
The Antibacterial and Antifungal Capacity of Eight Commercially Available Types of Mouthwash against Oral Microorganisms: An In Vitro Study

 , , ,
, , , 
 and
and 
Abstract
:1. Introduction
2. Results
2.1. Mouthwashes Evaluated
2.2. Antibacterial/Antifungal Activity
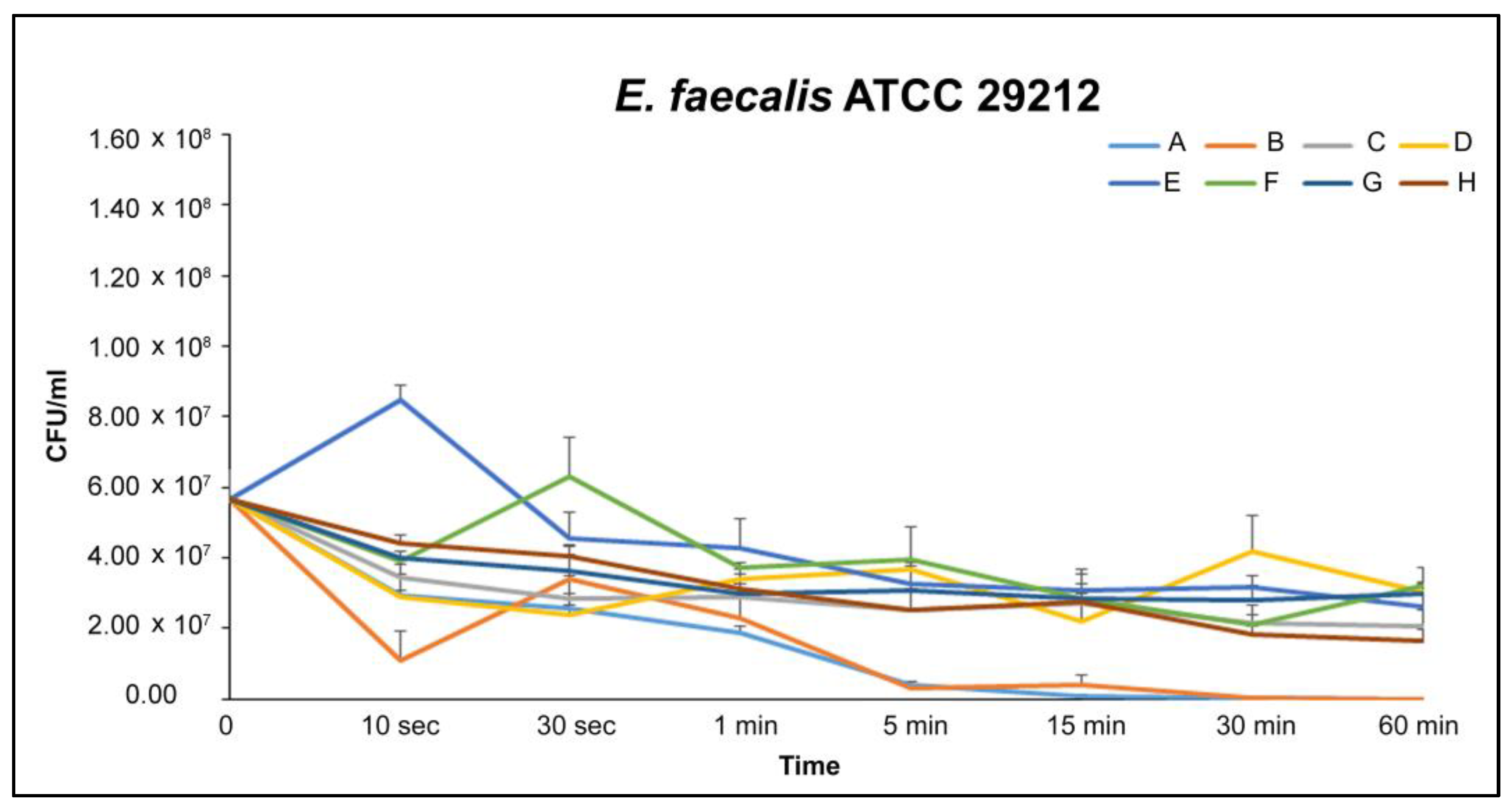
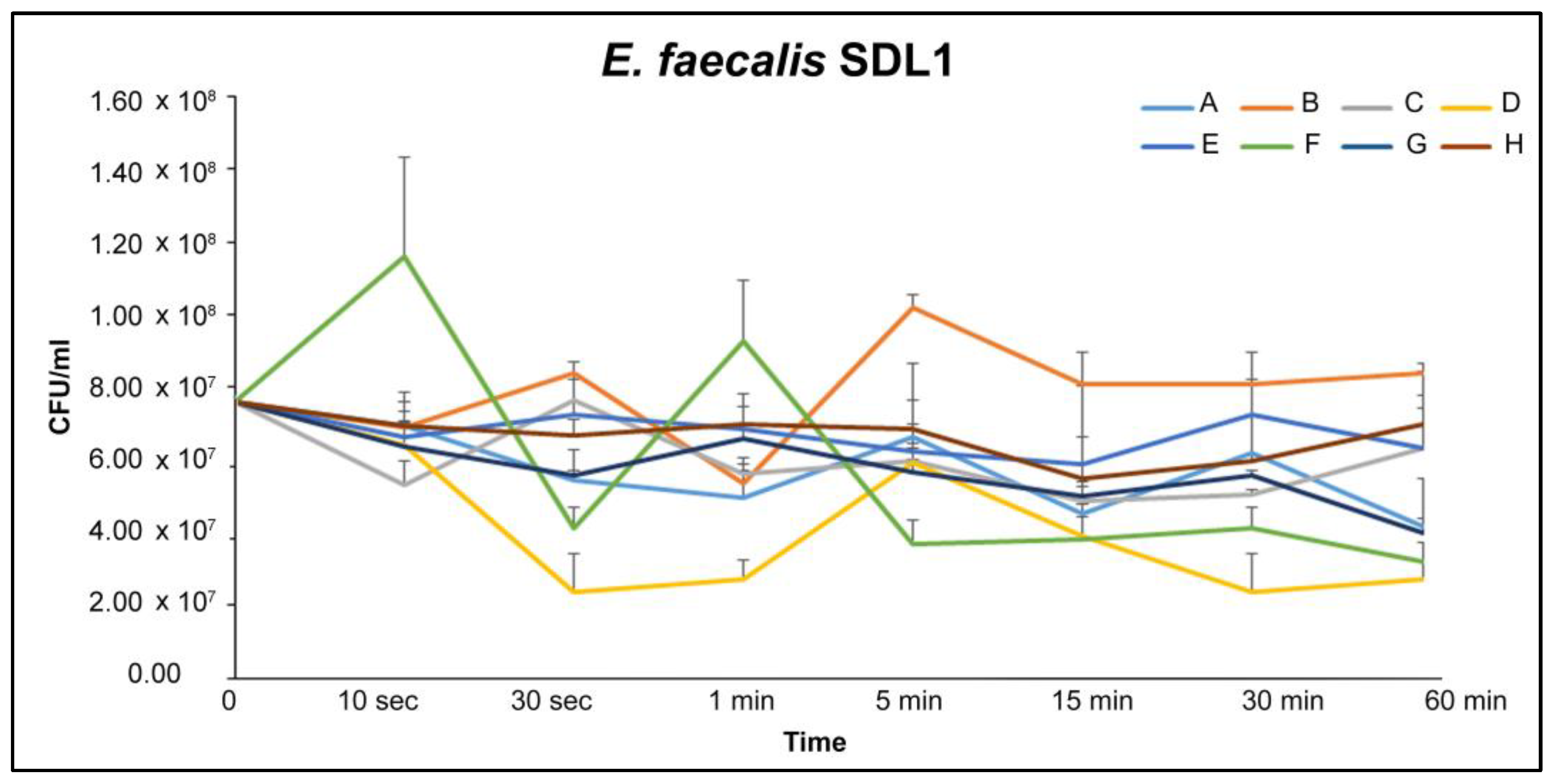
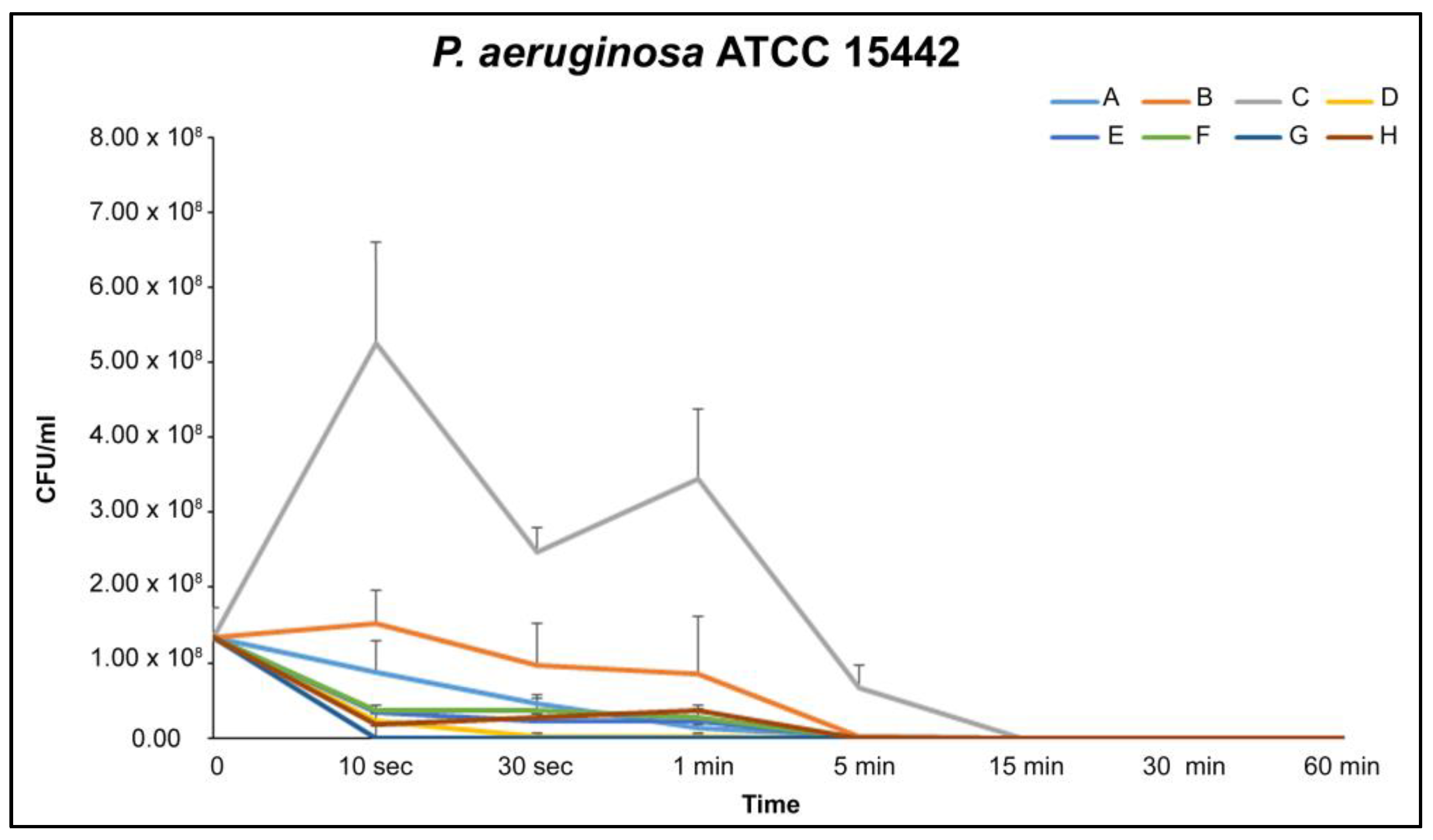
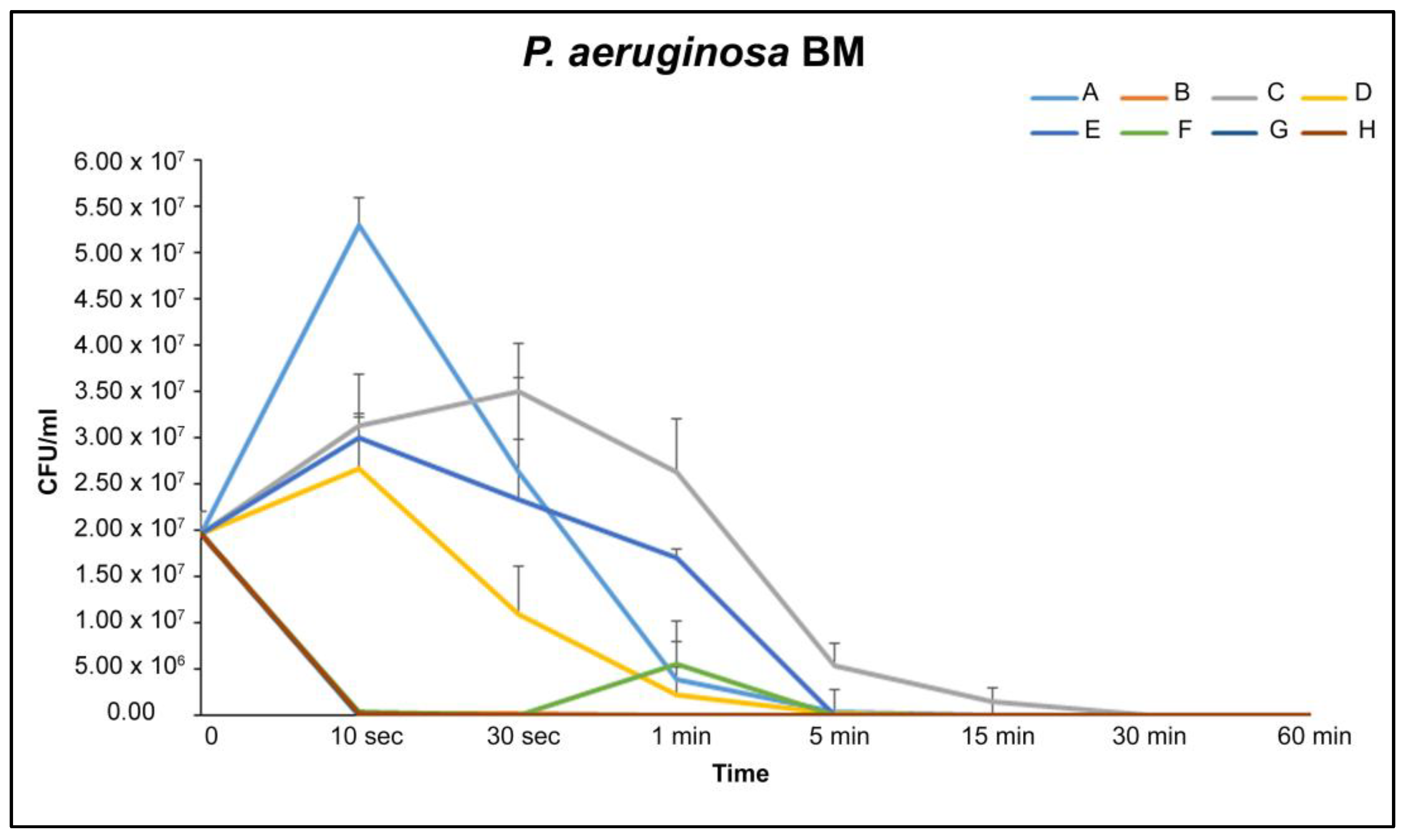
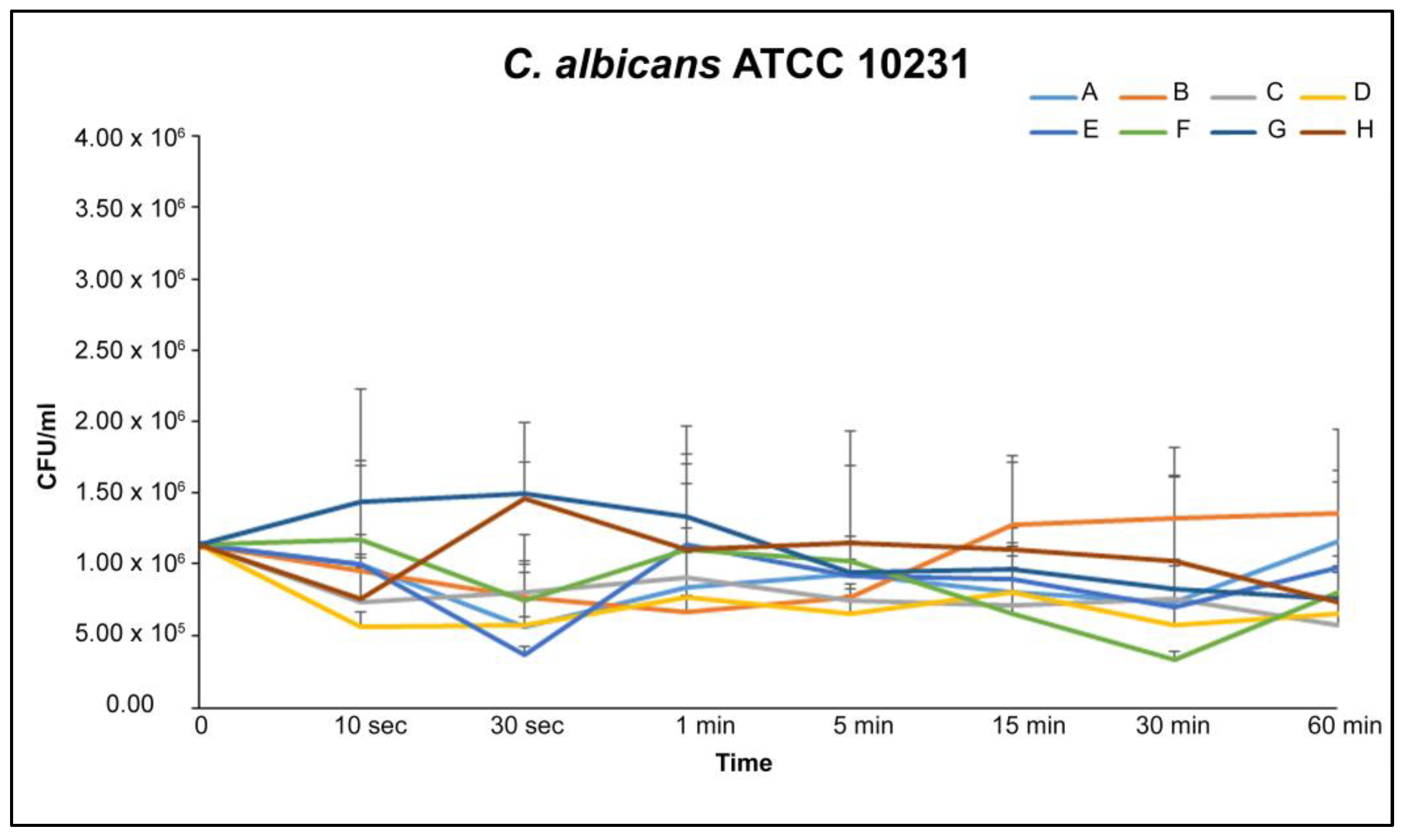
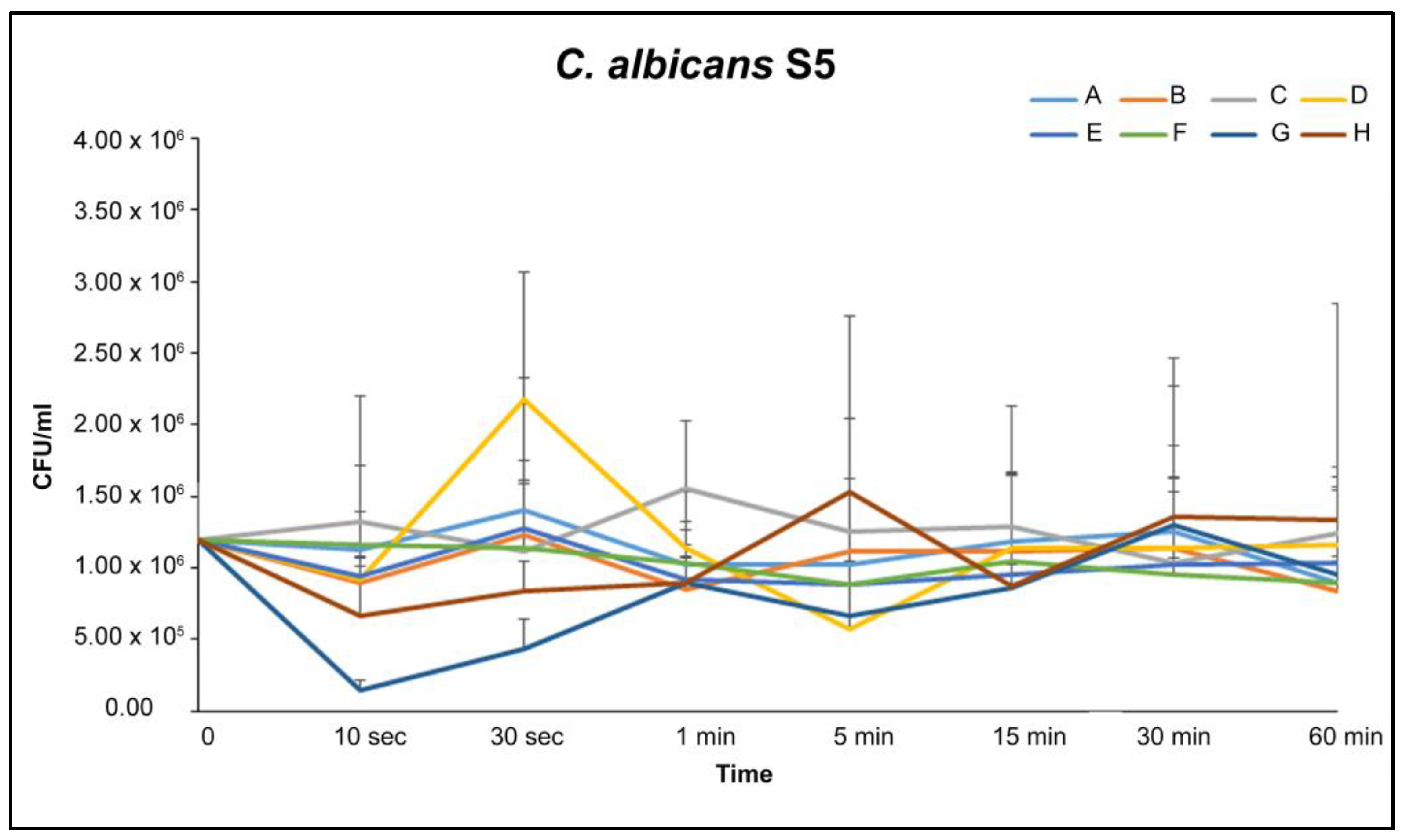
2.3. Antibacterial/Antifungal Activity over Time
3. Discussion
4. Materials and Methods
4.1. Mouthwashes
4.2. Substances
4.3. Microorganism Cultures
4.4. Mouthwashes Antimicrobial Action
4.5. Time Kill Curves
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khorolsuren, Z.; Lang, O.; Vag, J.; Kohidai, L. Effect of dental antiseptic agents on the viability of human periodontal ligament cells. Saudi Dent. J. 2021, 33, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Serrano, J.; Escribano, M.; Roldán, S.; Martín, C.; Herrera, D. Efficacy of adjunctive anti-plaque chemical agents in managing gingivitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42, 106–138. [Google Scholar] [CrossRef] [PubMed]
- Deus, F.P.; Ouanounou, A. Chlorhexidine in Dentistry: Pharmacology, Uses, and Adverse Effects. Int. Dent. J. 2022, 72, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Brookes, Z.L.S.; Bescos, R.; Belfield, L.A.; Ali, K.; Roberts, A. Current uses of chlorhexidine for management of oral disease: A narrative review. J. Dent. 2020, 103, 103497. [Google Scholar] [CrossRef] [PubMed]
- Van Strydonck, D.A.C.; Slot, D.E.; Van der Velden, U.; Van der Weijden, F. Effect of a chlorhexidine mouthrinse on plaque, gingival inflammation and staining in gingivitis patients: A systematic review. J. Clin. Periodontol. 2012, 39, 1042–1055. [Google Scholar] [CrossRef] [PubMed]
- Cunha, B.G.; Duque, C.; Caiaffa, K.S.; Massunari, L.; Catanoze, I.A.; dos Santos, D.M.; de Oliveira, S.H.P.; Guiotti, A.M. Cytotoxicity and antimicrobial effects of citronella oil (Cymbopogon nardus) and commercial mouthwashes on S. aureus and C. albicans biofilms in prosthetic materials. Arch. Oral Biol. 2020, 1, 109. [Google Scholar]
- Mao, X.; Auer, D.L.; Buchalla, W.; Hiller, K.-A.; Maisch, T.; Hellwig, E.; Al-Ahmad, A.; Cieplik, F. Cetylpyridinium Chloride: Mechanism of Action, Antimicrobial Efficacy in Biofilms, and Potential Risks of Resistance. Antimicrob. Agents Chemother. 2020, 64, e00576-20. [Google Scholar] [CrossRef]
- Brookes, Z.L.; A Belfield, L.; Ashworth, A.; Casas-Agustench, P.; Raja, M.; Pollard, A.J.; Bescos, R. Effects of chlorhexidine mouthwash on the oral microbiome. J. Dent. 2021, 113, 103768. [Google Scholar] [CrossRef]
- Amorim, C.V.G.; Aun, C.E.; Pinto, M.; Mayer, A. Susceptibility of some oral microorganisms to chlorhexidine and paramonochlorophenol Susceptibilidade de alguns microrganismos orais frente à clorexidina e ao paramonoclorofenol. Braz. Oral Res. 2004, 18, 242–248. [Google Scholar] [CrossRef]
- Câmara, A.C.; de Albuquerque, M.M.; Aguiar, C.M.; Correia, A.C.R.B. In vitro antimicrobial activity of 0.5%, 1%, and 2.5% sodium hypochlorite in root canals instrumented with the ProTaper Universal system. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 55–61. [Google Scholar] [CrossRef]
- Pourhajibagher, M.; Ghorbanzadeh, R.; Parker, S.; Chiniforush, N.; Bahador, A. The evaluation of cultivable microbiota profile in patients with secondary endodontic infection before and after photo-activated disinfection. Photodiagnosis Photodyn. Ther. 2017, 18, 198–203. [Google Scholar] [CrossRef] [PubMed]
- D’Ercole, S.; Di Fermo, P.; Di Giulio, M.; Di Lodovico, S.; Di Campli, E.; Scarano, A.; Tripodi, D.; Cellini, L.; Petrini, M. Near-infrared NIR irradiation and sodium hypochlorite: An efficacious association to counteract the Enterococcus faecalis biofilm in endodontic infections. J. Photochem. Photobiol. B 2020, 210, 111989. [Google Scholar] [CrossRef] [PubMed]
- Ardizzoni, A.; Blasi, E.; Rimoldi, C.; Giardino, L.; Ambu, E.; Righi, E.; Neglia, R. An in vitro and ex vivo study on two antibiotic-based endodontic irrigants: A challenge to sodium hypochlorite. New Microbiol. 2009, 32, 57–66. [Google Scholar]
- Ardizzoni, A.; Pericolini, E.; Paulone, S.; Orsi, C.F.; Castagnoli, A.; Oliva, I.; Strozzi, E.; Blasi, E. In Vitro effects of commercial mouthwashes on several virulence traits of Candida albicans, viridans streptococci and Enterococcus faecalis colonizing the oral cavity. PLoS ONE 2018, 13, e0207262. [Google Scholar] [CrossRef] [Green Version]
- Colombo, A.P.V.; Magalhães, C.B.; Hartenbach, F.A.R.R.; Souto, R.M.; Silva-Boghossian, C.M. Periodontal-disease-associated biofilm: A reservoir for pathogens of medical importance. Microb. Pathog. 2016, 94, 27–34. [Google Scholar] [CrossRef] [PubMed]
- D’Ercole, S.; Di Lodovico, S.; Iezzi, G.; Pierfelice, T.V.; D’Amico, E.; Cipollina, A.; Piattelli, A.; Cellini, L.; Petrini, M. Complex electromagnetic fields reduce candida albicans planktonic growth and its adhesion to titanium surfaces. Biomedicines 2021, 9, 1261. [Google Scholar] [CrossRef]
- Bürgers, R.; Schneider-Brachert, W.; Rosentritt, M.; Handel, G.; Hahnel, S. Candida albicans adhesion to composite resin materials. Clin. Oral Investig. 2009, 13, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.E.; Liu, Y.; Dhall, A.; Bawazir, M.; Koo, H.; Hwang, G. Synergism of Streptococcus mutans and Candida albicans Reinforces Biofilm Maturation and Acidogenicity in Saliva: An In Vitro Study. Front. Cell. Infect. Microbiol. 2021, 10, 623980. [Google Scholar] [CrossRef] [PubMed]
- da Costa, L.F.N.P.; Amaral, C.S.F.; Barbirato, D.S.; Leão, A.T.T.; Fogacci, M.F. Chlorhexidine mouthwash as an adjunct to mechanical therapy in chronic periodontitis: A meta-analysis. J. Am. Dent. Assoc. 2017, 148, 308–318. [Google Scholar] [CrossRef]
- Nagappan, N.; Ejaj, M.M.; D’Cruz, T.; Subbiah, G.; Tajuddin, R.; Subbiah, K. An In vitro Study to determine the antibacterial activity of chlorhexidine and herbal mouthrinses against Enterococcus faecalis. J. Pharm. Bioallied Sci. 2022, 14, 995. [Google Scholar] [CrossRef]
- Leshem, T.; Gilron, S.; Azrad, M.; Peretz, A. Characterization of reduced susceptibility to chlorhexidine among Gram-negative bacteria. Microbes Infect. 2022, 24, 104981. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G. Biocidal agents used for disinfection can enhance antibiotic resistance in gram-negative species. Antibiotics 2018, 7, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, L.; Narvekar, U.; McDonald, A.; Mullany, P. Prevalence of antibiotic resistance genes in the oral cavity and mobile genetic elements that disseminate antimicrobial resistance: A systematic review. Mol. Oral Microbiol. 2022, 37, 133–153. [Google Scholar] [CrossRef]
- Chavarría-Bolaños, D.; Esparza-Villalpando, V.; Ramírez, K. Antibacterial and Antifungal Capacity of Three Commercially Available Mouthwashes with Different Concentrations of Chlorhexidine. Int. J. Dent. Sci. 2022, 24, 57–68. [Google Scholar] [CrossRef]
- Shino, B.; Peedikayil, F.C.; Jaiprakash, S.R.; Ahmed Bijapur, G.; Kottayi, S.; Jose, D. Comparison of Antimicrobial Activity of Chlorhexidine, Coconut Oil, Probiotics, and Ketoconazole on Candida albicans Isolated in Children with Early Childhood Caries: An in Vitro Study. Scientifica 2016, 2016, 7061587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varoni, E.; Tarce, M.; Lodi, G.; Carrassi, A. Chlorhexidine (CHX) in dentistry: State of the art. Minerva Stomatol. 2012, 61, 399–419. [Google Scholar] [PubMed]
- Łukomska-Szymańska, M.; Sokołowski, J.; Łapińska, B. Chlorhexidine–mechanism of action and its application to dentistry. J. Stomatol. 2017, 70, 405–417. [Google Scholar]
- Hagi, A.; Iwata, K.; Nii, T.; Nakata, H.; Tsubotani, Y.; Inoue, Y. Bactericidal effects and mechanism of action of olanexidine gluconate, a new antiseptic. Antimicrob. Agents Chemother. 2015, 59, 4551–4559. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.I. The antibacterial and antiplaque effectiveness of mouthwashes containing cetylpyridinium chloride with and without alcohol in improving gingival health. J. Clin. Dent. 2011, 22, 179–182. [Google Scholar]
- Ayad, F.; Prado, R.; Mateo, L.R.; Stewart, B.; Szewczyk, G.; Arvanitidou, E.; Panagakos, F.S. A comparative investigation to evaluate the clinical efficacy of an alcohol-free CPC-containing mouthwash as compared to a control mouthwash in controlling dental plaque and gingivitis: A six-month clinical study on adults in San Jose, Costa Rica. J. Clin. Dent. 2011, 22, 204–212. [Google Scholar]
- Abouhussein, D.; El Nabarawi, M.A.; Shalaby, S.H.; El-Bary, A.A. Cetylpyridinium chloride chitosan blended mucoadhesive buccal films for treatment of pediatric oral diseases. J. Drug Deliv. Sci. Technol. 2020, 57, 101676. [Google Scholar] [CrossRef]
- Becker, K.; Brunello, G.; Scotti, L.; Drescher, D.; John, G. Efficacy of 0.05% chlorhexidine and 0.05% cetylpyridinium chloride mouthwash to eliminate living bacteria on in situ collected biofilms: An in vitro study. Antibiotics 2021, 10, 730. [Google Scholar] [CrossRef] [PubMed]
- Santos, S.; Herrera, D.; López, E.; O’Connor, A.; González, I.; Sanz, M. A randomized clinical trial on the short-term clinical and microbiological effects of the adjunctive use of a 0.05% chlorhexidine mouth rinse for patients in supportive periodontal care. J. Clin. Periodontol. 2004, 31, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Soers, C.; Desnyder, M.; Dekeyser, C.; Pauwels, M.; Van Steenberghe, D. A 0.05% cetyl pyridinium chloride/ 0.05% chlorhexidine mouth rinse during maintenance phase after initial periodontal therapy. J. Clin. Periodontol. 2005, 32, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Escribano, M.; Herrera, D.; Morante, S.; Teughels, W.; Quirynen, M.; Sanz, M. Efficacy of a low-concentration chlorhexidine mouth rinse in non-compliant periodontitis patients attending a supportive periodontal care programme: A randomized clinical trial. J. Clin. Periodontol. 2010, 37, 266–275. [Google Scholar] [CrossRef]
- Aghazadeh, M.; Eslami, H.; Samadi Kafil, H.; Aghazadeh, Z.; Behruzian, A.; Motahari, P. A Comparison of antimicrobial effect of the mouthwash containing chlorhexidine, Cetylpyridinium chloride, and zinc lactate (Halita) and chlorhexidine against Pseudomonas aeruginosa and Staphylococcus aureus: In vitro study. Sch. Bull. 2016, 2, 547–553. [Google Scholar]
- Neglia, R.; Ardizzoni, A.; Giardino, L.; Ambu, E.; Grazi, S.; Calignano, S.; Rimoldi, C.; Righi, E.; Blasi, E. Comparative in vitro and ex vivo studies on the bactericidal activity of Tetraclean, a new generation endodontic irrigant, and sodium hypochlorite. New Microbiol. 2008, 31, 57–65. [Google Scholar]
- Di Lodovico, S.; Bacchetti, T.; D’Ercole, S.; Covone, S.; Petrini, M.; Di Giulio, M.; Di Fermo, P.; Diban, F.; Ferretti, G.; Cellini, L. Complex Chronic Wound Biofilms Are Inhibited in vitro by the Natural Extract of Capparis spinose. Front. Microbiol. 2022, 13, 832919. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mouthwash | Composition | Manufacturer | LOTE |
|---|---|---|---|
| A—GUM® PAROEX® | 0.12% CHX + 0.05% CPC | GUM PAROEX, Saronno, Italy | I2112421 |
| B—GUM® PAROEX® | 0.06% CHX + 0.05% CPC | GUM PAROEX, Saronno, Italy | T11 |
| C—CURASEPT ADS 212 | 0.12% CHX + 0.05% CPC | CURASEPT S.p.A, Saronno, Italy | 045 2 |
| D—CURASEPT ADS 205 | 0.05% CHX | CURASEPT S.p.A, Saronno, Italy | 041 2 |
| E—PERIOAID® Intensive Care | 0.12% CHX + 0.05% CPC | DENTAID, S.L., Cerdanyola, Spain | S1142 |
| F—PERIOAID® Active Control | 0.05% CHX + 0.05% CPC | DENTAID, S.L., Cerdanyola, Spain | S1033 |
| G—Eludril Classic | 0.10% CHX + 0.50% Chlorobutanol | Pierre Fabre ORAL CARE—Lisboa, Portugal | G00202 |
| H—Eluday Care | 0.05% CHX + 0.05% CPC | Pierre Fabre ORAL CARE—Boulogne, France | G00023 |
| MIC (%vol/vol) | MBC/MFC (%vol/vol) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mouthwashes | E. faecalis | P. aeruginosa | C. albicans | E. faecalis | P. aeruginosa | C. albicans | ||||||
| ATCC 29212 | SDL1 | ATCC 15442 | BM | ATCC 10231 | S5 | ATCC 29213 | SDL1 | ATCC 15442 | BM | ATCC 10231 | S5 | |
| A | 0.19 | 0.04 | 1.56 | 3.12 | 0.04 | 0.04 | 1.56 | 0.09 | 3.12 | 3.12 | 0.04 | 0.04 |
| B | 0.19 | 0.09 | 3.12 | 12.50 | 0.09 | 0.02 | 1.56 | 0.78 | 3.12 | 12.50 | 0.09 | 0.02 |
| C | 0.19 | 0.39 | 1.56 | 1.56 | 0.09 | 0.02 | 1.56 | 6.25 | 6.25 | 12.50 | 0.09 | 0.02 |
| D | 0.78 | 1.56 | 6.25 | 6.25 | 0.09 | 0.02 | 1.56 | 12.50 | 12.50 | 50 | 0.09 | 0.19 |
| E | 0.19 | 0.09 | 1.56 | 3.12 | 0.09 | 0.04 | 0.39 | 0.39 | 3.12 | 3.12 | 0.09 | 0.04 |
| F | 0.19 | 0.09 | 3.12 | 12.50 | 0.02 | 0.04 | 1.56 | 0.39 | 3.12 | 25 | 0.02 | 0.04 |
| G | 0.39 | 0.39 | >50 | >50 | 0.04 | 0.04 | 1.56 | 0.78 | >50 | >50 | 1.56 | 0.04 |
| H | 0.19 | 0.09 | 3.12 | 12.50 | 0.09 | 0.04 | 0.39 | 0.39 | 6.25 | 25 | 0.09 | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Lodovico, S.; Dotta, T.C.; Cellini, L.; Iezzi, G.; D’Ercole, S.; Petrini, M. The Antibacterial and Antifungal Capacity of Eight Commercially Available Types of Mouthwash against Oral Microorganisms: An In Vitro Study. Antibiotics 2023, 12, 675. https://doi.org/10.3390/antibiotics12040675
Di Lodovico S, Dotta TC, Cellini L, Iezzi G, D’Ercole S, Petrini M. The Antibacterial and Antifungal Capacity of Eight Commercially Available Types of Mouthwash against Oral Microorganisms: An In Vitro Study. Antibiotics. 2023; 12(4):675. https://doi.org/10.3390/antibiotics12040675
Chicago/Turabian StyleDi Lodovico, Silvia, Tatiane Cristina Dotta, Luigina Cellini, Giovanna Iezzi, Simonetta D’Ercole, and Morena Petrini. 2023. "The Antibacterial and Antifungal Capacity of Eight Commercially Available Types of Mouthwash against Oral Microorganisms: An In Vitro Study" Antibiotics 12, no. 4: 675. https://doi.org/10.3390/antibiotics12040675
APA StyleDi Lodovico, S., Dotta, T. C., Cellini, L., Iezzi, G., D’Ercole, S., & Petrini, M. (2023). The Antibacterial and Antifungal Capacity of Eight Commercially Available Types of Mouthwash against Oral Microorganisms: An In Vitro Study. Antibiotics, 12(4), 675. https://doi.org/10.3390/antibiotics12040675