
Assessing, Pricing and Funding Point-of-Care Diagnostic Tests for Community-Acquired Acute Respiratory Tract Infections–Overview of Policies Applied in 17 European Countries



Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Countries and Scope of Setting
2.2. Framework
2.3. Data Collection and Validation
3. Results
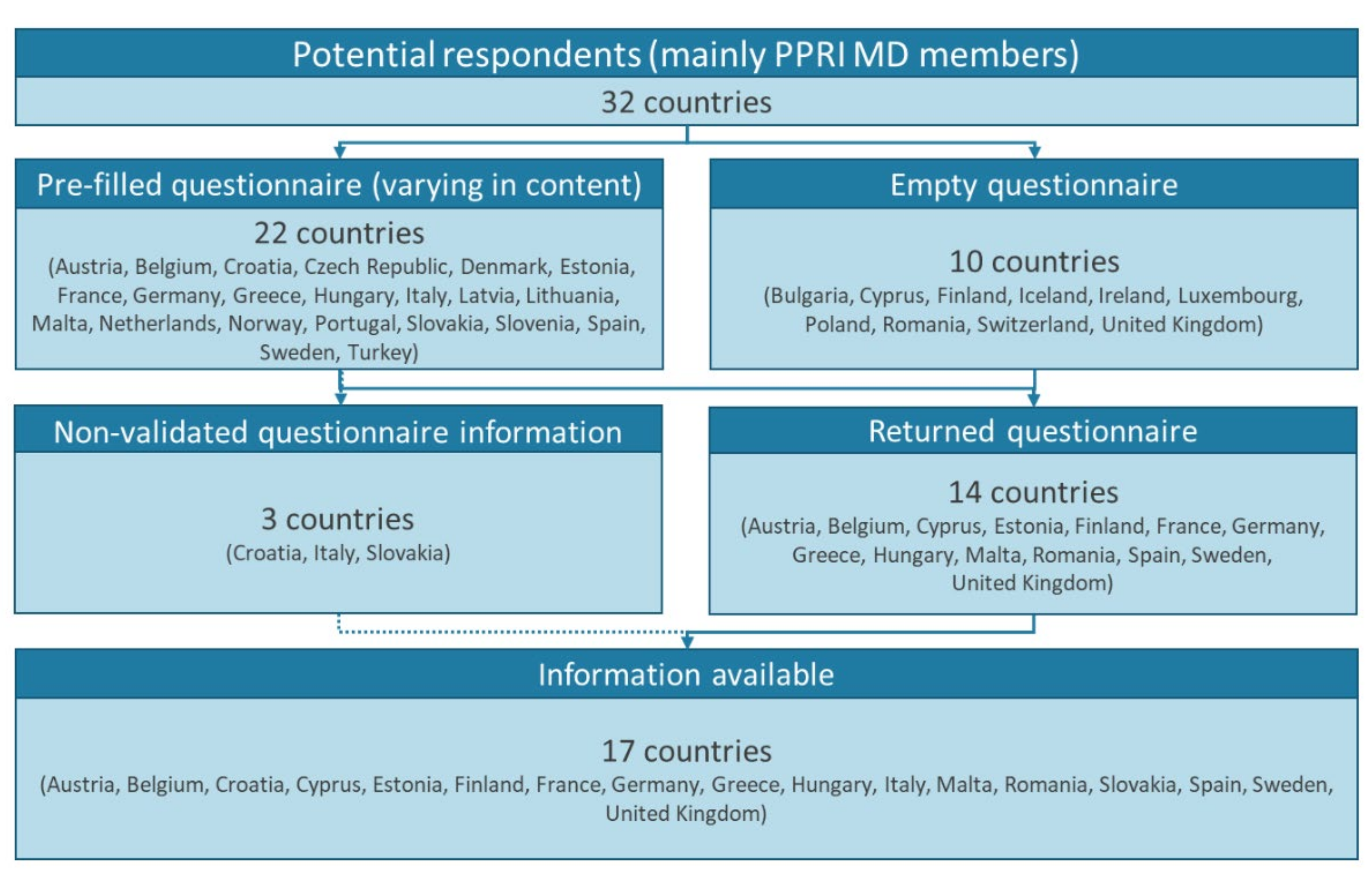
3.1. Included Countries
3.2. Use of HTA
3.3. Pricing Policies
3.4. Funding Policies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antoñanzas, F.; Goossens, H. The economics of antibiotic resistance: A claim for personalised treatments. Eur. J. Health Econ. 2019, 20, 483–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoñanzas, F.; Juárez-Castelló, C.A.; Rodríguez-Ibeas, R. Using point-of-care diagnostic testing for improved antibiotic prescription: An economic model. Health Econ. Rev. 2021, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Lin, S.; Zhang, H.; Liang, L.; Shen, S. Methods of Respiratory Virus Detection: Advances towards Point-of-Care for Early Intervention. Micromachines 2021, 12, 697. [Google Scholar] [CrossRef]
- Essack, S.; Bell, J.; Burgoyne, D.; Tongrod, W.; Duerden, M.; Sessa, A.; Altiner, A.; Shephard, A. Point-of-Care Testing for Pharyngitis in the Pharmacy. Antibiotics 2020, 9, 743. [Google Scholar] [CrossRef]
- Vaezipour, N.; Fritschi, N.; Brasier, N.; Bélard, S.; Domínguez, J.; Tebruegge, M.; Portevin, D.; Ritz, N. Towards Accurate Point-of-Care Tests for Tuberculosis in Children. Pathogens 2022, 11, 327. [Google Scholar] [CrossRef]
- Etienne, E.E.; Nunna, B.B.; Talukder, N.; Wang, Y.; Lee, E.S. COVID-19 Biomarkers and Advanced Sensing Technologies for Point-of-Care (POC) Diagnosis. Bioengineering 2021, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, M.; Razavi Bazaz, S.; Zhand, S.; Sayyadi, N.; Jin, D.; Stewart, M.P.; Ebrahimi Warkiani, M. Point of Care Diagnostics in the Age of COVID-19. Diagnostics 2021, 11, 9. [Google Scholar] [CrossRef] [PubMed]
- Strömer, A.; Rose, R.; Schäfer, M.; Schön, F.; Vollersen, A.; Lorentz, T.; Fickenscher, H.; Krumbholz, A. Performance of a Point-of-Care Test for the Rapid Detection of SARS-CoV-2 Antigen. Microorganisms 2021, 9, 58. [Google Scholar] [CrossRef] [PubMed]
- Shaffaf, T.; Forouhi, S.; Ghafar-Zadeh, E. Towards Fully Integrated Portable Sensing Devices for COVID-19 and Future Global Hazards: Recent Advances, Challenges, and Prospects. Micromachines 2021, 12, 915. [Google Scholar] [CrossRef]
- Hunter, R. Cost-Effectiveness of Point-of-Care C-Reactive Protein Tests for Respiratory Tract Infection in Primary Care in England. Adv. Ther. 2015, 32, 69–85. [Google Scholar] [CrossRef] [Green Version]
- Cals, J.W.L.; Schot, M.J.C.; de Jong, S.A.M.; Dinant, G.-J.; Hopstaken, R.M. Point-of-Care C-Reactive Protein Testing and Antibiotic Prescribing for Respiratory Tract Infections: A Randomized Controlled Trial. Ann. Fam. Med. 2010, 8, 124–133. [Google Scholar] [CrossRef]
- Martínez-González, N.A.; Keizer, E.; Plate, A.; Coenen, S.; Valeri, F.; Verbakel, J.Y.J.; Rosemann, T.; Neuner-Jehle, S.; Senn, O. Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: Systematic Review and Meta-Analysis of Randomised Controlled Trials. Antibiotics 2020, 9, 610. [Google Scholar] [CrossRef]
- Minnaard, M.C.; van de Pol, A.C.; Hopstaken, R.M.; van Delft, S.; Broekhuizen, B.D.; Verheij, T.J.; de Wit, N.J. C-reactive protein point-of-care testing and associated antibiotic prescribing. Fam. Pract. 2016, 33, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Chen, R.; Wu, T.; Wei, X.; Guo, A. Association between point-of-care CRP testing and antibiotic prescribing in respiratory tract infections: A systematic review and meta-analysis of primary care studies. Br. J. Gen. Pract. 2013, 63, e787–e794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemiengre, M.B.; Verbakel, J.Y.; Colman, R.; Van Roy, K.; De Burghgraeve, T.; Buntinx, F.; Aertgeerts, B.; De Baets, F.; De Sutter, A. Point-of-care CRP matters: Normal CRP levels reduce immediate antibiotic prescribing for acutely ill children in primary care: A cluster randomized controlled trial. Scand. J. Prim. Health Care 2018, 36, 423–436. [Google Scholar] [CrossRef] [Green Version]
- Oppong, R.; Jit, M.; Smith, R.D.; Butler, C.C.; Melbye, H.; Mölstad, S.; Coast, J. Cost-effectiveness of point-of-care C-reactive protein testing to inform antibiotic prescribing decisions. Br. J. Gen. Pract. 2013, 63, e465–e471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers Van Katwyk, S.; Grimshaw, J.M.; Nkangu, M.; Nagi, R.; Mendelson, M.; Taljaard, M.; Hoffman, S.J. Government policy interventions to reduce human antimicrobial use: A systematic review and evidence map. PLoS Med. 2019, 16, e1002819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renwick, M.J.; Brogan, D.; Mossialos, E. A systematic review and critical assessment of incentive strategies for discovery and development of novel antibiotics. J. Antibiot. 2015, 69, 73–88. [Google Scholar] [CrossRef] [Green Version]
- Anderson, M.; Cecchini, M.; Mossialos, E. Challenges to Tackling Antimicrobial Resistance; Cambridge University Press: Cambridge, UK, 2019. [Google Scholar]
- Bauer, K.A.; Perez, K.K.; Forrest, G.N.; Goff, D.A. Review of Rapid Diagnostic Tests Used by Antimicrobial Stewardship Programs. Clin. Infect. Dis. 2014, 59, S134–S145. [Google Scholar] [CrossRef]
- Holmes, E.A.F.; Harris, S.D.; Hughes, A.; Craine, N.; Hughes, D.A. Cost-Effectiveness Analysis of the Use of Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing in Primary Care. Antibiotics 2018, 7, 106. [Google Scholar] [CrossRef] [Green Version]
- Mitsakakis, K.; Kaman, W.E.; Elshout, G.; Specht, M.; Hays, J.P. Challenges in identifying antibiotic resistance targets for point-of-care diagnostics in general practice. Future Microbiol. 2018, 13, 1157–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.F.; Hughes, D.A. Challenges for Economic Evaluation of Health Care Strategies to Contain Antimicrobial Resistance. Antibiotics 2019, 8, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Parliament; Council of the European Union. Regulation (EU) 2017/746 of the European Parliament and of the Council of 5 April 2017 on In Vitro Diagnostic Medical Devices and Repealing Directive 98/79/EC and Commission Decision 2010/227/EU; European Parliament: Strasbourg, France; Council of the European Union: Strasbourg, France, 2017. [Google Scholar]
- Zhou, Y.-J.; Wang, G.; Tang, Y.-W. Companion diagnostics: New opportunities for safe and effective anti-infectious disease therapies. Emerg. Microbes Infect. 2018, 7, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Leopold, C.; Vogler, S.; Habl, C.; Mantel-Teeuwisse, A.K.; Espin, J. Personalised medicine as a challenge for public pricing and reimbursement authorities—A survey among 27 European countries on the example of trastuzumab. Health Policy 2013, 113, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Govaerts, L.; Simoens, S.; Van Dyck, W.; Huys, I. Shedding Light on Reimbursement Policies of Companion Diagnostics in European Countries. Value Health 2020, 23, 606–615. [Google Scholar] [CrossRef] [Green Version]
- Miller, I.; Ashton-Chess, J.; Spolders, H.; Fert, V.; Ferrara, J.; Kroll, W.; Askaa, J.; Larcier, P.; Terry, P.F.; Bruinvels, A.; et al. Market access challenges in the EU for high medical value diagnostic tests. Pers. Med. 2011, 8, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dailey, P.J.; Elbeik, T.; Holodniy, M. Companion and complementary diagnostics for infectious diseases. Expert Rev. Mol. Diagn. 2020, 20, 619–636. [Google Scholar] [CrossRef]
- Vogler, S. Fair prices for medicines? Exploring competent authorities’ and public payers’ preferences on pharmaceutical policies. Empirica 2019, 46, 443–469. [Google Scholar] [CrossRef]
- Vogler, S.; Zimmermann, N.; Haasis, M.A. PPRI Report 2018: Pharmaceutical Pricing and Reimbursement Policies in 47 PPRI Network Member Countries; Gesundheit Österreich GmbH (GÖG/Austrian National Public Health Institute): Vienna, Austria; WHO Collaborating Centre for Pricing and Reimbursement Policies: Vienna, Austria, 2019. [Google Scholar]
- Vogler, S.; Schneider, P.; Zuba, M.; Busse, R.; Panteli, D. Policies to Encourage the Use of Biosimilars in European Countries and Their Potential Impact on Pharmaceutical Expenditure. Front. Pharmacol. 2021, 12, 1479. [Google Scholar] [CrossRef]
- Moorkens, E.; Vulto, A.G.; Huys, I.; Dylst, P.; Godman, B.; Keuerleber, S.; Claus, B.; Dimitrova, M.; Petrova, G.; Sović-Brkičić, L.; et al. Policies for biosimilar uptake in Europe: An overview. PLoS ONE 2017, 12, e0190147. [Google Scholar] [CrossRef] [Green Version]
- Vogler, S.; Haasis, A.; Dedet, G.; Lam, J.; Bak Pedersen, H. Medicines Reimbursement Policies in Europe; World Health Organization Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- WHO. WHO Guideline on Country Pharmaceutical Pricing Policies, 2nd ed.; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Access to New Medicines in Europe: Technical Review of Policy Initiatives and Opportunities for Collaboration and Research; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- Wettstein, D.J.; Boes, S. Effectiveness of National Pricing Policies for Patent-Protected Pharmaceuticals in the OECD: A Systematic Literature Review. Appl. Health Econ. Health Policy 2018, 17, 143–162. [Google Scholar] [CrossRef] [PubMed]
- Vogler, S.; Paris, V.; Panteli, D. Ensuring Access to Medicines: How to Redesign Pricing, Reimbursement and Procurement? WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Webb, E.; Richardson, E.; Vogler, S.; Panteli, D. What Are the Implications of Policies Increasing Transparency of Prices Paid for Pharmaceuticals? WHO Regional Office for Europe: Copenhagen, Denmark, 2022. [Google Scholar]
- Vogler, S.; Lepuschütz, L.; Schneider, P.; Stühlinger, V. Study on Enhanced Cross-Country Coordination in the Area of Pharmaceutical Product Pricing; Publications Office of the European Union: Brussels, Belgium, 2016. [Google Scholar]
- WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies. Glossary of Pharmaceutical Terms; Gesundheit Österreich (GÖG/Austrian National Public Health Institute): Vienna, Austria, 2022. [Google Scholar]
- Vogler, S.; Leopold, C.; Zimmermann, N.; Habl, C.; de Joncheere, K. The Pharmaceutical Pricing and Reimbursement Information (PPRI) initiative–experiences from engaging with pharmaceutical policy makers. Health Policy Technol. 2014, 3, 139–148. [Google Scholar] [CrossRef]
- Vogler, S.; Zimmermann, N. Improving medicines access in Brazil through collaboration in the PPRI network. Rev. Bras. Farmácia Hosp. Serviços Saúde 2022, 13, 677. [Google Scholar] [CrossRef]
- Krüger, L.J.; Evers, S.M.A.A.; Hiligsmann, M.; Wild, C. Divergent evidence requirements for authorization and reimbursement of high-risk medical devices—The European situation. Health Policy Technol. 2014, 3, 253–263. [Google Scholar] [CrossRef]
- Sorenson, C.; Drummond, M.; Burns, L.R. Evolving Reimbursement And Pricing Policies For Devices In Europe And The United States Should Encourage Greater Value. Health Aff. 2013, 32, 788–796. [Google Scholar] [CrossRef] [Green Version]
- Sorenson, C.; Drummond, M.; Torbica, A.; Callea, G.; Mateus, C. The role of hospital payments in the adoption of new medical technologies: An international survey of current practice. Health Econ. Policy Law 2015, 10, 133–159. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.; Retèl, V.; Bhairosing, P.; Brekel, M.V.D.; van Harten, W. Barriers and facilitators of patient access to medical devices in Europe: A systematic literature review. Health Policy 2019, 123, 1185–1198. [Google Scholar] [CrossRef]
- Schreyögg, J.; Bäumler, M.; Busse, R. Balancing adoption and affordability of medical devices in Europe. Health Policy 2009, 92, 218–224. [Google Scholar] [CrossRef]
- HAS. Parcours du Dispositif Médical en France; Haute Autorité de Santé: Paris, France, 2021. [Google Scholar]
- Daubner-Bendes, R.; Kovács, S.; Niewada, M.; Huic, M.; Drummond, M.; Ciani, O.; Blankart, C.R.; Mandrik, O.; Torbica, A.; Yfantopoulos, J.; et al. Quo Vadis HTA for Medical Devices in Central and Eastern Europe? Recommendations to Address Methodological Challenges. Front. Public Health 2021, 8, 612410. [Google Scholar] [CrossRef]
- Blüher, M.; Saunders, S.J.; Mittard, V.; Torrejon Torres, R.; Davis, J.A.; Saunders, R. Critical Review of European Health-Economic Guidelines for the Health Technology Assessment of Medical Devices. Front. Med. 2019, 6, 278. [Google Scholar] [CrossRef]
- Ciani, O.; Wilcher, B.; Blankart, C.R.; Hatz, M.; Rupel, V.P.; Erker, R.S.; Varabyova, Y.; Taylor, R.S. Health Technology Assessment of Medical Devices: A survey of Non-European Union agencies. Int. J. Technol. Assess. Health Care 2015, 31, 154–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnell-Inderst, P.; Mayer, J.; Lauterberg, J.; Hunger, T.; Arvandi, M.; Conrads-Frank, A.; Nachtnebel, A.; Wild, C.; Siebert, U. Health technology assessment of medical devices: What is different? An overview of three European projects. Z. Evidenz Fortbild. Qual. Gesundh. 2015, 109, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Rintoul, A.; Colbert, A.; Garner, S.; Kotwani, A.; Vogler, S.; Bouvy, J.; Hill, A. Medicines with one seller and many buyers: Strategies to increase the power of the payer. BMJ 2020, 369, m1705. [Google Scholar] [CrossRef]
- Ferrario, A.; Arāja, D.; Bochenek, T.; Čatić, T.; Dankó, D.; Dimitrova, M.; Fürst, J.; Greičiūtė-Kuprijanov, I.; Hoxha, I.; Jakupi, A. The implementation of managed entry agreements in Central and Eastern Europe: Findings and implications. Pharmacoeconomics 2017, 35, 1271–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrario, A.; Kanavos, P. Dealing with uncertainty and high prices of new medicines: A comparative analysis of the use of managed entry agreements in Belgium, England, the Netherlands and Sweden. Soc. Sci. Med. 2015, 124, 39–47. [Google Scholar] [CrossRef]
- Pauwels, K.; Huys, I.; Vogler, S.; Casteels, M.; Simoens, S. Managed Entry Agreements for oncology drugs: Lessons from the European experience to inform the future. Front. Pharmacol. 2017, 8, 171. [Google Scholar] [CrossRef]
- Paris, V.; Belloni, A. Value in Pharmaceutical Pricing; OECD Health Working Papers, No. 63; OECD Publishing: Paris, France, 2013. [Google Scholar]
- Ferrario, A.; Dedet, G.; Humbert, T.; Vogler, S.; Suleman, F.; Pedersen, H.B. Strategies to achieve fairer prices for generic and biosimilar medicines. BMJ 2020, 368, l5444. [Google Scholar] [CrossRef] [Green Version]
- Henschke, C.; Sundmacher, L.; Busse, R. Structural changes in the German pharmaceutical market: Price setting mechanisms based on the early benefit evaluation. Health Policy 2013, 109, 263–269. [Google Scholar] [CrossRef]
- Papastergiou, J.; Trieu, C.R.; Saltmarche, D.; Diamantouros, A. Community pharmacist–directed point-of-care group A Streptococcus testing: Evaluation of a Canadian program. J. Am. Pharm. Assoc. 2018, 58, 450–456. [Google Scholar] [CrossRef]
- Borek, A.J.; on behalf of the STEP-UP study team; Campbell, A.; Dent, E.; Butler, C.C.; Holmes, A.; Moore, M.; Walker, A.S.; McLeod, M.; Tonkin-Crine, S. Implementing interventions to reduce antibiotic use: A qualitative study in high-prescribing practices. BMC Fam. Pract. 2021, 22, 25. [Google Scholar] [CrossRef]
- Shephard, A.; Smith, G.; Aspley, S.; Schachtel, B.P. Randomised, double-blind, placebo-controlled studies on flurbiprofen 8.75 mg lozenges in patients with/without group A or C streptococcal throat infection, with an assessment of clinicians’ prediction of ‘strep throat’. Int. J. Clin. Pract. 2015, 69, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Lean, W.L.; Arnup, S.; Danchin, M.; Steer, A.C. Rapid Diagnostic Tests for Group A Streptococcal Pharyngitis: A Meta-analysis. Pediatrics 2014, 134, 771–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hays, J.P.; Mitsakakis, K.; Luz, S.; van Belkum, A.; Becker, K.; van den Bruel, A.; Harbarth, S.; Rex, J.H.; Simonsen, G.S.; Werner, G.; et al. The successful uptake and sustainability of rapid infectious disease and antimicrobial resistance point-of-care testing requires a complex ‘mix-and-match’ implementation package. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1015–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suleman, F.; Low, M.; Moon, S.; Morgan, S.G. New business models for research and development with affordability requirements are needed to achieve fair pricing of medicines. BMJ 2020, 368, l4408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtemanche, G.; Wadanamby, R.; Kiran, A.; Toro-Alzate, L.F.; Diggle, M.; Chakraborty, D.; Blocker, A.; van Dongen, M. Looking for Solutions to the Pitfalls of Developing Novel Antibacterials in an Economically Challenging System. Microbiol. Res. 2021, 12, 173–185. [Google Scholar] [CrossRef]
- Dutescu, I.A.; Hillier, S.A. Encouraging the Development of New Antibiotics: Are Financial Incentives the Right Way Forward? A Systematic Review and Case Study. Infect Drug Resist 2021, 14, 415–434. [Google Scholar] [CrossRef]
- Gotham, D.; Moja, L.; van der Heijden, M.; Paulin, S.; Smith, I.; Beyer, P. Reimbursement models to tackle market failures for antimicrobials: Approaches taken in France, Germany, Sweden, the United Kingdom, and the United States. Health Policy 2021, 125, 296–306. [Google Scholar] [CrossRef]
- Vogler, S.; Habimana, K.; Fischer, S.; Haasis, M.A. Novel Policy Options for Reimbursement, Pricing and Procurement of AMR Health Technologies; Gesundheit Österreich (GÖG/Austrian National Public Health Institute): Vienna, Austria, 2021. [Google Scholar]
- Rothery, C.; Woods, B.; Schmitt, L.; Claxton, K.; Palmer, S.; Sculpher, M. Framework for Value Assessment of New Antimicrobials: Implications of Alternative Funding Arrangements for NICE Appraisal Policy; Research Unit in Economic Evaluation of Health and Care Interventions (EEPRU): York and Sheffield, UK, 2018. [Google Scholar]
- Global AMR R&D Hub. Incentivizing Antibiotic Access and Innovation; Global AMR R&D Hub: Berlin, Germany, 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Country | Price Regulation for | |
|---|---|---|
| CA-ARTI Diagnostics | Further Medical Devices | |
| Austria | No | No |
| Belgium | No | Only for hearing aids |
| Croatia | No | No |
| Cyprus | No | No |
| Estonia | No | No |
| Finland | No answer available | No answer available |
| France | No | For MD included in the reimbursement list |
| Germany | No | No |
| Greece | No | For MD included in the reimbursement list |
| Hungary | No | For MD included in the reimbursement list |
| Italy | No | No |
| Malta | No | No |
| Romania | No | No |
| Slovakia | No | For MD included in the reimbursement list |
| Spain | No | For MD included in the reimbursement list |
| Sweden | No | For MD included in the reimbursement list |
| United Kingdom | No | No |
| Reimbursement Status of POC Diagnostic Tests for CA-ARTI | Country |
|---|---|
| Public payer pays, full coverage of CA-ARTI Dx classified as reimbursable | Cyprus, Estonia, Finland, Romania, Slovakia |
| Public payer pays for CA-ARTI Dx classified as reimbursable, supplemented by patient co-payments | Austria 1, France 2 |
| Patients pay out-of-pocket for CA-ARTI Dx | Belgium, Croatia, Germany 3, Greece, Hungary, Italy 4, Malta 4, Spain 4, Sweden 5, United Kingdom |
| Country | Reimbursement for the Device | Remuneration for the Service | ||
|---|---|---|---|---|
| POC CA-ARTI Dx | Further MD | POC CA-ARTI Dx | Further MD | |
| Austria | Yes | Yes | Yes | Yes |
| Belgium | No | Yes | No | Yes |
| Croatia | No | Yes | No information | No information |
| Cyprus | Yes | Yes | Yes | Yes |
| Estonia | Yes | Yes | Yes | Yes |
| Finland | Yes | Yes | No information | No information |
| France | No | Yes | Yes | Yes |
| Germany | No | Yes | No | Yes |
| Greece | No | Yes | No | Yes |
| Hungary | No | Yes | No | Yes |
| Italy | No | No | No | No |
| Malta | No | No | No | No |
| Romania | Yes | Yes | No | Yes |
| Slovakia | Yes | Yes | No | Yes |
| Spain | Yes, partly | Yes | No | No |
| Sweden | No | No | No | Yes |
| United Kingdom | No | Yes | No | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vogler, S.; Windisch, F. Assessing, Pricing and Funding Point-of-Care Diagnostic Tests for Community-Acquired Acute Respiratory Tract Infections–Overview of Policies Applied in 17 European Countries. Antibiotics 2022, 11, 987. https://doi.org/10.3390/antibiotics11080987
Vogler S, Windisch F. Assessing, Pricing and Funding Point-of-Care Diagnostic Tests for Community-Acquired Acute Respiratory Tract Infections–Overview of Policies Applied in 17 European Countries. Antibiotics. 2022; 11(8):987. https://doi.org/10.3390/antibiotics11080987
Chicago/Turabian StyleVogler, Sabine, and Friederike Windisch. 2022. "Assessing, Pricing and Funding Point-of-Care Diagnostic Tests for Community-Acquired Acute Respiratory Tract Infections–Overview of Policies Applied in 17 European Countries" Antibiotics 11, no. 8: 987. https://doi.org/10.3390/antibiotics11080987
APA StyleVogler, S., & Windisch, F. (2022). Assessing, Pricing and Funding Point-of-Care Diagnostic Tests for Community-Acquired Acute Respiratory Tract Infections–Overview of Policies Applied in 17 European Countries. Antibiotics, 11(8), 987. https://doi.org/10.3390/antibiotics11080987