
Development and Validation of a Prognostic Model for Multi-Drug-Resistant Non-Hospital-Acquired Bloodstream Infection

 ,
,  , , and
, , and
Abstract
:1. Introduction
1.1. Pathogen-Related Prognostic Risk Factors
1.2. Host-Related Prognostic Risk Factors
1.3. Bloodstream Infection Classification
2. Results
2.1. Demographic Characteristics and Risk Factors
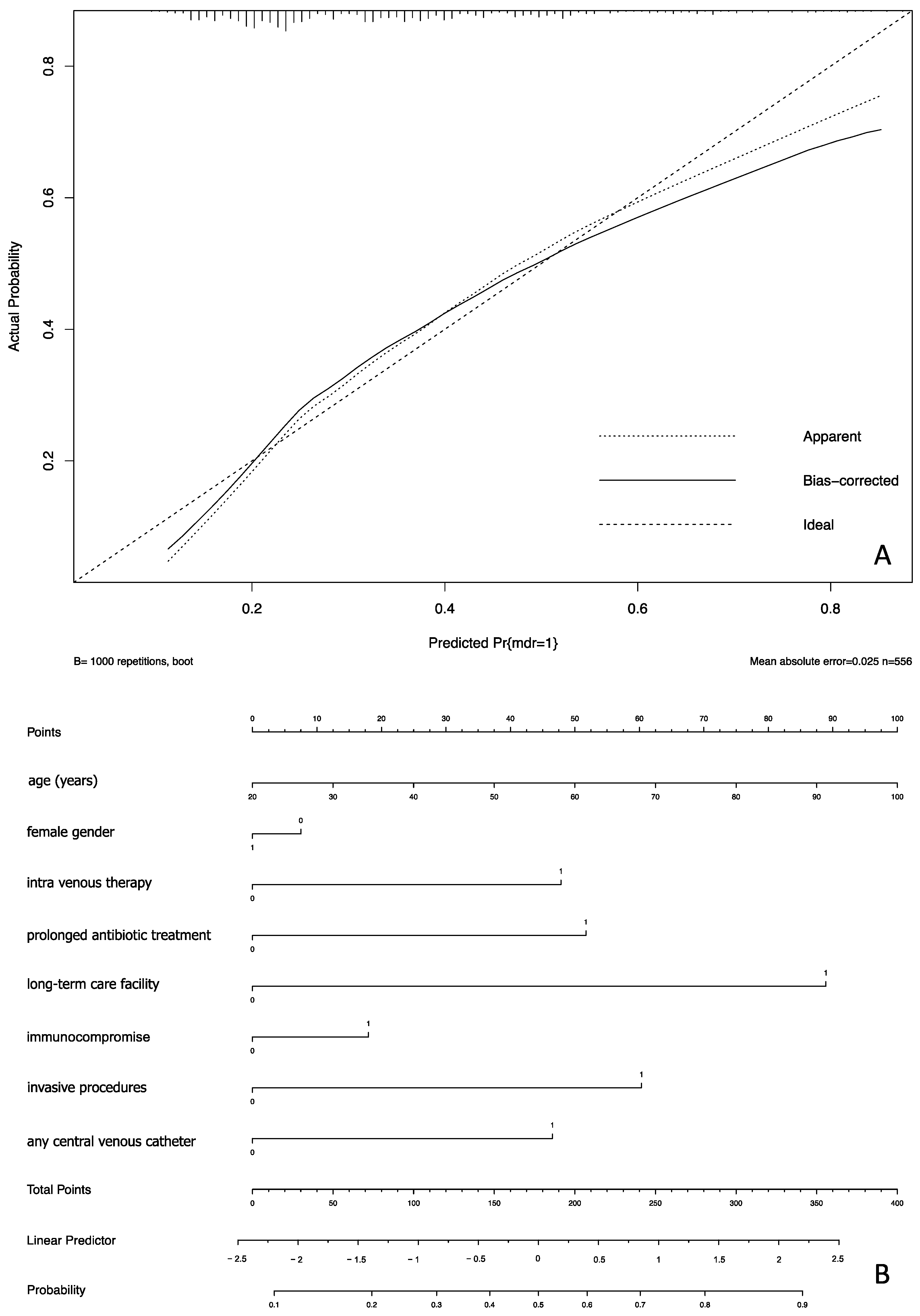
2.2. Prognostic Model Development
2.3. Model External Validation
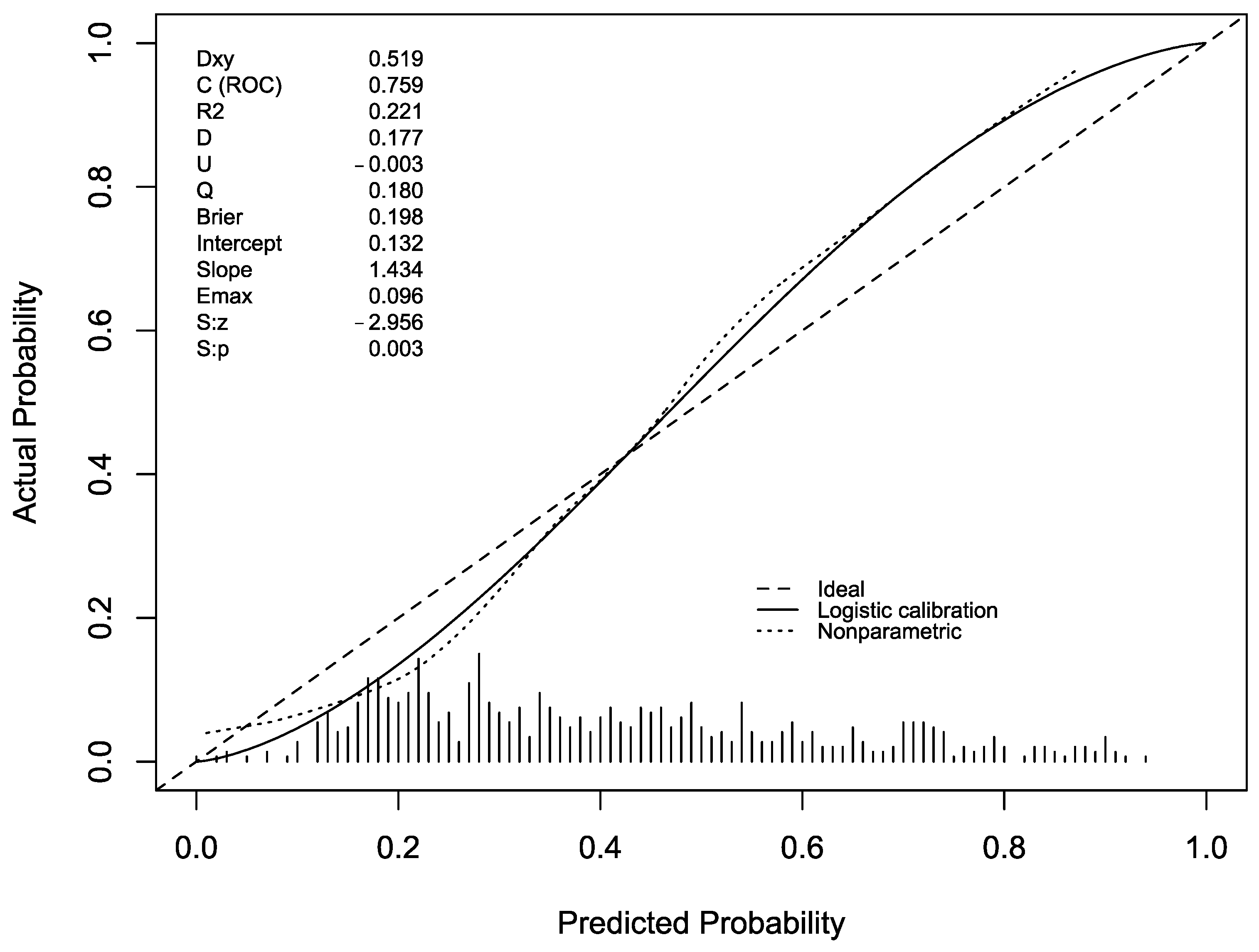
2.3.1. Temporal Study
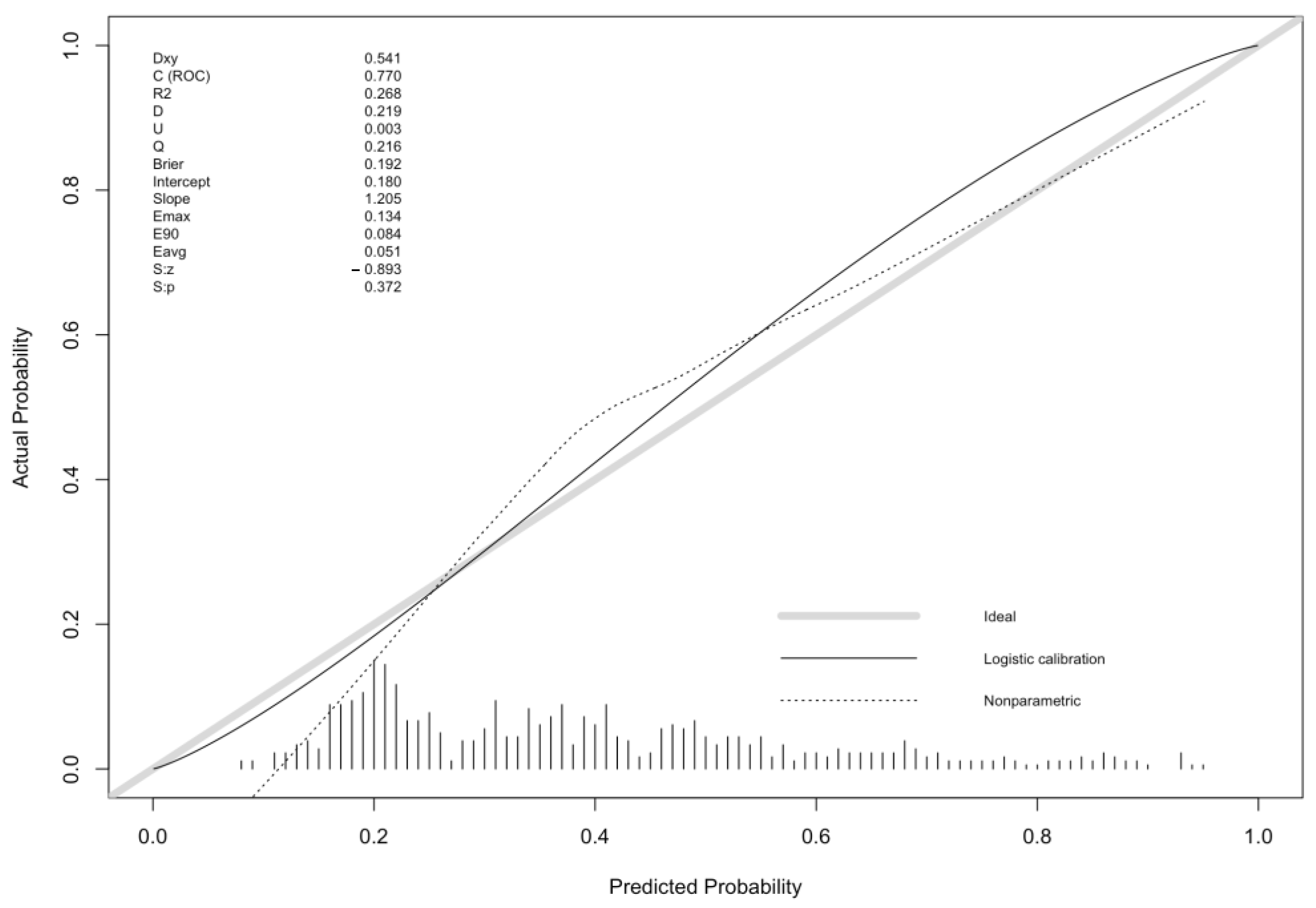
2.3.2. Spatial Study
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kern, W.V.; Rieg, S. Burden of Bacterial Bloodstream Infection—A Brief Update on Epidemiology and Significance of Multidrug-Resistant Pathogens. Clin. Microbiol. Infect. 2020, 26, 151–157. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, G.; Fiori, B.; Menchinelli, G.; D’Inzeo, T.; Liotti, F.M.; Morandotti, G.A.; Sanguinetti, M.; Posteraro, B.; Spanu, T. Incidence and Antimicrobial Resistance Trends in Bloodstream Infections Caused by ESKAPE and Escherichia Coli at a Large Teaching Hospital in Rome, a 9-Year Analysis (2007–2015). Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1627–1636. [Google Scholar] [CrossRef] [PubMed]
- Goto, M.; Al-Hasan, M.N. Overall Burden of Bloodstream Infection and Nosocomial Bloodstream Infection in North America and Europe. Clin. Microbiol. Infect. 2013, 19, 501–509. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.F.; Righi, E.; Wright, H.; Hartel, G.F.; Harris, P.N.A.; Paterson, D.L. Long-Term Morbidity and Mortality Following Bloodstream Infection: A Systematic Literature Review. J. Infect. 2018, 77, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ju, M.; Huang, Y.; Xu, X.; Qian, Y.; Bi, Y.; Liu, S.; Dong, S.; Yuan, J.; Lin, D. Predictors of Mortality in Adult Patients with Methicillin-Resistant Staphylococcus Aureus Bloodstream Infection: A Meta-Analysis and Systematic Review. Ann. Palliat. Med. 2021, 10, 8617–8627. [Google Scholar] [CrossRef] [PubMed]
- Jiang, A.-M.; Liu, N.; Zhao, R.; Zheng, H.-R.; Chen, X.; Fan, C.-X.; Zhang, R.; Zheng, X.-Q.; Fu, X.; Yao, Y.; et al. Clinical Outcomes and Prognostic Factors in Bloodstream Infections Due to Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae among Patients with Malignancy: A Meta-Analysis. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 53. [Google Scholar] [CrossRef]
- Alevizakos, M.; Gaitanidis, A.; Andreatos, N.; Arunachalam, K.; Flokas, M.E.; Mylonakis, E. Bloodstream Infections Due to Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae among Patients with Malignancy: A Systematic Review and Meta-Analysis. Int. J. Antimicrob. Agents 2017, 50, 657–663. [Google Scholar] [CrossRef]
- Russo, A.; Falcone, M.; Gutiérrez-Gutiérrez, B.; Calbo, E.; Almirante, B.; Viale, P.L.; Oliver, A.; Ruiz-Garbajosa, P.; Gasch, O.; Gozalo, M.; et al. Predictors of Outcome in Patients with Severe Sepsis or Septic Shock Due to Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae. Int. J. Antimicrob. Agents 2018, 52, 577–585. [Google Scholar] [CrossRef]
- Wang, L.; Xin, Y.; Zhou, J.; Tian, Z.; Liu, C.; Yu, X.; Meng, X.; Jiang, W.; Zhao, S.; Dong, Q. Gastric Mucosa-Associated Microbial Signatures of Early Gastric Cancer. Front. Microbiol. 2020, 11, 1548. [Google Scholar] [CrossRef]
- Dicksved, J.; Lindberg, M.; Rosenquist, M.; Enroth, H.; Jansson, J.K.; Engstrand, L. Molecular Characterization of the Stomach Microbiota in Patients with Gastric Cancer and in Controls. J. Med. Microbiol. 2009, 58, 509–516. [Google Scholar] [CrossRef]
- Zhou, S.; Li, C.; Liu, L.; Yuan, Q.; Miao, J.; Wang, H.; Ding, C.; Guan, W. Gastric Microbiota: An Emerging Player in Gastric Cancer. Front. Microbiol. 2023, 14, 1130001. [Google Scholar] [CrossRef] [PubMed]
- Osamura, Y.; Nishiyama, H.; Hattori, T.; Gunji, M.; Yuasa, N. Clinico-Bacterial and Prognostic Factors in Patients with Suspected Blood Stream Infection and Elevated Serum Procalcitonin Levels. Nagoya J. Med. Sci. 2022, 84, 230. [Google Scholar] [PubMed]
- Gao, Y.; Tang, M.; Li, Y.; Niu, X.; Li, J.; Fu, C.; Wang, Z.; Liu, J.; Song, B.; Chen, H.; et al. Machine-Learning Based Prediction and Analysis of Prognostic Risk Factors in Patients with Candidemia and Bacteraemia: A 5-Year Analysis. PeerJ 2022, 10, e13594. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Gao, Y.; Qiu, Y.; Zhu, H.; Zhang, S.; Summah, H.D.; Shi, G.; Cheng, T.; Yang, Z.; Feng, Y. The Prognostic Factors of Bloodstream Infection in Immunosuppressed Elderly Patients: A Retrospective, Single-Center, Five-Year Cohort Study. CIA 2022, 17, 1647–1656. [Google Scholar] [CrossRef]
- Friedman, N.D. Health Care–Associated Bloodstream Infections in Adults: A Reason to Change the Accepted Definition of Community-Acquired Infections. Ann. Intern. Med. 2002, 137, 791–797. [Google Scholar] [CrossRef]
- Lujan, M.; Gallego, M.; Rello, J. Healthcare-Associated Infections. A Useful Concept? Curr. Opin. Crit. Care 2009, 15, 419–424. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Klastersky, J.; De Naurois, J.; Rolston, K.; Rapoport, B.; Maschmeyer, G.; Aapro, M.; Herrstedt, J. Management of Febrile Neutropaenia: ESMO Clinical Practice Guidelines. Ann. Oncol. 2016, 27, v111–v118. [Google Scholar] [CrossRef]
- Pien, B.C.; Sundaram, P.; Raoof, N.; Costa, S.F.; Mirrett, S.; Woods, C.W.; Reller, L.B.; Weinstein, M.P. The Clinical and Prognostic Importance of Positive Blood Cultures in Adults. Am. J. Med. 2010, 123, 819–828. [Google Scholar] [CrossRef]
- Wang, W.; Chen, W.; Liu, Y.; Li, L.; Li, S.; Tan, J.; Sun, X. Blood Glucose Levels and Mortality in Patients With Sepsis: Dose–Response Analysis of Observational Studies. J. Intensive Care Med. 2021, 36, 182–190. [Google Scholar] [CrossRef]
- Wang, J.; Zhu, C.-K.; Yu, J.-Q.; Tan, R.; Yang, P.-L. Hypoglycemia and Mortality in Sepsis Patients: A Systematic Review and Meta-Analysis. Heart Lung 2021, 50, 933–940. [Google Scholar] [CrossRef]
- Steyerberg, E.W. Clinical Prediction Models: A Practical Approach to Development, Validation, and Updating; Statistics for biology and health; Springer: New York, NY, USA, 2009; ISBN 978-0-387-77243-1. [Google Scholar]
- Mann, H.B.; Whitney, D.R. On a Test of Whether One of Two Random Variables Is Stochastically Larger than the Other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- McNemar, Q. Note on the Sampling Error of the Difference between Correlated Proportions or Percentages. Psychometrika 1947, 12, 153–157. [Google Scholar] [CrossRef]
- Kollef, M.H.; Morrow, L.E.; Baughman, R.P.; Craven, D.E.; McGowan, J.E., Jr.; Micek, S.T.; Niederman, M.S.; Ost, D.; Paterson, D.L.; Segreti, J. Health Care–Associated Pneumonia (HCAP): A Critical Appraisal to Improve Identification, Management, and Outcomes—Proceedings of the HCAP Summit. Clin. Infect. Dis. 2008, 46, S296–S334. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zheng, Z.; Shi, Q.; Wu, H.; Li, Y.; Zheng, C. Multidrug-Resistant Acinetobacter Baumannii May Cause Patients to Develop Polymicrobial Bloodstream Infection. Can. J. Infect. Dis. Med. Microbiol. 2022, 2022, 8368578. [Google Scholar] [CrossRef]
- Lin, J.-N.; Lai, C.-H.; Chen, Y.-H.; Chang, L.-L.; Lu, P.-L.; Tsai, S.-S.; Lin, H.-L.; Lin, H.-H. Characteristics and Outcomes of Polymicrobial Bloodstream Infections in the Emergency Department: A Matched Case-Control Study: Polymicrobial bloodstream infections in the ED. Acad. Emerg. Med. 2010, 17, 1072–1079. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F. Regression Modeling Strategies—With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: New York, NY, USA, 2001; ISBN 978-1-4757-3462-1. [Google Scholar]
- Lubsen, J.; Pool, J.; van der Does, E. A Practical Device for the Application of a Diagnostic or Prognostic Function. Methods Inf. Med. 1978, 17, 127–129. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M. Predictive Accuracy and Explained Variation. Stat. Med. 2003, 22, 2299–2308. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST) Breakpoints (Version 11.0). 2021. Available online: https://www.eucast.org/eucast_news/news_singleview?tx_ttnews%5Btt_news%5D=404&cHash=74a1f440876cb3eefb60e6ad39c622e7 (accessed on 31 December 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Development Cohort (N = 556) | Temporal External Validation Cohort (N = 609) | Spatial External Validation Cohort (N = 253) | |
|---|---|---|---|
| Median age, years (IQR) 1 | 70.5 (19) | 73 (18) | 72.7 (20.1) |
| Male/female ratio | 1.35 | 1.26 | 1.1 |
| Mortality in hospital 2 | 69 (12.4%) | 75 (15.7%) | 34 (13.4%) |
| Long-term care facility | 31 (5.6%) | 51 (8.4%) | 22 (8.7%) |
| Recent hospitalization | 238 (42.8%) | 148 (24.3%) | 61 (24.1%) |
| Recent antibiotic treatment | 113 (20.3%) | 123 (20.2%) | 48 (19%) |
| Recent intravenous therapy | 117 (20%) | 120 (19.7%) | 40 (15.8%) |
| Hemodialysis | 17 (3.6%) | 15 (2.5%) | 5 (2%) |
| Immunocompromise 3 | 146 (26.3%) | 107 (17.6%) | 46 (18.2%) |
| Diabetes | 134 (24.1%) | 175 (28.7%) | 66 (26.1%) |
| COPD 4 | 63 (11.3%) | 79 (13%) | 33 (13%) |
| Any type of cardiopathy | 172 (30.9%) | 203 (33.3%) | 85 (33.6%) |
| Chronic renal failure | 118 (21.2%) | 102 (16.8%) | 40 (15.9%) |
| Liver cirrhosis | 48 (8.6%) | 35 (5.8%) | 26 (10.3%) |
| Cerebrovascular disease | 98 (17.6%) | 88 (14.5%) | 42 (16.6%) |
| Any type of solid tumor | 93 (16.7%) | 95 (15.6%) | 34 (13.8%) |
| Any type of hematological tumor | 45 (8.2%) | 34 (5.6%) | 18 (7.1%) |
| Neutropenia 5 at arrival in hospital | 33 (5.9%) | 12 (2%) | 8 (3.2%) |
| Development Cohort (N = 556) | Temporal External Validation Cohort (N = 609) | Spatial External Validation Cohort (N = 253) | |
|---|---|---|---|
| Any type or recent surgical operation 1 | 45 (8.1%) | 57 (9.4%) | 24 (9.5%) |
| Any valvular prosthesis | 24 (4.3%) | 49 (8%) | 39 (15.4%) |
| Any vascular prosthesis | 8 (1.4%) | 22 (3.6%) | 7 (2.8%) |
| Any central venous catheterization 2 | 154 (27.7%) | 71 (11.7%) | 52 (20.6%) |
| Any invasive procedures 3 | 124 (22.3%) | 63 (10.34%) | 40 (15.8%) |
| Development Cohort (N = 556) | Temporal External Validation Cohort (N = 609) | Spatial External Validation Cohort (N = 253) | |
|---|---|---|---|
| Staphylococcus aureus | 47 (24.7%) | 42 (23.7%) | 18 (21.9%) |
| Staphylococcus epidermidis | 15 (8.5%) | 17 (9.6%) | 10 (12.2%) |
| Staphylococcus hominis | 24 (12.6%) | 25 (14.1%) | 12 (14.6%) |
| Coagulase-negative Staphylococci | 6 (3.2%) | 6 (3.4%) | 3 (3.7%) |
| Enterococcus faecium | 8 (4.2%) | 3 (1.7%) | 2 (2.4%) |
| Escherichia coli | 61 (32.1%) | 70 (39.5%) | 30 (39%) |
| Klebsiella pneumoniae | 12 (6.3%) | 10 (5.7%) | 4 (4.9%) |
| Pseudomonas aeruginosa | 4 (2.2%) | 4 (2.3%) | 1 (1.2%) |
| Univariable Model OR | Multivariable Model OR | |
|---|---|---|
| Age (year) | 1.01 (0.99–1.02) | 1.02 (1.00–1.03) |
| Female gender | 0.94 (0.66–1.34) | 0.9 (0.62–1.34) |
| Long-term care facility admission | 3.8 (1.78–8.1) | 3.3 (1.46–7.43) |
| Immunocompromise 1 | 1.5 (1.05–2.16) | 1.27 (0.83–1.94) |
| Any recent invasive procedures 2 | 2.27 (1.51–3.42) | 2.25 (1.45–3.47) |
| Any central venous catheterization 3 | 2.46 (1.68–3.61) | 1.87 (1.18–2.94) |
| Recent intravenous treatment | 3 (1.97–4.56) | 1.9 (1.16–3.11) |
| Recent antibiotic treatment | 2.37 (1.56–3.61) | 2 (1.26–3.17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pivetta, E.; Corcione, S.; Peasso, P.; Cara, I.; Capodanno, A.; Brussino, A.; Petitti, P.; Galli, E.; Galmozzi, M.; Ghisetti, V.; et al. Development and Validation of a Prognostic Model for Multi-Drug-Resistant Non-Hospital-Acquired Bloodstream Infection. Antibiotics 2023, 12, 955. https://doi.org/10.3390/antibiotics12060955
Pivetta E, Corcione S, Peasso P, Cara I, Capodanno A, Brussino A, Petitti P, Galli E, Galmozzi M, Ghisetti V, et al. Development and Validation of a Prognostic Model for Multi-Drug-Resistant Non-Hospital-Acquired Bloodstream Infection. Antibiotics. 2023; 12(6):955. https://doi.org/10.3390/antibiotics12060955
Chicago/Turabian StylePivetta, Emanuele, Silvia Corcione, Paolo Peasso, Irene Cara, Alberto Capodanno, Andrea Brussino, Paolo Petitti, Eleonora Galli, Maddalena Galmozzi, Valeria Ghisetti, and et al. 2023. "Development and Validation of a Prognostic Model for Multi-Drug-Resistant Non-Hospital-Acquired Bloodstream Infection" Antibiotics 12, no. 6: 955. https://doi.org/10.3390/antibiotics12060955
APA StylePivetta, E., Corcione, S., Peasso, P., Cara, I., Capodanno, A., Brussino, A., Petitti, P., Galli, E., Galmozzi, M., Ghisetti, V., Cavallo, R., Aprà, F., Lupia, E., De Rosa, F. G., & Montrucchio, G. (2023). Development and Validation of a Prognostic Model for Multi-Drug-Resistant Non-Hospital-Acquired Bloodstream Infection. Antibiotics, 12(6), 955. https://doi.org/10.3390/antibiotics12060955