



Antibiotic Treatment for Lower Respiratory Tract Infections in Primary Care: A Register-Based Study Examining the Role of Radiographic Imaging


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Data Extraction
2.3. Statistical Methods
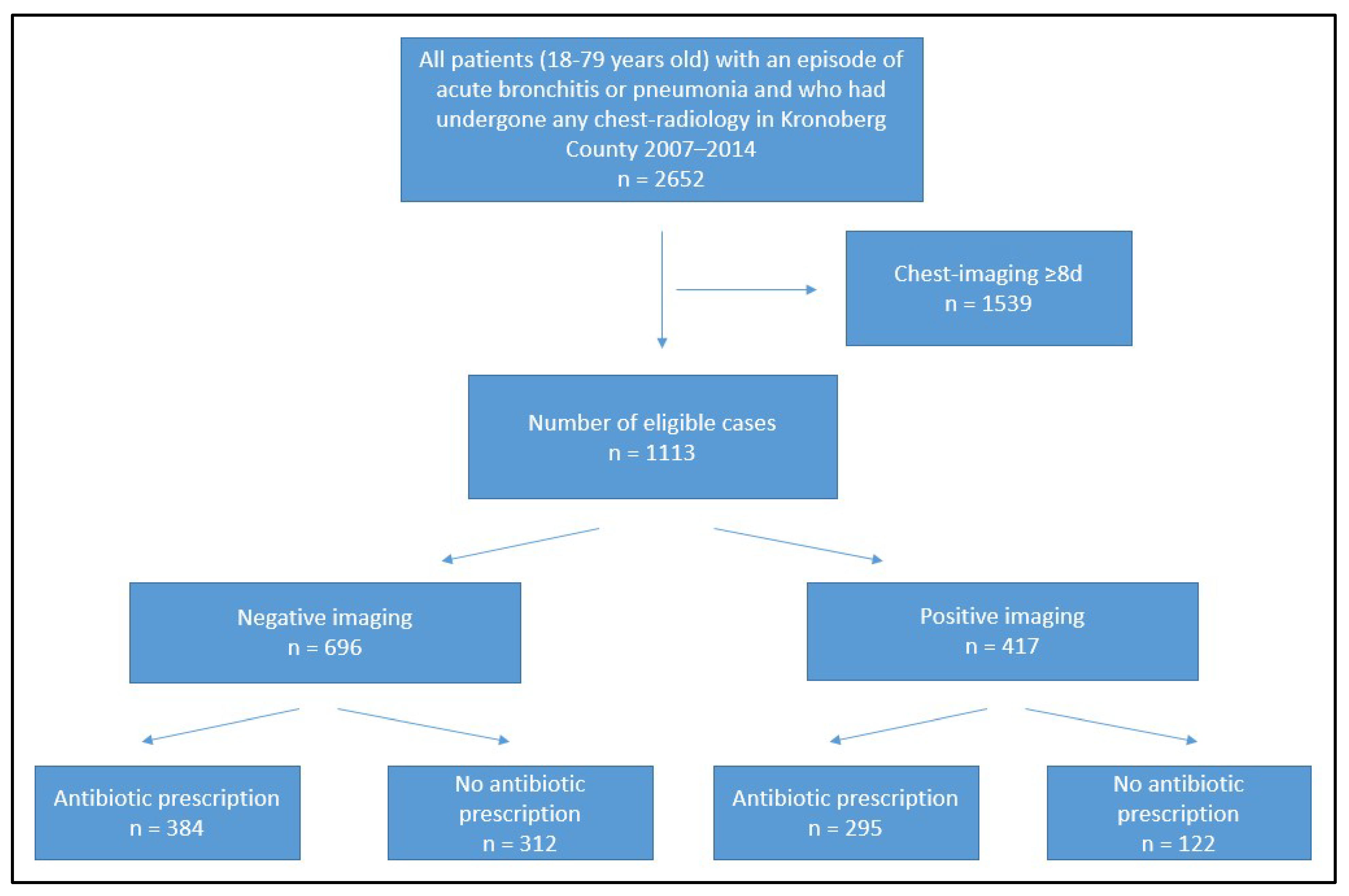
3. Results
3.1. General Characteristics
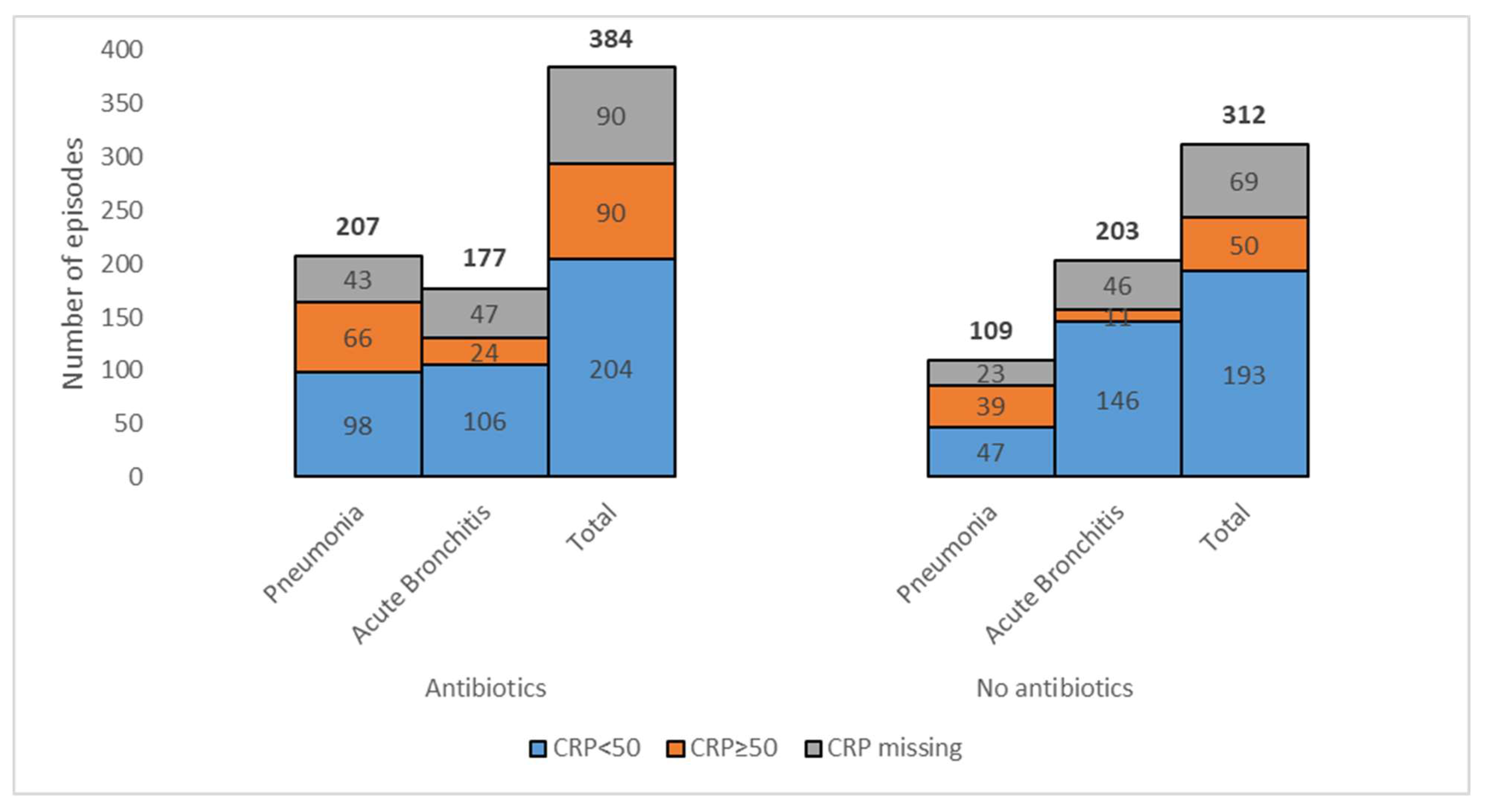
3.2. Antibiotic Prescribing in Cases with Negative Imaging
3.3. All cases with Antibiotic Prescribing
4. Discussion
4.1. Summary
4.2. Strengths and Limitations
4.3. Comparison with Existing Literature
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hak, E.; Rovers, M.M.; Kuyvenhoven, M.M.; Schellevis, F.G.; Verheij, T.J. Incidence of GP-diagnosed respiratory tract infections according to age, gender and high-risk co-morbidity: The Second Dutch National Survey of General Practice. Fam. Pract. 2006, 23, 291–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodhead, M.; Blasi, F.; Ewig, S.; Garau, J.; Huchon, G.; Ieven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; van der Heijden, G.; et al. Guidelines for the management of adult lower respiratory tract infections—Full version. Clin. Microbiol. Infect. 2011, 17 (Suppl. 6), E1–E59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedlund, J.; Holmberg, H.; Mölstad, S. Pneumoni hos vuxna i öppenvård. Inf. Från Läkemedelsverket 2008, 19, 27–32. [Google Scholar]
- Groeneveld, G.H.; van’t Wout, J.W.; Aarts, N.J.; van Rooden, C.J.; Verheij, T.J.M.; Cobbaert, C.M.; Kuijper, E.J.; de Vries, J.J.C.; van Dissel, J.T. Prediction model for pneumonia in primary care patients with an acute respiratory tract infection: Role of symptoms, signs, and biomarkers. BMC Infect. Dis. 2019, 19, 976. [Google Scholar] [CrossRef]
- Strama—The Swedish Strategic Programme Against Antibiotic Resistance. Available online: https://strama.se/?lang=en (accessed on 3 July 2023).
- WHO. Interagency Coordination Group on Antimicrobial Resistance (IACG) Report: No Time to Wait: Securing the Future from Drug-Resistant Infections. 2019. Available online: https://www.who.int/publications/i/item/no-time-to-wait-securing-the-future-from-drug-resistant-infections (accessed on 9 May 2023).
- Groenveld, G.H.; van de Peppel, R.J.; de Waal, M.W.M.; Verheij, T.J.M.; van Dissel, J.T. Clinical factors, C-reactive protein point of care test and chest X-ray in patients with pneumonia: A survey in primary care. Eur. J. Gen. Pract. 2019, 25, 229–235. [Google Scholar] [CrossRef]
- van Vugt, S.F.; Broekhuizen, B.D.L.; Lammens, C.; Zuithoff, N.P.; de Jong, P.A.; Coenen, S.; Ieven, M.; Butler, C.C.; Goossens, H.; Little, P.; et al. Use of serum C reactive protein and procalcitonin concentrations in addition to symptoms and signs to predict pneumonia in patients presenting to primary care with acute cough: Diagnostic study. Prim. Care Respir. J. 2013, 22, 454–458. [Google Scholar] [CrossRef] [Green Version]
- Htun, T.P.; Sun, Y.; Chua, H.L.; Pang, J. Clinical features for diagnosis of pneumonia among adults in primary care setting: A systematic and meta-review. Sci. Rep. 2019, 9, 7600. [Google Scholar] [CrossRef] [Green Version]
- Graffelman, A.W.; le Cessie, S.; Knuistingh Neven, A.; Wilemssen, F.E.; Zonderland, H.M.; van den Broek, P.J. Can history and exam alone reliably predict pneumonia? J. Fam. Pract. 2007, 56, 465–470. [Google Scholar]
- Moore, M.; Stuart, B.; Little, P.; Smith, S.; Thompson, M.J.; Knox, K.; van den Bruel, A.; Lown, M.; Mant, D. Predictors of pneumonia in lower respiratory tract infections: 3C prospective cough complication cohort study. Eur. Resp. J. 2017, 50, 1700434. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, J.G.; Dowell, S.F.; Mandell, L.A.; File, T.M., Jr.; Musher, D.M.; Fine, M.J. Practice guidelines for the management of community-aquired pneumonia in adults. Infectious Diseases Society of America. Clin. Infect. Dis. 2000, 31, 347–382. [Google Scholar] [CrossRef] [Green Version]
- Moberg, A.B.; Kling, M.; Paues, J.; Fransson, S.G.; Falk, M. Use of chest X-ray in the assessment of community acquired pneumonia in primary care—An intervention study. Scand. J. Prim. Health Care 2020, 38, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Blaeuer, S.R.; Bally, K.; Tschudi, P.; Martina, B.; Zeller, A. Acute cough illness in general practice—Predictive value of clinical judgement and accuracy of requesting chest X-rays. Praxis 2013, 102, 1287–1292. [Google Scholar] [CrossRef] [PubMed]
- Cronberg, O.; Tyrstrup, M.; Ekblom, K.; Hedin, K. Diagnosis-linked antibiotic prescribing in Swedish primary care—A comparison between in-hours and out-of-hours. BMC Infect. Dis. 2020, 20, 616. [Google Scholar] [CrossRef] [PubMed]
- Moberg, A.B.; Cronberg, O.; Falk, M.; Hedin, K. Change in the use of diagnostic tests in the management of lower respiratory tract infections: A register-based study in primary care. BJGP Open 2020, 4, bjgpopen20X101015. [Google Scholar] [CrossRef] [Green Version]
- Steurer, J.; Held, U.; Spaar, A.; Bausch, B.; Zoller, M.; Hunziker, R.; Bachmann, L.M. A decision aid to rule out pneumonia and reduce unnecessary prescriptions of antibiotics in primary care patients with cough and fever. BMC Med. 2011, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Little, P.; Francis, N.A.; Stuart, B.; O’Reilly, G.; Thompson, N.; Becque, T.; Hay, A.D.; Wang, K.; Sharland, M.; Harnden, A.; et al. Antibiotics for lower respiratory tract infection in children presenting in primary care in England (ARTIC PC): A double-blind, randomised, placebo-controlled trial. Lancet 2021, 398, 1417–1426. [Google Scholar] [CrossRef]
- Hagaman, J.T.; Rouan, G.W.; Shipley, R.T.; Panos, R.J. Admission chest radiograph lacks sensitivity in the diagnosis of community-aquired pneumonia. Am. J. Med. Sci. 2009, 337, 236–240. [Google Scholar] [CrossRef]
- Butler, C.C.; Hood, K.; Verheij, T.; Little, P.; Melbye, H.; Nuttall, J.; Kelly, M.J.; Mölstad, S.; Godycki-Cwirko, M.; Almirall, J.; et al. Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: Prospective study in 13 countries. BMJ 2009, 338, b2242. [Google Scholar] [CrossRef] [Green Version]
- Lagerstöm, F.; Bader, M.; Foldevi, M.; Fredlund, H.; Nordin-Olsson, I.; Holmberg, H. Microbiological etiology in clinically diagnosed community-acquired pneumonia in primary care in Örebro, Sweden. Clin. Microbiol. Infect. 2003, 9, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Rögnvaldsson, K.G.; Bjarnason, A.; Ólafsdóttir, I.S.; Helgason, K.O.; Guðmundsson, A.; Gottfreðsson, M. Adults with symptoms of pneumonia: A prospective comparison of patients with and without infiltrates on chest radiography. Clin. Microbiol. Infect. 2023, 29, e1–e108. [Google Scholar] [CrossRef]
- Moberg, A.B.; Taléus, U.; Garvin, P.; Fransson, S.G.; Falk, M. Community-acquired pneumonia in primary care: Clinical assessment and the usability of chest radiography. Scand. J. Prim. Health Care 2016, 34, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Stolz, D.; Christ-Crain, M.; Gencay, M.M.; Bingisser, R.; Huber, P.R.; Müller, B.; Tamm, M. Diagnostic value of signs, symptoms and laboratory values in lower respiratory tract infection. Swiss Med. Wkly. 2006, 136, 434–440. [Google Scholar]
- Melbye, H.; Straume, B.; Aasebø, U.; Brox, J. The diagnosis of adult pneumonia in general practice, the diagnostic value of history, physical examination and some blood tests. Scand. J. Prim. Health Care 1988, 6, 111–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akkerman, A.E.; Kuyvenhoven, M.M.; van der Wouden, J.C.; Verheij, T.J. Prescribing antibiotics for respiratory tract infetions by GPs: Management and prescriber characteristics. Br. J. Gen. Pract. 2005, 55, 114–118. [Google Scholar] [PubMed]
- Strandberg, E.L.; Brorsson, A.; André, M.; Gröndal, H.; Mölstad, S.; Hedin, K. Interacting factors associated with low antibiotic prescribing for respiratory tract infections in primary health care—A mixed methods study in Sweden. BMC Fam. Pract. 2016, 17, 78. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, J.M.; Jelinski, S.; Hefferton, D.; Desaulniers, G.; Parfrey, P.S. Role of diagnostic labelling in antibiotic prescription. Can. Fam. Physician 2001, 47, 1217–1224. [Google Scholar]
- Gjelstad, S.; Dalen, I.; Lindbæk, M. GPs’ antibiotic prescription patterns for respiratory tract infections—Still room for improvement. Scan. J. Prim. Health Care 2009, 27, 208–215. [Google Scholar] [CrossRef] [Green Version]
- Boiko, O.; Burgess, C.; Fox, R.; Ashworth, M.; Gulliford, M.C. Risks of use and non-use of antibiotics in primary care: Qualitative study of prescribers’ views. BMJ Open 2020, 10, e038851. [Google Scholar] [CrossRef]
- Björkman, I.; Berg, J.; Viberg, N.; Stålsby Lundborg, C. Awareness of antibiotic resistance and antibiotic prescribing in UTI treatment: A qualitative study among primary care physicians in Sweden. Scan. J. Prim. Health Care 2013, 31, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Sydenham, R.V.; Jarbøl, D.E.; Hansen, M.P.; Justesen, U.S.; Watson, V.; Pedersen, L.B. Prescribing antibiotics: Factors driving decision-making in general practice. A discrete choice experiment. Soc. Sci. Med. 2022, 305, 115033. [Google Scholar] [CrossRef]
- Lum, E.P.; Page, K.; Whitty, J.A.; Doust, J.; Graves, N. Antibiotic prescribing in primary healthcare: Dominant factors and trade-offs in decision-making. Infect. Dis. Health 2018, 23, 74–86. [Google Scholar] [CrossRef] [Green Version]
- Bel Haj Ali, K.; Sekma, A.; Messous, S.; Trabelsi, I.; Ben Youssef, J.; Maghraoui, H.; Razgallah, R.; Walha, A.; Grissa, M.H.; Beltaief, K.; et al. Appropriateness of antibiotic treatment of acute respiratory tract infections in Tunisian primary care and emergency departments: A multicenter cross-sectional study. BMC Prim. Care 2022, 23, 295. [Google Scholar] [CrossRef] [PubMed]
- Shively, N.R.; Buehrle, D.J.; Clancy, C.J.; Decker, B.K. Prevalence of inappropriate antibiotic prescribing in primary care clinics within a veterans affairs health care system. Antimicrob. Agents Chemother. 2018, 62, e00337-18. [Google Scholar] [CrossRef] [Green Version]
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M., Jr.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiessen, K.; Lloyd, A.E.; Miller, M.J.; Homco, J.; Gildon, B.; O’Neal, K.S. Assessing guideline-concordant prescribing for community-acquired pneumonia. Inf. J. Clin. Pharm. 2017, 39, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Almatar, M.A.; Peterson, G.M.; Thompson, A.; McKenzie, D.S.; Anderson, T.L. Community-acquired pneumonia: Why aren’t national antibiotic guidelines followed? Int. J. Clin. Pract. 2015, 69, 259–266. [Google Scholar] [CrossRef]
- Pallon, J.; Sundqvist, M.; Rööst, M.; Hedin, K. Association between bacterial finding, antibiotic treatment and clinical course in patients with pharyngotonsillitis: A registry-based study in primary healthcare in Sweden. BMC Infect. Dis. 2021, 21, 779. [Google Scholar] [CrossRef]
- Little, P.; Gould, C.; Williamson, I.; Warner, G.; Gantley, M.; Kinmonth, A.L. Reattendance and complications in a randomised trial of prescribing strategies for sore throat: The medicalising effect of prescribing antibiotics. BMJ 1997, 315, 350–352. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total (n = 1113) | Negative Imaging (n = 696) | Positive Imaging (n = 417) | p Value | |
|---|---|---|---|---|
| Age (years), median (IQR) | 58 (42;67) | 59 (43;67) | 57 (41;68) | 0.53 a |
| Men, n (%) | 563 (51) | 349 (50) | 214 (51) | 0.70 |
| Co-morbidity, n (%) | 493 (44) | 335 (48) | 158 (38) | <0.001 |
| CRP mg/L, median (IQR) | 30 (10;103) | 13 (10;53) | 79 (33;160) | <0.001 a |
| Antibiotics, n (%) | 679 (61) | 384 (55) | 295 (71) | <0.001 |
| PcV, n (%) | 195 (20) | 90 (13) | 105 (25) | <0.001 |
| Diagnosis of pneumonia, n (%) | 685 (62) | 316 (45) | 369 (89) | <0.001 |
| Antibiotic Prescribed (n = 384) | No Antibiotic Prescribed (n = 312) | p Value | |
|---|---|---|---|
| Age (years), median (IQR) | 58 (43;67) | 59 (43;67) | 0.89 a |
| Age ≥ 65 years, n | 124 | 107 | 0.58 |
| Men, n (%) | 199 (52) | 150 (48) | 0.33 |
| Co-morbidity, n (%) | 184 (48) | 151 (48) | 0.90 |
| CRP mg/L, median (IQR) | 21 (10;60) | 10 (10;37) | <0.001 a |
| CRP > 50 mg/L, n (%) | 90 (64) | 50 (36) | <0.05 |
| Physician’s level of competence, n (%) | <0.001 | ||
| Specialist | 229 (50) | 228 (50) | |
| Resident physician | 121 (67) | 59 (33) | |
| Intern | 34 (58) | 25 (42) |
| Negative Imaging (n = 384) | Positive Imaging (n = 295) | p Value | |
|---|---|---|---|
| Age (years), median (IQR) | 58 (43;67) | 55 (37;67) | 0.13 |
| Men, n (%) | 199 (52) | 156 (53) | 0.79 |
| Co-morbidity, n (%) | 184 (48) | 108 (37) | <0.05 |
| CRP mg/L, median (IQR) | 21 (10;60) | 72 (30;148) | <0.001 a |
| First-line antibiotics, n (%) | 90 (23) | 105 (36) | <0.001 |
| Diagnosis of pneumonia, n (%) | 207 (54) | 261 (89) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlsson, S.; Hedin, K.; Cronberg, O.; Moberg, A. Antibiotic Treatment for Lower Respiratory Tract Infections in Primary Care: A Register-Based Study Examining the Role of Radiographic Imaging. Antibiotics 2023, 12, 1165. https://doi.org/10.3390/antibiotics12071165
Carlsson S, Hedin K, Cronberg O, Moberg A. Antibiotic Treatment for Lower Respiratory Tract Infections in Primary Care: A Register-Based Study Examining the Role of Radiographic Imaging. Antibiotics. 2023; 12(7):1165. https://doi.org/10.3390/antibiotics12071165
Chicago/Turabian StyleCarlsson, Sara, Katarina Hedin, Olof Cronberg, and Anna Moberg. 2023. "Antibiotic Treatment for Lower Respiratory Tract Infections in Primary Care: A Register-Based Study Examining the Role of Radiographic Imaging" Antibiotics 12, no. 7: 1165. https://doi.org/10.3390/antibiotics12071165
APA StyleCarlsson, S., Hedin, K., Cronberg, O., & Moberg, A. (2023). Antibiotic Treatment for Lower Respiratory Tract Infections in Primary Care: A Register-Based Study Examining the Role of Radiographic Imaging. Antibiotics, 12(7), 1165. https://doi.org/10.3390/antibiotics12071165