
C/MIC > 4: A Potential Instrument to Predict the Efficacy of Meropenem

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
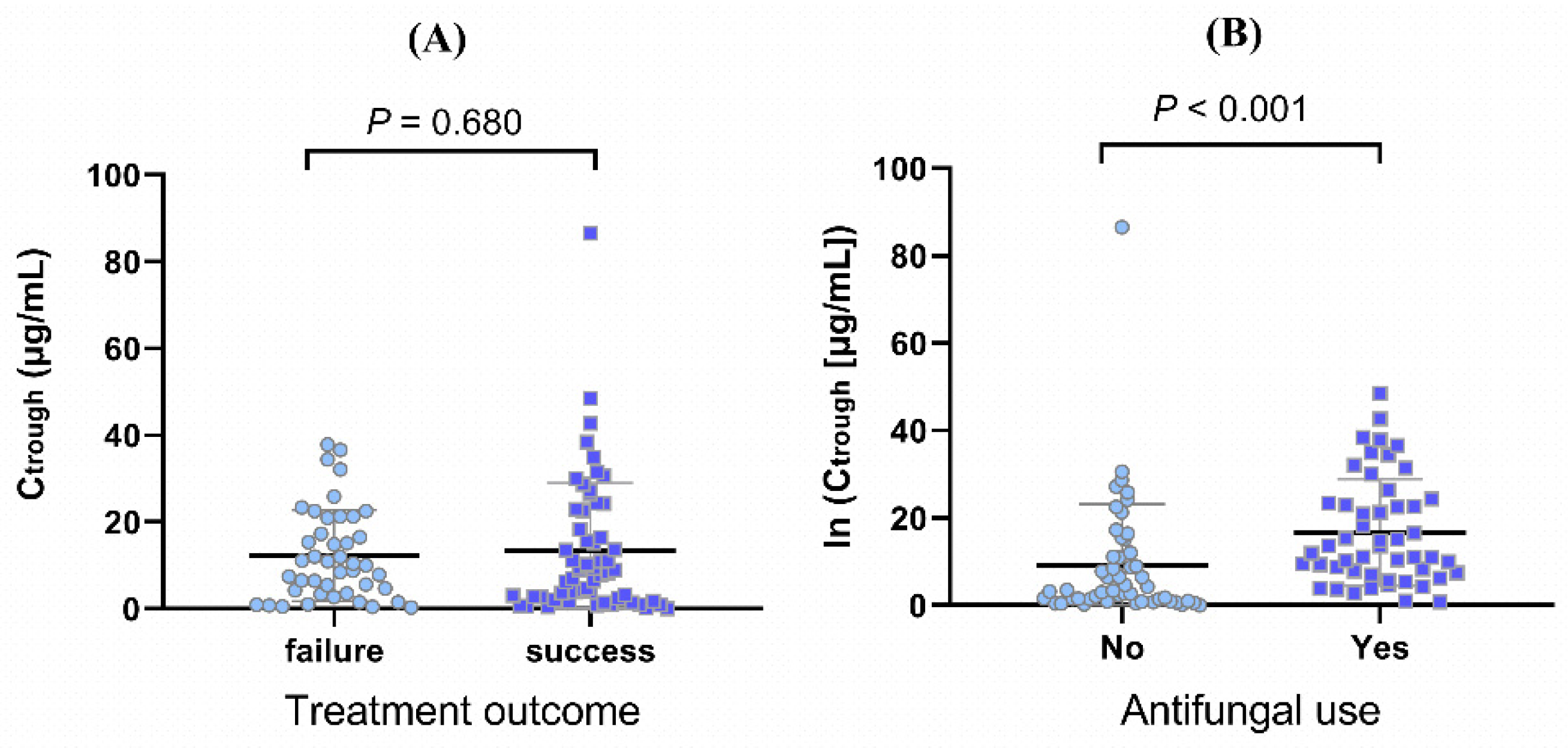
2.2. Univariate Analysis of Meropenem trough Concentration
2.3. Renal Function Indexes: Determinants of Meropenem trough Concentration
2.4. Diagnosis of the Multiple Linear Model
2.5. Ctrough/MIC > 4 Was Associated with Efficacy
2.6. Receiver Operating Characteristic Curve Analysis
3. Discussion
4. Materials and Methods
4.1. Patients and Data Collection
4.2. Blood Sampling and Analytical Assays
4.3. Determinants of Meropenem trough Concentration
4.4. Analysis of Association between Meropenem Concentration and Efficacy
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lanks, C.W.; Musani, A.I.; Hsia, D.W. Community-acquired Pneumonia and Hospital-acquired Pneumonia. Med. Clin. N. Am. 2019, 103, 487–501. [Google Scholar] [CrossRef] [PubMed]
- Muscedere, J.G.; Day, A.; Heyland, D.K. Mortality, attributable mortality and clinical events as end points for clinical trials of ventilator-associated pneumonia and hospital-acquired pneumonia. Clin. Infect. Dis. 2010, 51 (Suppl. S1), S120–S125. [Google Scholar] [CrossRef] [PubMed]
- Hraiech, S.; Alingrin, J.; Dizier, S.; Brunet, J.; Forel, J.M.; La Scola, B.; Roch, A.; Papazian, L.; Pauly, V. Time to intubation is associated with outcome in patients with community-acquired pneumonia. PLoS ONE 2013, 8, e74937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortensen, E.M.; Restrepo, M.; Anzueto, A.; Pugh, J. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am. J. Med. 2004, 117, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Ulldemolins, M.; Lisboa, T.; Koulenti, D.; Mañez, R.; Martin-Loeches, I.; De Waele, J.J.; Putensen, C.; Guven, M.; Deja, M.; et al. Determinants of prescription and choice of empirical therapy for hospital-acquired and ventilator-associated pneumonia. Eur. Respir. J. 2011, 37, 1332–1339. [Google Scholar] [CrossRef] [Green Version]
- Hansen, G.T. Continuous Evolution: Perspective on the Epidemiology of Carbapenemase Resistance Among Enterobacterales and Other Gram-Negative Bacteria. Infect. Dis. Ther. 2021, 10, 75–92. [Google Scholar] [CrossRef]
- Restrepo, M.I.; Mortensen, E.M.; Rello, J.; Brody, J.; Anzueto, A. Late admission to the ICU in patients with community-acquired pneumonia is associated with higher mortality. Chest 2010, 137, 552–557. [Google Scholar] [CrossRef] [Green Version]
- Indrajith, S.; Mukhopadhyay, A.K.; Chowdhury, G.; Farraj, D.A.A.; Alkufeidy, R.M.; Natesan, S.; Meghanathan, V.; Gopal, S.; Muthupandian, S. Molecular insights of Carbapenem resistance Klebsiella pneumoniae isolates with focus on multidrug resistance from clinical samples. J. Infect. Public Health 2021, 14, 131–138. [Google Scholar] [CrossRef]
- Dhillon, S. Meropenem/Vaborbactam: A Review in Complicated Urinary Tract Infections. Drugs 2018, 78, 1259–1270. [Google Scholar] [CrossRef] [Green Version]
- Wiseman, L.R.; Wagstaff, A.J.; Brogden, R.N.; Bryson, H.M. Meropenem: A review of its antibacterial activity, pharmacokinetic properties and clinical efficacy. Drugs 1995, 50, 73–101. [Google Scholar] [CrossRef]
- Henderson, A.; Paterson, D.L.; Chatfield, M.D.; Tambyah, P.A.; Lye, D.C.; De, P.P.; Lin, R.T.P.; Chew, K.L.; Yin, M.; Lee, T.H.; et al. Association Between Minimum Inhibitory Concentration, Beta-lactamase Genes and Mortality for Patients Treated with Piperacillin/Tazobactam or Meropenem from the MERINO Study. Clin. Infect. Dis. 2021, 73, e3842–e3850. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.T.; He, B.; Shen, N.; Liang, Y.; Sun, L.N. Meropenem Dosing Based on a Population Pharmacokinetic-Pharmacodynamic Model in Elderly Patients with Infection of the Lower Respiratory Tract. Drugs Aging 2017, 34, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Alobaid, A.S.; Wallis, S.C.; Jarrett, P.; Starr, T.; Stuart, J.; Lassig-Smith, M.; Ordóñez Mejia, J.L.; Roberts, M.S.; Lipman, J.; Roberts, J.A. Effect of Obesity on the Population Pharmacokinetics of Meropenem in Critically Ill Patients. Antimicrob. Agents Chemother. 2016, 60, 4577–4584. [Google Scholar] [CrossRef] [Green Version]
- Doh, K.; Woo, H.; Hur, J.; Yim, H.; Kim, J.; Chae, H.; Han, S.; Yim, D.S. Population pharmacokinetics of meropenem in burn patients. J. Antimicrob. Chemother. 2010, 65, 2428–2435. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef] [Green Version]
- Hartman, S.J.F.; Brüggemann, R.J.; Orriëns, L.; Dia, N.; Schreuder, M.F.; de Wildt, S.N. Pharmacokinetics and Target Attainment of Antibiotics in Critically Ill Children: A Systematic Review of Current Literature. Clin. Pharmacokinet. 2020, 59, 173–205. [Google Scholar] [CrossRef] [Green Version]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Maier, B.; Schmitt, M.V.; Hartung, N.; Huisinga, W.; Vogeser, M.; Frey, L.; et al. Role of renal function in risk assessment of target non-attainment after standard dosing of meropenem in critically ill patients: A prospective observational study. Crit. Care 2017, 21, 263. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Aziz, M.H.; Alffenaar, J.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef]
- Thémans, P.; Marquet, P.; Winkin, J.J.; Musuamba, F.T. Towards a Generic Tool for Prediction of Meropenem Systemic and Infection-Site Exposure: A Physiologically Based Pharmacokinetic Model for Adult Patients with Pneumonia. Drugs R&D 2019, 19, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Huisinga, W.; Zander, J.; Kloft, C. Development of a dosing algorithm for meropenem in critically ill patients based on a population pharmacokinetic/pharmacodynamic analysis. Int. J. Antimicrob. Agents 2019, 54, 309–317. [Google Scholar] [CrossRef]
- Jaruratanasirikul, S.; Thengyai, S.; Wongpoowarak, W.; Wattanavijitkul, T.; Tangkitwanitjaroen, K.; Sukarnjanaset, W.; Jullangkoon, M.; Samaeng, M. Population pharmacokinetics and Monte Carlo dosing simulations of meropenem during the early phase of severe sepsis and septic shock in critically ill patients in intensive care units. Antimicrob. Agents Chemother. 2015, 59, 2995–3001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Q.T.; He, B.; Zhang, C.; Zhai, S.D.; Liu, Z.Y.; Zhang, J. Pharmacokinetics and pharmacodynamics of meropenem in elderly chinese with lower respiratory tract infections: Population pharmacokinetics analysis using nonlinear mixed-effects modelling and clinical pharmacodynamics study. Drugs Aging 2011, 28, 903–912. [Google Scholar] [CrossRef] [PubMed]
- Ramon-Lopez, A.; Allen, J.M.; Thomson, A.H.; Dheansa, B.S.; James, S.E.; Hanlon, G.W.; Stewart, B.; Davies, J.G. Dosing regimen of meropenem for adults with severe burns: A population pharmacokinetic study with Monte Carlo simulations. J. Antimicrob. Chemother. 2015, 70, 882–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, J.A.; Udy, A.A.; Jarrett, P.; Wallis, S.C.; Hope, W.W.; Sharma, R.; Kirkpatrick, C.M.; Kruger, P.S.; Roberts, M.S.; Lipman, J. Plasma and target-site subcutaneous tissue population pharmacokinetics and dosing simulations of cefazolin in post-trauma critically ill patients. J. Antimicrob. Chemother. 2015, 70, 1495–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cies, J.J.; Moore, W.S.; Enache, A.; Chopra, A. Population Pharmacokinetics and Pharmacodynamic Target Attainment of Meropenem in Critically Ill Young Children. J. Pediatr. Pharmacol. Ther. 2017, 22, 276–285. [Google Scholar] [CrossRef] [Green Version]
- Usman, M.; Frey, O.R.; Hempel, G. Population pharmacokinetics of meropenem in elderly patients: Dosing simulations based on renal function. Eur. J. Clin. Pharmacol. 2017, 73, 333–342. [Google Scholar] [CrossRef]
- Hites, M.; Taccone, F.S.; Wolff, F.; Cotton, F.; Beumier, M.; De Backer, D.; Roisin, S.; Lorent, S.; Surin, R.; Seyler, L.; et al. Case-control study of drug monitoring of β-lactams in obese critically ill patients. Antimicrob. Agents Chemother. 2013, 57, 708–715. [Google Scholar] [CrossRef] [Green Version]
- Veiga, R.P.; Paiva, J.A. Pharmacokinetics-pharmacodynamics issues relevant for the clinical use of beta-lactam antibiotics in critically ill patients. Crit. Care 2018, 22, 233. [Google Scholar] [CrossRef] [Green Version]
- Udy, A.A.; Varghese, J.M.; Altukroni, M.; Briscoe, S.; McWhinney, B.C.; Ungerer, J.P.; Lipman, J.; Roberts, J.A. Subtherapeutic initial β-lactam concentrations in select critically ill patients: Association between augmented renal clearance and low trough drug concentrations. Chest 2012, 142, 30–39. [Google Scholar] [CrossRef]
- Li, C.; Du, X.; Kuti, J.L.; Nicolau, D.P. Clinical pharmacodynamics of meropenem in patients with lower respiratory tract infections. Antimicrob. Agents Chemother. 2007, 51, 1725–1730. [Google Scholar] [CrossRef] [Green Version]
- Tam, V.H.; McKinnon, P.S.; Akins, R.L.; Rybak, M.J.; Drusano, G.L. Pharmacodynamics of cefepime in patients with Gram-negative infections. J. Antimicrob. Chemother. 2002, 50, 425–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouton, J.W.; Den Hollander, J.G. Killing of Pseudomonas aeruginosa during continuous and intermittent infusion of ceftazidime in an in vitro pharmacokinetic model. Antimicrob. Agents Chemother. 1994, 38, 931–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, J.A.; Ulldemolins, M.; Roberts, M.S.; McWhinney, B.; Ungerer, J.; Paterson, D.L.; Lipman, J. Therapeutic drug monitoring of beta-lactams in critically ill patients: Proof of concept. Int. J. Antimicrob. Agents 2010, 36, 332–339. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Carrette, S.; Carlier, M.; Stove, V.; Boelens, J.; Claeys, G.; Leroux-Roels, I.; Hoste, E.; Depuydt, P.; Decruyenaere, J.; et al. Therapeutic drug monitoring-based dose optimisation of piperacillin and meropenem: A randomised controlled trial. Intensive Care Med. 2014, 40, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Alosaimy, S.; Lagnf, A.M.; Morrisette, T.; Scipione, M.R.; Zhao, J.J.; Jorgensen, S.C.J.; Mynatt, R.; Carlson, T.J.; Jo, J.; Garey, K.W.; et al. Real-world, Multicenter Experience With Meropenem-Vaborbactam for Gram-Negative Bacterial Infections Including Carbapenem-Resistant Enterobacterales and Pseudomonas aeruginosa. Open Forum Infect. Dis. 2021, 8, ofab371. [Google Scholar] [CrossRef]
- Roger, C.; Louart, B. Beta-Lactams Toxicity in the Intensive Care Unit: An Underestimated Collateral Damage? Microorganisms 2021, 9, 1505. [Google Scholar] [CrossRef]
- Imani, S.; Buscher, H.; Marriott, D.; Gentili, S.; Sandaradura, I. Too much of a good thing: A retrospective study of β-lactam concentration-toxicity relationships. J. Antimicrob. Chemother. 2017, 72, 2891–2897. [Google Scholar] [CrossRef]
- Razzazzadeh, S.; Darazam, I.A.; Hajiesmaeili, M.; Salamzadeh, J.; Mahboubi, A.; Sadeghnezhad, E.; Sahraei, Z. Investigation of pharmacokinetic and clinical outcomes of various meropenem regimens in patients with ventilator-associated pneumonia and augmented renal clearance. Eur. J. Clin. Pharmacol. 2022, 78, 823–829. [Google Scholar] [CrossRef]
- Win, E.E.; Htun, K.W.; Tragulpiankit, P.; Tangtrakultham, S.; Montakantikul, P. The Evaluation of Meropenem Dosing Regimens against ESBL-Producing Escherichia coli in ICU Patients Using Monte Carlo Simulation. Infect. Drug Resist. 2022, 15, 439–453. [Google Scholar] [CrossRef]
- Lan, J.; Wu, Z.; Wang, X.; Wang, Y.; Yao, F.; Zhao, B.X.; Wang, Y.; Chen, J.; Chen, C. Population Pharmacokinetics Analysis and Dosing Simulations Of Meropenem in Critically Ill Patients with Pulmonary Infection. J. Pharm. Sci. 2022, 22, 00025–00029. [Google Scholar] [CrossRef]
- Kahlmeter, G.; Brown, D.F.; Goldstein, F.W.; MacGowan, A.P.; Mouton, J.W.; Odenholt, I.; Rodloff, A.; Soussy, C.J.; Steinbakk, M.; Soriano, F.; et al. European Committee on Antimicrobial Susceptibility Testing (EUCAST) Technical Notes on antimicrobial susceptibility testing. Clin. Microbiol. Infect. 2006, 12, 501–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crandon, J.L.; Ariano, R.E.; Zelenitsky, S.A.; Nicasio, A.M.; Kuti, J.L.; Nicolau, D.P. Optimization of meropenem dosage in the critically ill population based on renal function. Intensive Care Med. 2011, 37, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Humphries, R.; Bobenchik, A.M.; Hindler, J.A.; Schuetz, A.N. Overview of Changes to the Clinical and Laboratory Standards Institute Performance Standards for Antimicrobial Susceptibility Testing, M100, 31st Edition. J. Clin. Microbiol. 2021, 59, e0021321. [Google Scholar] [CrossRef] [PubMed]
- Bianco, G.; Boattini, M.; Comini, S.; Iannaccone, M.; Cavallo, R.; Costa, C. Rapid determination of ceftazidime/avibactam susceptibility of carbapenemase-producing Enterobacterales directly from blood cultures: A comparative evaluation of EUCAST disc diffusion RAST and direct Etest® RAST. J. Antimicrob. Chemother. 2022, dkac092. [Google Scholar] [CrossRef]
- Van Hasselt, J.G.; Rizk, M.L.; Lala, M.; Chavez-Eng, C.; Visser, S.A.; Kerbusch, T.; Danhof, M.; Rao, G.; Van Der Graaf, P.H. Pooled population pharmacokinetic model of imipenem in plasma and the lung epithelial lining fluid. Br. J. Clin. Pharmacol. 2016, 81, 1113–1123. [Google Scholar] [CrossRef] [Green Version]
- Boucher, B.A.; Hudson, J.Q.; Hill, D.M.; Swanson, J.M.; Wood, G.C.; Laizure, S.C.; Arnold-Ross, A.; Hu, Z.Y.; Hickerson, W.L. Pharmacokinetics of Imipenem/Cilastatin Burn Intensive Care Unit Patients Undergoing High-Dose Continuous Venovenous Hemofiltration. Pharmacotherapy 2016, 36, 1229–1237. [Google Scholar] [CrossRef]
- Gonçalves-Pereira, J.; Póvoa, P. Antibiotics in critically ill patients: A systematic review of the pharmacokinetics of β-lactams. Crit. Care 2011, 15, R206. [Google Scholar] [CrossRef] [Green Version]
- Varghese, J.M.; Roberts, J.A.; Lipman, J. Antimicrobial pharmacokinetic and pharmacodynamic issues in the critically ill with severe sepsis and septic shock. Crit. Care Clin. 2011, 27, 19–34. [Google Scholar] [CrossRef]
- Mahmoudi, M.; Brenner, T.; Hatiboglu, G.; Burhenne, J.; Weiss, J.; Weigand, M.A.; Haefeli, W.E. Substantial Impairment of Voriconazole Clearance by High-Dose Meropenem in a Patient with Renal Failure. Clin. Infect. Dis. 2017, 65, 1033–1036. [Google Scholar] [CrossRef] [Green Version]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Sungurlu, S.; Balk, R.A. The Role of Biomarkers in the Diagnosis and Management of Pneumonia. Clin. Chest Med. 2018, 39, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Jiang, Z.; Li, W.H.; Wei, H.Y.; Su, G.D. Clinical significance of serum procalcitonin level monitoring on early diagnosis of severe pneumonia on children. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4300–4303. [Google Scholar] [PubMed]
- Chen, C.; Yan, M.; Hu, C.; Lv, X.; Zhang, H.; Chen, S. Diagnostic efficacy of serum procalcitonin, C-reactive protein concentration and clinical pulmonary infection score in Ventilator-Associated Pneumonia. Med. Sci. 2018, 34, 26–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porfyridis, I.; Georgiadis, G.; Vogazianos, P.; Mitis, G.; Georgiou, A. C-reactive protein, procalcitonin, clinical pulmonary infection score, and pneumonia severity scores in nursing home acquired pneumonia. Respir. Care 2014, 59, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Nunes, M.B.G.; Filho, A.C.; Alvares, V.R.C.; Meneguz-Moreno, R.; Lamas, E.; Loures, V.; Chamié, D.; Abizaid, A. CKD-EPI versus Cockcroft-Gault formula for predicting contrast-induced nephropathy following percutaneous coronary intervention in patients without significant renal impairment. Rev. Port. Cardiol. 2018, 37, 25–33. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Mathew, S.K.; Mathew, B.S.; Neely, M.N.; Naik, G.S.; Prabha, R.; Jacob, G.G.; Subramani, K.; Fleming, D.H. A Nonparametric Pharmacokinetic Approach to Determine the Optimal Dosing Regimen for 30-Minute and 3-Hour Meropenem Infusions in Critically Ill Patients. Ther. Drug Monit. 2016, 38, 593–599. [Google Scholar] [CrossRef]
- Nguyen, C.P.; Dan Do, T.N.; Bruggemann, R.; Ten Oever, J.; Kolwijck, E.; Adang, E.M.M.; Wertheim, H.F.L. Clinical cure rate and cost-effectiveness of carbapenem-sparing beta-lactams vs. meropenem for Gram-negative infections: A systematic review, meta-analysis, and cost-effectiveness analysis. Int. J. Antimicrob. Agents 2019, 54, 790–797. [Google Scholar] [CrossRef]
- Valachis, A.; Samonis, G.; Kofteridis, D.P. The role of aerosolized colistin in the treatment of ventilator-associated pneumonia: A systematic review and metaanalysis. Crit. Care Med. 2015, 43, 527–533. [Google Scholar] [CrossRef]
- Burger, R.; Guidi, M.; Calpini, V.; Lamoth, F.; Decosterd, L.; Robatel, C.; Buclin, T.; Csajka, C.; Marchetti, O. Effect of renal clearance and continuous renal replacement therapy on appropriateness of recommended meropenem dosing regimens in critically ill patients with susceptible life-threatening infections. J. Antimicrob. Chemother. 2018, 73, 3413–3422. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Treatment Success (n = 39; 60.9%) | Treatment Failure (n = 25; 39.1%) |
|---|---|---|
| Male, n (%) | 30 (76.9%) | 17 (68.0%) |
| Age (years) | 64.9 ± 15.2 | 64.0 (51.0–71.0) |
| Weight (kg) | 61.1 ± 13.0 | 64.0 (55.5–68.5) |
| APACHE II score | 17.0 (12.0–23.0) | 16.0 ± 7.7 |
| Meropenem concentration (n = 210, μg/mL) | 18.33 (5.92–33.42) | 17.47 (7.34–31.99) |
| Ctrough (n = 101, μg/mL) | 8.53 (2.39–22.69) | 10.07 (3.53–20.92) |
| Concomitant drug use (yes), n (%) | ||
| Antibiotic | 27 (69.2%) | 21 (84.0%) |
| Antifungal | 16 (41.0%) | 13 (52.0%) |
| Antiviral drug | 12 (30.8%) | 14 (56.0%) |
| Physiological and biochemical indexes | ||
| PO2 (mmHg) | 67.2 (57.1–83.8) | 67.7 (58.3–85.9) |
| PCO2 (mmHg) | 35.0 (28.9–53.4) | 38.0 (34.5–50.0) |
| [Na+] (mmol/L) | 135 ± 6.7 | 135 (131–141) |
| [Cl−] (mmol/L) | 106 ± 8.3 | 107 (101–110) |
| Hemoglobin (g/L) | 105 ± 26 | 99 ± 25 |
| Red blood cells (1012/L) | 3.5 ± 0.9 | 3.3 ± 0.9 |
| Platelets (109/L) | 166 (130–333) | 175 ± 123 |
| Alanine transaminase (U/L) | 32.5 (20.3–53.2) | 35.1 (11.9–57.8) |
| Aspartate aminotransferase (U/L) | 40.0 (26.7–65.8) | 50.5 (33.5–91.9) |
| Albumin (g/L) | 27.1 ± 5.0 | 26.9 ± 3.6 |
| Total bile acid (μmol/L) | 5.2 (3.5–12.9) | 5.4 (2.2–10.1) |
| Blood urea nitrogen (mmol/L) | 7.81 (5.19–15.96) | 9.46 (5.96–17.13) |
| Creatinine (μmol/L) | 66.7 (54.4–154.4) | 80.8 (52.7–164.7) |
| Uric acid (μmol/L) | 175.8 (112.6–345.7) | 188.6 (146.6–346.9) |
| CG-CLCR (mL/min) | 76.9 (40.2–100.9) | 74.2 (40.3–100.2) |
| Inflammatory indicators | ||
| Procalcitonin (μg/L) | 0.69 (0.14–4.08) | 0.32 (0.15–3.13) |
| C-reactive protein (mg/L) | 124.0 (93.0–214.0) | 124.0 (30.5–245.0) |
| Erythrocyte sedimentation rate (mm/h) | 74 ± 40 | 70 ± 40 |
| Temperature (°C) | 38.0 ± 1.0 | 38.2 ± 0.8 |
| C/MIC > 4 (yes), n (%, n = 139) | 55 (68.8%, 55/80) | 23 (39.0%, 23/59) |
| Ctrough/MIC > 4 (yes), n (%, n = 70) | 20 (48.8%, 20/41) | 6 (20.7%, 6/29) |
| MIC (yes), n (%, n = 70) | ||
| ≤1 | 14 (34.1%, 14/41) | 1 (3.4%, 1/29) |
| 2 | 12 (29.3%, 12/41) | 4 (13.8%, 4/29) |
| ≥8 | 15 (36.6%, 15/41) | 24 (82.8%, 24/29) |
| Variable | Coefficient Index | p-Value |
|---|---|---|
| Gender | −0.192 | 0.055 |
| Age | 0.388 ** | <0.001 |
| Weight | −0.147 | 0.143 |
| APACHE II score | 0.086 | 0.391 |
| dose | −0.289 ** | 0.003 |
| infusion duration | 0.207 * | 0.038 |
| Concomitant drug use (yes), n (%) | ||
| Antibiotic | 0.034 | 0.735 |
| Antifungal | 0.424 ** | <0.001 |
| Antiviral drug | 0.110 | 0.275 |
| Physiological and biochemical indexes | ||
| PO2 | 0.070 | 0.490 |
| PCO2 | −0.140 | 0.164 |
| [Na+] | 0.402 ** | <0.001 |
| [Cl−] | 0.093 | 0.353 |
| Hemoglobin | −0.429 ** | <0.001 |
| Red blood cells | −0.416 ** | <0.001 |
| Platelets | −0.040 | 0.694 |
| Alanine transaminase | −0.110 | 0.274 |
| Aspartate aminotransferase | 0.126 | 0.211 |
| Albumin | 0.237 * | 0.017 |
| Total bile acid | −0.010 | 0.918 |
| Blood urea nitrogen | 0.606 ** | <0.001 |
| Creatinine | 0.548 ** | <0.001 |
| Uric acid | 0.560 ** | <0.001 |
| CG-CLCR | −0.694 ** | <0.001 |
| Inflammatory indicators | ||
| Procalcitonin | 0.332 ** | 0.001 |
| C-reactive protein | 0.020 | 0.841 |
| Erythrocyte sedimentation rate | 0.206 * | 0.038 |
| Temperature | 0.037 | 0.713 |
| Variable | Coefficient | Standardized Coefficient | T | p-Value | VIF |
|---|---|---|---|---|---|
| Blood urea nitrogen | 0.051 | 0.390 | 4.820 | <0.001 | 1.396 |
| CG−CLCR | −0.009 | −0.386 | −4.801 | <0.001 | 1.382 |
| Albumin | 0.071 | 0.232 | 3.243 | 0.002 | 1.088 |
| Infusion duration | 0.495 | 0.195 | 2.839 | 0.006 | 1.008 |
| Constant value | −0.914 | −1.154 | 0.251 | ||
| F | 29.360 | ||||
| p | <0.001 | ||||
| R2 | 0.531 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Xiao, C.; Hou, J.; Wu, J.; Xiao, Y.; Zhang, B.; Sandaradura, I.; Luo, H.; Li, J.; Yan, M. C/MIC > 4: A Potential Instrument to Predict the Efficacy of Meropenem. Antibiotics 2022, 11, 670. https://doi.org/10.3390/antibiotics11050670
Zhao Y, Xiao C, Hou J, Wu J, Xiao Y, Zhang B, Sandaradura I, Luo H, Li J, Yan M. C/MIC > 4: A Potential Instrument to Predict the Efficacy of Meropenem. Antibiotics. 2022; 11(5):670. https://doi.org/10.3390/antibiotics11050670
Chicago/Turabian StyleZhao, Yichang, Chenlin Xiao, Jingjing Hou, Jiamin Wu, Yiwen Xiao, Bikui Zhang, Indy Sandaradura, Hong Luo, Jinhua Li, and Miao Yan. 2022. "C/MIC > 4: A Potential Instrument to Predict the Efficacy of Meropenem" Antibiotics 11, no. 5: 670. https://doi.org/10.3390/antibiotics11050670
APA StyleZhao, Y., Xiao, C., Hou, J., Wu, J., Xiao, Y., Zhang, B., Sandaradura, I., Luo, H., Li, J., & Yan, M. (2022). C/MIC > 4: A Potential Instrument to Predict the Efficacy of Meropenem. Antibiotics, 11(5), 670. https://doi.org/10.3390/antibiotics11050670