

Real-World Data in Pharmacovigilance Database Provides a New Perspective for Understanding the Risk of Clostridium difficile Infection Associated with Antibacterial Drug Exposure

 ,
,
Abstract
:1. Introduction
2. Results
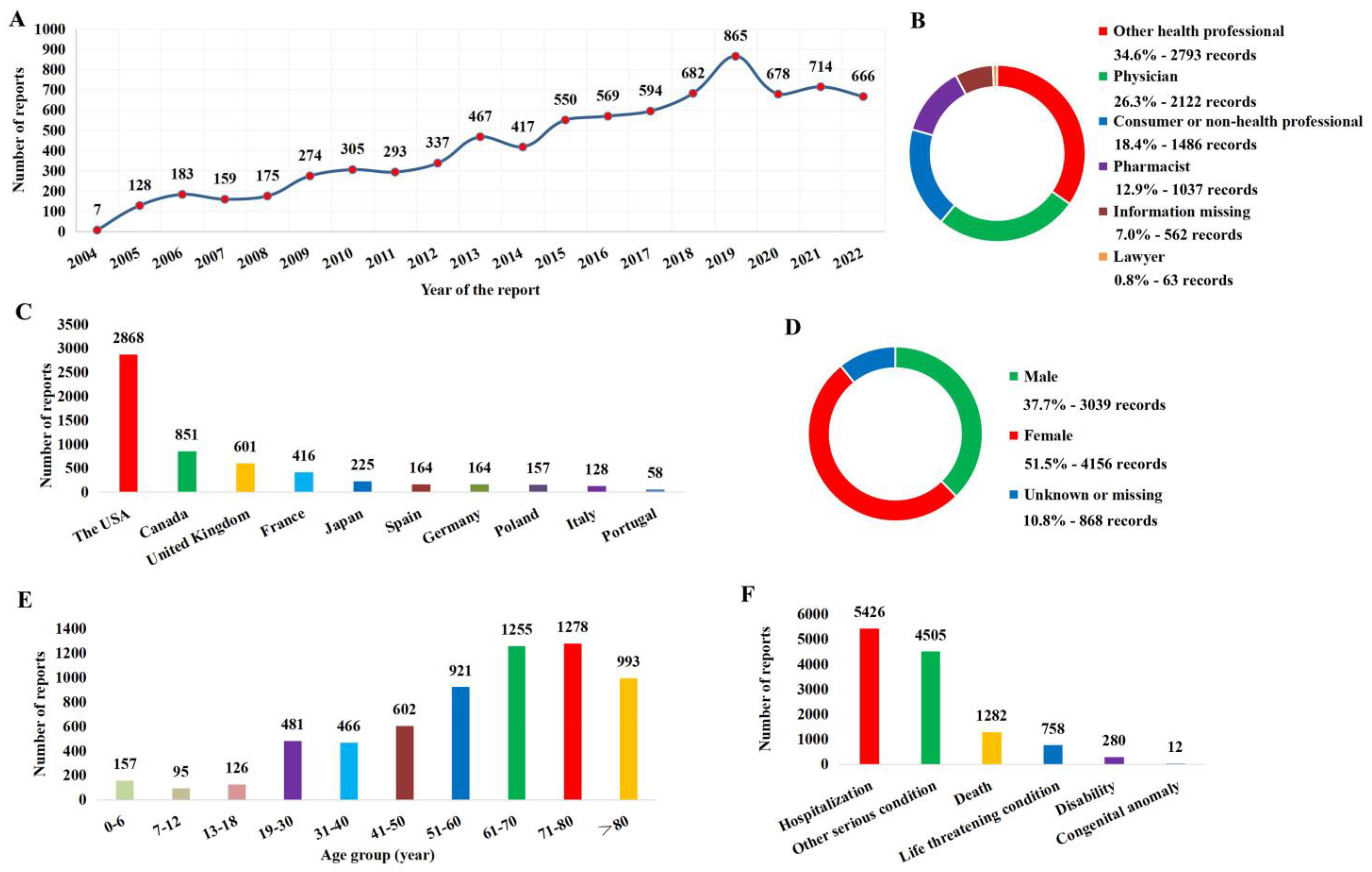
2.1. Report Basic Information and Patient Characteristics
2.2. ADR Signal Detection Results
2.3. Distribution of ADR Signals
3. Discussion
4. Materials and Methods
4.1. Data Source
4.2. Identification of CDI Reports Associated with Antibacterial Drug Use in FAERS
4.3. ADR Signal Detection Method
4.4. Data Collection and Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martin, J.S.; Monaghan, T.M.; Wilcox, M.H. Clostridium difficile infection: Epidemiology, diagnosis and understanding transmission. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 206–216. [Google Scholar] [CrossRef] [Green Version]
- Owens, R.C., Jr.; Donskey, C.J.; Gaynes, R.P.; Loo, V.G.; Muto, C.A. Antimicrobial-associated risk factors for Clostridium difficile infection. Clin. Infect. Dis. 2008, 46 (Suppl. 1), S19–S31. [Google Scholar] [CrossRef] [Green Version]
- Karas, J.A.; Enoch, D.A.; Aliyu, S.H. A review of mortality due to Clostridium difficile infection. J. Infect. 2010, 61, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.P.; LaMont, J.T. Clostridium difficile—More difficult than ever. N. Engl. J. Med. 2008, 359, 1932–1940. [Google Scholar] [CrossRef] [PubMed]
- Trubiano, J.A.; Cheng, A.C.; Korman, T.M.; Roder, C.; Campbell, A.; May, M.L.; Blyth, C.C.; Ferguson, J.K.; Blackmore, T.K.; Riley, T.V.; et al. Australasian Society of Infectious Diseases updated guidelines for the management of Clostridium difficile infection in adults and children in Australia and New Zealand. Intern. Med. J. 2016, 46, 479–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Sartelli, M.; Di Bella, S.; McFarland, L.V.; Khanna, S.; Furuya-Kanamori, L.; Abuzeid, N.; Abu-Zidan, F.M.; Ansaloni, L.; Augustin, G.; Bala, M.; et al. 2019 update of the WSES guidelines for management of Clostridioides (Clostridium) difficile infection in surgical patients. World J. Emerg. Surg. 2019, 14, 8. [Google Scholar] [CrossRef] [Green Version]
- Kelly, C.R.; Fischer, M.; Allegretti, J.R.; LaPlante, K.; Stewart, D.B.; Limketkai, B.N.; Stollman, N.H. ACG Clinical Guidelines: Prevention, Diagnosis, and Treatment of Clostridioides difficile Infections. Am. J. Gastroenterol. 2021, 116, 1124–1147. [Google Scholar] [CrossRef]
- van Prehn, J.; Reigadas, E.; Vogelzang, E.H.; Bouza, E.; Hristea, A.; Guery, B.; Krutova, M.; Noren, T.; Allerberger, F.; Coia, J.E.; et al. European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin. Microbiol. Infect. 2021, 27 (Suppl. 2), S1–S21. [Google Scholar] [CrossRef]
- Gaffin, N.; Spellberg, B. Sustained reductions in unnecessary antimicrobial administration and hospital Clostridioides difficile rates via stewardship in a nonacademic setting. Infect. Control. Hosp. Epidemiol. 2023, 44, 491–493. [Google Scholar] [CrossRef]
- Hecker, M.T.; Son, A.H.; Alhmidi, H.; Wilson, B.M.; Wiest, P.M.; Donskey, C.J. Efficacy of a stewardship intervention focused on reducing unnecessary use of non-Clostridioides difficile antibiotics in patients with Clostridioides difficile infection. Infect. Control. Hosp. Epidemiol. 2020, 41, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Morgan, F.; Belal, M.; Lisa, B.; Ford, F.; LeMaitre, B.; Psevdos, G. Antimicrobial stewardship program achieved marked decrease in Clostridium difficile infections in a Veterans Hospital. Am. J. Infect. Control. 2020, 48, 1119–1121. [Google Scholar] [CrossRef]
- Pepin, J.; Saheb, N.; Coulombe, M.A.; Alary, M.E.; Corriveau, M.P.; Authier, S.; Leblanc, M.; Rivard, G.; Bettez, M.; Primeau, V.; et al. Emergence of fluoroquinolones as the predominant risk factor for Clostridium difficile-associated diarrhea: A cohort study during an epidemic in Quebec. Clin. Infect. Dis. 2005, 41, 1254–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, K.; Bergeron, L.; Bernatchez, H.; Goyette, M.; Savoie, M.; Thirion, D. Clostridium difficile-associated diarrhoea rates and global antibiotic consumption in five Quebec institutions from 2001 to 2004. Int. J. Antimicrob. Agents 2007, 30, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Blondeau, J.M. What have we learned about antimicrobial use and the risks for Clostridium difficile-associated diarrhoea? J. Antimicrob. Chemother. 2009, 63, 238–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raschi, E.; La Placa, M.; Poluzzi, E.; De Ponti, F. The value of case reports and spontaneous reporting systems for pharmacovigilance and clinical practice. Br. J. Dermatol. 2021, 184, 581–583. [Google Scholar] [CrossRef]
- Bohm, R.; von Hehn, L.; Herdegen, T.; Klein, H.J.; Bruhn, O.; Petri, H.; Hocker, J. OpenVigil FDA—Inspection of U.S. American Adverse Drug Events Pharmacovigilance Data and Novel Clinical Applications. PLoS ONE 2016, 11, e0157753. [Google Scholar] [CrossRef]
- Seo, H.; Kim, E. Electrolyte Disorders Associated with Piperacillin/Tazobactam: A Pharmacovigilance Study Using the FAERS Database. Antibiotics 2023, 12, 240. [Google Scholar] [CrossRef]
- Patek, T.M.; Teng, C.; Kennedy, K.E.; Alvarez, C.A.; Frei, C.R. Comparing Acute Kidney Injury Reports Among Antibiotics: A Pharmacovigilance Study of the FDA Adverse Event Reporting System (FAERS). Drug Saf. 2020, 43, 17–22. [Google Scholar] [CrossRef]
- Calderwood, S.B.; Moellering, R.C., Jr. Common adverse effects of antibacterial agents on major organ systems. Surg. Clin. N. Am. 1980, 60, 65–81. [Google Scholar] [CrossRef]
- Slimings, C.; Riley, T.V. Antibiotics and hospital-acquired Clostridium difficile infection: Update of systematic review and meta-analysis. J. Antimicrob. Chemother. 2014, 69, 881–891. [Google Scholar] [CrossRef]
- Webb, B.J.; Subramanian, A.; Lopansri, B.; Goodman, B.; Jones, P.B.; Ferraro, J.; Stenehjem, E.; Brown, S.M. Antibiotic Exposure and Risk for Hospital-Associated Clostridioides difficile Infection. Antimicrob. Agents Chemother. 2020, 64, e02169-19. [Google Scholar] [CrossRef] [PubMed]
- Schechner, V.; Fallach, N.; Braun, T.; Temkin, E.; Carmeli, Y. Antibiotic exposure and the risk of hospital-acquired diarrhoea and Clostridioides difficile infection: A cohort study. J. Antimicrob. Chemother. 2021, 76, 2182–2185. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.J.; Daneman, N.; van Walraven, C. Influence of antibiotics and case exposure on hospital-acquired Clostridium difficile infection independent of illness severity. J. Hosp. Infect. 2017, 95, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Alatawi, Y.M.; Hansen, R.A. Empirical estimation of under-reporting in the U.S. Food and Drug Administration Adverse Event Reporting System (FAERS). Expert. Opin. Drug Saf. 2017, 16, 761–767. [Google Scholar] [CrossRef]
- Li, D.; Gou, J.; Zhu, J.; Zhang, T.; Liu, F.; Zhang, D.; Dai, L.; Li, W.; Liu, Q.; Qin, C.; et al. Severe cutaneous adverse reactions to drugs: A real-world pharmacovigilance study using the FDA Adverse Event Reporting System database. Front. Pharmacol. 2023, 14, 1117391. [Google Scholar] [CrossRef]
- Hoffman, K.B.; Dimbil, M.; Erdman, C.B.; Tatonetti, N.P.; Overstreet, B.M. The Weber effect and the United States Food and Drug Administration’s Adverse Event Reporting System (FAERS): Analysis of sixty-two drugs approved from 2006 to 2010. Drug Saf. 2014, 37, 283–294. [Google Scholar] [CrossRef] [Green Version]
- Neha, R.; Subeesh, V.; Beulah, E.; Gouri, N.; Maheswari, E. Existence of Notoriety Bias in FDA Adverse Event Reporting System Database and Its Impact on Signal Strength. Hosp. Pharm. 2021, 56, 152–158. [Google Scholar] [CrossRef]
- Wichelmann, T.A.; Abdulmujeeb, S.; Ehrenpreis, E.D. Bevacizumab and gastrointestinal perforations: A review from the FDA Adverse Event Reporting System (FAERS) database. Aliment. Pharmacol. Ther. 2021, 54, 1290–1297. [Google Scholar] [CrossRef]
- Altebainawi, A.F.; Alfaraj, L.A.; Alharbi, A.A.; Alkhuraisi, F.F.; Alshammari, T.M. Association between proton pump inhibitors and rhabdomyolysis risk: A post-marketing surveillance using FDA adverse event reporting system (FAERS) database. Ther. Adv. Drug Saf. 2023, 14, 20420986231154075. [Google Scholar] [CrossRef]
- Kass-Hout, T.A.; Xu, Z.; Mohebbi, M.; Nelsen, H.; Baker, A.; Levine, J.; Johanson, E.; Bright, R.A. OpenFDA: An innovative platform providing access to a wealth of FDA’s publicly available data. J. Am. Med. Inform. Assoc. 2016, 23, 596–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, P.; Pan, X.; Liu, R.; Qu, Y.; Xie, L.; Xie, J.; Cao, L.; Chen, Y. Ocular adverse events associated with anti-VEGF therapy: A pharmacovigilance study of the FDA adverse event reporting system (FAERS). Front. Pharmacol. 2022, 13, 1017889. [Google Scholar] [CrossRef] [PubMed]
- Mozzicato, P. Standardised MedDRA queries: Their role in signal detection. Drug. Saf. 2007, 30, 617–619. [Google Scholar] [CrossRef] [PubMed]
- Farooq, P.D.; Urrunaga, N.H.; Tang, D.M.; von Rosenvinge, E.C. Pseudomembranous colitis. Dis. Mon. 2015, 61, 181–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakaeda, T.; Tamon, A.; Kadoyama, K.; Okuno, Y. Data mining of the public version of the FDA Adverse Event Reporting System. Int. J. Med. Sci. 2013, 10, 796–803. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Lin, W.; Yang, J.; Weng, L. Differences in Hypersensitivity Reactions to Iodinated Contrast Media: Analysis of the FDA Adverse Event Reporting System Database (FAERS). J. Allergy Clin. Immunol. Pract. 2023, 11, 1494–1502.e6. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PT | MedDRA Code |
|---|---|
| Antibiotic associated colitis | 10052815 |
| Clostridium bacteraemia | 10058852 |
| Clostridium colitis | 10058305 |
| Clostridium difficile colitis | 10009657 |
| Clostridium difficile infection | 10054236 |
| Clostridial infection | 10061043 |
| Clostridial sepsis | 10078496 |
| Clostridium test positive | 10070027 |
| Gastroenteritis clostridial | 10017898 |
| Pseudomembranous colitis | 10037128 |
| Medication | Drug of Interest with AE of Interest (a) | Other Drugs with AE of Interest (b) | Drug of Interest with Other AEs (c) | Other Drugs with Other AEs (d) | ROR (95% CI) |
|---|---|---|---|---|---|
| Tetracyclines (J01AA) | |||||
| Doxycycline | 227 | 30,710 | 46,700 | 15,933,262 | 2.52 (2.21–2.87) |
| Tigecycline | 78 | 30,859 | 4193 | 15,975,769 | 9.63 (7.70–12.05) |
| Minocycline | 32 | 30,905 | 12,056 | 15,967,906 | 1.37 (0.97–1.94) |
| Combinations of tetracyclines | 17 | 30,920 | 816 | 15,979,146 | 10.77 (6.66–17.41) |
| Tetracycline | 2 | 30,935 | 371 | 15,979,591 | 2.78 (0.69–11.18) |
| Sarecycline | 1 | 30,936 | 105 | 15,979,857 | 4.92 (0.69–35.25) |
| Amphenicols (J01BA) | |||||
| Chloramphenicol | 1 | 30,936 | 26 | 15,979,936 | 19.87 (2.70–146.41) |
| Penicillins with extended spectrum (J01CA) | |||||
| Amoxicillin | 566 | 30,371 | 57,359 | 15,922,603 | 5.17 (4.76–5.62) |
| Ampicillin | 88 | 30,849 | 6189 | 15,973,773 | 7.36 (5.96–9.09) |
| Beta-lactamase sensitive penicillins (J01CE) | |||||
| Phenoxymethylpenicillin | 10 | 30,927 | 1592 | 15,978,370 | 3.25 (1.74–6.04) |
| Benzylpenicillin | 8 | 30,929 | 1613 | 15,978,349 | 2.56 (1.28–5.13) |
| Benzathine benzylpenicillin | 1 | 30,936 | 559 | 15,979,403 | 0.92 (0.13–6.57) |
| Beta-lactamase resistant penicillins (J01CF) | |||||
| Oxacillin | 10 | 30,927 | 893 | 15,979,069 | 5.79 (3.10–10.79) |
| Nafcillin | 10 | 30,927 | 802 | 15,979,160 | 6.44 (3.45–12.02) |
| Dicloxacillin | 1 | 30,936 | 116 | 15,979,846 | 4.45 (0.62–31.88) |
| Combinations of penicillins, incl. beta-lactamase inhibitors (J01CR) | |||||
| Piperacillin and beta-lactamase inhibitor | 483 | 30,454 | 19,305 | 15,960,657 | 13.11 (11.97–14.36) |
| Amoxicillin and beta-lactamase inhibitor | 326 | 30,611 | 21,834 | 15,958,128 | 7.78 (6.97–8.69) |
| Ampicillin and beta-lactamase inhibitor | 51 | 30,886 | 2129 | 15,977,833 | 12.39 (9.39–16.36) |
| First-generation cephalosporins (J01DB) | |||||
| Cefazolin | 162 | 30,775 | 8401 | 15,971,561 | 10.01 (8.56–11.7) |
| Cefalexin | 150 | 30,787 | 15,184 | 15,964,778 | 5.12 (4.36–6.02) |
| Cefadroxil | 12 | 30,925 | 1293 | 15,978,669 | 4.80 (2.72–8.47) |
| Second-generation cephalosporins (J01DC) | |||||
| Cefuroxime | 311 | 30,626 | 11,920 | 15,968,042 | 13.60 (12.15–15.23) |
| Cefaclor | 34 | 30,903 | 1157 | 15,978,805 | 15.19 (10.80–21.37) |
| Cefprozil | 11 | 30,926 | 609 | 15,979,353 | 9.33 (5.14–16.94) |
| Cefoxitin | 10 | 30,927 | 954 | 15,979,008 | 5.42 (2.90–10.10) |
| Cefotetan | 2 | 30,935 | 101 | 15,979,861 | 10.23 (2.52–41.47) |
| Third-generation cephalosporins (J01DD) | |||||
| Ceftriaxone | 548 | 30,389 | 25,953 | 15,954,009 | 11.09 (10.18–12.07) |
| Ceftazidime | 126 | 30,811 | 5422 | 15,974,540 | 12.05 (10.09–14.38) |
| Cefdinir | 89 | 30,848 | 5739 | 15,974,223 | 8.03 (6.51–9.90) |
| Cefotaxime | 64 | 30,873 | 3257 | 15,976,705 | 10.17 (7.94–13.03) |
| Cefixime | 50 | 30,887 | 1972 | 15,977,990 | 13.12 (9.90–17.37) |
| Cefpodoxime | 26 | 30,911 | 698 | 15,979,264 | 19.26 (13.02–28.49) |
| Ceftazidime and beta-lactamase inhibitor | 1 | 30,936 | 126 | 15,979,836 | 4.10 (0.57–29.33) |
| Fourth-generation cephalosporins (J01DE) | |||||
| Cefepime | 288 | 30,649 | 10,696 | 15,969,266 | 14.03 (12.47–15.78) |
| Monobactams (J01DF) | |||||
| Aztreonam | 42 | 30,895 | 6063 | 15,973,899 | 3.58 (2.64–4.85) |
| Carbapenems (J01DH) | |||||
| Meropenem | 507 | 30,430 | 20,575 | 15,959,387 | 12.92 (11.83–14.12) |
| Ertapenem | 166 | 30,771 | 5163 | 15,974,799 | 16.69 (14.30–19.49) |
| Imipenem and cilastatin | 88 | 30,849 | 3343 | 15,976,619 | 13.63 (11.03–16.85) |
| Other cephalosporins and penems (J01DI) | |||||
| Ceftolozane and beta-lactamase inhibitor | 7 | 30,930 | 749 | 15,979,213 | 4.83 (2.29–10.16) |
| Ceftaroline fosamil | 5 | 30,932 | 501 | 15,979,461 | 5.16 (2.14–12.44) |
| Cefiderocol | 1 | 30,936 | 112 | 15,979,850 | 4.61 (0.64–33.03) |
| Trimethoprim and derivatives (J01EA) | |||||
| Trimethoprim | 165 | 30,772 | 8967 | 15,970,995 | 9.55 (8.18–11.14) |
| Intermediate-acting sulfonamides (J01EC) | |||||
| Sulfadiazine | 4 | 30,933 | 1252 | 15,978,710 | 1.65 (0.62–4.40) |
| Combinations of sulfonamides and trimethoprim, incl. derivatives (J01EE) | |||||
| Sulfamethoxazole and trimethoprim | 470 | 30,467 | 64,143 | 15,915,819 | 3.83 (3.49–4.19) |
| Macrolides (J01FA) | |||||
| Clarithromycin | 300 | 30,637 | 26,676 | 15,953,286 | 5.86 (5.22–6.57) |
| Azithromycin | 178 | 30,759 | 38,046 | 15,941,916 | 2.42 (2.09–2.81) |
| Erythromycin | 118 | 30,819 | 14,595 | 15,965,367 | 4.19 (3.49–5.02) |
| Lincosamides (J01FF) | |||||
| Clindamycin | 823 | 30,114 | 26,769 | 15,953,193 | 16.29 (15.18–17.47) |
| Lincomycin | 7 | 30,930 | 230 | 15,979,732 | 15.72 (7.41–33.36) |
| Streptogramins (J01FG) | |||||
| Quinupristin/dalfopristin | 2 | 30,935 | 102 | 15,979,860 | 10.13 (2.50–41.05) |
| Streptomycins (J01GA) | |||||
| Streptomycin | 4 | 30,933 | 1002 | 15,978,960 | 2.06 (0.77–5.51) |
| Other aminoglycosides (J01GB) | |||||
| Gentamicin | 210 | 30,727 | 12,309 | 15,967,653 | 8.87 (7.73–10.17) |
| Amikacin | 142 | 30,795 | 11,578 | 15,968,384 | 6.36 (5.39–7.51) |
| Tobramycin | 68 | 30,869 | 19,561 | 15,960,401 | 1.80 (1.42–2.28) |
| Fluoroquinolones (J01MA) | |||||
| Ciprofloxacin | 1176 | 29,761 | 77,260 | 15,902,702 | 8.13 (7.67–8.63) |
| Levofloxacin | 536 | 30,401 | 44,317 | 15,935,645 | 6.34 (5.82–6.91) |
| Moxifloxacin | 75 | 30,862 | 11,887 | 15,968,075 | 3.26 (2.60–4.10) |
| Ofloxacin | 39 | 30,898 | 5249 | 15,974,713 | 3.84 (2.80–5.26) |
| Gatifloxacin | 33 | 30,904 | 1570 | 15,978,392 | 10.87 (7.70–15.34) |
| Delafloxacin | 1 | 30,936 | 218 | 15,979,744 | 2.37 (0.33–16.9) |
| Glycopeptide antibacterials (J01XA) | |||||
| Vancomycin | 1793 | 29,144 | 46,032 | 15,933,930 | 21.30 (20.29–22.36) |
| Dalbavancin | 2 | 30,935 | 556 | 15,979,406 | 1.86 (0.46–7.45) |
| Telavancin | 1 | 30,936 | 116 | 15,979,846 | 4.45 (0.62–31.88) |
| Oritavancin | 1 | 30,936 | 791 | 15,979,171 | 0.65 (0.09–4.64) |
| Polymyxins (J01XB) | |||||
| Polymyxin B | 14 | 30,923 | 975 | 15,978,987 | 7.42 (4.38–12.58) |
| Colistin | 9 | 30,928 | 958 | 15,979,004 | 4.85 (2.52–9.36) |
| Imidazole derivatives (J01XD) | |||||
| Metronidazole | 2004 | 28,933 | 49,926 | 15,930,036 | 22.10 (21.10–23.14) |
| Tinidazole | 6 | 30,931 | 355 | 15,979,607 | 8.73 (3.90–19.57) |
| Nitrofuran derivatives (J01XE) | |||||
| Nitrofurantoin | 15 | 30,922 | 2636 | 15,977,326 | 2.94 (1.77–4.88) |
| Other antibacterials (J01XX) | |||||
| Linezolid | 168 | 30,769 | 20,272 | 15,959,690 | 4.30 (3.69–5.01) |
| Daptomycin | 70 | 30,867 | 11,035 | 15,968,927 | 3.28 (2.59–4.15) |
| Fosfomycin | 9 | 30,928 | 634 | 15,979,328 | 7.33 (3.80–14.16) |
| Tedizolid | 3 | 30,934 | 499 | 15,979,463 | 3.11 (1.00–9.66) |
| Target PT | Drug of Interest with AE of Interest (a) | Other Drugs with AE of Interest (b) | Drug of Interest with Other AEs (c) | Other Drugs with Other AEs (d) | ROR (95% CI) |
|---|---|---|---|---|---|
| Antibiotic associated colitis | 3 | 20 | 51,927 | 15,958,949 | 46.10 (13.70–155.14) |
| Clostridium bacteraemia | 10 | 131 | 51,920 | 15,958,838 | 23.46 (12.33–44.64) |
| Clostridium colitis | 49 | 750 | 51,881 | 15,958,219 | 20.10 (15.05–26.83) |
| Clostridium difficile colitis | 535 | 7710 | 51,395 | 15,951,259 | 21.54 (19.72–23.52) |
| Clostridium difficile infection | 725 | 15,071 | 51,205 | 15,943,898 | 14.98 (13.90–16.15) |
| Clostridial infection | 140 | 2877 | 51,790 | 15,956,092 | 14.99 (12.65–17.77) |
| Clostridial sepsis | 1 | 141 | 51,929 | 15,958,828 | 2.18 (0.30–15.58) |
| Clostridium test positive | 104 | 1296 | 51,826 | 15,957,673 | 24.71 (20.23–30.18) |
| Gastroenteritis clostridial | 4 | 277 | 51,926 | 15,958,692 | 4.44 (1.65–11.91) |
| Pseudomembranous colitis | 140 | 1778 | 51,790 | 15,957,191 | 24.26 (20.42–28.82) |
| SMQ level | 1863 | 29,074 | 50,067 | 15,929,895 | 20.39 (19.44–21.38) |
| Target PT | Drug of Interest with AE of Interest (a) | Other Drugs with AE of Interest (b) | Drug of Interest with Other AEs (c) | Other Drugs with Other AEs (d) | ROR (95% CI) |
|---|---|---|---|---|---|
| Clostridium bacteraemia | 10 | 131 | 47,815 | 15,962,943 | 25.48 (13.40–48.48) |
| Clostridium colitis | 47 | 752 | 47,778 | 15,962,322 | 20.88 (15.55–28.04) |
| Clostridium difficile colitis | 434 | 7811 | 47,391 | 15,955,263 | 18.71 (16.98–20.61) |
| Clostridium difficile infection | 759 | 15,037 | 47,066 | 15,948,037 | 17.10 (15.89–18.41) |
| Clostridial infection | 98 | 2919 | 47,727 | 15,960,155 | 11.23 (9.18–13.73) |
| Clostridial sepsis | 8 | 134 | 47,817 | 15,962,940 | 19.93 (9.77–40.68) |
| Clostridium test positive | 100 | 1300 | 47,725 | 15,961,774 | 25.73 (20.99–31.54) |
| Gastroenteritis clostridial | 9 | 272 | 47,816 | 15,962,802 | 11.05 (5.69–21.46) |
| Pseudomembranous colitis | 136 | 1782 | 47,689 | 15,961,292 | 25.54 (21.45–30.42) |
| SMQ level | 1503 | 29,434 | 46,322 | 15,933,640 | 17.56 (16.66–18.51) |
| Drug of Interest | Other Drugs | Total | |
|---|---|---|---|
| AE of interest | a | b | a + b |
| Other AEs | c | d | c + d |
| Total | a + c | b + d | a + b + c + d |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Song, Y.; Bai, Z.; Xi, X.; Liu, F.; Zhang, Y.; Qin, C.; Du, D.; Du, Q.; Liu, S. Real-World Data in Pharmacovigilance Database Provides a New Perspective for Understanding the Risk of Clostridium difficile Infection Associated with Antibacterial Drug Exposure. Antibiotics 2023, 12, 1109. https://doi.org/10.3390/antibiotics12071109
Li D, Song Y, Bai Z, Xi X, Liu F, Zhang Y, Qin C, Du D, Du Q, Liu S. Real-World Data in Pharmacovigilance Database Provides a New Perspective for Understanding the Risk of Clostridium difficile Infection Associated with Antibacterial Drug Exposure. Antibiotics. 2023; 12(7):1109. https://doi.org/10.3390/antibiotics12071109
Chicago/Turabian StyleLi, Dongxuan, Yi Song, Zhanfeng Bai, Xin Xi, Feng Liu, Yang Zhang, Chunmeng Qin, Dan Du, Qian Du, and Songqing Liu. 2023. "Real-World Data in Pharmacovigilance Database Provides a New Perspective for Understanding the Risk of Clostridium difficile Infection Associated with Antibacterial Drug Exposure" Antibiotics 12, no. 7: 1109. https://doi.org/10.3390/antibiotics12071109
APA StyleLi, D., Song, Y., Bai, Z., Xi, X., Liu, F., Zhang, Y., Qin, C., Du, D., Du, Q., & Liu, S. (2023). Real-World Data in Pharmacovigilance Database Provides a New Perspective for Understanding the Risk of Clostridium difficile Infection Associated with Antibacterial Drug Exposure. Antibiotics, 12(7), 1109. https://doi.org/10.3390/antibiotics12071109