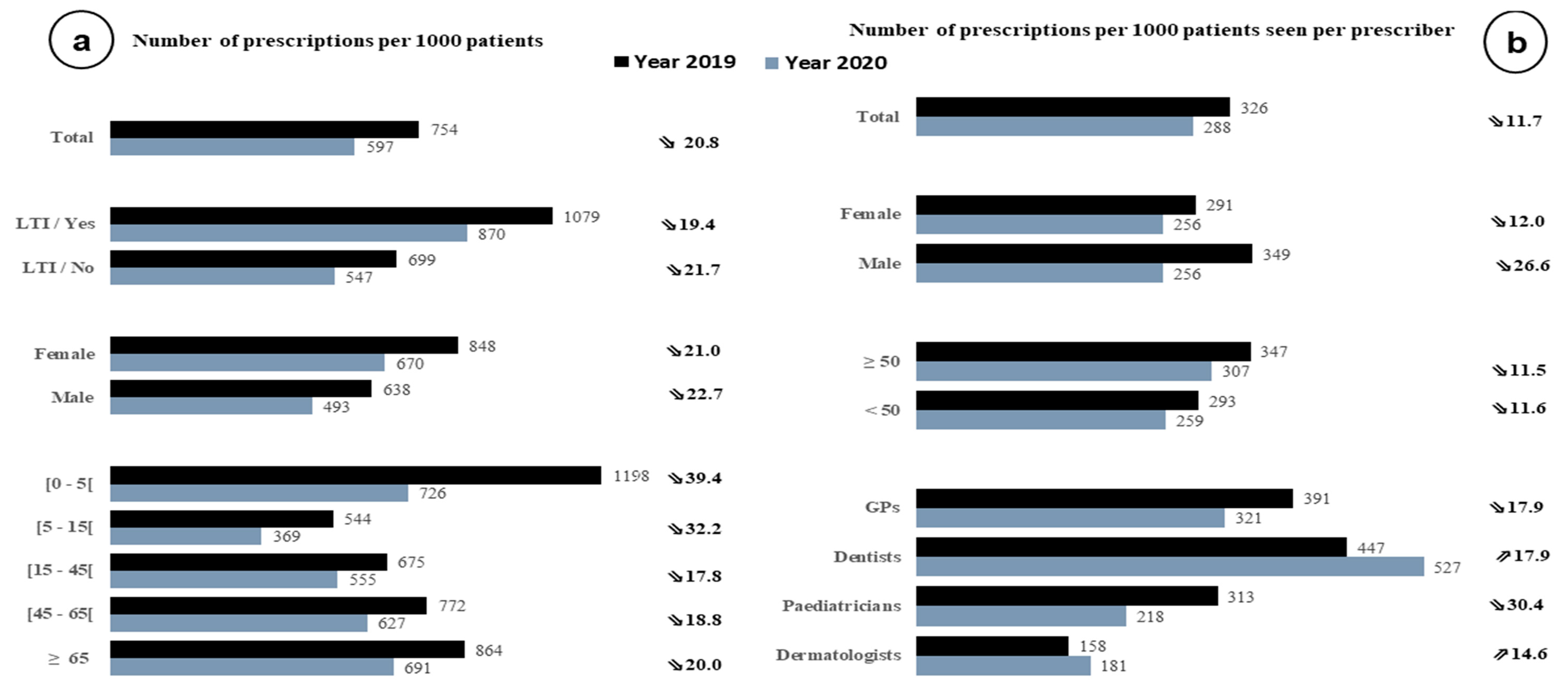
2.4. Prescribing Indicators
3. Discussion
4. Materials and Methods
4.1. Source of Data
4.2. Study Populations
4.3. Variables Studied
4.4. Prescribing Indicators
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spellberg, B.; Bartlett, J.G.; Gilbert, D.N. The Future of Antibiotics and Resistance. N. Engl. J. Med. 2013, 368, 299–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biggest Threats and Data|Antibiotic/Antimicrobial Resistance|CDC. Available online: https://www.cdc.gov/drugresistance/biggest-threats.html (accessed on 23 November 2020).
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Burden of AMR Collaborative Group, Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Opatowski, M.; Tuppin, P.; Cosker, K.; Touat, M.; De Lagasnerie, G.; Guillemot, D.; Salomon, J.; Brun-Buisson, C.; Watier, L. Hospitalisations with infections related to antimicrobial-resistant bacteria from the French nationwide hospital discharge database, 2016. Epidemiol. Infect. 2019, 147, e144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, A.H.; Moore, L.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.; Piddock, L. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Goossens, H.; Ferech, M.; Stichele, R.V.; Elseviers, M. ESAC Project Group, Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance—The need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control, Antimicrobial Consumption in the EU/EEA—Annual Epidemiological Report 2019. 2020. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2019 (accessed on 16 December 2020).
- Cavalié, P.; Djeraba, A. [The Evolution of Antibiotic Consumption in France between 2000 and 2013] in French. ANSM. 2014. Available online: https://ansm.sante.fr/var/ansm_site/storage/original/application/28f39921e2a8d8368a1fbfcdc496bd88.pdf (accessed on 2 March 2021).
- Schmidt, M.L.; Spencer, M.D.; Davidson, L.E. Patient, Provider, and Practice Characteristics Associated with Inappropriate Antimicrobial Prescribing in Ambulatory Practices. Infect. Control Hosp. Epidemiol. 2018, 39, 307–315. [Google Scholar] [CrossRef] [Green Version]
- Fleming-Dutra, K.E.; Bartoces, M.; Roberts, R.M.; Hicks, L.A. Characteristics of primary care physicians associated with high outpatient antibiotic prescribing volume. Open Forum Infect. Dis. 2018, 5, ofx279. [Google Scholar] [CrossRef]
- Gerber, J.S.; Prasad, P.A.; Localio, A.R.; Fiks, A.G.; Grundmeier, R.W.; Bell, L.M.; Wasserman, R.C.; Keren, R.; Zaoutis, T.E. Variation in antibiotic prescribing across a pediatric primary care network. J. Pediatr. Infect. Dis. Soc. 2015, 4, 297–304. [Google Scholar] [CrossRef] [Green Version]
- Ternhag, A.; Grünewald, M.; Nauclér, P.; Wisell, K.T. Antibiotic consumption in relation to socio-demographic factors, co-morbidity, and accessibility of primary health care. Scand. J. Infect. Dis. 2014, 46, 888–896. [Google Scholar] [CrossRef]
- Kourlaba, G.; Gkrania-Klotsas, E.; Kourkouni, E.; Mavrogeorgos, G.; Zaoutis, T.E. Antibiotic prescribing and expenditures in outpatient adults in Greece, 2010 to 2013: Evidence from real-world practice. Eurosurveillance 2016, 21, 30266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klevens, R.M.; Caten, E.; Olesen, S.W.; DeMaria, A.; Troppy, S.; Grad, Y.H. Outpatient Antibiotic Prescribing in Massachusetts, 2011–2015. Open Forum Infect. Dis. 2019, 6, ofz169. [Google Scholar] [CrossRef] [PubMed]
- Imanpour, S.; Nwaiwu, O.; McMaughan, D.K.; DeSalvo, B.; Bashir, A. Factors associated with antibiotic prescriptions for the viral origin diseases in office-based practices, 2006–2012. JRSM Open 2017, 8, 2054270417717668. [Google Scholar] [CrossRef] [PubMed]
- Morley, V.J.; Firgens, E.P.C.; Vanderbilt, R.R.; Zhou, Y.; Zook, M.; Read, A.F.; MacGeorge, E.L. Factors associated with antibiotic prescribing for acute bronchitis at a university health center. BMC Infect. Dis. 2020, 20, 177. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, M.S.; Maneno, M.K.; Daftary, M.N.; Wingate, L.; Ettienne, E.B. Factors Associated with Prescribing Broad-Spectrum Antibiotics for Children with Upper Respiratory Tract Infections in Ambulatory Care Settings. Clin. Med. Insights Pediatri. 2018, 12, 1179556518784300. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, N.A.; di Gangi, S.; Pichierri, G.; Neuner-Jehle, S.; Senn, O.; Plate, A. Time Trends and Factors Associated with Antibiotic Prescribing in Swiss Primary Care (2008 to 2020). Antibiotics 2020, 9, 837. [Google Scholar] [CrossRef] [PubMed]
- Shallcross, L.; Beckley, N.; Rait, G.; Hayward, A.; Petersen, I. Antibiotic prescribing frequency amongst patients in primary care: A cohort study using electronic health records. J. Antimicrob. Chemother. 2017, 72, 1818–1824. [Google Scholar] [CrossRef] [Green Version]
- Malo, S.; Rabanaque, M.J.; Feja, C.; Lallana, M.J.; Aguilar, I.; Bjerrum, L. High antibiotic consumption: A characterization of heavy users in Spain. Basic Clin. Pharmacol. Toxicol. 2014, 115, 231–236. [Google Scholar] [CrossRef]
- Pouwels, K.B.; Dolk, F.C.K.; Smith, D.R.M.; Smieszek, T.; Robotham, J.V. Explaining variation in antibiotic prescribing between general practices in the UK. J. Antimicrob. Chemother. 2018, 73, ii27–ii35. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.E.; Sauer, B.; Jones, M.M.; Campo, J.; Damal, K.; He, T.; Ying, J.; Greene, T.; Goetz, M.B.; Neuhauser, M.M.; et al. Variation in Outpatient Antibiotic Prescribing for Acute Respiratory Infections in the Veteran Population: A Cross-sectional Study. Ann. Intern. Med. 2015, 163, 73–80. [Google Scholar] [CrossRef]
- Schwartz, K.L.; Brown, K.A.; Etches, J.; Langford, B.J.; Daneman, N.; Tu, K.; Johnstone, J.; Achonu, C.; Garber, G. Predictors and variability of antibiotic prescribing amongst family physicians. J. Antimicrob. Chemother. 2019, 74, 2098–2105. [Google Scholar] [CrossRef] [PubMed]
- Swe, M.M.M.; Ashley, E.A.; Althaus, T.; Lubell, Y.; Smithuis, F.; Mclean, A.R.D. Inter-prescriber variability in the decision to prescribe antibiotics to febrile patients attending primary care in Myanmar. JAC Antimicrob. Resist. 2021, 3, dlaa118. [Google Scholar] [CrossRef] [PubMed]
- Weill, A.; Drouin, J.; Desplas, D.; Cuenot, F.; Spira, R.D.; Zureik, M. [Outpatient Use of Drugs in France during the COVID-19 Epidemic—Update to April 25, 2021. Pharmacoepidemiological Study Based on SNDS Reimbursement Data] in French (EPI—PHARE Scientific Interest Grouping (GIS) ANSM—Cnam, 2021). Available online: https://www.epi-phare.fr/rapports-detudes-et-publications/usage-des-medicaments-de-ville-en-france-durant-lepidemie-de-covid-19-point-de-situation-a-la-fin-mars-2020/ (accessed on 22 September 2021).
- Sluggett, J.K.; Dinh, Y.H.; Wesselingh, S.L.; Inacio, M.C.; Caughey, G.E. National changes in outpatient systemic antibiotic use during the coronavirus disease 2019 pandemic in australia. Clin. Infect. Dis. 2021, 73, 2150–2152. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.Z.; Paudyal, V.; Hadi, M.A. Impact of the COVID-19 Pandemic on the Prescribing Patterns of First-Line Antibiotics in English Primary Care: A Longitudinal Analysis of National Prescribing Dataset. Antibiotics 2021, 10, 591. [Google Scholar] [CrossRef]
- Buehrle, D.J.; Nguyen, M.H.; Wagener, M.M.; Clancy, C.J. Impact of the coronavirus disease 2019 pandemic on outpatient antibiotic prescriptions in the united states. Open Forum Infect. Dis. 2020, 7, ofaa575. [Google Scholar] [CrossRef]
- Jung, S.; Sexton, M.E.; Owens, S.; Spell, N.; Fridkin, S. Variability of Antibiotic Prescribing in a Large Healthcare Network Despite Adjusting for Patient-Mix: Reconsidering Targets for Improved Prescribing. Open Forum Infect. Dis. 2019, 6, ofz018. [Google Scholar] [CrossRef]
- Dolk, F.C.K.; Pouwels, K.B.; Smith, D.R.M.; Robotham, J.V.; Smieszek, T. Antibiotics in primary care in England: Which antibiotics are prescribed and for which conditions? J. Antimicrob. Chemother. 2018, 73, ii2–ii10. [Google Scholar] [CrossRef]
- Schröder, W.; Sommer, H.; Gladstone, B.P.; Foschi, F.; Hellman, J.; Evengard, B.; Tacconelli, E. Gender differences in antibiotic prescribing in the community: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2016, 71, 1800–1806. [Google Scholar] [CrossRef]
- Bernabeu-Mira, J.C.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. Prescription of Antibiotic Prophylaxis for Dental Implant Surgery in Healthy Patients: A Systematic Review of Survey-Based Studies. Front. Pharmacol. 2020, 11, 588333. [Google Scholar] [CrossRef]
- Agossa, K.; Sy, K.; Mainville, T.; Gosset, M.; Jeanne, S.; Grosgogeat, B.; Siepmann, F.; Loingeville, F.; Dubar, M. Antibiotic Use in Periodontal Therapy among French Dentists and Factors Which Influence Prescribing Practices. Antibiotics 2021, 10, 303. [Google Scholar] [CrossRef]
- Mian, M.; Teoh, L.; Hopcraft, M. Trends in Dental Medication Prescribing in Australia during the COVID-19 Pandemic. JDR Clin. Trans. Res. 2021, 6, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Teoh, L.; Stewart, K.; Marino, R.J.; McCullough, M.J. Part 1. Current prescribing trends of antibiotics by dentists in Australia from 2013 to 2016. Aust. Dent. J. 2018, 63, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Hellman, J.; Aspevall, O.; Bengtsson, B.; Pringle, M. Swedres-Svarm 2015. Consumption of Antibiotics and Occurrence of Antibiotic Resistance in Sweden (Public Health Agency of Sweden and National Veterinary Institute, 2015). Available online: https://www.folkhalsomyndigheten.se/contentassets/e52354e8f91b43b9b25186f06b7a1b48/swedres-svarm-2015-15099.pdf (accessed on 4 March 2022).
- National Plan against Antibiotic Resistance (PRAN). [Antibiotic Consumption Community Sector] in Spanish. Consumos Antibióticos Sector Comunitario. 2021. Available online: https://resistenciaantibioticos.es/en/node/333 (accessed on 19 October 2021).
- van de Pol, A.C.; Boeijen, J.A.; Venekamp, R.P.; Platteel, T.; Damoiseaux, R.A.M.J.; Kortekaas, M.F.; van der Velden, A.W. Impact of the COVID-19 Pandemic on Antibiotic Prescribing for Common Infections in The Netherlands: A Primary Care-Based Observational Cohort Study. Antibiotics 2021, 10, 196. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.A.; Eickhoff, J.; Wald, E.R. Impact of COVID-19 Quarantine and School Cancelation on Other Common Infectious Diseases. Pediatr. Infect. Dis. J. 2020, 39, e449–e452. [Google Scholar] [CrossRef] [PubMed]
- Santé Publique France. [Seasonal Influenza Surveillance Report 2020–2021] in French (Santé Publique France, 2021). Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/grippe (accessed on 29 October 2021).
- Kitano, T.; Brown, K.A.; Daneman, N.; MacFadden, D.R.; Langford, B.J.; Leung, V.; So, M.; Leung, E.; Burrows, L.; Manuel, D.; et al. The Impact of COVID-19 on Outpatient Antibiotic Prescriptions in Ontario, Canada: An Interrupted Time Series Analysis. Open Forum Infect. Dis. 2021, 8, ofab533. [Google Scholar] [CrossRef]
- Santé Publique France. [Bronchiolitis Epidemiological Bulletin] in French (Bulletin Hebdomadaire, 2022). Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/bronchiolite (accessed on 5 February 2022).
- Gillies, M.B.; Burgner, D.P.; Ivancic, L.; Nassar, N.; Miller, J.E.; Sullivan, S.G.; Todd, I.M.F.; Pearson, S.-A.; Schaffer, A.L.; Zoega, H. Changes in antibiotic prescribing following COVID-19 restrictions: Lessons for post-pandemic antibiotic stewardship. Br. J. Clin. Pharmacol. 2021, 88, 1143–1151. [Google Scholar] [CrossRef]
- Knight, B.D.; Shurgold, J.; Smith, G.; MacFadden, D.R.; Schwartz, K.L.; Daneman, N.; Tropper, D.G.; Brooks, J. The impact of COVID-19 on community antibiotic use in Canada: An ecological study. Clin. Microbiol. Infect. 2021, 28, 426–432. [Google Scholar] [CrossRef]
- Tuppin, P.; Rudant, J.; Constantinou, P.; Gastaldi-Ménager, C.; Rachas, A.; de Roquefeuil, L.; Maura, G.; Caillol, H.; Tajahmady, A.; Coste, J.; et al. Value of a national administrative database to guide public decisions: From the système national d’information interrégimes de l’Assurance Maladie (SNIIRAM) to the système national des données de santé (SNDS) in France. Rev. Epidemiol. Sante Publique 2017, 65 (Suppl. 4), S149–S167. [Google Scholar] [CrossRef]
- Rey, G.; Jougla, E.; Fouillet, A.; Hémon, D. Ecological association between a deprivation index and mortality in France over the period 1997–2001: Variations with spatial scale, degree of urbanicity, age, gender and cause of death. BMC Public Health 2009, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- Method of Mapping Pathologies and Health Insurance Expenditure (Detailed Definitions and Expert Review of the Algorithms are Publicly Available in French). Available online: https://assurance-maladie.ameli.fr/sites/default/files/2021_methode-reperage-pathologies_cartographie_1.pdf (accessed on 5 November 2021).
- Demidenko, E. The p-Value You Can’t Buy. Am. Stat. 2016, 70, 33–38. [Google Scholar] [CrossRef] [Green Version]
- French Ministry for Solidarity and Health, 2022–2025 National Strategy for Preventing Infections and Antibiotic Resistance. Available online: https://solidarites-sante.gouv.fr/IMG/pdf/national_strategy_for_preventing_infections_and_antibiotic_resistance_2022-2025_.pdf (accessed on 3 May 2022).




{kind=link}
{kind=link}
{kind=link}
| Year 2019 | Year 2020 | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Without-Atb | With-Atb | Without-Atb | With-Atb | ||||
| n | % | n | % | n | % | n | % | |
| 26,477,028 | 58.6 | 18,703,821 | 41.4 | 30,492,755 | 65.3 | 16,174,425 | 34.7 | |
| Sex | ||||||||
| Male | 12,949,452 | 48.9 | 7,681,528 | 41.1 | 14,804,256 | 48.6 | 6,616,141 | 41.0 |
| Female | 13,527,448 | 51.1 | 11,022,193 | 58.9 | 15,688,489 | 51.4 | 9,532,590 | 59.0 |
| Age in years | ||||||||
| [0–4] | 1,243,498 | 4.7 | 1,528,973 | 8.2 | 1,616,231 | 5.3 | 1,133,255 | 7.0 |
| [5–14] | 3,751,652 | 14.2 | 1,972,825 | 10.6 | 4,170,206 | 13.7 | 1,491,278 | 9.2 |
| [15–44] | 9,787,330 | 37.0 | 6,482,426 | 34.7 | 10,787,768 | 35.4 | 5,695,477 | 35.2 |
| [45–64] | 6,632,635 | 25.1 | 4,806,033 | 25.7 | 7,746,405 | 25.4 | 4,327,717 | 26.8 |
| ≥65 | 5,061,799 | 19.1 | 3,913,564 | 20.9 | 6,172,145 | 20.2 | 3,526,698 | 21.8 |
| Median (IQR 1) | 40 (19–59) | - | 42 (20–61) | - | 41 (20–60) | - | 43 (23–62) | - |
| Number of long-term illnesses (LTI) | ||||||||
| 0 | 21,927,912 | 84.1 | 14,596,193 | 79.6 | 24,868,480 | 82.8 | 12,422,238 | 78.4 |
| 1 | 3,199,233 | 12.3 | 2,734,653 | 14.9 | 3,981,177 | 13.3 | 2,514,039 | 15.9 |
| ≥2 | 959,540 | 3.7 | 1,011,325 | 5.5 | 1,175,989 | 3.9 | 903,731 | 5.7 |
| Comorbidities | ||||||||
| Chronic respiratory | 979,191 | 4.0 | 1,465,344 | 8.2 | 1,282,053 | 4.5 | 1,301,885 | 8.4 |
| Cardiovascular | 1,556,421 | 6.3 | 1,418,797 | 8.0 | 1,970,846 | 6.9 | 1,307,048 | 8.4 |
| Diabetes | 1,347,042 | 5.5 | 1,149,997 | 6.5 | 1,663,939 | 5.9 | 1,059,982 | 6.8 |
| Types of cancer | 972,843 | 4.0 | 948,449 | 5.3 | 121,226 | 4.3 | 871,066 | 5.6 |
| Complementary universal health insurance CMUc | ||||||||
| Population < 60 years | 19,909,570 | 75.2 | 13,642,472 | 73.0 | 22,984,453 | 74.1 | 11,616,489 | 71.9 |
| Yes | 2,026,487 | 10.2 | 1,801,283 | 13.2 | 2,712,922 | 11.8 | 1,782,625 | 15.3 |
| Residence area | ||||||||
| Rural | 8,233,538 | 32.0 | 5,735,200 | 31.4 | 9,549,105 | 31.7 | 4,927,830 | 31.3 |
| Urban | 17,496,612 | 68.0 | 12,507,620 | 68.6 | 20,574,085 | 68.3 | 10,819,973 | 68.7 |
| Regions of residence | ||||||||
| Auvergne-Rhône-Alpes | 3,512,752 | 13.6 | 2,139,269 | 11.7 | 3,922,996 | 13.3 | 1,802,396 | 11.4 |
| Bourgogne-Franche-Comté | 1,071,646 | 4.2 | 792.034 | 4.3 | 1,220,548 | 4.1 | 672.196 | 4.3 |
| Brittany | 1,407,558 | 5.5 | 878.389 | 4.8 | 1,603,757 | 5.4 | 746.349 | 4.7 |
| Centre-Val de Loire | 1,043,472 | 4.0 | 667.860 | 3.6 | 1,161,773 | 3.9 | 568.459 | 3.6 |
| Corsica | 96.200 | 0.4 | 95.367 | 0.5 | 120.946 | 0.4 | 87.748 | 0.6 |
| Grand Est | 2,224,183 | 8.6 | 163.7714 | 8.9 | 2,517,511 | 8.5 | 1,389,502 | 8.8 |
| Hauts-de-France | 2,274,070 | 8.8 | 1,903,928 | 10.4 | 2,635,567 | 8.9 | 1,645,956 | 10.4 |
| Île-de-France | 4,707,424 | 18.2 | 3,289,329 | 17.9 | 5,367,918 | 18.1 | 2,800,595 | 17.8 |
| Normandy | 1,246,605 | 4.8 | 914.042 | 5.0 | 1,437,588 | 4.8 | 781.745 | 5.0 |
| Nouvelle-Aquitaine | 2,295,033 | 8.9 | 1,733,969 | 9.5 | 2,705,874 | 9.1 | 1,523,883 | 9.7 |
| Occitanie | 2,318,158 | 9.0 | 1,747,434 | 9.5 | 2,728,435 | 9.2 | 1,518,379 | 9.6 |
| Pays de la Loire | 1,623,283 | 6.3 | 910.753 | 5.0 | 1,820,213 | 6.2 | 778.280 | 4.9 |
| Provence-Alpes-Côte d’Azur | 2,001,770 | 7.8 | 1,631,496 | 8.9 | 2,372,981 | 8.0 | 1,457,778 | 9.2 |
| Social deprivation index | ||||||||
| Q1 (least disadvantaged) | 5,332,126 | 20.6 | 3,668,352 | 20.0 | 6,277,265 | 20.8 | 3,149,281 | 19.9 |
| Q2 | 5,357,867 | 20.7 | 3,700,019 | 20.2 | 6,256,429 | 20.7 | 3,174,668 | 20.1 |
| Q3 | 5,282,014 | 20.5 | 3,732,332 | 20.4 | 6,152,617 | 20.4 | 3,212,878 | 20.3 |
| Q4 | 5,072,874 | 19.6 | 3,584,209 | 19.6 | 5,892,691 | 19.5 | 3,100,271 | 19.6 |
| Q5 (most disadvantaged) | 4,785,247 | 18.5 | 3,625,804 | 19.8 | 5,660,298 | 18.7 | 3,164,046 | 20.0 |
| Number of consultations | ||||||||
| [1–2] | 9,961,149 | 37.6 | 2,851,634 | 15.3 | 13,492,844 | 44.2 | 3,504,330 | 21.7 |
| [3–4] | 7,109,098 | 26.8 | 3,969,442 | 21.2 | 8,119,038 | 26.6 | 3,889,795 | 24.1 |
| [5–9] | 6,980,363 | 26.4 | 7,272,078 | 38.9 | 6,770,662 | 22.2 | 5,684,991 | 35.1 |
| ≥10 | 2,426,304 | 9.2 | 4,610,567 | 24.7 | 2,110,211 | 6.9 | 3,095,309 | 19.1 |
| Number of prescriptions per patient | ||||||||
| 1 | - | 10,734,648 | 57.4 | - | 9,892,615 | 61.2 | ||
| 2 | - | 4,352,182 | 23.3 | - | 3,598,891 | 22.3 | ||
| 3 | - | 1,878,977 | 10.1 | - | 1,433,011 | 8.9 | ||
| 4 or more | - | 1,737,914 | 9.3 | - | 1,249,908 | 7.7 | ||
| All HCPs 1 | GPs 2 | Dentists | Paediatricians | Dermatologists | Other | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Sex | ||||||||||||
| Women | 54,471 | 40.1 | 23,359 | 40.7 | 15,543 | 43.2 | 1717 | 65.9 | 1937 | 69.5 | 11,915 | 32.3 |
| Men | 81,201 | 59.9 | 34,086 | 59.3 | 20,416 | 56.8 | 888 | 34.1 | 852 | 30.5 | 24,959 | 67.7 |
| Age, in years | ||||||||||||
| <50 | 52,580 | 39.1 | 21,071 | 37.0 | 18,595 | 51.9 | 888 | 34.8 | 641 | 23.4 | 11,385 | 31.3 |
| ≥50 | 81,900 | 60.9 | 35,927 | 63.0 | 17,226 | 48.1 | 1664 | 65.2 | 2096 | 76.6 | 24,959 | 67.7 |
| Mean ± SD 3 | 52 ± 12.2 | - | 52.7 ± 11.8 | 47.5 ± 12.9 | 54.2 ± 11.2 | 56.4 ± 10.1 | 54.8 ± 10.8 | |||||
| Years of experience | ||||||||||||
| Junior ≤ 15 years | 52,164 | 39.0 | 21,360 | 37.8 | 14,393 | 40.5 | 1191 | 46.9 | 710 | 25.9 | 14,510 | 39.7 |
| Intermediate 15–30 years | 49,399 | 36.9 | 21,000 | 37.2 | 12,318 | 34.7 | 836 | 32.9 | 1175 | 42.9 | 14,070 | 38.5 |
| Senior ≥ 30 years | 32,236 | 24.1 | 14,090 | 25.0 | 8838 | 24.9 | 514 | 20.2 | 8838 | 24.9 | 7938 | 21.7 |
| Mean ± SD | 19.4 ± 12.5 | - | 19.7 ± 12.7 | 19.2 ± 12.6 | 17.4 ± 12.7 | 22.7 ± 11.5 | 18.9 ± 12.0 | |||||
| Type of practice | ||||||||||||
| Private | 127,288 | 93.4 | 54,496 | 94.7 | 35,023 | 96.4 | 2239 | 85.8 | 2488 | 88.9 | 33,042 | 89.3 |
| Mixed | 8854 | 6.5 | 2924 | 5.1 | 1289 | 3.6 | 370 | 14.2 | 311 | 11.1 | 3960 | 10.7 |
| Salaried | 146 | 0.1 | 143 | 0.3 | - | - | - | 2 | 0.0 | |||
| Conventional status | ||||||||||||
| Sector 1 | 110,028 | 81.2 | 53,315 | 93.5 | 36,225 | 100.0 | 1502 | 57.7 | 1552 | 55.9 | 17,434 | 47.3 |
| Sector 2 | 25,469 | 18.8 | 3714 | 6.5 | - | 1100 | 42.3 | 1225 | 44.1 | 19,430 | 52.7 | |
| Activity | ||||||||||||
| Consultations | 253,421,882 | - | 194,404,033 | 76.6 | 10,351,166 | 4.1 | 6,363,102 | 2.5 | 4,636,225 | 1.8 | 37,667,356 | 14.9 |
| Patients seen | 104,286,371 | - | 67,863,794 | 65.1 | 9,306,050 | 8.9 | 2,370,138 | 2.3 | 3,558,126 | 3.4 | 21,188,263 | 20.3 |
| Prescriptions 4 | 34,047,337 | - | 26,566,106 | 78.0 | 4,164,192 | 12.2 | 742,006 | 2.2 | 563,016 | 1.7 | 2,012,017 | 5.9 |
| Prescription per 1000 consultations | 134 | - | 137 | - | - | - | 117 | - | 121 | - | 53 | |
| All Providers | 136,380 | - | 57,573 | 42.2 | 36,330 | 26.6 | 2612 | 1.9 | 2800 | 2.1 | 37,065 | 27.2 |
| Number of Antibiotic Prescriptions per Year | ∆ 2019–2020, n (%) | ||||
|---|---|---|---|---|---|
| 2019 | % | 2020 | % | ||
| Socio-demographic characteristics of recipients | |||||
| Sex | |||||
| Male | 13,186,680 | 38.7 | 10,714,622 | 38.5 | ↓ 2,472,058 (18.7) |
| Female | 20,860,657 | 61.3 | 17,137,640 | 61.5 | ↓ 3,723,017 (17.8) |
| Long-term illness (LTI) | |||||
| No | 25,516,739 | 74.9 | 20,392,046 | 73.2 | ↓ 5,124,693 (20.1) |
| Yes | 8,530,598 | 25.1 | 7,460,216 | 26.8 | ↓ 1,070,382 (12.5) |
| Age, in years | |||||
| [0–4] | 3,325,334 | 9.8 | 2,023,230 | 7.3 | ↓ 1,302,104 (39.2) |
| [5–14] | 3,121,348 | 9.2 | 2,118,555 | 7.6 | ↓ 1,002,793 (32.1) |
| [15–44] | 10,996,596 | 32.3 | 9,306,849 | 33.4 | ↓ 1,689,747 (15.4) |
| [45–64] | 8,837,130 | 26.0 | 7,653,068 | 27.5 | ↓ 1,184,062 (13.4) |
| ≥65 | 7,766,929 | 22.8 | 6,750,560 | 24.2 | ↓ 1,016,369 (13.1) |
| Socio-demographic characteristics of prescribers | |||||
| Sex | |||||
| Male | 22,205,010 | 65.4 | 17,967,750 | 64.7 | ↓ 4,237,260 (19.1) |
| Female | 11,760,626 | 34.6 | 9,808,765 | 35.3 | ↓ 1,951,861 (16.6) |
| Age, in years | |||||
| <50 | 11,691,815 | 34.6 | 9,972,842 | 36.0 | ↓ 1,718,973 (14.7) |
| ≥50 | 22,085,071 | 65.4 | 17,699,356 | 64.0 | ↓ 4,385,715 (19.9) |
| Years of experience | |||||
| Junior ≤15 years | 11,597,693 | 34.4 | 9,930,308 | 35.9 | ↓ 1,667,385 (14.4) |
| Intermediate 15–30 years | 13,886,717 | 41.1 | 10,771,737 | 39.0 | ↓ 3,114,980 (22.4) |
| Senior ≥ 30 years | 8,310,943 | 24.6 | 6,925,732 | 25.1 | ↓ 1,385,211 (16.7) |
| Provider speciality | |||||
| General practitioners (GPs) | 26,566,106 | 78.0 | 20,786,542 | 74.6 | ↓ 5,779,564 (21.8) |
| Dental surgeons | 4,164,192 | 12.2 | 4,208,530 | 15.1 | ↑ 44,338 (1.1) |
| Paediatricians | 742,006 | 2.2 | 486,840 | 1.8 | ↓ 255,166 (34.4) |
| Dermatologists | 563,016 | 1.7 | 560,958 | 2.0 | ↓ 2058 (0.4) |
| Other specialisms | 2,012,017 | 5.9 | 1,809,392 | 6.5 | ↓ 202,625 (10.1) |
| Therapeutic class | |||||
| J01A Tetracyclines | 1,132,043 | 3.3 | 1,126,738 | 4.1 | ↓ 5305 (0.5) |
| J01C Penicillins | 17,991,482 | 52.8 | 13,820,626 | 49.6 | ↓ 4,170,856 (23.2) |
| J01CA Penicillins with extended spectrum | 13,472,862 | 39.6 | 9,897,223 | 35.5 | ↓ 3,575,639 (26.5) |
| J01CR Combinations of penicillins | 4,306,958 | 12.7 | 3,731,584 | 13.4 | ↓ 575,374 (13.3) |
| J01D Other beta-lactams | 3,425,607 | 10.1 | 2,377,932 | 8.5 | ↓ 1,047,675 (30.6) |
| J01DD 3G cephalosporins | 2,904,226 | 8.5 | 2,098,008 | 7.5 | ↓ 806,218 (27.8) |
| J01E Sulphonamides and trimethoprim | 375,785 | 1.1 | 387,661 | 1.4 | ↑ 11,876 (3.2) |
| J01F Macrolides | 5,110,174 | 15.0 | 4,371,751 | 15.7 | ↓ 738,423 (14.4) |
| J01FA10: Azithromycin | 1,637,132 | 4.8 | 1,801,862 | 6.5 | ↑ 164,730 (10.1) |
| J01M Quinolones | 1,508,069 | 5.6 | 1,339,817 | 4.8 | ↓ 168,252 (11.1) |
| J01R Combinations of antibacterials 1 | 1,934,692 | 5.7 | 1,909,135 | 6.9 | ↓ 25,557 (1.3) |
| J01X Other antibacterials | 2,550,694 | 7.5 | 2,505,787 | 9.0 | ↓ 44,907 (1.8) |
| All prescriptions | 34,047,337 | 27,852,262 | ↓ 6,195,075 (18.2) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
BARA, W.; Brun-Buisson, C.; Coignard, B.; Watier, L. Outpatient Antibiotic Prescriptions in France: Patients and Providers Characteristics and Impact of the COVID-19 Pandemic. Antibiotics 2022, 11, 643. https://doi.org/10.3390/antibiotics11050643
BARA W, Brun-Buisson C, Coignard B, Watier L. Outpatient Antibiotic Prescriptions in France: Patients and Providers Characteristics and Impact of the COVID-19 Pandemic. Antibiotics. 2022; 11(5):643. https://doi.org/10.3390/antibiotics11050643
Chicago/Turabian StyleBARA, Wilfried, Christian Brun-Buisson, Bruno Coignard, and Laurence Watier. 2022. "Outpatient Antibiotic Prescriptions in France: Patients and Providers Characteristics and Impact of the COVID-19 Pandemic" Antibiotics 11, no. 5: 643. https://doi.org/10.3390/antibiotics11050643
APA StyleBARA, W., Brun-Buisson, C., Coignard, B., & Watier, L. (2022). Outpatient Antibiotic Prescriptions in France: Patients and Providers Characteristics and Impact of the COVID-19 Pandemic. Antibiotics, 11(5), 643. https://doi.org/10.3390/antibiotics11050643