
Clinical Characteristics and Outcomes of Persistent Staphylococcal Bacteremia in a Tertiary Care Hospital


Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics of Persistent S. aureus and CoNS Bacteremia
2.2. Clinical Characteristics of Persistent S. aureus and CoNS Bacteremia in Terms of Methicillin Resistance
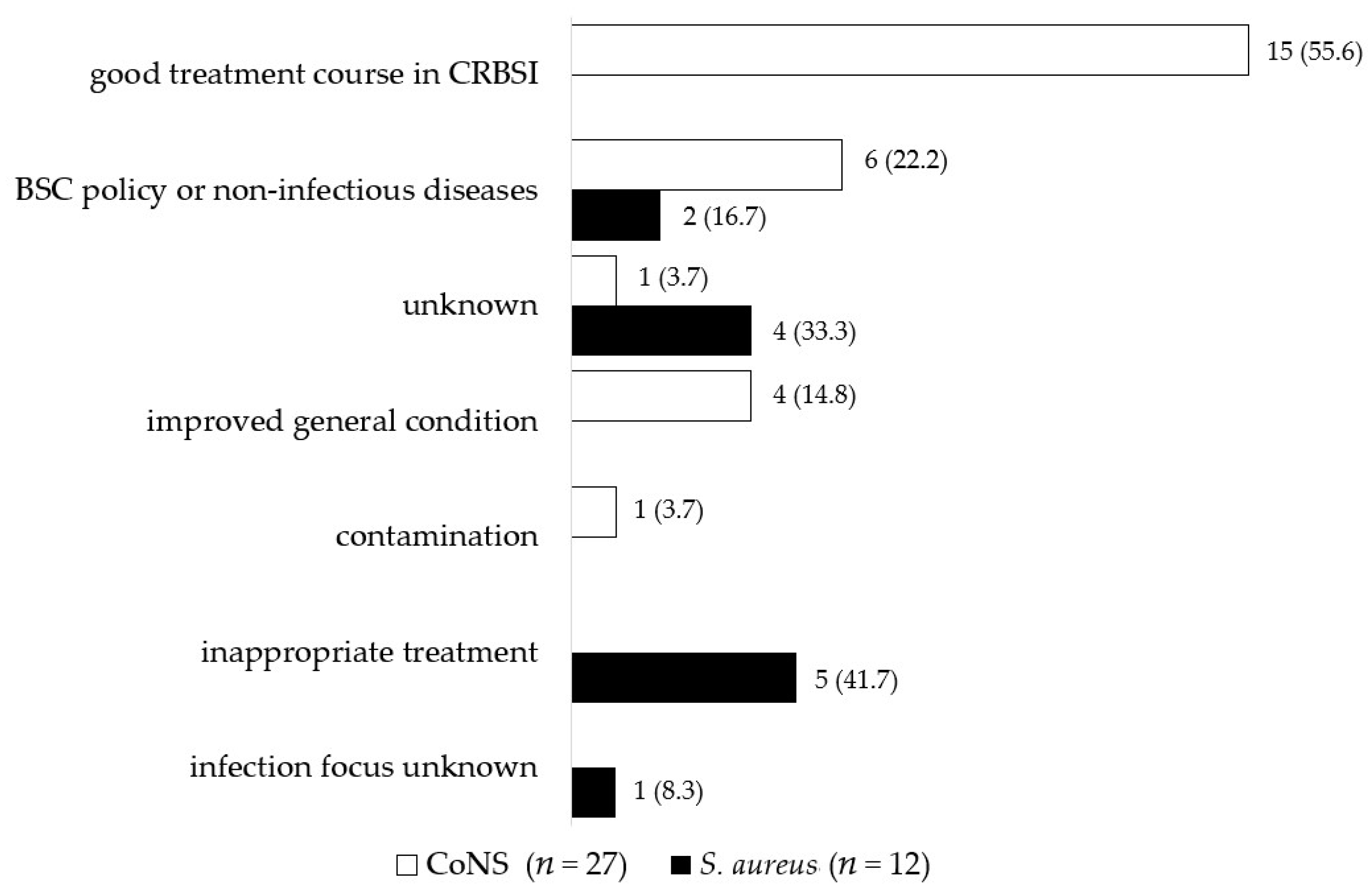
2.3. Reasons for Non-Clearance of Persistent Staphylococcal Bacteremia
3. Discussion
3.1. Differences in Clinical Characteristics between Persistent S. aureus and CoNS Bacteremia
3.2. Differences in Clinical Characteristics between Persistent S. aureus and CoNS Bacteremia in Terms of Methicillin Resistance
3.3. Causes of Non-Clearance of Persistent Staphylococcal Bacteremia
4. Materials and Methods
4.1. Study Design and Setting
4.2. Definitions and Outcomes
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guimaraes, A.O.; Cao, Y.; Hong, K.; Mayba, O.; Peck, M.C.; Gutierrez, J.; Ruffin, F.; Carrasco-Triguero, M.; Dinoso, J.B.; Clemenzi-Allen, A.; et al. A Prognostic Model of Persistent Bacteremia and Mortality in Complicated Staphylococcus aureus Bloodstream Infection. Clin. Infect. Dis. 2019, 68, 1502–1511. [Google Scholar] [CrossRef]
- Lewis, P.O.; Heil, E.L.; Covert, K.L.; Cluck, D.B. Treatment strategies for persistent methicillin-resistant Staphylococcus aureus bacteraemia. J. Clin. Pharm. Ther. 2018, 43, 614–625. [Google Scholar] [CrossRef] [Green Version]
- Khashu, M.; Osiovich, H.; Henry, D.; Al Khotani, A.; Solimano, A.; Speert, D.P. Persistent bacteremia and severe thrombocytopenia caused by coagulase-negative Staphylococcus in a neonatal intensive care unit. Pediatrics 2006, 117, 340–348. [Google Scholar] [CrossRef]
- Kitaya, S.; Kanamori, H.; Baba, H.; Oshima, K.; Takei, K.; Katsumi, M.; Katori, Y.; Tokuda, K. Clinical and Epidemiological Characteristics of Persistent Bacteremia: A Decadal Observational Study. Pathogens 2023, 12, 212. [Google Scholar] [CrossRef]
- Wiggers, J.B.; Xiong, W.; Daneman, N. Sending repeat cultures: Is there a role in the management of bacteremic episodes? (SCRIBE study). BMC Infect. Dis. 2016, 16, 286. [Google Scholar] [CrossRef] [Green Version]
- Kuehl, R.; Morata, L.; Boeing, C.; Subirana, I.; Seifert, H.; Rieg, S.; Kern, W.V.; Kim, H.B.; Kim, E.S.; Liao, C.H.; et al. Defining persistent Staphylococcus aureus bacteraemia: Secondary analysis of a prospective cohort study. Lancet Infect. Dis. 2020, 20, 1409–1417. [Google Scholar] [CrossRef]
- Chong, Y.P.; Park, S.J.; Kim, H.S.; Kim, E.S.; Kim, M.N.; Park, K.H.; Kim, S.H.; Lee, S.O.; Choi, S.H.; Jeong, J.Y.; et al. Persistent Staphylococcus aureus bacteremia: A prospective analysis of risk factors, outcomes, and microbiologic and genotypic characteristics of isolates. Medicine 2013, 92, 98–108. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, C.; Huang, J.; Jin, N.; Noskin, G.A.; Zembower, T.R.; Bolon, M. Persistent Staphylococcus aureus bacteremia: An analysis of risk factors and outcomes. Arch. Intern. Med. 2007, 167, 1861–1867. [Google Scholar] [CrossRef] [Green Version]
- Bellou, V.; Gkentzi, D.; Giormezis, N.; Vervenioti, A.; Spiliopoulou, I.; Dimitriou, G. Persistent Coagulase-Negative Staphylococcal Bacteremia in Neonates: Clinical, Microbiological Characteristics and Changes within a Decade. Antibiotics 2022, 11, 765. [Google Scholar] [CrossRef]
- Gkentzi, D.; Kolyva, S.; Spiliopoulou, I.; Marangos, M.; Dimitriou, G. Treatment Options for Persistent Coagulase Negative Staphylococcal Bacteremia in Neonates. Curr. Pediatr. Rev. 2016, 12, 199–208. [Google Scholar] [CrossRef]
- Dimitriou, G.; Fouzas, S.; Giormezis, N.; Giannakopoulos, I.; Tzifas, S.; Foka, A.; Anastassiou, D.E.; Spiliopoulou, I.; Mantagos, S. Clinical and microbiological profile of persistent coagulase-negative staphylococcal bacteraemia in neonates. Clin. Microbiol. Infect. 2011, 17, 1684–1690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linder, N.; Hernandez, A.; Amit, L.; Klinger, G.; Ashkenazi, S.; Levy, I. Persistent coagulase-negative Staphylococci bacteremia in very-low-birth-weight infants. Eur. J. Pediatr. 2011, 170, 989–995. [Google Scholar] [CrossRef]
- Furuichi, M.; Miyairi, I. Risk factors for persistent bacteremia in infants with catheter-related bloodstream infection due to coagulase-negative Staphylococcus in the neonatal intensive care unit. J. Infect. Chemother. 2016, 22, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Neuner, E.A.; Casabar, E.; Reichley, R.; McKinnon, P.S. Clinical, microbiologic, and genetic determinants of persistent methicillin-resistant Staphylococcus aureus bacteremia. Diagn. Microbiol. Infect. Dis. 2010, 67, 228–233. [Google Scholar] [CrossRef]
- Chung, H.; Kim, E.; Yang, E.; Lee, Y.W.; Park, J.H.; Bae, S.; Jung, J.; Kim, M.J.; Chong, Y.P.; Kim, S.H.; et al. C-reactive protein predicts persistent bacteremia caused by community-acquired methicillin-resistant Staphylococcus aureus strain. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2497–2504. [Google Scholar] [CrossRef] [PubMed]
- Moise, P.A.; Sakoulas, G.; Forrest, A.; Schentag, J.J. Vancomycin in vitro bactericidal activity and its relationship to efficacy in clearance of methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob. Agents Chemother. 2007, 51, 2582–2586. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.H.; Liao, W.H.; Lai, C.C.; Liao, C.H.; Tan, C.K.; Wang, C.Y.; Huang, Y.T.; Hsueh, P.R. Risk factors for mortality in patients with persistent methicillin-resistant Staphylococcus aureus bacteraemia in a tertiary care hospital in Taiwan. J. Antimicrob. Chemother. 2010, 65, 1792–1798. [Google Scholar] [CrossRef]
- Karlowicz, M.G.; Furigay, P.J.; Croitoru, D.P.; Buescher, E.S. Central venous catheter removal versus in situ treatment in neonates with coagulase-negative staphylococcal bacteremia. Pediatr. Infect. Dis. J. 2002, 21, 22–27. [Google Scholar] [CrossRef]
- Heybati, K.; Seeger, R.; Thyagu, S.; Piticaru, J.; Ahluwalia, N.; Munshi, L. Catheter management across patients with hematologic malignancies and catheter-related blood stream infections: A systematic review. Ann. Hematol. 2022, 101, 2515–2524. [Google Scholar] [CrossRef]
- Otto, M. Virulence factors of the coagulase-negative staphylococci. Front. Biosci. 2004, 9, 841–863. [Google Scholar] [CrossRef]
- Otto, M. Staphylococcus epidermidis—The ‘accidental’ pathogen. Nat. Rev. Microbiol. 2009, 7, 555–567. [Google Scholar] [CrossRef] [Green Version]
- Wertheim, H.F.; Melles, D.C.; Vos, M.C.; van Leeuwen, W.; van Belkum, A.; Verbrugh, H.A.; Nouwen, J.L. The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect. Dis. 2005, 5, 751–762. [Google Scholar] [CrossRef]
- Medis, S.; Dissanayake, T.; Kottahachchi, J.; Namali, D.; Gunasekara, S.; Wijesinghe, G.; Dilrukshi, N.; Weerasekera, M. Biofilm formation and antibiotic resistance among Coagulase Negative Staphylococcus species isolated from central venous catheters of intensive care unit patients. Indian J. Med. Microbiol. 2022, in press. [Google Scholar] [CrossRef]
- Ocal, D.; Tekeli, A.; Dolapci, I. Investigation of Biofilm Formation Properties of Coagulase Negative Staphylococci Isolated from Catheter-Related Bloodstream Infections. Mikrobiyol. Bul. 2022, 56, 506–524. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Heilmann, C.; Peters, G. Coagulase-negative staphylococci. Clin. Microbiol. Rev. 2014, 27, 870–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebeaux, D.; Fernandez-Hidalgo, N.; Chauhan, A.; Lee, S.; Ghigo, J.M.; Almirante, B.; Beloin, C. Management of infections related to totally implantable venous-access ports: Challenges and perspectives. Lancet Infect. Dis. 2014, 14, 146–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagao, M.; Iinuma, Y.; Saito, T.; Matsumura, Y.; Shirano, M.; Matsushima, A.; Takakura, S.; Ito, Y.; Ichiyama, S. Close cooperation between infectious disease physicians and attending physicians can result in better management and outcome for patients with Staphylococcus aureus bacteraemia. Clin. Microbiol. Infect. 2010, 16, 1783–1788. [Google Scholar] [CrossRef]
- Jenkins, T.C.; Price, C.S.; Sabel, A.L.; Mehler, P.S.; Burman, W.J. Impact of routine infectious diseases service consultation on the evaluation, management, and outcomes of Staphylococcus aureus bacteremia. Clin. Infect. Dis. 2008, 46, 1000–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horino, T.; Hori, S. Metastatic infection during Staphylococcus aureus bacteremia. J. Infect. Chemother. 2020, 26, 162–169. [Google Scholar] [CrossRef]
- Azih, A.; Enabulele, I. Species distribution and virulence factors of coagulase negative staphylococci isolated from clinical samples from the University of Benin Teaching Hospital, Edo State, Nigeria. J. Nat. Sci. Res. 2013, 3, 38–44. [Google Scholar]
- Cantey, J.B.; Anderson, K.R.; Kalagiri, R.R.; Mallett, L.H. Morbidity and mortality of coagulase-negative staphylococcal sepsis in very-low-birth-weight infants. World J. Pediatr. 2018, 14, 269–273. [Google Scholar] [CrossRef]
- Molina, J.; Penuela, I.; Lepe, J.A.; Gutierrez-Pizarraya, A.; Gomez, M.J.; Garcia-Cabrera, E.; Cordero, E.; Aznar, J.; Pachon, J. Mortality and hospital stay related to coagulase-negative Staphylococci bacteremia in non-critical patients. J. Infect. 2013, 66, 155–162. [Google Scholar] [CrossRef]
- Chen, C.P.; Liu, M.F.; Lin, C.F.; Lin, S.P.; Shi, Z.Y. The association of molecular typing, vancomycin MIC, and clinical outcome for patients with methicillin-resistant Staphylococcus aureus infections. J. Microbiol. Immunol. Infect. 2017, 50, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Fowler, V.G., Jr.; Boucher, H.W.; Corey, G.R.; Abrutyn, E.; Karchmer, A.W.; Rupp, M.E.; Levine, D.P.; Chambers, H.F.; Tally, F.P.; Vigliani, G.A.; et al. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. N. Engl. J. Med. 2006, 355, 653–665. [Google Scholar] [CrossRef] [Green Version]
- Cosgrove, S.E.; Sakoulas, G.; Perencevich, E.N.; Schwaber, M.J.; Karchmer, A.W.; Carmeli, Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: A meta-analysis. Clin. Infect. Dis. 2003, 36, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Chaves, F.; Garnacho-Montero, J.; Del Pozo, J.L.; Bouza, E.; Capdevila, J.A.; de Cueto, M.; Domínguez, M.; Esteban, J.; Fernández-Hidalgo, N.; Fernández Sampedro, M.; et al. Diagnosis and treatment of catheter-related bloodstream infection: Clinical guidelines of the Spanish Society of Infectious Diseases and Clinical Microbiology and (SEIMC) and the Spanish Society of Spanish Society of Intensive and Critical Care Medicine and Coronary Units (SEMICYUC). Med. Intensiv. 2018, 42, 5–36. [Google Scholar] [CrossRef]
- Mermel, L.A.; Allon, M.; Bouza, E.; Craven, D.E.; Flynn, P.; O’Grady, N.P.; Raad, I.I.; Rijnders, B.J.; Sherertz, R.J.; Warren, D.K. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 49, 1–45. [Google Scholar] [CrossRef]
- Sohail, M.R.; Palraj, B.R.; Khalid, S.; Uslan, D.Z.; Al-Saffar, F.; Friedman, P.A.; Hayes, D.L.; Lohse, C.M.; Wilson, W.R.; Steckelberg, J.M.; et al. Predicting risk of endovascular device infection in patients with Staphylococcus aureus bacteremia (PREDICT-SAB). Circ. Arrhythm. Electrophysiol. 2015, 8, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Uslan, D.Z.; Dowsley, T.F.; Sohail, M.R.; Hayes, D.L.; Friedman, P.A.; Wilson, W.R.; Steckelberg, J.M.; Baddour, L.M. Cardiovascular implantable electronic device infection in patients with Staphylococcus aureus bacteremia. Pacing Clin. Electrophysiol. 2010, 33, 407–413. [Google Scholar] [CrossRef]
- Chesdachai, S.; Baddour, L.M.; Sohail, M.R.; Palraj, B.R.; Madhavan, M.; Tabaja, H.; Fida, M.; Lahr, B.D.; DeSimone, D.C. Evaluation of European Heart Rhythm Association consensus in patients with cardiovascular implantable electronic devices and Staphylococcus aureus bacteremia. Heart Rhythm 2022, 19, 570–577. [Google Scholar] [CrossRef]
- Koval, C.E.; Rakita, R.; AST Infectious Diseases Community of Practice. Ventricular assist device related infections and solid organ transplantation. Am. J. Transplant. 2013, 13, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.T.; Guo, Y.; Simkins, J.; Puius, Y.A.; Muggia, V.A.; Goldstein, D.J.; D’Alessandro, D.A.; Minamoto, G.Y. Left ventricular assist device exchange for persistent infection: A case series and review of the literature. Transpl. Infect. Dis. 2014, 16, 453–460. [Google Scholar] [CrossRef]
- O’Horo, J.C.; Abu Saleh, O.M.; Stulak, J.M.; Wilhelm, M.P.; Baddour, L.M.; Rizwan Sohail, M. Left Ventricular Assist Device Infections: A Systematic Review. ASAIO J. 2018, 64, 287–294. [Google Scholar] [CrossRef] [PubMed]
- M7-A8; Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically Eighth Edition: Approved Standard. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2009.


{kind=link}
| Persistent S. aureus Bacteremia (n = 92) | Persistent CoNS Bacteremia (n = 88) | Odds Ratio [95% CI] | p-Value | |
|---|---|---|---|---|
| Demography | ||||
| Sex (male, %) | 65 (70.7) | 48 (54.5) | 2 [1.1, 3.7] | 0.031 |
| Age, years, median (IQR) | 63.5 (56.5–69.3) | 55.5 (40.3–58.8) | 0.003 | |
| Comorbidities | ||||
| Diabetes mellitus | 25 (27.2) | 9 (10.2) | 3.3 [1.4, 7.5] | 0.004 |
| ESDR on hemodialysis | 11 (12.0) | 6 (6.8) | 1.9 [0.7, 5.3] | |
| Liver cirrhosis | 13 (14.1) | 7 (8.0) | 1.9 [0.7, 5] | |
| Solid malignancy | 28 (30.4) | 24 (27.3) | 1.2 [0.6, 2.3] | |
| Hematologic malignancy | 2 (2.2) | 15 (17.0) | 0.1 [0, 0.5] | 0.001 |
| Neutropenia | 1 (1.1) | 7 (8.0) | 0.1 [0, 1.1] | 0.032 |
| Immunosuppression | 12 (13.0) | 24 (27.3) | 0.4 [0.2, 0.9] | 0.025 |
| Vital signs | ||||
| BMI, kg/m2, median (IQR) | 21.1 (18.4–23.8) | 22.2 (18.6–24.1) | ||
| Body temperature, °C, median (IQR) | 38.7 (38.0–39.1) (n = 82) | 38.0 (37.5–38.9) (n = 84) | 0.009 | |
| Laboratory markers | ||||
| White blood cell count, 109/L, median (IQR) | 9550.0 (7375.0–12,200.0) | 8000.0 (4100.0–12,725.0) | 0.022 | |
| Neutrophil count, 109/L, median (IQR) | 8160.0 (6210.0–10,950.0) (n = 89) | 5940.0 (3190.0–10,697.5) (n = 81) | 0.006 | |
| C-reactive protein, mg/dL, median (IQR) | 10.0 (4.6–16.9) | 4.2 (1.7–7.6) | <0.001 | |
| Devices | ||||
| Intravascular device | 53 (57.6) | 76 (86.4) | 0.2 [0.1, 0.4] | <0.001 |
| Intravascular device removal | 46 (86.8) | 58 (76.3) | 2 [0.8, 5.3] | |
| Cardiovascular surgery | 28 (30.4) | 14 (15.9) | 2.5 [1.2, 5.3] | 0.013 |
| ECMO | 0 (0) | 2 (2.3) | 0 | |
| Continuous hemodiafiltration | 0 (0) | 19 (21.6) | 0 | |
| Mechanical ventilation | 24 (26.1) | 20 (22.7) | 1.2 [0.6, 2.4] | |
| Status of persistent bacteremia | ||||
| Period until FUBC is carried out, median (IQR) | 3.0 (2.0–4.0) | 3.0 (1.0–5.0) | ||
| Duration of bacteremia, median (IQR) | 3.5 (2.0–6.3) | 3.0 (1.0–7.0) | ||
| Site of infection | ||||
| CRBSI | 40 (29.2) | 73 (77.7) | 0.1 [0.1, 0.2] | <0.001 |
| Abscess | 15 (10.9) | 1 (1.1) | 11.4 [1.5, 88.1] | 0.003 |
| Infectious endocarditis | 14 (10.2) | 2 (2.1) | 5.2 [1.2, 23.6] | 0.018 |
| Endovascular devices infections | 12 (8.8) | 1 (1.1) | 8.9 [1.1, 69.9] | 0.017 |
| Septic embolism | 10 (7.3) | 1 (1.1) | 7.3 [0.9, 58.2] | 0.030 |
| Pyogenic spondylitis | 10 (7.3) | 1 (1.1) | 7.3 [0.9, 58.2] | 0.030 |
| Thrombophlebitis | 9 (6.6) | 4 (4.3) | 1.6 [0.5, 5.3] | |
| Surgical site infection | 5 (3.6) | 0 (0) | – | |
| Suppurative arthritis | 4 (2.9) | 0 (0) | – | |
| Skin and soft tissue infections | 3 (2.2) | 1 (1.1) | 2.1 [0.2, 20.3] | |
| Osteomyelitis | 2 (1.5) | 1 (1.1) | 1.4 [0.1, 15.4] | |
| Others | 4 (2.9) | 0 (0) | – | |
| Unknown | 9 (6.6) | 9 (9.6) | 0.7 [0.3, 1.7] | |
| Hospital stays | ||||
| Duration of hospitalization, days, median (IQR) | 59.5 (36.8–104.3) | 78.0 (39.5–127.0) | ||
| Presence of ICU | 28 (30.4) | 40 (45.5) | 0.5 [0.3, 1] | 0.046 |
| Duration of ICU stay, days, median (IQR) | 0 (0–8) | 0 (0–18.3) | 0.034 | |
| Intervention | ||||
| The use of antibiotics (Appropriate) | 76 (82.6) | 81 (92.0) | 0.4 [0.2, 1.1] | |
| Source control | 61 (66.3) | 66 (75.0) | 0.7 [0.3, 1.3] | |
| Mortality | ||||
| Early (30-day) mortality | 5 (5.4) | 2 (3.2) | 2.5 [0.5, 13.1] | |
| Late (30–90 days) mortality | 2 (2.2) | 4 (6.5) | 0.5 [0.1, 2.6] | |
| 90-day mortality | 7 (7.6) | 6 (9.7) | 0.9 [0.3, 2.8] |
| Persistent MRSA Bacteremia (n = 43) | Persistent MSSA Bacteremia (n = 49) | Odds Ratio [95% CI] | p-Value | Persistent MRCoNS Bacteremia (n = 70) | Persistent MSCoNS Bacteremia (n = 18) | Odds Ratio [95% CI] | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Demography | ||||||||
| Sex (male, %) | 31 (72.1) | 34 (69.4) | 1.1 [0.5, 2.8] | 37 (52.9) | 11 (61.1) | 0.7 [0.2, 2.1] | ||
| Age, years, median (IQR) | 66.0 (64.3–67.8) | 57.0 (51.5–69.3) | 58.0 (53.0–59.0) | 43.5 (33.3–63.3) | ||||
| Comorbidities | ||||||||
| Diabetes mellitus | 11 (25.6) | 14 (28.6) | 0.9 [0.3, 2.2] | 8 (11.4) | 1 (5.6) | 2.2 [0.3, 18.8] | ||
| ESDR on hemodialysis | 4 (9.3) | 7 (14.3) | 0.6 [0.2, 2.3] | 4 (5.7) | 2 (11.1) | 0.5 [0.1, 2.9] | ||
| Liver cirrhosis | 6 (14.0) | 7 (14.3) | 1 [0.3, 3.2] | 6 (8.6) | 1 (5.6) | 1.6 [0.2, 14.1] | ||
| Solid malignancy | 16 (37.2) | 12 (24.5) | 1.8 [0.7, 4.5] | 19 (27.1) | 5 (27.8) | 1 [0.3, 3.1] | ||
| Hematologic malignancy | 2 (4.7) | 0 (0) | – | 15 (21.4) | 0 (0) | – | 0.034 | |
| Neutropenia | 1 (2.3) | 0 (0) | – | 7 (10.0) | 0 (0) | – | ||
| Immunosuppression | 8 (18.6) | 4 (8.2) | 2.6 [0.7, 9.2] | 21 (30.0) | 2 (11.1) | 3.7 [0.8, 17.3] | ||
| Devices | ||||||||
| Intravascular device | 25 (58.1) | 28 (57.1) | 1 [0.5, 2.4] | 66 (94.3) | 13 (72.2) | 3.5 [0.9, 12.6] | ||
| Intravascular device removal | 21 (84.0) | 25 (89.3) | 0.6 [0.1, 3.1] | 55 (83.3) | 7 (53.8) | 4.3 [1.2, 15.2] | 0.028 | |
| Cardiovascular surgery | 16 (37.2) | 12 (24.5) | 1.8 [0.7, 4.5] | 12 (17.1) | 3 (16.7) | 1.1 [0.3, 4.3] | ||
| ECMO | 0 (0) | 0 (0) | – | 0 (0) | 2 (11.1) | 0 | 0.040 | |
| Continuous hemodiafiltration | 8 (18.6) | 7 (14.3) | 1.4 [0.5, 4.2] | 18 (25.7) | 1 (5.6) | 5.9 [0.7, 47.4] | ||
| Mechanical ventilation | 15 (34.9) | 9 (18.4) | 2.4 [0.9, 6.2] | 17 (24.3) | 3 (16.7) | 1.6 [0.4, 6.2] | ||
| Status of persistent bacteremia | ||||||||
| The period until FUBC is carried out, median (IQR) | 3.0 (2.0–4.0) | 2.0 (2.0–4.0) | 3.0 (1.0–5.0) | 3.0 (1.0–4.0) | ||||
| Duration of bacteremia, median (IQR) | 6.0 (3.0–9.0) | 3.0 (2.0–4.0) | <0.001 | 3.0 (1.3–7.0) | 3.5 (1.3–7.0) | |||
| Hospital stays | ||||||||
| Duration of hospitalization, days, median (IQR) | 63.0 (42.5–99.0) | 56.0 (36.0–108.0) | 93.0 (43.0–138.5) | 53.0 (31.0–82.0) | 0.029 | |||
| Intervention | ||||||||
| Use of antibiotics (Appropriate) | 36 (83.7) | 40 (81.6) | 1.2 [0.4, 3.4] | 65 (92.9) | 16 (88.9) | 1.6 [0.3, 9.2] | ||
| Source control | 29 (67.4) | 32 (65.3) | 1.1 [0.5, 2.6] | 53 (75.7) | 13 (72.2) | 1.2 [0.4, 3.9] | ||
| Mortality | ||||||||
| Early (30-day) mortality | 4 (9.3) | 1 (2.0) | 4.9 [0.5, 45.9] | 2 (2.9) | 0 (0) | – | ||
| Late (30–90 days) mortality | 1 (2.3) | 1 (2.0) | 1.1 [0.1, 18.8] | 3 (4.3) | 1 (5.6) | 0.8 [0.1, 7.8] | ||
| 90-day mortality | 5 (11.6) | 2 (4.1) | 3.1 [0.6, 16.8] | 5 (21.4) | 1 (5.6) | 1.3 [0.1, 11.9] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitaya, S.; Kanamori, H.; Katori, Y.; Tokuda, K. Clinical Characteristics and Outcomes of Persistent Staphylococcal Bacteremia in a Tertiary Care Hospital. Antibiotics 2023, 12, 454. https://doi.org/10.3390/antibiotics12030454
Kitaya S, Kanamori H, Katori Y, Tokuda K. Clinical Characteristics and Outcomes of Persistent Staphylococcal Bacteremia in a Tertiary Care Hospital. Antibiotics. 2023; 12(3):454. https://doi.org/10.3390/antibiotics12030454
Chicago/Turabian StyleKitaya, Shiori, Hajime Kanamori, Yukio Katori, and Koichi Tokuda. 2023. "Clinical Characteristics and Outcomes of Persistent Staphylococcal Bacteremia in a Tertiary Care Hospital" Antibiotics 12, no. 3: 454. https://doi.org/10.3390/antibiotics12030454
APA StyleKitaya, S., Kanamori, H., Katori, Y., & Tokuda, K. (2023). Clinical Characteristics and Outcomes of Persistent Staphylococcal Bacteremia in a Tertiary Care Hospital. Antibiotics, 12(3), 454. https://doi.org/10.3390/antibiotics12030454