
A Qualitative Study on the Policy Process and Development of the National Action Plan on Antimicrobial Resistance in Singapore

 , , , , and
, , , , and
Abstract
:1. Introduction

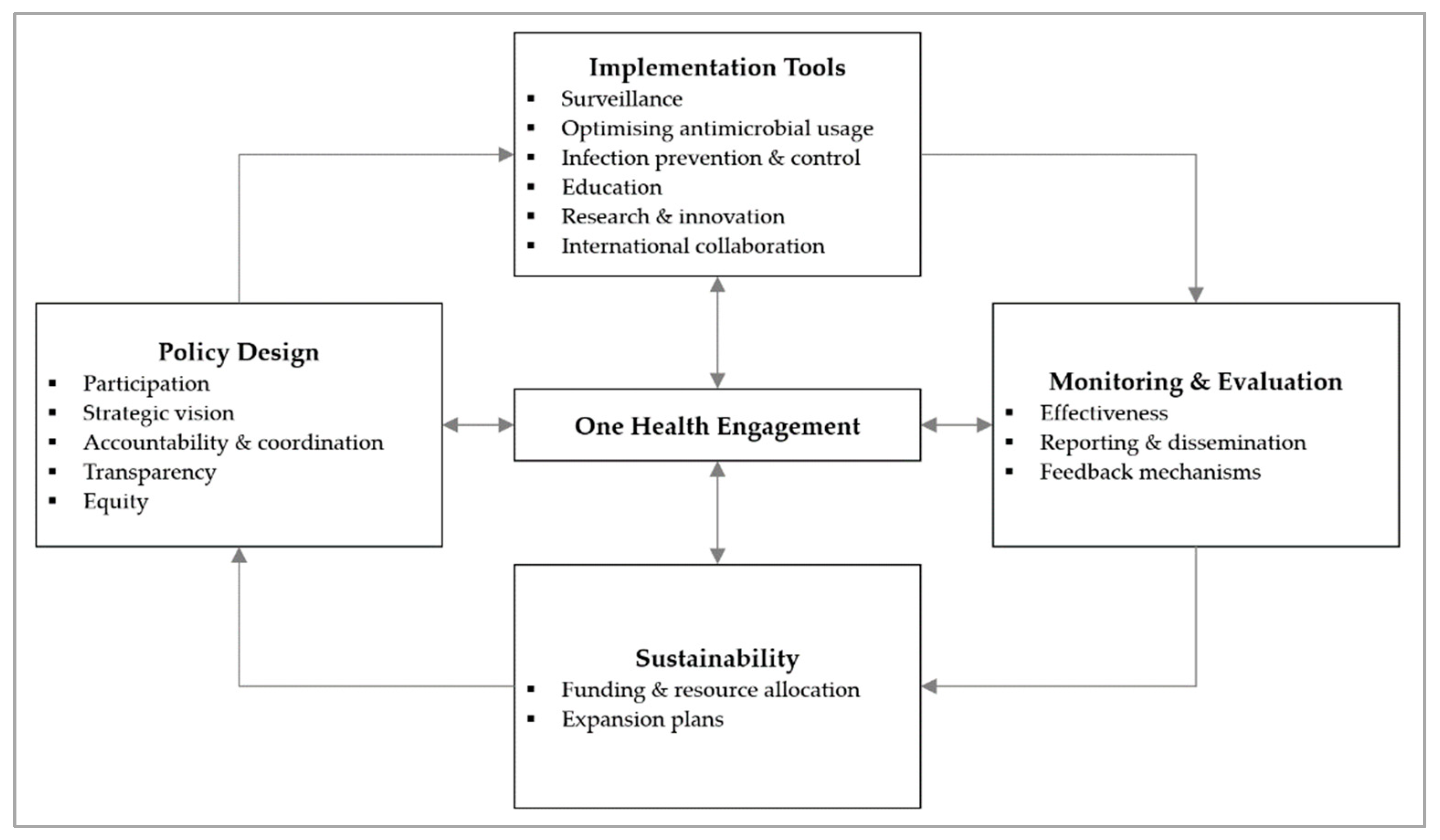
Conceptual Framework
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Analysis
2.3. Ethical Considerations
3. Results
3.1. Participation
“Everyone is given sufficient airtime to speak and share. I don’t think we are dominated by a particular agency. But we’re all at different stages of our work, so some agencies would be able to share more, and some agencies won’t. It’s not unusual to expect those that have more to share to be more vocal. There’s nothing to stop people from sharing what they want to.”—IDI10, Animal Health
“I’m afraid I may not be involved at that level. I suspect the emphasis is still in the hospitals… I’m not aware of this AMRCO. Perhaps, we will be involved when they find that the community is at stake because the spread of AMR has gone to the community… or maybe that they do not want to involve us so early yet.”—IDI06, Human Health
“It’s imperative that the people making the products to help solve the problem, have a voice… It’s like having one stakeholder who’s not at the table. We need strong partnerships from government, industry, and academia. The pharmaceutical voice would be very useful… at some point within the plan to consider financing mechanisms. There needs to be some eyes on that, just like there is in other countries.”—IDI18, Human Health
“It’s building upon the commitment from the leaders… at least at the ASEAN level, the highest level of government has already given their commitment that they would put in a lot of effort to control AMR in their countries.”—IDI04, Human Health
“Our minister, she recently joined the Global Leaders Group on AMR early this year. So now there are quarterly meetings on those. It got everyone even more active into this despite the COVID situation.”—IDI13, Environment
“Our policymakers… I wish that there’s a course…. Then they know at least the basics of infections and AMR. I think this is important, education of policymakers.”—IDI08, Human Health
“Fundamentally, the chief gap that we have is governance and support from administration… it’s a different ballgame in the private sector. They will not really do something unless somebody pushes them. And that push cannot come from me… if that push comes from MOH, then maybe they will start to do something.”—IDI03, Human Health
“We make medicines, and we bring them to market, but that needs to align with the government’s priorities in order to be able to get funding… Once there’s a great product, we need to fix the rest of the policy landscape to be able to bring it all the way to market, which means giving it to a patient in a hospital or someone who needs it.”—IDI18, Human Health
“You need to develop the legislation together with the sector involved… It’s very important because then you work with them from the start instead of this notion that you are against them. In the end, you are trying to work with them to improve things for their production.”—IDI19, Animal Health
“Get the ASP team and the work that they do recognised by the hospital administrators. You have to do it top-down, at the same time, bottom-up to prepare the ground… be willing to spend more time with the ground or the prescribers on the issues about stewardship and the intention of the stewardship team… I would say engagements, a lot of engagements.”—IDI02, Human Health
“Education to doctors in general is done by NCID. We supported them in 2019 when we developed a GP resource. This is an A5-size standee which talks about the role of antibiotics, side effects, and why you shouldn’t take antibiotics for viral infections. We have disseminated to all GPs and healthcare institutions… to support doctors in general because sometimes they are also feeling pressured… sometimes when you go to a doctor you just expect to get medication. We wanted simple infographics to help them to explain to the patients.”—IDI15, Human Health
“We’re tracking it from who the wholesalers sell it to. It’s on a voluntary basis. They give us their sales data to the different animal sectors… I would think most of the wholesalers now ask for a prescription before they sell antimicrobials. They are aware of the need for these. But eventually, we will start doing more active engagement with this group of entities as the legislation and regulations kick in, you know. We will engage them as part of the drafting of these documents.”—IDI10, Animal Health
“…Most of them are engineers, they are not well versed to know that resistant genes do not necessarily mean infectivity… every time we have genetic data, they will ask us ‘Is there a health risk?’… we’ll just try to contextualise for them.”—IDI13, Environment
“No one asked me for feedback on my issues… or rather I mentioned to some staff who were in charge of One Health at that time… don’t know whether he’s still around, but nothing happened.”—IDI08, Human Health
“When we talk about education… it is still focused on public, school children or healthcare workers. We forget the reporters… up till now they don’t know what a virus or bacteria is. Very hard to talk to them, frankly speaking.”—IDI08, Human Health
3.2. Strategic Vision
“We did gaps analyses prior to the publication of the action plan… what’s the current status, what are the gaps, and what we are moving forward on… the future direction.”—IDI09, Animal Health
“AMRCO has this Gantt chart, and it is tracked. We have a five-year work plan and my office is tracking the progress… annually we will also send it to the agencies to ask, ‘Can you help us indicate where are you along in the timeline now?’”—IDI12, Human Health
“In Singapore the action plan did not have hard targets. It’s because for quite a lot of issues, we don’t even know what’s the baseline problem yet. So, we just hope to see that there is a reduction, but in the action plan there’s no target.”—IDI12, Human Health
“For AMR, a lot of things you can’t account for it… How do you hold someone accountable for it when it’s not within their control? I think it can be a bit demoralizing for people… So unless you have some very tangible things, for example you want to achieve a 10% reduction in something very definite, like antimicrobial prescription in ARI.—IDI12, Human Health
3.3. Accountability and Coordination
“…There were formal networks to work together in areas of communicable disease control already. For example, whenever there is a zoonotic disease or food poisoning. We just leverage on that.”—IDI04, Human Health
“There needs to be a dedicated group of people paid to do this instead of being a side job. Or else, it’s very difficult to push things forward… that was the impetus. Also, previously when all agencies are working separately, you may lose track of each other. So that’s why AMRCO was set up to drive the agenda.”—IDI12, Human Health
“From time to time, some of these people may change, but there’s continuity because it is not driven by specific persons but driven by the organisation itself. So even if people change it’s fine.”—IDI04, Human Health
“…what I could see is that it’s a lot more coordinated. And because now we know people from different agencies working on AMR, when we have issues, we are able to go back to these people… I think that since the NSAP that got all of us together, we start to see this issue not just an issue that we need to tackle within our sector. We start to see that, ‘Hey, maybe what I’m doing could help you. Or maybe what you are doing could help me. Maybe we could do something together that makes more sense than what we have been trying to do individually.’”—IDI13, Environment
“We formed three sub-working groups when we were writing up the plan… surveillance, education, and research. These are the three areas that needed cross-sectorial discussions. Whereas optimising use, it’s either human or animal but they don’t intersect. And neither does IPC…”—IDI17, Human Health
“What I hope to improve will be workflow or red tape issues… the accounting and finance work is quite challenging because there is no such system. We are not under a single ministry so that’s the challenge. We have to work on each other’s tempo… it cannot be that one agency says, ‘Hey, let’s go ahead and do that.’, while the others are lagging behind. We have to balance out and support each other.”—IDI12, Human Health
“I know there’s an action plan but I’m not sure whether there is a task force set up. If there is a task force, it will be the work of this task force to make sure that all of us talk.”—IDI02, Human Health
“For accountability… at the start of the year, they will plan what they want to achieve. If they don’t come up with it, I suppose there’s no punitive measures. But being professionals, everyone understands what they have promised. Delay sometimes is inevitable due to some other reasons or because your other work partners cannot deliver within that timeframe. So, you just have to take that… they will catch up after that.”—IDI12, Human Health
“Usually, they are accountable to the management. These things are presented to the senior management, medical boards….”—IDI05, Human Health
“Why am I not scared that my hospital’s numbers are going up? Because no one cares… currently there’s no accountability in the hospital. You can’t say CEOs are responsible for everything. The accountability should be from MOH… It should say this person is accountable for this pathogen or this particular KPI. You are accountable for it, if not, your bonus will be cut. It should be tied to finance… I think that’s probably better than what they’re doing now.”—IDI07, Human Health
3.4. Transparency
“I am an infectious diseases physician… I don’t know what came out of this AMR action plan…If your publicity is so good that even I don’t know, imagine others… The information that’s made is not publicly available. When I say public, I’m talking about medical professionals, infectious disease physicians who are involved in public health decision making…”—IDI07, Human Health
“How open are we ready to share the data, I think that would be the biggest barrier… I still see some constraint in the sharing… it’s just the way the culture is.”—IDI01, Environment
“Animal sites should tell us what they’re finding in terms of VRE in animals because we are consuming them after all. We bring in the chickens, we consume them. But they were either not monitoring or they’re very reluctant to share how much VRE they’re picking up.”—IDI08, Human Health
“…if we want to make the data sharing more transparent, the system needs to be changed. For example, the data on the sales and use of antimicrobials from farms and specific industries… it needs to be quite transparently shared. Right now, most of this information is shared through the reports.”—IDI10, Animal Health
3.5. One Health Engagement
“I think it’s relevant and extremely important because we can’t work in silos. Whatever we’re doing in our little world, in our little, tiny niche can only contribute so much to the drama of antibiotic abuse. If the whole ecology is threatened by so many different arms, then I think every arm should be looked at… what they call the One Health concept.”—IDI03, Human Health
“You need to have a surveillance where you can detect whatever you’re looking for in the animals preferably, but at least in the food and then the humans. And then you have to be able to link the data between the food and the humans and then find out where do you want to do something about…”—IDI19, Animal Health
“It is interesting because when it’s shared from another sector, sometimes you have the ‘aha!’ moments about your own sector. We start to think, ‘Oh, yeah. This target is relevant to you, then maybe do you want to look at my sector as well on this?’”—IDI13, Environment
“Within these two years, we have quite serious discussions on surveillance of certain hotspots. But we still have to work with the other agencies to see whether our targets and sampling points makes sense from the cross-sectoral approach.”—IDI13, Environment
3.6. Funding and Resource Allocation
“We just went through a budget-cutting exercise in view of the new wave of COVID restrictions. We are asked to tighten our belts a little bit, so the one thing that’s easiest to take away is AMR as the direct impact of the work is not as immediate.—IDI11, Human Health
“There are regular meetings amongst the committee members, and we are committing a sizable sum of funding for the work to be carried out through this committee… we have put out support from the agency for the funding, so there’s a very positive outlook from our management towards this One Health work.”—IDI01, Environment
“Many governments globally are exploring options for practical market level incentives to ensure that novel antibiotics are commercially sustainable. So, there’s an AMR Action Fund… all the big pharma companies put in one billion dollars in investment to bring new antibiotics to market. But again, we’ve got to work with our governments to actually get them into market.”—IDI18, Human Health
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 17 November 2022).
- World Health Organization. Global Action Plan on Antimicrobial Resistance. Available online: http://www.wpro.who.int/entity/drug_resistance/resources/global_action_plan_eng.pdf (accessed on 17 November 2022).
- United Nations. Political Declaration of the High-Level Meeting of the General Assembly on Antimicrobial Resistance. Available online: https://digitallibrary.un.org/record/842813?ln=en (accessed on 17 November 2022).
- World Health Organization. Antimicrobial Resistance Global Report on Surveillance. Available online: http://www.who.int/iris/bitstream/10665/112642/1/9789241564748_eng.pdf?ua=1 (accessed on 17 November 2022).
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Barış, E. Antimicrobial Resistance: Another Long-Term Consequence of COVID-19? Available online: https://blogs.worldbank.org/health/antimicrobial-resistance-another-long-term-consequence-covid-19 (accessed on 17 November 2022).
- Department of Statistics Singapore. Singapore Population. Available online: https://www.singstat.gov.sg/modules/infographics/population (accessed on 17 November 2022).
- One Health Antimicrobial Resistance Workgroup Singapore. One Health Report on Antimicrobial Utilisation and Resistance in Singapore. 2019. Available online: https://www.moh.gov.sg/resources-statistics/reports/one-health-report-on-antimicrobial-utilisation-and-resistance-2019 (accessed on 17 November 2022).
- One Health Antimicrobial Resistance Workgroup Singapore. One Health Report on Antimicrobial Utilisation and Resistance in Singapore. 2017. Available online: https://www.moh.gov.sg/resources-statistics/reports/one-health-report-on-antimicrobial-utilisation-and-resistance-2017 (accessed on 17 November 2022).
- Pek, H.B.; Kadir, S.A.; Osman, S.; Mohamed, R.; Ismail, H.; Garbo, G.; You, L.; Gin, K.Y.-H.; Ng, L.C.; Octavia, S.; et al. Antimicrobial resistant bacteria in coastal water and linked waterways. In Proceedings of the 7th World One Health Congress, Singapore, 7–11 November 2022. [Google Scholar]
- One Health Antimicrobial Resistance Workgroup Singapore. The National Strategic Action Plan on Antimicrobial Resistance: Singapore. Available online: https://www.moh.gov.sg/resources-statistics/reports/national-strategic-action-plan-on-antimicrobial-resistance (accessed on 17 November 2022).
- Chua, A.Q.; Verma, M.; Hsu, L.Y.; Legido-Quigley, H. An analysis of national action plans on antimicrobial resistance in Southeast Asia using a governance framework approach. Lancet Reg. Health-West. Pac. 2021, 7, 100084. [Google Scholar] [CrossRef] [PubMed]
- Chua, A.Q.; Kwa, A.L.; Tan, T.Y.; Legido-Quigley, H.; Hsu, L.Y. Ten-year narrative review on antimicrobial resistance in Singapore. Singap. Med. J. 2019, 60, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.R.; Chua, A.Q.; Tan, S.T.; Tam, C.C.; Hsu, L.Y.; Legido-Quigley, H. Combating Antimicrobial Resistance in Singapore: A Qualitative Study Exploring the Policy Context, Challenges, Facilitators, and Proposed Strategies. Antibiotics 2019, 8, 201. [Google Scholar] [CrossRef] [PubMed]
- One Health Antimicrobial Resistance Workgroup Singapore. Progress Report for the National Strategic Action Plan on Antimicrobial Resistance (2018–2020). Available online: https://www.moh.gov.sg/resources-statistics/reports/nsap-amr-progress-report-2020 (accessed on 17 November 2022).
- Anderson, M.; Schulze, K.; Cassini, A.; Plachouras, D.; Mossialos, E. A governance framework for development and assessment of national action plans on antimicrobial resistance. Lancet Infect. Dis. 2019, 19, e371–e384. [Google Scholar] [CrossRef] [PubMed]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis; Sage: London, UK, 2006. [Google Scholar]
- Strauss, A.L. Qualitative Analysis for Social Scientists; Cambridge University Press: New York, NY, USA, 1987. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. One Health Joint Plan of Action (2022–2026): Working Together for the Health of Humans, Animals, Plants and the Environment. Available online: https://www.who.int/publications/i/item/9789240059139 (accessed on 17 November 2022).
- Laaser, U.; Bjegovic-Mikanovic, V.; Wenzel, H.; Seifman, R.; Stroud, C.; Craig, C.; Kaplan, B.; Kahn, L.; Roopnarine, R. Exchange and Coordination: Deficits of the Global One Health Movement. In Proceedings of the The 7th World One Health Congress, Singapore, 7–11 November 2022. [Google Scholar]
- Frumence, G.; Mboera, L.E.G.; Sindato, C.; Katale, B.Z.; Kimera, S.; Metta, E.; Durrance-Bagale, A.; Jung, A.S.; Mshana, S.E.; Clark, T.G.; et al. The Governance and Implementation of the National Action Plan on Antimicrobial Resistance in Tanzania: A Qualitative Study. Antibiotics 2021, 10, 273. [Google Scholar] [CrossRef]
- Song, M.; Deng, Z.; Chan, O.; Grepin, K.A. Understanding the Implementation of Antimicrobial Policies: Lessons from the Hong Kong Strategy and Action Plan. Antibiotics 2022, 11, 636. [Google Scholar] [CrossRef]
- Lota, M.M.M.; Chua, A.Q.; Azupardo, K.; Lumangaya, C.; Reyes, K.A.V.; Villanueva, S.; Legido-Quigley, H.; Roxas, E.A. A Qualitative Study on the Design and Implementation of the National Action Plan on Antimicrobial Resistance in the Philippines. Antibiotics 2022, 11, 820. [Google Scholar] [CrossRef]
- Acharya, K.P.; Subramanya, S.H.; Lopes, B.S. Combatting antimicrobial resistance in Nepal: The need for precision surveillance programmes and multi-sectoral partnership. JAC Antimicrob. Resist. 2019, 1, dlz066. [Google Scholar] [CrossRef]
- Sommanustweechai, A.; Tangcharoensathien, V.; Malathum, K.; Sumpradit, N.; Kiatying-Angsulee, N.; Janejai, N.; Jaroenpoj, S. Implementing national strategies on antimicrobial resistance in Thailand: Potential challenges and solutions. Public Health 2018, 157, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Khalik, S. New Workgroup Set Up to Fight Antimicrobial Resistance. Available online: https://www.straitstimes.com/singapore/health/new-workgroup-set-up-by-govt-to-fight-antimicrobial-resistance (accessed on 17 November 2022).
- Ministry of Sustainability and the Environment Singapore. The Inaugural Meeting of the Global Leaders Group on Antimicrobial Resistance (First Day)-Ms Grace Fu. Available online: https://www.mse.gov.sg/resource-room/category/2021-01-26-intervention-at-the-first-day-of-the-inaugural-meeting-of-the-glg-on-amr/ (accessed on 17 November 2022).
- Global Leaders Group on Antimicrobial Resistance. Priorities of the Global Leaders Group on AMR for 2021–2022. Available online: https://cdn.who.int/media/docs/default-source/antimicrobial-resistance/glg-action-plan-july-2021_final.pdf (accessed on 17 November 2022).
- Society for Public Health Education. Guide to Effectively Educating State and Local Policymakers. Available online: https://www.sophe.org/resources/guide-effectively-educating-state-local-policymakers/ (accessed on 17 November 2022).
- Martin, A.; Gravelle, T.B.; Baekkeskov, E.; Lewis, J.; Kashima, Y. Enlisting the support of trusted sources to tackle policy problems: The case of antimicrobial resistance. PLoS ONE 2019, 14, e0212993. [Google Scholar] [CrossRef] [PubMed]
- Legido-Quigley, H.; Khan, M.S.; Durrance-Bagale, A.; Hanefeld, J. Something Borrowed, Something New: A Governance and Social Construction Framework to Investigate Power Relations and Responses of Diverse Stakeholders to Policies Addressing Antimicrobial Resistance. Antibiotics 2018, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Kickbusch, I.; Gleicher, D. Governance for Health in the 21st Century. Available online: http://www.euro.who.int/__data/assets/pdf_file/0019/171334/RC62BD01-Governance-for-Health-Web.pdf (accessed on 10 January 2022).
- Willemsen, A.; Reid, S.; Assefa, Y. A review of national action plans on antimicrobial resistance: Strengths and weaknesses. Antimicrob. Resist. Infect. Control 2022, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.M.; Naher, N.; Tune, S.N.B.K.; Islam, B.Z. The Implementation of National Action Plan (NAP) on Antimicrobial Resistance (AMR) in Bangladesh: Challenges and Lessons Learned from a Cross-Sectional Qualitative Study. Antibiotics 2022, 11, 690. [Google Scholar] [CrossRef]
- Frumence, G.; Mboera, L.E.G.; Katale, B.Z.; Sindato, C.; Kimera, S.; Durrance-Bagale, A.; Mshana, S.E.; Clark, T.G.; Rweyemamu, M.M.; Legido-Quigley, H.; et al. Policy actors and human and animal health practitioners’ perceptions of antimicrobial use and resistance in Tanzania: A qualitative study. J. Glob. Antimicrob. Resist. 2021, 25, 40–47. [Google Scholar] [CrossRef]
- Mariappan, V.; Vellasamy, K.M.; Mohamad, N.A.; Subramaniam, S.; Vadivelu, J. OneHealth Approaches Contribute Towards Antimicrobial Resistance: Malaysian Perspective. Front. Microbiol. 2021, 12, 718774. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.; Lin, A.; Lin, E.; Lin, H.L.; Lim, K.; Fernandez, C.J.; Chua, T.H.; Chang, S.F.; Yap, H.H. An Engagement and Advocacy lesson for rabies prevention: Singapore’s Trap-Neuter-Release-Manage Programme and mass rabies vaccination. In Proceedings of the The 7th World One Health Congress, Singapore, 7–11 November 2022. [Google Scholar]
- Pek, H.B.; Kadir, S.A.; Arivalan, S.; Osman, S.; Mohamed, R.; Ng, L.C.; Wong, J.C.C.; Octavia, S. Extended-Spectrum Beta Lactamase E. coli not detected in recreational beach waters in Singapore. In Proceedings of the The 7th World One Health Congress, Singapore, 7–11 November 2022. [Google Scholar]
- World Health Organization. UN Environment Programme Joins Alliance to Implement One Health Approach. Available online: https://www.who.int/news/item/18-03-2022-un-environment-programme-joins-alliance-to-implement-one-health-approach (accessed on 17 November 2022).
- Catalan-Matamoros, D.; Pariente, A.; Elias-Perez, C. What we know about media communication on antibiotics and antimicrobial resistance: A systematic review of the scientific literature. Patient Educ. Couns. 2019, 102, 1427–1438. [Google Scholar] [CrossRef]
- Liao, Q.; Yuan, J.; Dong, M.; Paterson, P.; Lam, W.W.T. Drivers of global media attention and representations for antimicrobial resistance risk: An analysis of online English and Chinese news media data, 2015–2018. Antimicrob. Resist. Infect. Control 2021, 10, 152. [Google Scholar] [CrossRef]
- Jin, L.; Pruden, A.; Boehm, A.B.; Alvarez, P.J.J.; Raskin, L.; Kohn, T.; Li, X. Integrating Environmental Dimensions of “One Health” to Combat Antimicrobial Resistance: Essential Research Needs. Environ. Sci. Technol. 2022, 56, 14871–14874. [Google Scholar] [CrossRef]
- Pruden, A.; Alcalde, R.E.; Alvarez, P.J.J.; Ashbolt, N.; Bischel, H.; Capiro, N.L.; Crossette, E.; Frigon, D.; Grimes, K.; Haas, C.N.; et al. An Environmental Science and Engineering Framework for Combating Antimicrobial Resistance. Environ. Eng. Sci. 2018, 35, 1005–1011. [Google Scholar] [CrossRef]
- Harant, A. Assessing transparency and accountability of national action plans on antimicrobial resistance in 15 African countries. Antimicrob. Resist. Infect. Control 2022, 11, 15. [Google Scholar] [CrossRef] [PubMed]
- Paschke, A.; Dimancesco, D.; Vian, T.; Kohler, J.C.; Forte, G. Increasing transparency and accountability in national pharmaceutical systems. Bull. World Health Organ. 2018, 96, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.; Aceron, J. Doing Accountability Differently, a Proposal for the Vertical Integration of Civil Society Monitoring and Advocacy. Available online: https://www.cmi.no/publications/5951-doing-accountability-differently (accessed on 17 November 2022).
- Cultural Atlas. Singaporean Culture. Available online: https://culturalatlas.sbs.com.au/singaporean-culture/singaporean-culture-business-culture (accessed on 17 November 2022).
- Yam, E.L.Y.; Hsu, L.Y.; Yap, E.P.; Yeo, T.W.; Lee, V.; Schlundt, J.; Lwin, M.O.; Limmathurotsakul, D.; Jit, M.; Dedon, P.; et al. Antimicrobial Resistance in the Asia Pacific region: A meeting report. Antimicrob. Resist. Infect. Control 2019, 8, 202. [Google Scholar] [CrossRef] [PubMed]
- Interagency Coordination Group on Antimicrobial Resistance. Meeting the Challenge of Antimicrobial Resistance: From Communication to Collective Action, IACG Discussion Paper. Available online: https://www.who.int/antimicrobial-resistance/interagency-coordination-group/IACG_Meeting_challenge_AMR_communication_to_collective_action_270718.pdf (accessed on 17 November 2022).
- World Health Organization; Food and Agriculture Organization of the United Nations; World Organisation for Animal Health (OIE). Monitoring and Evaluation of the Global Action Plan on Antimicrobial Resistance: Framework and Recommended Indicators. Available online: https://apps.who.int/iris/handle/10665/325006 (accessed on 17 November 2022).


{kind=link}
{kind=link}
| Type of Institution | Sector | Total | ||
|---|---|---|---|---|
| Human Health | Animal Health | Environment | ||
| Academia | 1 | 1 | 2 | |
| Government agency | 6 | 3 | 2 | 11 |
| Hospital (public and private) | 5 | 5 | ||
| Industry | 1 | 1 | ||
| Primary care | 1 | 1 | ||
| Total | 13 | 4 | 3 | 20 |
| S/N | Policy Recommendations | Details |
|---|---|---|
| 1 | Appoint a dedicated inter-ministerial/cross-sectoral joint secretariat |
|
| 2 | Enhance engagement of all stakeholders at all levels |
|
| 3 | Increase participation from stakeholders beyond the One Health agencies involved in human health, animal health, and environment |
|
| 4 | Better policy advocacy for increased awareness and sustained behavioural change |
|
| 5 | Develop efficient data sharing systems to improve transparency |
|
| 6 | Set context specific indicators for the implementation plans |
|
| 7 | Increase mobilisation of financial resources to support sustainability of implementation plans |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chua, A.Q.; Verma, M.; Azupardo, K.; Lota, M.M.; Hsu, L.Y.; Legido-Quigley, H. A Qualitative Study on the Policy Process and Development of the National Action Plan on Antimicrobial Resistance in Singapore. Antibiotics 2023, 12, 1322. https://doi.org/10.3390/antibiotics12081322
Chua AQ, Verma M, Azupardo K, Lota MM, Hsu LY, Legido-Quigley H. A Qualitative Study on the Policy Process and Development of the National Action Plan on Antimicrobial Resistance in Singapore. Antibiotics. 2023; 12(8):1322. https://doi.org/10.3390/antibiotics12081322
Chicago/Turabian StyleChua, Alvin Qijia, Monica Verma, Karen Azupardo, Maria Margarita Lota, Li Yang Hsu, and Helena Legido-Quigley. 2023. "A Qualitative Study on the Policy Process and Development of the National Action Plan on Antimicrobial Resistance in Singapore" Antibiotics 12, no. 8: 1322. https://doi.org/10.3390/antibiotics12081322
APA StyleChua, A. Q., Verma, M., Azupardo, K., Lota, M. M., Hsu, L. Y., & Legido-Quigley, H. (2023). A Qualitative Study on the Policy Process and Development of the National Action Plan on Antimicrobial Resistance in Singapore. Antibiotics, 12(8), 1322. https://doi.org/10.3390/antibiotics12081322