
Moving toward Extensively Drug-Resistant: Four-Year Antimicrobial Resistance Trends of Acinetobacter baumannii from the Largest Department of Internal Medicine in Slovakia



Abstract
:1. Introduction
2. Results
2.1. Patients Characteristics and Demographic Data
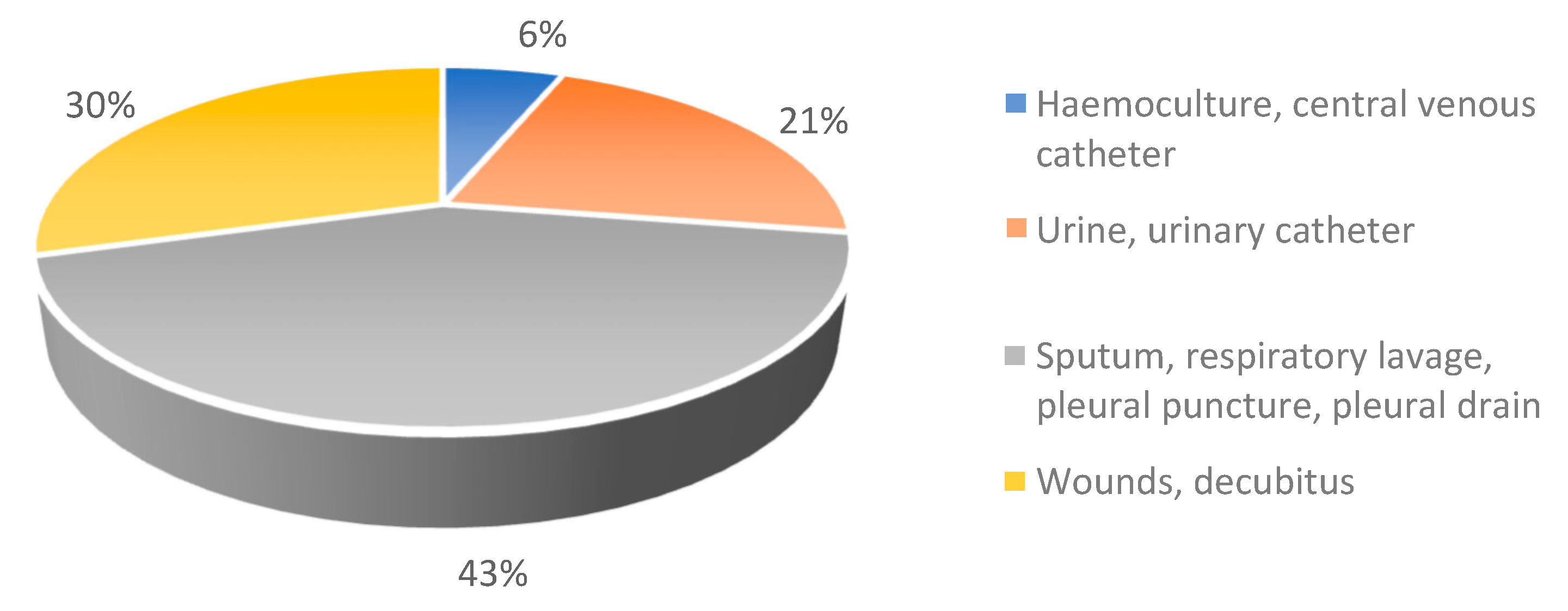
2.2. Distribution of Samples’ Isolation
2.3. Demographic Data and Prevalence of Carbapenem Resistant Isolates
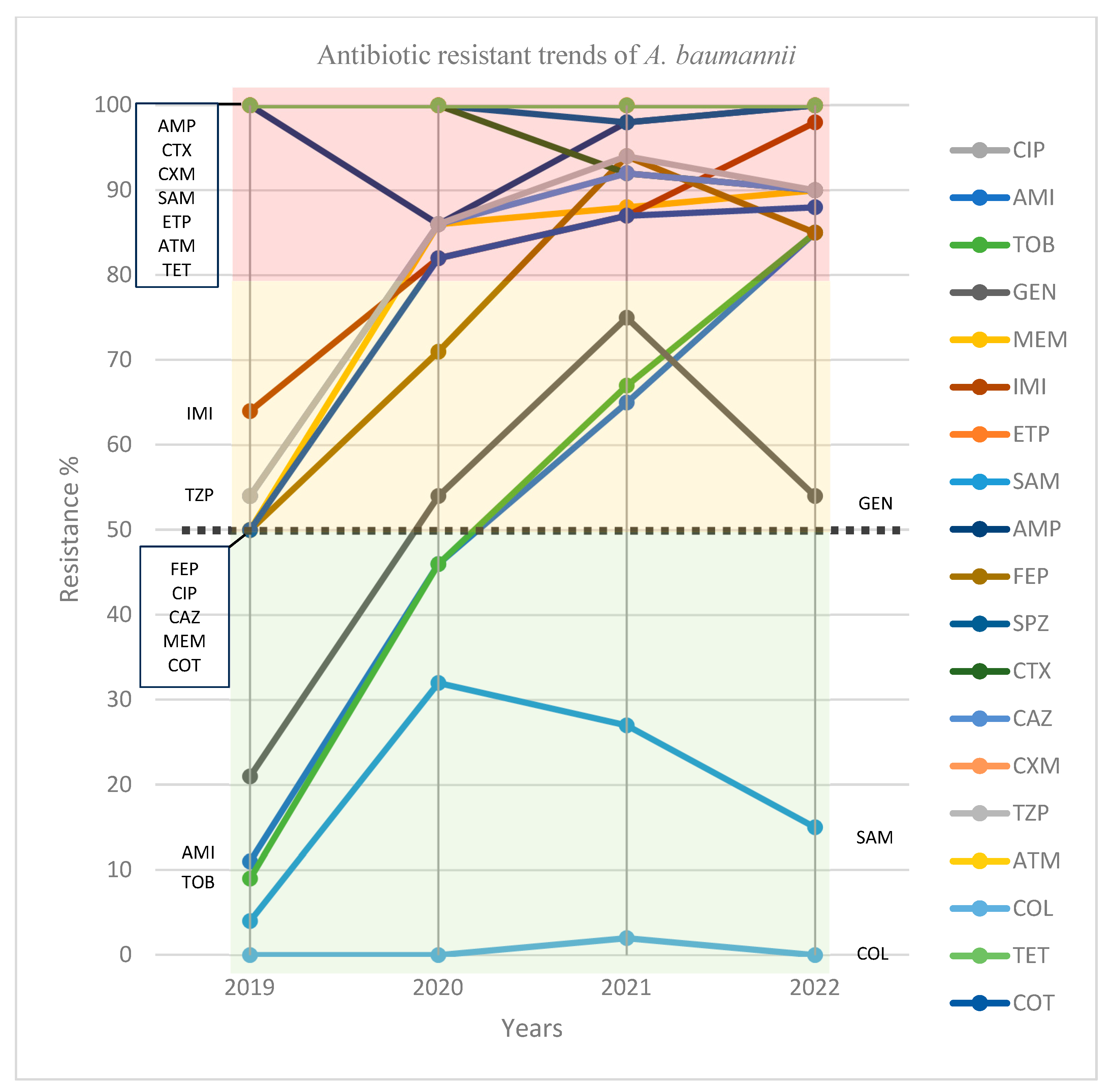
2.4. Trends of Antibiotic Resistance
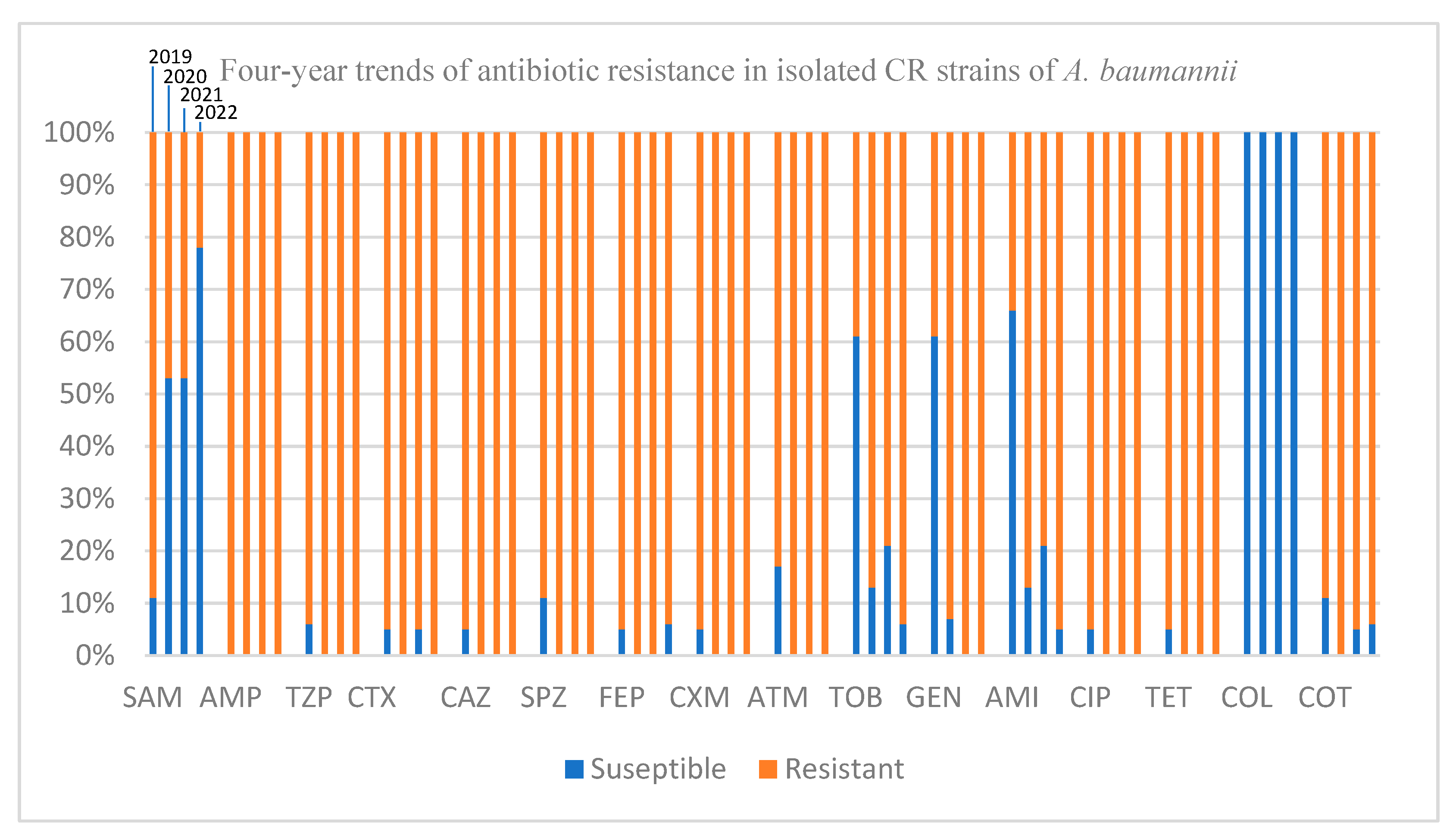
2.5. Trends of Antibiotic Resistance among CR Isolates
3. Discussion
4. Materials and Methods
4.1. Healthcare Facilities, Patients, and Specimens
4.2. Isolation and Proof of Bacterial Strains
4.3. Statistical Analysis
4.4. Ethical Consent
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ma, C.; McClean, S. Mapping Global Prevalence of Acinetobacter baumannii and Recent Vaccine Development to Tackle It. Vaccines 2021, 9, 570. [Google Scholar] [CrossRef]
- Almasaudi, S.B. Acinetobacter spp. as nosocomial pathogens: Epidemiology and resistance features. Saudi J. Biol. Sci. 2018, 25, 586–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fournier, P.E.; Richet, H.; Weinstein, R.A. The Epidemiology and Control of Acinetobacter baumannii in Health Care Facilities. Clin. Infect. Dis. 2006, 42, 692–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yashar, J.; Monika, J.; Juraj, P. Acinetobacter baumannii: Emergence of a Superbug, Past, Present, and Future. In The Global Antimicrobial Resistance Epidemic; Guillermo, T.-I., Ed.; IntechOpen: Rijeka, Croatia, 2022; Chapter 13. [Google Scholar]
- Ko, S.-Y.; Kim, N.; Park, S.-Y.; Kim, S.-Y.; Shin, M.; Lee, J.-C. Acinetobacter baumannii under Acidic Conditions Induces Colistin Resistance through PmrAB Activation and Lipid A Modification. Antibiotics 2023, 12, 813. [Google Scholar] [CrossRef] [PubMed]
- Nasr, P. Genetics, epidemiology, and clinical manifestations of multidrug-resistant Acinetobacter baumannii. J. Hosp. Infect. 2020, 104, 4–11. [Google Scholar] [CrossRef]
- Vázquez-López, R.; Solano-Gálvez, S.G.; Juárez Vignon-Whaley, J.J.; Abello Vaamonde, J.A.; Padró Alonzo, L.A.; Rivera Reséndiz, A.; Muleiro Álvarez, M.; Vega López, E.N.; Franyuti-Kelly, G.; Álvarez-Hernández, D.A.; et al. Acinetobacter baumannii Resistance: A Real Challenge for Clinicians. Antibiotics 2020, 9, 205. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Surveillance Atlas of Infectious Diseases; ECDC: Solna, Sweden, 2021.
- Novović, K.; Jovčić, B. Colistin Resistance in Acinetobacter baumannii: Molecular Mechanisms and Epidemiology. Antibiotics 2023, 12, 516. [Google Scholar] [CrossRef]
- Arefian, H.; Hagel, S.; Fischer, D.; Scherag, A.; Brunkhorst, F.M.; Maschmann, J.; Hartmann, M. Estimating extra length of stay due to healthcare-associated infections before and after implementation of a hospital-wide infection control program. PLoS ONE 2019, 14, e0217159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, J.; Upfill-Brown, A.; Dann, A.M.; Kim, S.S.; Girgis, M.D.; King, J.C.; Donahue, T.R. Association of Hospital Length of Stay and Complications With Readmission After Open Pancreaticoduodenectomy. JAMA Surg. 2019, 154, 88–90. [Google Scholar] [CrossRef] [Green Version]
- Sulzgruber, P.; Schnaubelt, S.; Koller, L.; Laufer, G.; Pilz, A.; Kazem, N.; Winter, M.-P.; Steinlechner, B.; Andreas, M.; Fleck, T.; et al. An Extended Duration of the Pre-Operative Hospitalization is Associated with an Increased Risk of Healthcare-Associated Infections after Cardiac Surgery. Sci. Rep. 2020, 10, 8006. [Google Scholar] [CrossRef] [PubMed]
- Jalali, Y.; Sturdik, I.; Jalali, M.; Payer, J. Isolated carbapenem resistant bacteria, their multidrug resistant profile, percentage of healthcare associated infection and associated mortality, in hospitalized patients in a University Hospital in Bratislava. Bratisl. Lek. Listy 2021, 122, 379–385. [Google Scholar] [CrossRef]
- Beavers, S.F.; Blossom, D.B.; Wiemken, T.L.; Kawaoka, K.Y.; Wong, A.; Goss, L.; McCormick, M.I.; Thoroughman, D.; Srinivasan, A. Comparison of risk factors for recovery of Acinetobacter baumannii during outbreaks at two Kentucky hospitals, 2006. Public Health Rep. 2009, 124, 868–874. [Google Scholar] [CrossRef]
- Sheng, W.-H.; Liao, C.-H.; Lauderdale, T.-L.; Ko, W.-C.; Chen, Y.-S.; Liu, J.-W.; Lau, Y.-J.; Wang, L.-S.; Liu, K.-S.; Tsai, T.-Y.; et al. A multicenter study of risk factors and outcome of hospitalized patients with infections due to carbapenem-resistant Acinetobacter baumannii. Int. J. Infect. Dis. 2010, 14, e764–e769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alrahmany, D.; Omar, A.F.; Alreesi, A.; Harb, G.; Ghazi, I.M. Acinetobacter baumannii Infection-Related Mortality in Hospitalized Patients: Risk Factors and Potential Targets for Clinical and Antimicrobial Stewardship Interventions. Antibiotics 2022, 11, 1086. [Google Scholar] [CrossRef]
- Ellis, D.; Cohen, B.; Liu, J.; Larson, E. Risk factors for hospital-acquired antimicrobial-resistant infection caused by Acinetobacter baumannii. Antimicrob. Resist. Infect. Control 2015, 4, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chusri, S.; Chongsuvivatwong, V.; Silpapojakul, K.; Singkhamanan, K.; Hortiwakul, T.; Charernmak, B.; Doi, Y. Clinical characteristics and outcomes of community and hospital-acquired Acinetobacter baumannii bacteremia. J. Microbiol. Immunol. Infect. 2019, 52, 796–806. [Google Scholar] [CrossRef] [PubMed]
- Mehta, Y.; Gupta, A.; Todi, S.; Myatra, S.; Samaddar, D.P.; Patil, V.; Bhattacharya, P.K.; Ramasubban, S. Guidelines for prevention of hospital acquired infections. Indian J. Crit. Care Med. 2014, 18, 149–163. [Google Scholar] [CrossRef] [Green Version]
- Zanetti, G.; Blanc, D.S.; Federli, I.; Raffoul, W.; Petignat, C.; Maravic, P.; Francioli, P.; Berger, M.M. Importation of Acinetobacter baumannii Into a Burn Unit: A Recurrent Outbreak of Infection Associated With Widespread Environmental Contamination. Infect. Control Hosp. Epidemiol. 2007, 28, 723–725. [Google Scholar] [CrossRef] [Green Version]
- Blanco, N.; Harris, A.D.; Rock, C.; Johnson, J.K.; Pineles, L.; Bonomo, R.A.; Srinivasan, A.; Pettigrew, M.M.; Thom, K.A. Risk Factors and Outcomes Associated with Multidrug-Resistant Acinetobacter baumannii upon Intensive Care Unit Admission. Antimicrob. Agents Chemother. 2018, 62, e01631-17. [Google Scholar] [CrossRef] [Green Version]
- Zeighami, H.; Valadkhani, F.; Shapouri, R.; Samadi, E.; Haghi, F. Virulence characteristics of multidrug resistant biofilm forming Acinetobacter baumannii isolated from intensive care unit patients. BMC Infect. Dis. 2019, 19, 629. [Google Scholar] [CrossRef] [Green Version]
- Ababneh, Q.; Abulaila, S.; Jaradat, Z. Isolation of extensively drug resistant Acinetobacter baumannii from environmental surfaces inside intensive care units. Am. J. Infect. Control 2022, 50, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Ceparano, M.; Baccolini, V.; Migliara, G.; Isonne, C.; Renzi, E.; Tufi, D.; De Vito, C.; De Giusti, M.; Trancassini, M.; Alessandri, F.; et al. Acinetobacter baumannii Isolates from COVID-19 Patients in a Hospital Intensive Care Unit: Molecular Typing and Risk Factors. Microorganisms 2022, 10, 722. [Google Scholar] [CrossRef]
- Sirijatuphat, R.; Thawornkaew, S.; Ruangkriengsin, D.; Thamlikitkul, V. Colistin Monotherapy versus Colistin plus Sitafloxacin for Therapy of Carbapenem-Resistant Acinetobacter baumannii Infections: A Preliminary Study. Antibiotics 2022, 11, 1707. [Google Scholar] [CrossRef] [PubMed]
- Kogilathota Jagirdhar, G.S.; Rama, K.; Reddy, S.T.; Pattnaik, H.; Qasba, R.K.; Elmati, P.R.; Kashyap, R.; Schito, M.; Gupta, N. Efficacy of Cefoperazone Sulbactam in Patients with Acinetobacter Infections: A Systematic Review of the Literature. Antibiotics 2023, 12, 582. [Google Scholar] [CrossRef] [PubMed]
- Ungthammakhun, C.; Vasikasin, V.; Changpradub, D. A Randomized Controlled Trial of Colistin Combined with Sulbactam: 9 g per Day versus 12 g per Day in the Treatment of Extensively Drug-Resistant Acinetobacter baumannii Pneumonia: An Interim Analysis. Antibiotics 2022, 11, 1112. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report for 2021; ECDC: Solna, Sweden, 2021; p. 28.
- European Centre for Disease Prevention and Control. Antimicrobial resistance in the EU/EEA (EARS-Net). In Yearly, 2022th ed.; European Centre for Disease Prevention and Control: Solna, Sweden, 2022; p. 36. [Google Scholar]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Mabrouk, S.S.; Abdellatif, G.R.; El-Ansary, M.R.; Aboshanab, K.M.; Ragab, Y.M. Carbapenemase Producers Among Extensive Drug-Resistant Gram-Negative Pathogens Recovered from Febrile Neutrophilic Patients in Egypt. Infect. Drug Resist. 2020, 13, 3113–3124. [Google Scholar] [CrossRef]
- Naik, P.; Pandey, S.; Gagan, S.; Biswas, S.; Joseph, J. Virulence factors in multidrug (MDR) and Pan-drug resistant (XDR) Pseudomonas aeruginosa: A cross-sectional study of isolates recovered from ocular infections in a high-incidence setting in southern India. J. Ophthalmic Inflamm. Infect. 2021, 11, 36. [Google Scholar] [CrossRef]
- Appaneal, H.J.; Lopes, V.V.; LaPlante, K.L.; Caffrey, A.R. Treatment, Clinical Outcomes, and Predictors of Mortality among a National Cohort of Admitted Patients with Acinetobacter baumannii Infection. Antimicrob. Agents Chemother. 2022, 66, e0197521. [Google Scholar] [CrossRef]
- Wachino, J.I.; Jin, W.; Kimura, K.; Arakawa, Y. Intercellular Transfer of Chromosomal Antimicrobial Resistance Genes between Acinetobacter baumannii Strains Mediated by Prophages. Antimicrob. Agents Chemother. 2019, 63, e00334-19. [Google Scholar] [CrossRef] [Green Version]
- Leungtongkam, U.; Thummeepak, R.; Tasanapak, K.; Sitthisak, S. Acquisition and transfer of antibiotic resistance genes in association with conjugative plasmid or class 1 integrons of Acinetobacter baumannii. PLoS ONE 2018, 13, e0208468. [Google Scholar] [CrossRef] [Green Version]
- Semenec, L.; Cain, A.K.; Dawson, C.J.; Liu, Q.; Dinh, H.; Lott, H.; Penesyan, A.; Maharjan, R.; Short, F.L.; Hassan, K.A.; et al. Cross-protection and cross-feeding between Klebsiella pneumoniae and Acinetobacter baumannii promotes their co-existence. Nat. Commun. 2023, 14, 702. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, S.; John, J.J.; Vasudevan, K.; Mathur, P.; Ray, P.; Neeravi, A.; Baskaran, A.; Kirubananthan, A.; Anandan, S.; Biswas, I.; et al. Genomic rearrangements of mobile genetic elements associated with carbapenem resistance of Acinetobacter baumannii. bioRxiv 2022. [Google Scholar] [CrossRef]
- Wyres, K.L.; Holt, K.E. Klebsiella pneumoniae as a key trafficker of drug resistance genes from environmental to clinically important bacteria. Curr. Opin. Microbiol. 2018, 45, 131–139. [Google Scholar] [CrossRef]
- Lam, M.M.C.; Wick, R.R.; Wyres, K.L.; Gorrie, C.L.; Judd, L.M.; Jenney, A.W.J.; Brisse, S.; Holt, K.E. Genetic diversity, mobilisation and spread of the yersiniabactin-encoding mobile element ICEKp in Klebsiella pneumoniae populations. Microb. Genom. 2018, 4, e000196. [Google Scholar] [CrossRef]
- Koreň, J.; Andrezál, M.; Drahovská, H.; Hubenáková, Z.; Liptáková, A.; Maliar, T. Next-Generation Sequencing of Carbapenem-Resistant Klebsiella pneumoniae Strains Isolated from Patients Hospitalized in the University Hospital Facilities. Antibiotics 2022, 11, 1538. [Google Scholar] [CrossRef] [PubMed]
- Koren, J.; Hubenakova, Z.; Drahovska, H.; Ozaee, E.; Markuskova, B.; Lichvarikova, A. Emergence of extended-spectrum β-lactamase (ESBL) and/or carbapenemase producing Enterobacteriaceae (CPE) and their antimicrobial resistance. Bratisl. Lek. Listy 2019, 120, 935–940. [Google Scholar] [CrossRef]
- Nowak, J.; Zander, E.; Stefanik, D.; Higgins, P.G.; Roca, I.; Vila, J.; McConnell, M.J.; Cisneros, J.M.; Seifert, H.; WP4, M.W.G. High incidence of pandrug-resistant Acinetobacter baumannii isolates collected from patients with ventilator-associated pneumonia in Greece, Italy and Spain as part of the MagicBullet clinical trial. J. Antimicrob. Chemother. 2017, 72, 3277–3282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Chen, I.; Tang, T. Colistin Monotherapy versus Colistin plus Meropenem Combination Therapy for the Treatment of Multidrug-Resistant Acinetobacter baumannii Infection: A Meta-Analysis. J. Clin. Med. 2022, 11, 3239. [Google Scholar] [CrossRef]
- Ayerbe-Algaba, R.; Gil-Marques, M.L.; Jimenez-Mejias, M.E.; Sanchez-Encinales, V.; Parra-Millan, R.; Pachon-Ibanez, M.E.; Pachon, J.; Smani, Y. Synergistic Activity of Niclosamide in Combination With Colistin Against Colistin-Susceptible and Colistin-Resistant Acinetobacter baumannii and Klebsiella pneumoniae. Front. Cell. Infect. Microbiol. 2018, 8, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunalan, A.; Sarumathi, D.; Sastry, A.S.; Ramanathan, V.; Rajaa, S.; Sistla, S. Effect of combined colistin and meropenem against meropenem resistant Acinetobacter baumannii and Pseudomonas aeruginosa by checkerboard method: A cross sectional analytical study. Indian J. Pharmacol. 2021, 53, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Katip, W.; Uitrakul, S.; Oberdorfer, P. A Comparison of Colistin versus Colistin Plus Meropenem for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients: A Propensity Score-Matched Analysis. Antibiotics 2020, 9, 647. [Google Scholar] [CrossRef] [PubMed]
- Kaye, K.S.; Marchaim, D.; Thamlikitkul, V.; Carmeli, Y.; Chiu, C.-H.; Daikos, G.; Dhar, S.; Durante-Mangoni, E.; Gikas, A.; Kotanidou, A.; et al. Colistin Monotherapy versus Combination Therapy for Carbapenem-Resistant Organisms. NEJM Evid. 2023, 2, EVIDoa2200131. [Google Scholar] [CrossRef]
- Peyclit, L.; Baron, S.A.; Rolain, J.M. Drug Repurposing to Fight Colistin and Carbapenem-Resistant Bacteria. Front. Cell. Infect. Microbiol. 2019, 9, 193. [Google Scholar] [CrossRef]
- Sun, W.; Sanderson, P.E.; Zheng, W. Drug combination therapy increases successful drug repositioning. Drug Discov. Today 2016, 21, 1189–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merck. MALDI-MS Analysis of Proteins. 2020. Available online: https://www.sigmaaldrich.com/life-science/proteomics/recombinant-protein-expression/protocols/maldims-analysis-of-proteins.html?gclid=Cj0KCQiAk53-BRD0ARIsAJuNhpvUwYCIMd5NxDbG8_w2Btapg0Mg0Ixf1ueMvjLxZgSP302NkYcR6CQaApLTEALw_wcB (accessed on 20 July 2020).
- EUCAST. Clinical Breakpoints—Breakpoints and Guidance; EUCAST: Copenhagen, Denmark, 2023. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Total | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|
| Number of hospitalised patients | 11,856 | 3618 | 2940 | 2579 | 2719 |
| Number of isolated A. baumannii | 149 | 28 | 28 | 52 | 41 |
| Number of male patients (n/N, cases %) | 85/149, 57% | ||||
| Age of male patients (Mean) | 72.7 (SD ± 18.2) | ||||
| Number of female patients (n/N, cases %) | 64/149, 43% | ||||
| Age of female patients (Mean) | 60.2 (SD ± 20.2) | ||||
| Hospitalisation duration (Av. days) | 25.3 | ||||
| Healthcare-associated infection (n/N) | 126/149 | 17/28 | 24/28 | 48/52 | 37/41 |
| Cases (%) | 85% | 60% | 85% | 92% | 90% |
| Associated mortality rate (n/N) | 61/149 | 11/28 | 12/28 | 23/52 | 15/41 |
| Cases (%) | 40% | 39% | 43% | 44% | 37% |
| Prevalence (P1 %) | 0.8% | 1% | 2% | 1.5% | |
| Number of MDR strains among all isolates (n/N) | 78/149 | 9/28 | 12/28 | 35/52 | 22/41 |
| Cases (%) | 52% | 32% | 43% | 67% | 53% |
| Number of XDR strains among all isolates (n/N) | 50/149 | 9/28 | 12/28 | 14/52 | 15/41 |
| Cases (%) | 33% | 32% | 42% | 26% | 36% |
| Total | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|
| Number of CR strains among all isolates (n/N) | 78/149 | 19/28 | 21/28 | 20/52 | 18/41 |
| Cases (%) | 52% | 68% | 75% | 39% | 44% |
| Prevalence of CR isolates (P2 %) | 0.5% | 0.7% | 0.7% | 0.6% | |
| Healthcare-associated infection among CR isolates (n/N) | 62/78 | 12/19 | 16/21 | 17/20 | 17/18 |
| Cases (%) | 79% | 63% | 76% | 85% | 94% |
| Associated mortality rate among CR isolates (n/N) | 36/78 | 9/19 | 10/21 | 10/20 | 7/18 |
| Cases (%) | 46% | 50% | 48% | 50% | 39% |
| Number of MDR cases among CR isolates (n/N) | 15/78 | 4/19 | 3/21 | 5/20 | 3/18 |
| Cases (%) | 19% | 21% | 14% | 25% | 16% |
| Number of XDR strains among CR isolates (n/N) | 50/78 | 9/19 | 12/21 | 14/20 | 15/18 |
| Cases (%) | 64% | 47% | 57% | 70% | 83% |
| 2019 | 2020 | 2021 | 2022 | R2-p (CL: 95%) | |
|---|---|---|---|---|---|
| ATB | No. R/S (%) | No. R/S (%) | No. R/S (%) | No. R/S (%) | |
| Ampicillin | 28/0 (100%) | 24/4 (86%) | 51/1 (98%) | 41/0 (100%) | - |
| Ampicillin-sulbactam | 1/27 (4%) | 9/23 (32%) | 14/38 (27%) | 6/34 (15%) | - |
| Piperacillin-tazobactam | 15/13 (54%) | 24/4 (86%) | 47/5 (94%) | 37/4 (90%) | 0.67–0.18 |
| Cefotaxime | 28/0 (100%) | 28/0 (100%) | 48/4 (92%) | 37/4 (90%) | - |
| Ceftazidime | 15/13 (54%) | 24/4 (86%) | 48/4 (92%) | 37/4 (90%) | 0.68–0.17 |
| Cefuroxime | 28/0 (100%) | 28/0 (100%) | 52/0 (100%) | 41/0 (100%) | - |
| Cefepime | 14/14 (50%) | 20/8 (71%) | 49/3 (94%) | 35/6 (85%) | 0.74–0.13 |
| Cefoperazone-sulbactam | 28/0 (100%) | 28/0 (100%) | 51/1 (98%) | 41/0 (100%) | - |
| Imipenem | 18/10 (64%) | 23/5 (82%) | 45/7 (87%) | 40/1 (98%) | 0.94–0.02 |
| Meropenem | 14/14 (50%) | 24/4 (86%) | 46/6 (88%) | 37/4 (90%) | 0.68–0.17 |
| Ertapenem | 28/0 (100%) | 28/0 (100%) | 52/0 (100%) | 41/0 (100%) | - |
| Aztreonam | 28/0 (100%) | 28/0 (100%) | 52/0 (100%) | 41/0 (100%) | - |
| Ciprofloxacin | 15/13 (54%) | 24/4 (86%) | 48/4 (92%) | 37/4 (90%) | 0.68–0.17 |
| Amikacin | 3/15 (11%) | 13/15 (46%) | 34/18 (65%) | 356 (85%) | 0.97–0.01 |
| Tobramycin | 3/25 (9%) | 13/15 (46%) | 35/17 (67%) | 35/6 (85%) | 0.96–0.01 |
| Gentamycin | 6/22 (21%) | 15/13 (54%) | 3913 (75%) | 22/19 (54%) | - |
| Tetracycline | 28/0 (100%) | 28/0 (100%) | 52/0 (100%) | 41/0 (100%) | - |
| Trimethoprim sulfamethoxazole | 14/14 (50%) | 23/5 (82%) | 45/7 (87%) | 36/5 (88%) | 0.72–0.14 |
| Colistin | 0/28 (0%) | 0/28 (0%) | 2/49 (4%) | 0/41 (0%) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jalali, Y.; Liptáková, A.; Jalali, M.; Payer, J. Moving toward Extensively Drug-Resistant: Four-Year Antimicrobial Resistance Trends of Acinetobacter baumannii from the Largest Department of Internal Medicine in Slovakia. Antibiotics 2023, 12, 1200. https://doi.org/10.3390/antibiotics12071200
Jalali Y, Liptáková A, Jalali M, Payer J. Moving toward Extensively Drug-Resistant: Four-Year Antimicrobial Resistance Trends of Acinetobacter baumannii from the Largest Department of Internal Medicine in Slovakia. Antibiotics. 2023; 12(7):1200. https://doi.org/10.3390/antibiotics12071200
Chicago/Turabian StyleJalali, Yashar, Adriána Liptáková, Monika Jalali, and Juraj Payer. 2023. "Moving toward Extensively Drug-Resistant: Four-Year Antimicrobial Resistance Trends of Acinetobacter baumannii from the Largest Department of Internal Medicine in Slovakia" Antibiotics 12, no. 7: 1200. https://doi.org/10.3390/antibiotics12071200
APA StyleJalali, Y., Liptáková, A., Jalali, M., & Payer, J. (2023). Moving toward Extensively Drug-Resistant: Four-Year Antimicrobial Resistance Trends of Acinetobacter baumannii from the Largest Department of Internal Medicine in Slovakia. Antibiotics, 12(7), 1200. https://doi.org/10.3390/antibiotics12071200