
Clonal, Plasmidic and Genetic Diversity of Multi-Drug-Resistant Enterobacterales from Hospitalized Patients in Tripoli, Libya

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
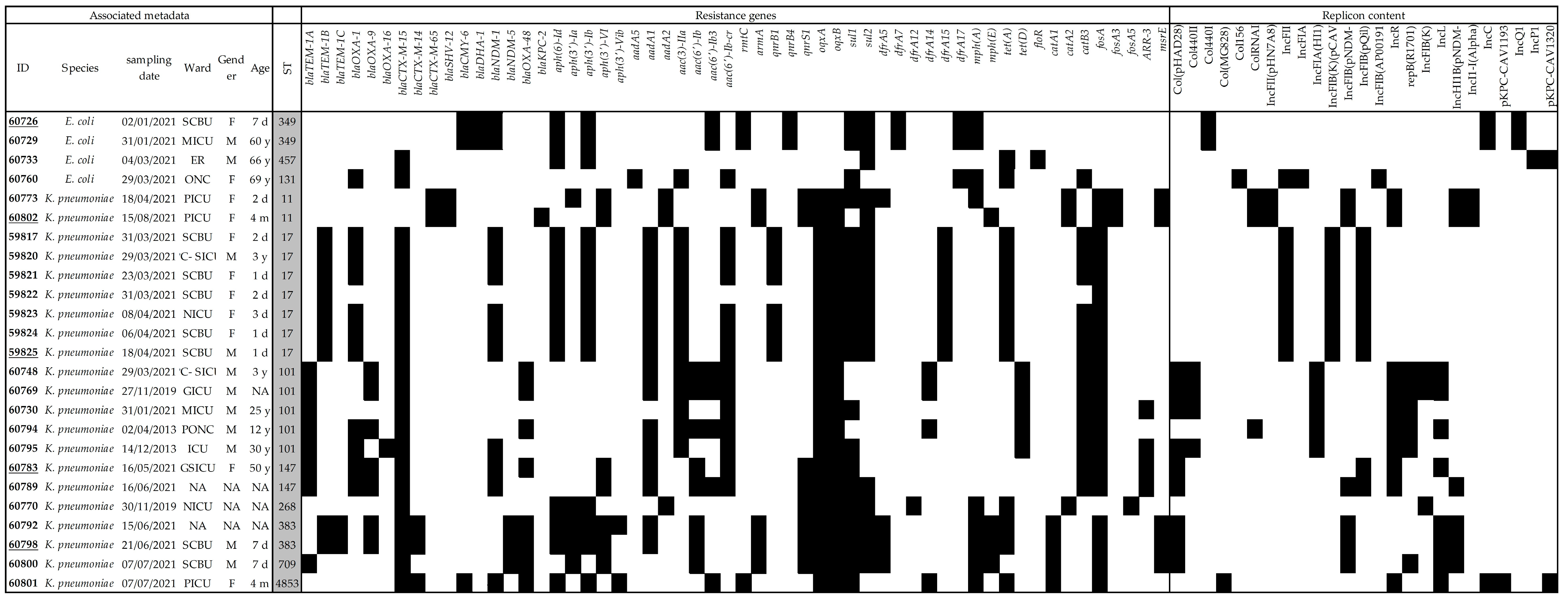
2.1. Genetic Diversity
2.2. Resistance Phenotypes and Detection of Beta-Lactam Resistance Genes
2.3. Genetic Characterization of the Resistance Genes
2.4. Genetic Determinants Carrying the Beta-Lactam Resistance Genes
3. Discussion
4. Materials and Methods
4.1. Study Design and Bacterial Isolation
4.2. Antimicrobial Susceptibility Testing
4.3. Detection of Resistance Genes and Strain Clonality
4.4. Illumina Short-Read Sequencing and Data Analyses
4.5. MinION Long-Read Sequencing
4.6. Characterization of Plasmids
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- WHO. WHO Integrated Global Surveillance on ESBL-Producing E. coli Using a “One Health” Approach: Implementation and Opportunities; World Health Organization: Geneva, Switzerland, 2021. Available online: https://apps.who.int/iris/handle/10665/340079 (accessed on 29 June 2023).
- Al-Mir, H.; Osman, M.; Drapeau, A.; Hamze, M.; Madec, J.Y.; Haenni, M. Spread of ESC-, carbapenem- and colistin-resistant Escherichia coli clones and plasmids within and between food workers in Lebanon. J. Antimicrob. Chemother. 2021, 76, 3135–3143. [Google Scholar] [CrossRef]
- Stracy, M.; Snitser, O.; Yelin, I.; Amer, Y.; Parizade, M.; Katz, R.; Rimler, G.; Wolf, T.; Herzel, E.; Koren, G.; et al. Minimizing treatment-induced emergence of antibiotic resistance in bacterial infections. Science 2022, 375, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Meletis, G. Carbapenem resistance: Overview of the problem and future perspectives. Ther. Adv. Infect. Dis. 2016, 3, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Stewardson, A.J.; Marimuthu, K.; Sengupta, S.; Allignol, A.; El-Bouseary, M.; Carvalho, M.J.; Hassan, B.; Delgado-Ramirez, M.A.; Arora, A.; Bagga, R.; et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): A multinational prospective cohort study. Lancet Infect. Dis. 2019, 19, 601–610. [Google Scholar] [CrossRef]
- Lafeuille, E.; Decré, D.; Mahjoub-Messai, F.; Bidet, P.; Arlet, G.; Bingen, E. OXA-48 carbapenemase-producing Klebsiella pneumoniae isolated from Libyan patients. Microb. Drug Resist. 2013, 19, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Kocsis, E.; Savio, C.; Piccoli, M.; Cornaglia, G.; Mazzariol, A. Klebsiella pneumoniae harbouring OXA-48 carbapenemase in a Libyan refugee in Italy. Clin. Microbiol. Infect. 2013, 19, E409–E411. [Google Scholar] [CrossRef]
- Kraiem, A.G.; Zorgani, A.; Elahmer, O.; El Salabi, A.A.; Ghenghesh, K.S. Carbapenem-resistant gram-negative bacilli in Tripoli, Libya. Am. J. Infect. Control. 2016, 44, 1192–1194. [Google Scholar] [CrossRef]
- Kieffer, N.; Ahmed, M.O.; Elramalli, A.K.; Daw, M.A.; Poirel, L.; Álvarez, R.; Nordmann, P. Colistin-resistant carbapenemase-producing isolates among Klebsiella spp. and Acinetobacter baumannii in Tripoli, Libya. J. Glob. Antimicrob. Resist. 2018, 13, 37–39. [Google Scholar] [CrossRef]
- Slimene, K.; Salabi, A.E.; Dziri, O.; Mathlouthi, N.; Diene, S.M.; Mohamed, E.A.; Amhalhal, J.M.A.; Aboalgasem, M.O.; Alrjael, J.F.; Rolain, J.M.; et al. Epidemiology, phenotypic and genotypic characterization of carbapenem-resistant gram-negative bacteria from a Libyan hospital. Microb. Drug Resist. 2023, in press. [Google Scholar] [CrossRef]
- Slimene, K.; Ali, A.A.; Mohamed, E.A.; El Salabi, A.; Suliman, F.S.; Elbadri, A.A.; El-Fertas, F.F.; El-Awjly, A.; Shokri, S.A.; Rolain, J.M.; et al. Isolation of carbapenem and colistin resistant gram-negative bacteria colonizing immunocompromised SARS-CoV-2 patients admitted to some Libyan hospitals. Microbiol. Spectr. 2023, 11, e0297222. [Google Scholar] [CrossRef] [PubMed]
- Okeke, I.N.; Laxminarayan, R.; Bhutta, Z.A.; Duse, A.G.; Jenkins, P.; O’Brien, T.F.; Pablos-Mendez, A.; Klugman, K.P. Antimicrobial resistance in developing countries. Part I: Recent trends and current status. Lancet Infect. Dis. 2005, 5, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef]
- Carattoli, A.; Villa, L.; Poirel, L.; Bonnin, R.A.; Nordmann, P. Evolution of IncA/C blaCMY-2-carrying plasmids by acquisition of the blaNDM-1 carbapenemase gene. Antimicrob. Agents Chemother. 2012, 56, 783–786. [Google Scholar] [CrossRef] [PubMed]
- Hudson, C.M.; Bent, Z.W.; Meagher, R.J.; Williams, K.P. Resistance determinants and mobile genetic elements of an NDM-1-encoding Klebsiella pneumoniae strain. PLoS ONE 2014, 9, e99209. [Google Scholar] [CrossRef]
- Martin, M.J.; Corey, B.W.; Sannio, F.; Hall, L.R.; MacDonald, U.; Jones, B.T.; Mills, E.G.; Harless, C.; Stam, J.; Maybank, R.; et al. Anatomy of an extensively drug-resistant Klebsiella pneumoniae outbreak in Tuscany, Italy. Proc. Natl. Acad. Sci. USA 2021, 118, e2110227118. [Google Scholar] [CrossRef]
- Hendrickx, A.P.A.; Landman, F.; de Haan, A.; Witteveen, S.; van Santen-Verheuvel, M.G.; Schouls, L.M.; the Dutch CPE surveillance Study Group. blaOXA-48-like genome architecture among carbapenemase-producing Escherichia coli and Klebsiella pneumoniae in the Netherlands. Microb. Genom. 2021, 7, 512. [Google Scholar] [CrossRef]
- Lv, L.C.; Lu, Y.Y.; Gao, X.; He, W.Y.; Gao, M.Y.; Mo, K.B.; Liu, J.H. Characterization of NDM-5-producing Enterobacteriaceae isolates from retail grass carp (Ctenopharyngodon idella) and evidence of blaNDM-5-bearing IncHI2 plasmid transfer between ducks and fish. Zool Res. 2022, 43, 255–264. [Google Scholar] [CrossRef]
- Wang, Q.; Sun, J.; Li, J.; Ding, Y.; Li, X.P.; Lin, J.; Hassan, B.; Feng, Y. Expanding landscapes of the diversified mcr-1-bearing plasmid reservoirs. Microbiome 2017, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, Y.; Yao, S.; Hu, J.; Zhao, Y.; Fu, S.; Song, Y.; Wang, C.; Zhang, G.; Wei, D.; et al. Epidemicity and clonal replacement of hypervirulent carbapenem-resistant Klebsiella pneumoniae with diverse pathotypes and resistance profiles in a hospital. J. Glob. Antimicrob. Resist. 2023, 32, 4–10. [Google Scholar] [CrossRef]
- Yang, X.; Liu, W.; Liu, Y.; Wang, J.; Lv, L.; Chen, X.; He, D.; Yang, T.; Hou, J.; Tan, Y.; et al. F33: A-: B-, IncHI2/ST3, and IncI1/ST71 plasmids drive the dissemination of fosA3 and blaCTX-M-55/-14/-65 in Escherichia coli from chickens in China. Front. Microbiol. 2014, 5, 688. [Google Scholar] [CrossRef] [PubMed]
- Zurfluh, K.; Treier, A.; Schmitt, K.; Stephan, R. Mobile fosfomycin resistance genes in Enterobacteriaceae—An increasing threat. MicrobiologyOpen 2020, 9, e1135. [Google Scholar] [CrossRef] [PubMed]
- Peirano, G.; Chen, L.; Kreiswirth, B.N.; Pitout, J.D.D. Emerging antimicrobial-resistant high-risk Klebsiella pneumoniae clones ST307 and ST147. Antimicrob. Agents Chemother. 2020, 64, e01148-20. [Google Scholar] [CrossRef]
- WHO. Global Priority List of Antibioticresistant Bacteria to Guide Research, Discovery and Development of New Antibiotics; WHO: Geneva, Switzerland, 2017. Available online: https://www.who.int/medicines/publications/global-priority-list-antibiotic-resistant-bacteria/en/ (accessed on 29 June 2023).
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Kochan, T.J.; Nozick, S.H.; Medernach, R.L.; Cheung, B.H.; Gatesy, S.W.M.; Lebrun-Corbin, M.; Mitra, S.D.; Khalatyan, N.; Krapp, F.; Qi, C.; et al. Genomic surveillance for multidrug-resistant or hypervirulent Klebsiella pneumoniae among United States bloodstream isolates. BMC Infect. Dis. 2022, 22, 603. [Google Scholar] [CrossRef] [PubMed]
- De Koster, S.; Rodriguez Ruiz, J.P.; Rajakani, S.G.; Lammens, C.; Glupczynski, Y.; Goossens, H.; Xavier, B.B. Diversity in the characteristics of Klebsiella pneumoniae ST101 of human, environmental, and animal origin. Front. Microbiol. 2022, 13, 838207. [Google Scholar] [CrossRef]
- Abderrahim, A.; Djahmi, N.; Loucif, L.; Nedjai, S.; Chelaghma, W.; Gameci-Kirane, D.; Dekhil, M.; Lavigne, J.-P.; Pantel, A. Dissemination of OXA-48- and NDM-1-producing Enterobacterales isolates in an Algerian hospital. Antibiotics 2022, 11, 750. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; An, J.; Ma, Y.; Ye, L.; Luo, Y.; Tao, C.; Yang, J. Nosocomial outbreak of OXA-48-producing Klebsiella pneumoniae in a Chinese hospital: Clonal transmission of ST147 and ST383. PLoS ONE 2016, 11, e0160754. [Google Scholar] [CrossRef]
- Turton, J.F.; Payne, Z.; Coward, A.; Hopkins, K.L.; Turton, J.A.; Doumith, M.; Woodford, N. Virulence genes in isolates of Klebsiella pneumoniae from the UK during 2016, including among carbapenemase gene-positive hypervirulent K1-ST23 and ‘non-hypervirulent’ types ST147, ST15 and ST383. J. Med. Microbiol. 2018, 67, 118–128. [Google Scholar] [CrossRef]
- Wu, R.; Lv, L.; Wang, C.; Gao, G.; Yu, K.; Cai, Z.; Liu, Y.; Yang, J.; Liu, J.H. IS26-mediated formation of a hybrid plasmid carrying mcr-1.1. Infect. Drug Resist. 2022, 15, 7227–7234. [Google Scholar] [CrossRef]
- Shibata, N.; Kurokawa, H.; Doi, Y.; Yagi, T.; Yamane, K.; Wachino, J.-i.; Suzuki, S.; Kimura, K.; Ishikawa, S.; Kato, H.; et al. PCR classification of CTX-M-type beta-lactamase genes identified in clinically isolated gram-negative bacilli in Japan. Antimicrob. Agents Chemother. 2006, 50, 791–795. [Google Scholar] [CrossRef]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Kieffer, N.; Poirel, L.; Nordmann, P.; Madec, J.Y.; Haenni, M. Emergence of colistin resistance in Klebsiella pneumoniae from veterinary medicine. J. Antimicrob. Chemother. 2015, 70, 1265–1267. [Google Scholar] [CrossRef] [PubMed]
- Doumith, M.; Day, M.J.; Hope, R.; Wain, J.; Woodford, N. Improved multiplex PCR strategy for rapid assignment of the four major Escherichia coli phylogenetic groups. J. Clin. Microbiol. 2012, 50, 3108–3110. [Google Scholar] [CrossRef]
- Caméléna, F.; Birgy, A.; Smail, Y.; Courroux, C.; Mariani-Kurkdjian, P.; Le Hello, S.; Bonacorsi, S.; Bidet, P. Rapid and simple universal Escherichia coli genotyping method based on multiple-locus variable-number tandem-repeat analysis using single-tube multiplex PCR and standard gel electrophoresis. Appl. Environ. Microbiol. 2019, 85, e02812–e02818. [Google Scholar] [CrossRef] [PubMed]
- Saidani, M.; Messadi, L.; Chaouechi, A.; Tabib, I.; Saras, E.; Soudani, A.; Daaloul-Jedidi, M.; Mamlouk, A.; Ben Chehida, F.; Chakroun, C.; et al. High genetic diversity of Enterobacteriaceae clones and plasmids disseminating resistance to extended-spectrum cephalosporins and colistin in healthy chicken in Tunisia. Microb. Drug Resist. 2019, 25, 1507–1513. [Google Scholar] [CrossRef]
- Tenover, F.C.; Arbeit, R.D.; Goering, R.V.; Mickelsen, P.A.; Murray, B.E.; Persing, D.H.; Swaminathan, B. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: Criteria for bacterial strain typing. J Clin Microbiol 1995, 33, 2233–2239. [Google Scholar] [CrossRef]
- Schwengers, O.; Jelonek, L.; Dieckmann, M.A.; Beyvers, S.; Blom, J.; Goesmann, A. Bakta: Rapid and standardized annotation of bacterial genomes via alignment-free sequence identification. Microb. Genom. 2021, 7, 000685. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| K. pneumoniae (n = 49) | Escherichia coli (n = 5) | |||
|---|---|---|---|---|
| n | % | n | % | |
| Amoxicillin 1 | − | − | 5 | 100.0 |
| AMC 2 | 39 | 79.6 | 3 | 60.0 |
| Cefalotin | 48 | 98.0 | 5 | 100.0 |
| Ceftiofur | 47 | 95.9 | 5 | 100.0 |
| Cefuroxime | 48 | 98.0 | 5 | 100.0 |
| Ceftazidime | 45 | 91.8 | 5 | 100.0 |
| Cefquinome | 48 | 98.0 | 4 | 80.0 |
| Cefepime | 44 | 89.8 | 4 | 80.0 |
| Cefoxitin | 41 | 83.7 | 3 | 60.0 |
| Ertapenem 3 | 32 | 65.3 | 2 | 40.0 |
| Streptomycin | 6 | 12.2 | 4 | 80.0 |
| Kanamycin | 43 | 87.8 | 4 | 80.0 |
| Gentamicin | 32 | 65.3 | 3 | 60.0 |
| Tobramycin | 39 | 79.6 | 4 | 80.0 |
| Netilmicin | 38 | 77.6 | 4 | 80.0 |
| Apramycin | 0 | 0.0 | 0 | 0.0 |
| Amikacin | 10 | 20.4 | 2 | 40.0 |
| Tetracycline | 33 | 67.3 | 2 | 40.0 |
| Chloramphenicol | 18 | 36.7 | 1 | 20.0 |
| Florfenicol | 0 | 0.0 | 1 | 20.0 |
| Colistin 4 | 6 | 12.2 | 0 | 0.0 |
| Sulfonamides | 41 | 83.7 | 5 | 100.0 |
| Trimethoprim | 37 | 75.5 | 4 | 80.0 |
| Nalidixic acid | 42 | 85.7 | 2 | 40.0 |
| Enrofloxacin | 42 | 85.7 | 2 | 40.0 |
| blaCTX-M group 1 | blaCTX-M group 9 | blaCTX-M group 1 + 9 | blaSHV-12 | blaOXA-48-like | blaNDM-like | blaKPC-like | blaCMY-like | Total | |
|---|---|---|---|---|---|---|---|---|---|
| K. pneumoniae | 36 | 24 | 6 | 1 | 21 | 21 | 5 | 1 | 115 |
| E. coli | 2 | 0 | 0 | 0 | 0 | 3 | 0 | 3 | 8 |
| Isolate | Species | ST | Long-Read Contig | Beta-Lactam Resistance Gene | Additional Resistance Genes | Replicon Type | Size (bp) |
|---|---|---|---|---|---|---|---|
| 59825 | K. pneumoniae | 17 | contig 2 contig 3 | CTX-M-15 NDM-1, CTX-M-15 | TEM-1, SCO-1, aadA, aac(3)-IIa, aph(6)-Id, sul2, dfrA15, tet(A) TEM-1, OXA-1, aac(6′)-Ib-cr, aac(3)-Iia, qnrB1, | IncFIBk IncFIIk, IncFIB (pQil) | 253,391 128,170 |
| 60783 | K. pneumoniae | 147 | contig 2 | OXA-48 | none | IncL | 63,600 |
| contig 3 | NDM-1, CTX-M-15 | aac(6′)-Ib-cr, aph(3′)-VI, qnrS1, sul1, OXA-1, catB3 | IncFIB (pQil) | 54,050 | |||
| 60798 | K. pneumoniae | 383 | contig 2 | NDM-5, CTX-M-15 | armA, aph(3′)-VI, aac(6′)-Ib, aadA1, qnrS1, sul1, sul2, dfrA5 | IncFIB/IncHI2 | 361,000 |
| contig 3 | OXA-48, CTX-M-14 | aph(6)-Id, aph(3″)-Ib | IncL | 59,000 | |||
| 60802 | K. pneumoniae | 11 | contig 3 | KPC-2, SHV-12, CTX-M-65 | fosA3 | IncF/IncR | 126,000 |
| 60726 | E. coli | 349 | contig 2 contig 3 | CMY-6 NDM-1 | aac(6′)-Ib3, rmtC, aac(6′)-Ib-cr, sul1 none | IncC No hit found | 127,679 9924 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elgriw, N.; Métayer, V.; Drapeau, A.; François, P.; Azaiez, S.; Mastouri, M.; Rhim, H.; Elzagheid, A.; Soufiyah, N.; Madec, J.-Y.; et al. Clonal, Plasmidic and Genetic Diversity of Multi-Drug-Resistant Enterobacterales from Hospitalized Patients in Tripoli, Libya. Antibiotics 2023, 12, 1430. https://doi.org/10.3390/antibiotics12091430
Elgriw N, Métayer V, Drapeau A, François P, Azaiez S, Mastouri M, Rhim H, Elzagheid A, Soufiyah N, Madec J-Y, et al. Clonal, Plasmidic and Genetic Diversity of Multi-Drug-Resistant Enterobacterales from Hospitalized Patients in Tripoli, Libya. Antibiotics. 2023; 12(9):1430. https://doi.org/10.3390/antibiotics12091430
Chicago/Turabian StyleElgriw, Nada, Véronique Métayer, Antoine Drapeau, Pauline François, Sana Azaiez, Maha Mastouri, Hajer Rhim, Adam Elzagheid, Najeeb Soufiyah, Jean-Yves Madec, and et al. 2023. "Clonal, Plasmidic and Genetic Diversity of Multi-Drug-Resistant Enterobacterales from Hospitalized Patients in Tripoli, Libya" Antibiotics 12, no. 9: 1430. https://doi.org/10.3390/antibiotics12091430
APA StyleElgriw, N., Métayer, V., Drapeau, A., François, P., Azaiez, S., Mastouri, M., Rhim, H., Elzagheid, A., Soufiyah, N., Madec, J. -Y., Chaouch, C., Mansour, W., & Haenni, M. (2023). Clonal, Plasmidic and Genetic Diversity of Multi-Drug-Resistant Enterobacterales from Hospitalized Patients in Tripoli, Libya. Antibiotics, 12(9), 1430. https://doi.org/10.3390/antibiotics12091430