
Impact of Three Nonsurgical, Full-Mouth Periodontal Treatments on Total Bacterial Load and Selected Pathobionts

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Clinical Benefit of the Three Full-Mouth Debridement Concepts in Comparison to Q-SRP
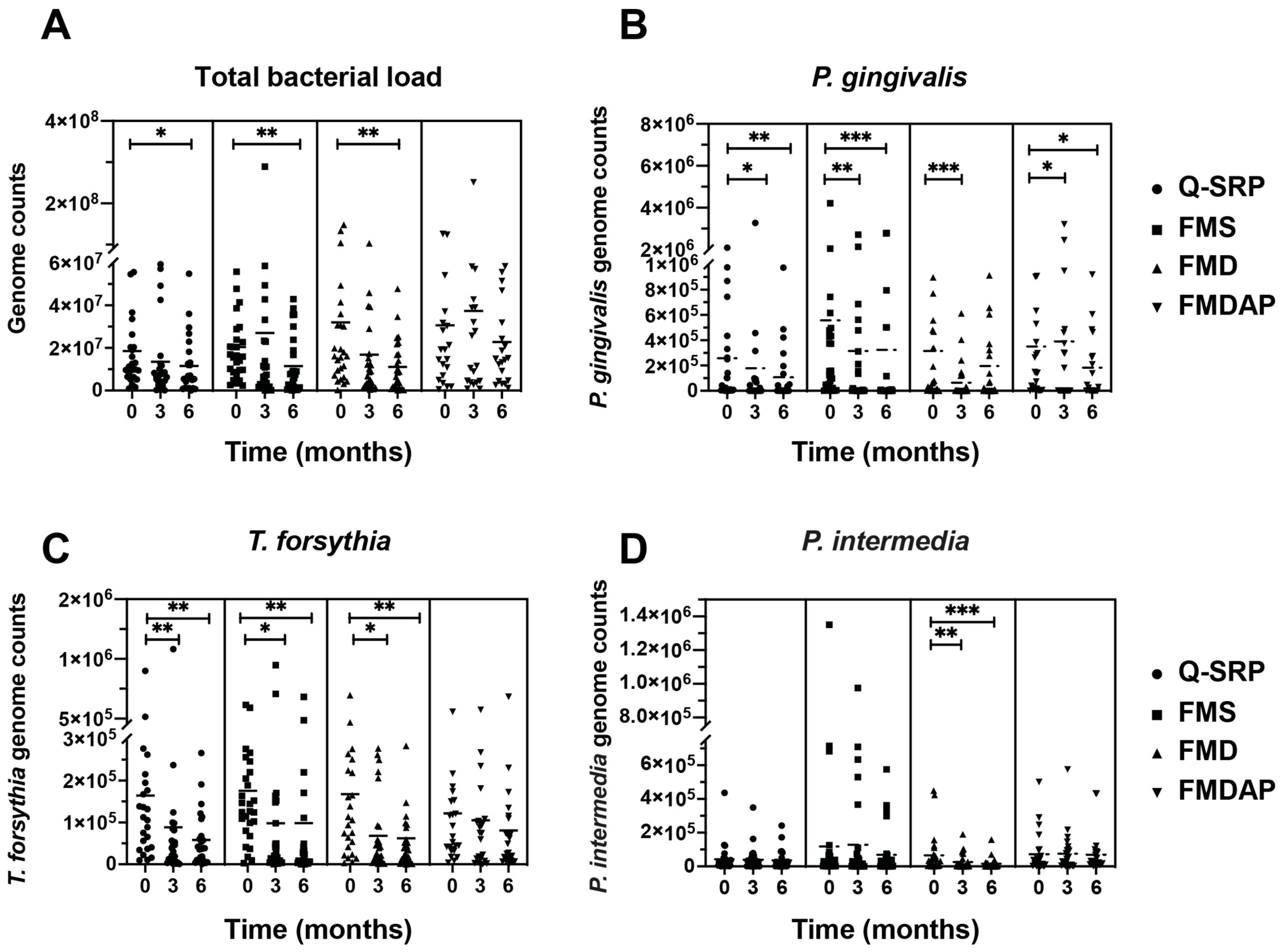
2.2. Reduction in Total Bacterial Load and Periodontal Pathobionts
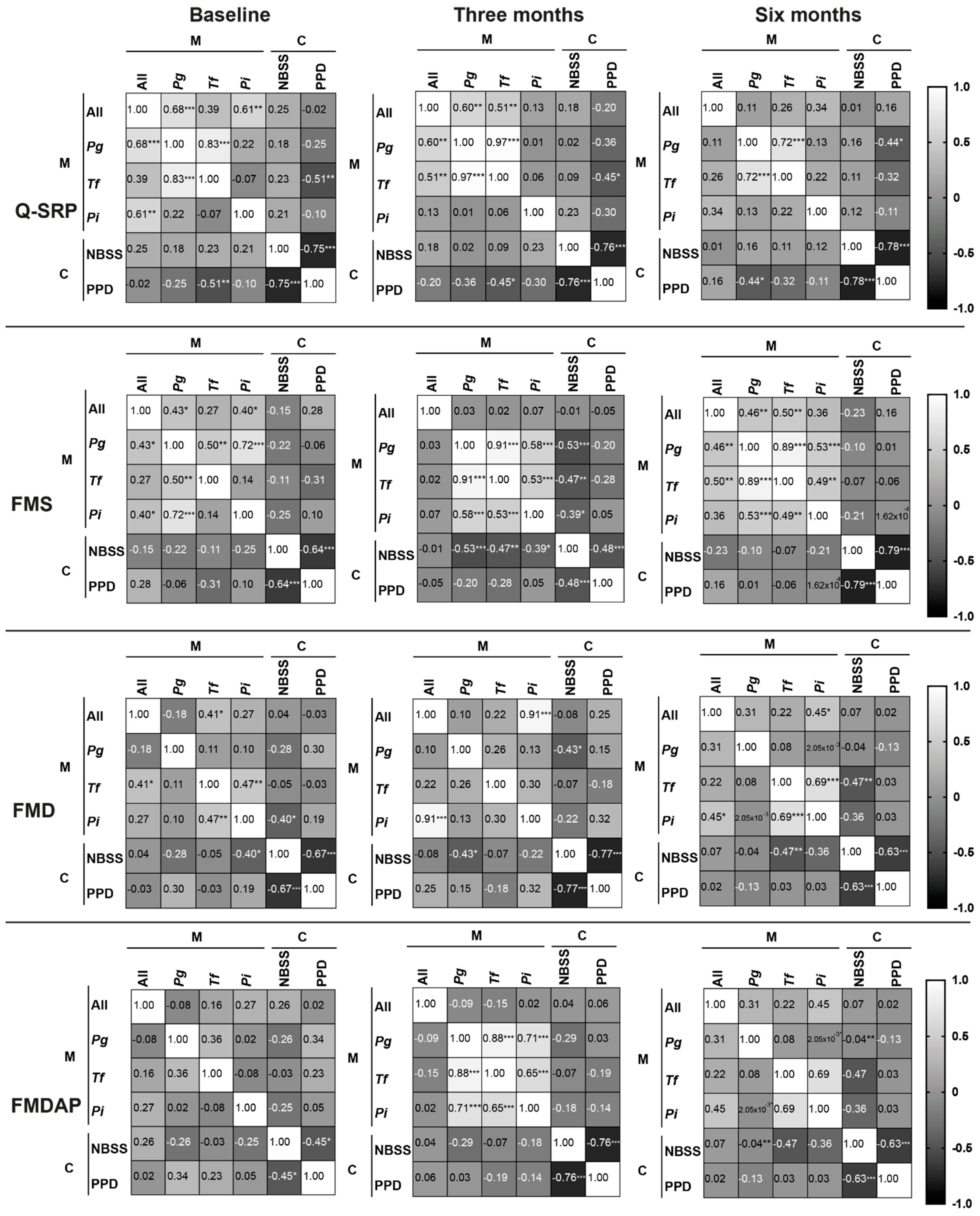
2.3. Correlation between Microbiological and Clinical Outcomes
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Microbiological Analysis
4.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Fragkioudakis, I.; Riggio, M.P.; Apatzidou, D.A. Understanding the microbial components of periodontal diseases and periodontal treatment-induced microbiological shifts. J. Med. Microbiol. 2021, 70, 001247. [Google Scholar] [CrossRef] [PubMed]
- Kornman, K.S. Contemporary approaches for identifying individual risk for periodontitis. Periodontology 2000 2018, 78, 12–29. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, R.; Al-Sabbagh, M.; Dawson III, D.; Ebersole, J.L. Integrated biomarker profiling of smokers with periodontitis. J. Clin. Periodontol. 2017, 44, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Haffajee, A.D.; Socransky, S.S.; Patel, M.R.; Song, X. Microbial complexes in supragingival plaque. Oral Microbiol. Immunol. 2008, 23, 196–205. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Dzink, J.L. Relationship of subgingival microbial complexes to clinical features at the sampled sites. J. Clin. Periodontol. 1988, 15, 440–444. [Google Scholar] [CrossRef]
- Fine, D.H.; Patil, A.G.; Velusamy, S.K. Aggregatibacter Actinomycetemcomitans (Aa) under the radar: Myths and misunderstandings of Aa and its role in aggressive periodontitis. Front. Immunol. 2019, 10, 728. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Quirynen, M.; Mongardini, C.; van Steenberghe, D. The effect of a 1-stage full-mouth disinfection on oral malodor and microbial colonization of the tongue in periodontitis patients. A pilot study. J. Periodontol. 1998, 69, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Eberhard, J.; Jepsen, S.; Jervøe-Storm, P.-M.; Needleman, I.; Worthington, H.V. Full-mouth Treatment Modalities (within 24 Hours) for Chronic Periodontitis in Adults. Cochrane Database Syst. Rev. 2015, 4, 1465–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, J.M.; Yekta-Michael, S.S.; Schittenhelm, F.; Reichert, S.; Kupietz, D.; Dommisch, H.; Kasaj, A.; Wied, S.; Vela, O.-C.; Stratul, S.-I. Comparison of three full-mouth concepts for the non-surgical treatment of stage III and IV periodontitis: A randomized controlled trial. J. Clin. Periodontol. 2021, 48, 1516–1527. [Google Scholar] [CrossRef] [PubMed]
- Schulz, S.; Stein, J.M.; Schumacher, A.; Kupitz, D.; Michael, S.; Schittenhelm, F.; Conrads, G.; Schaller, H.-G.; Reichert, S. Non-surgical periodontal treatment options and their impact on subgingival microbiome. J. Clin. Med. 2022, 11, 1187. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Teughels, W.; Soete, M.D.; Steenberghe, D.V. Topical antiseptics and antibiotics in the initial therapy of chronic adult periodontitis: Microbiological aspects. Periodontology 2002, 28, 72–90. [Google Scholar] [CrossRef]
- Apatzidou, D.A.; Riggio, M.P.; Kinane, D.F. Quadrant root planing versus same-day full-mouth root planing. J. Clin. Periodontol. 2004, 31, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.S.; Lourenção, D.S.; Lima Neto, L.G.; Pannuti, C.M.; Crespo Hirata, R.D.; Hirata, M.H.; Lotufo, R.F.M.; De Micheli, G. Clinical and microbiologic evaluation, by real-time polymerase chain reaction, of non-surgical treatment of aggressive periodontitis associated with amoxicillin and metronidazole. J. Periodontol. 2012, 83, 744–752. [Google Scholar] [CrossRef]
- Spooner, R.; Weigel, K.M.; Harrison, P.L.; Lee, K.; Cangelosi, G.A.; Yilmaz, Ö. In Situ anabolic activity of periodontal pathogens Porphyromonas Gingivalis and Filifactor Alocis in chronic periodontitis. Sci. Rep. 2016, 6, 33638. [Google Scholar] [CrossRef] [Green Version]
- Graziani, F.; Cei, S.; Orlandi, M.; Gennai, S.; Gabriele, M.; Filice, N.; Nisi, M.; D’Aiuto, F. Acute-phase response following full-mouth versus quadrant non-surgical periodontal treatment: A randomized clinical trial. J. Clin. Periodontol. 2015, 42, 843–852. [Google Scholar] [CrossRef]
- Thöne-Mühling, M.; Swierkot, K.; Nonnenmacher, C.; Mutters, R.; Flores-de-Jacoby, L.; Mengel, R. Comparison of two full-mouth approaches in the treatment of peri-implant mucositis: A pilot study. Clin. Oral Implant. Res. 2010, 21, 504–512. [Google Scholar] [CrossRef]
- Afacan, B.; Çınarcık, S.; Gürkan, A.; Özdemir, G.; İlhan, H.A.; Vural, C.; Köse, T.; Emingil, G. Full-mouth disinfection effects on gingival fluid calprotectin, osteocalcin, and N-Telopeptide of Type I collagen in severe periodontitis. J. Periodontol. 2020, 91, 638–650. [Google Scholar] [CrossRef]
- Löe, H. The gingival index, the plaque index and the retention index systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Nadkarni, M.A.; Martin, F.E.; Jacques, N.A.; Hunter, N. Determination of bacterial load by real-time PCR using a broad-range (universal) probe and primers set. Microbiology 2002, 148, 257–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, U.; Rogall, T.; Blöcker, H.; Emde, M.; Böttger, E.C. Isolation and direct complete nucleotide determination of entire genes. characterization of a gene coding for 16S ribosomal RNA. Nucleic Acids Res. 1989, 17, 7843–7853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conrads, G.; Mutters, R.; Fischer, J.; Brauner, A.; Lütticken, R.; Lampert, F. PCR reaction and dot-blot hybridization to monitor the distribution of oral pathogens within plaque samples of periodontally healthy individuals. J. Periodontol. 1996, 67, 994–1003. [Google Scholar] [CrossRef]
- Jansen, P.M.; Abdelbary, M.M.H.; Conrads, G. A concerted probiotic activity to inhibit periodontitis-associated bacteria. PLoS ONE 2021, 16, e0248308. [Google Scholar] [CrossRef]
- Conrads, G.; Flemmig, T.F.; Seyfarth, I.; Lampert, F.; Lütticken, R. Simultaneous detection of Bacteroides Forsythus and Prevotella intermedia by 16S RRNA gene-directed multiplex PCR. J. Clin. Microbiol. 1999, 37, 1621–1624. [Google Scholar] [CrossRef] [Green Version]
- Slots, J.; Ashimoto, A.; Flynn, M.J.; Li, G.; Chen, C. Detection of Putative Periodontal Pathogens in Subgingival Specimens by 16S Ribosomal DNA Amplification with the Polymerase Chain Reaction. Clin. Infect. Dis. 1995, 20, S304–S307. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Q-SRP (n = 25) | FMS (n = 28) | FMD (n = 27) | FMDAP (n = 25) |
|---|---|---|---|---|
| Age (years) | 61.1 ± 9.9 | 56.4 ± 10.4 | 59.2 ± 12.4 | 55.0 ± 11.8 |
| Gender (male/female) | 19/6 | 17/11 | 15/12 | 13/12 |
| Smokers (n) | 6 | 8 | 8 | 3 |
| Variable | Timepoint | Q-SRP (n = 25) | FMS (n = 28) | FMD (n = 27) | FMDAP (n = 25) |
|---|---|---|---|---|---|
| PI | Baseline | 1.21 ± 0.52 | 1.17 ± 0.60 | 1.17 ± 0.54 | 1.23 ± 0.68 |
| 3 months | 0.75 ± 0.43 | 0.79 ± 0.45 | 0.50 ± 0.40 | 0.46 ± 0.35 | |
| 6 months | 0.84 ± 0.51 | 0.84 ± 0.52 | 0.76 ± 0.48 | 0.43 ± 0.32 | |
| GI | Baseline | 1.08 ± 0.56 | 1.09 ± 0.65 | 1.07 ± 0.54 | 1.11 ± 0.47 |
| 3 months | 0.73 ± 0.54 | 0.71 ± 0.58 | 0.51 ± 0.41 | 0.37 ± 0.36 | |
| 6 months | 0.78 ± 0.56 | 0.68 ± 0.47 | 0.48 ± 0.36 | 0.34 ± 0.25 | |
| PPD (mm) | Baseline | 3.75 ± 0.68 | 3.74 ± 0.54 | 4.09 ± 0.61 | 4.09 ± 0.69 |
| 3 months | 3.33 ± 0.60 | 3.32 ± 0.44 | 3.45 ± 0.57 | 3.36 ± 0.71 | |
| 6 months | 3.32 ± 0.55 | 3.31 ± 0.53 | 3.34 ± 0.91 | 3.33 ± 0.73 | |
| CAL (mm) | Baseline | 4.32 ± 0.85 | 4.23 ± 0.71 | 4.92 ± 0.89 | 4.92 ± 1.01 |
| 3 months | 3.91 ± 0.73 | 3.90 ± 0.64 | 4.40 ± 0.83 | 4.37 ± 1.09 | |
| 6 months | 3.94 ± 0.70 | 3.92 ± 0.76 | 4.34 ± 0.91 | 4.38 ± 1.14 | |
| BOP (%) | Baseline | 33.33 ± 18.34 | 34.56 ± 19.10 | 34.79 ± 15.23 | 40.60 ± 22.30 |
| 3 months | 16.39 ± 15.70 | 17.37 ± 15.10 | 12.50 ± 9.22 | 12.80 ± 11.56 | |
| 6 months | 19.33 ± 15.71 | 16.30 ± 14.76 | 14.78 ± 12.46 | 11.91 ± 10.43 | |
| NBSS (%) | Baseline | 57.48 ± 20.64 | 56.37 ± 19.65 | 53.20 ± 18.76 | 49.83 ± 20.54 |
| 3 months | 73.80 ± 17.13 | 74.47 ± 15.63 | 76.62 ± 14.96 | 77.37 ± 15.70 | |
| 6 months | 72.42 ± 16.82 | 76.19 ± 16.63 | 75.39 ± 16.18 | 79.26 ± 14.95 |
| Target | Primer | Sequence 5′–3′ | Amplicon Size (bp) | Ta (°C) | Reference |
|---|---|---|---|---|---|
| All bacterial species | Nadkarni F | TCCTACGGGAGGCAGCAGT | 466 | 60 | [22] |
| Nadkarni R | GGACTACCAGGGTATCTAATCCTGTT | ||||
| Forward primer for all following species-specific qPCRs | pF-1 | AGAGTTTGATCCTGGCTCAG | [23] | ||
| P. gingivalis | Pg-R | CAATACTCGTATCGCCCGTTATTC | 478 | 59 | [24] |
| A. actinomycetemcomitans | Aa-R | GGCATGCTATTAACACAC | 469 | 54 | [25] |
| P. intermedia | Pi-R | GTTGCGTGCACTCAAGTCCGCC | 660 | 56 | [26] |
| T. forsythia | Tf-R | TGCTTCAGTGTCAGTTATACCT | 478 | 56 | [27] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelbary, M.M.H.; Schittenhelm, F.; Yekta-Michael, S.S.; Reichert, S.; Schulz, S.; Kasaj, A.; Braun, A.; Conrads, G.; Stein, J.M. Impact of Three Nonsurgical, Full-Mouth Periodontal Treatments on Total Bacterial Load and Selected Pathobionts. Antibiotics 2022, 11, 686. https://doi.org/10.3390/antibiotics11050686
Abdelbary MMH, Schittenhelm F, Yekta-Michael SS, Reichert S, Schulz S, Kasaj A, Braun A, Conrads G, Stein JM. Impact of Three Nonsurgical, Full-Mouth Periodontal Treatments on Total Bacterial Load and Selected Pathobionts. Antibiotics. 2022; 11(5):686. https://doi.org/10.3390/antibiotics11050686
Chicago/Turabian StyleAbdelbary, Mohamed M. H., Florian Schittenhelm, Sareh Said Yekta-Michael, Stefan Reichert, Susanne Schulz, Adrian Kasaj, Andreas Braun, Georg Conrads, and Jamal M. Stein. 2022. "Impact of Three Nonsurgical, Full-Mouth Periodontal Treatments on Total Bacterial Load and Selected Pathobionts" Antibiotics 11, no. 5: 686. https://doi.org/10.3390/antibiotics11050686
APA StyleAbdelbary, M. M. H., Schittenhelm, F., Yekta-Michael, S. S., Reichert, S., Schulz, S., Kasaj, A., Braun, A., Conrads, G., & Stein, J. M. (2022). Impact of Three Nonsurgical, Full-Mouth Periodontal Treatments on Total Bacterial Load and Selected Pathobionts. Antibiotics, 11(5), 686. https://doi.org/10.3390/antibiotics11050686