Antimicrobial Susceptibility Testing for Corynebacterium Species Isolated from Clinical Samples in Romania

 , and
, and 
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Bacterial Strains
4.2. Antimicrobial Susceptibility Testing
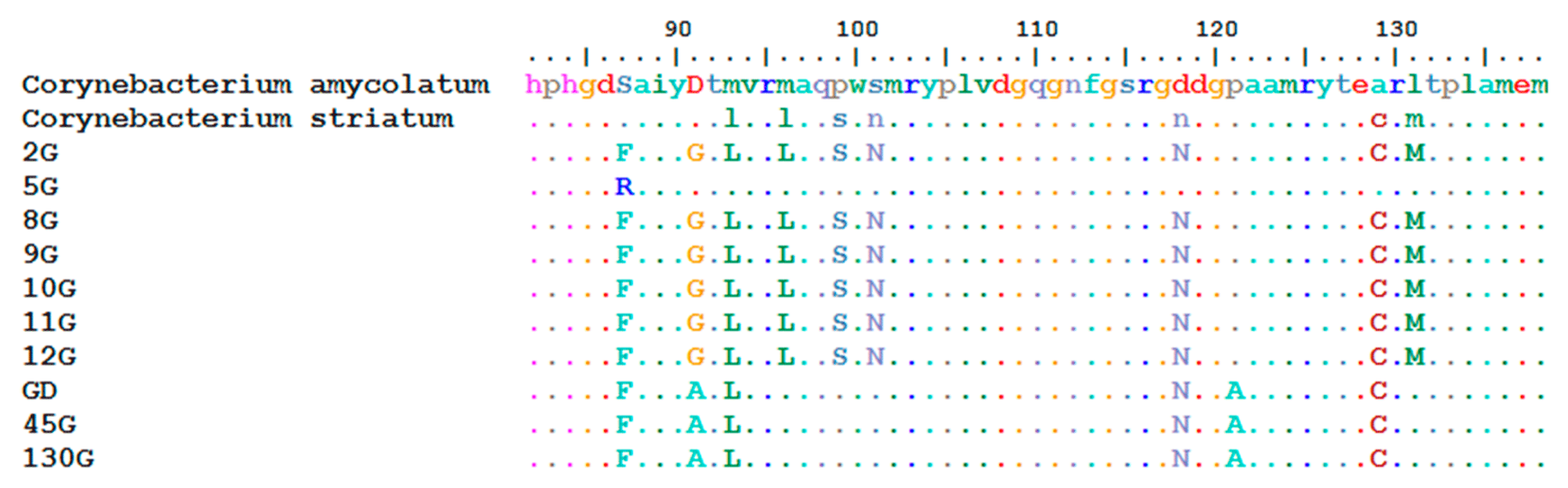
4.3. PCR Amplification of gyrA Gene
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zasada, A.A.; Mosiej, E. Contemporary microbiology and identification of Corynebacteria spp. causing infections in human. Lett. Appl. Microbiol. 2018, 66, 472–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funke, G.; von Graevenitz, A.; Clarridge, J.E.; Bernard, K.A. Clinical Microbiology of Coryneform Bacteria. Clin. Microbiol. Rev. 1997, 10, 125–159. [Google Scholar] [CrossRef] [PubMed]
- Dalal, A.; Urban, C.; Segal-Maurer, S. Endocartidis due to Corynebacterium amycolatum, Case report. J. Med. Microbiol. 2008, 57, 1299–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, S.; Kim, H.; Lee, Y.; Kim, S. Bacteriemia caused by Corynebacterium amycolatum with a novel mutation in gyrA gene that confers high-level quinolone resistance. Korean J. Lab. Med. 2011, 31, 47–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belmares, J.; Detterline, S.; Pak, J.B.; Parada, J.P. Corynebacterium endocarditis species-specific risk factors and outcomes. BMC Infect. Dis. 2007, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soriano, F.; Zapardiel, J.; Nieto, E. Antimicrobial susceptibilities of Corynebacterium species and other non-spore-forming gram-positive bacilli to 18 antimicrobial agents. Antimicrob. Agents Chemother. 1995, 39, 208–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos, J.N.; Souza, C.; Faria, Y.V.; da Silva, E.C.; Veras, J.F.C.; Baio, P.V.P.; Seabra, S.H.; de Oliveira Moreira, L.; Hirata Júnior, R.; Mattos-Guaraldi, A.L.; et al. Bloodstream and catheter-related infections due to different clones of multidrug-resistant and biofilm producer Corynebacterium striatum. BMC Infect. Dis. 2019, 19, 672. [Google Scholar] [CrossRef]
- Syed, M.A.; Ashcherkin, N.; Sundhu, M.; Hakam, L.; Gul, S. Recurrent Bacteremia with Corynebacterium striatum After Prosthetic Valve Replacement: A Case Report. Cureus 2019, 11, e4670. [Google Scholar] [CrossRef] [Green Version]
- Elkayam, N.; Urazov, A.; Tuneev, K.; Chapnick, E. Corynebacterium striatum bacteremia associated with cellulitis in a patient with cirrhosis. IDCases 2019, 17, e00575. [Google Scholar] [CrossRef]
- Dominguez-Gill, B.; Herrero, J.C.; Carreno, A.; Morales, E.; Andres, A.; Aguado, J.M.; Diaz-Gonzales, R.; Benito, A.; Morales, J.M. Ureteral stenosis secondary encrustation by urea-splitting Corynebacterium urealyticum in a kidney transplant patient. Nephrol. Dial. Transplant. 1999, 14, 977–978. [Google Scholar] [CrossRef] [Green Version]
- Soriano, F.; Fernández-Roblas, R. Infections caused by antibiotic-resistant Corynebacterium group D2. Eur. J. Clin. Microbiol. Infect. Dis. 1988, 7, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Chomarat, M.; Breton, P.; Dubost, J. Osteomyelitis due to Corynebacterium group D2. Eur. J. Clin. Microbiol. Infect. Dis. 1991, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Natal, I.; Guerra, J.; Alcoba, M.; Cachón, F.; Soriano, F. Bacteremia caused by multiply resistant Corynebacterium urealyticum: six case reports and review. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 514–517. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.D.; Abdur Rahman, M.; Saul, Z. Acase of recurrent Corynebacterium jeikeium endocarditis: Unanswered questions for the treatment of chronic endovascular infections. IDCases 2019, 18, e00610. [Google Scholar] [CrossRef] [PubMed]
- Saavedra, J.; Rodriguez, J.N.; Fernandez-Jurado, A.; Vega, M.D.; Pascual, L.; Prados, D. A Necrotic Soft-Tissue Lesion Due to Corynebacterium urealyticum in a Neutropenic Child. Clin. Infect. Dis. 1996, 22, 851–852. [Google Scholar] [CrossRef] [Green Version]
- Nieto, E.; Vindel, A.; Valero-Guillen, P.L.; Saez-Nieto, J.A.; Soriano, F. Biochemical, antimicrobial susceptibility and genotyping studies on Corynebacterium urealyticum isolates from diverse sources. J. Med. Microbiol. 2000, 49, 759–763. [Google Scholar] [CrossRef] [Green Version]
- Minkin, R.; Shapiro, J.M. Corynebacterium afermentans Lung Abscess and Empyema in a Patient with Human Immunodeficiency Virus Infect. South. Med. J. 2004, 97, 395–397. [Google Scholar] [CrossRef]
- Andavolu, R.H.; Jagadha, V.; Lue, Y.; McLean, T. Lung abscess involving Corynebacterium pseudodiphtheriticum in a patient with AIDS-related complex. N. Y. State J. Med. 1986, 86, 594–596. [Google Scholar]
- Chiner, E.; Arriero, J.M.; Signes-Costa, J.; Marco, J.; Corral, J.; Gomez-Esparrago, A.; Ortiz de la Tabla, V.; Martin, C. Corynebacterium pseudodiphtheriticum pneumonia in an immunocompetent patient. Monaldi Arch. Chest. Dis. 1999, 54, 325–327. [Google Scholar]
- Morris, A.; Guild, I. Endocarditis due to Corynebacterium pseudodiphtheriticum: five case reports, review and antibiotic susceptibilities of nine strains. Rev. Infect. Dis. 1991, 13, 887–892. [Google Scholar] [CrossRef]
- Dragomirescu, C.C.; Lixandru, B.E.; Coldea, I.L.; Palade, A.M.; Baltoiu, M.; Dinu, S.; Cristea, V.C.; Manolescu, L.; Popa, M.I. Comparative analysis of different phenotypic and molecular methods used for the taxonomic identification of Corynebacterium spp. isolated from clinical samples in Romania. Rom. Biotechnol. Lett. 2017, 22, 12926–12933. [Google Scholar]
- Hahn, W.O.; Werth, B.J.; Butler-Wu, S.M.; Rakita, R.M. Multidrug-resistant Corynebacterium striatum associated with increased use of parenteral antimicrobial drugs. Emerg. Infect. Dis. 2016, 22, 1908–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manolescu, L.S.C.; Boeru, C.; Căruntu, C.; Dragomirescu, C.C.; Goldis, M.; Jugulete, G.; Marin, M.; Popa, G.L.; Preda, M.; Radu, M.C.; et al. A Romanian experience of syphilis in pregnancy and childbirth. Midwifery 2019, 78, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Marinescu, P.; Manolescu, L.S.C. Association of hepatitis B infection in patients with HIV Encephalopathy. Rom. Biotechnol. Lett. 2012, 17, 7817–7824. [Google Scholar]
- FitzGerald, R.P.; Rosser, A.J.; Perera, D.N. Nontoxigenic penicillin-resistant cutaneous C. diphtheriae infection: a case report and review of the literature. J. Infect. Public Health 2015, 8, 98–100. [Google Scholar] [CrossRef] [Green Version]
- Rudresh, S.M.; Ravi, G.S.; Alex, A.M.; Mamatha, K.R.; Sunitha, L.; Ramya, K.T. Non Diphtheritic Corynebacteria: An Emerging Nosocomial Pathogen in Skin and Soft Tissue Infection. J. Clin. Diagn. Res. 2015, 9, DC19–DC21. [Google Scholar] [CrossRef]
- De Miguel-Martinez, I.; Fernández-Fuertes, F.; Ramos-Macías, A.; Bosch-Benitez, J.M.; Martín-Sánchez, A.M. Sepsis due to multiply resistant Corynebacteriu mamycolatum. Eur. J. Clin. Microbiol. Infect. Dis. 1996, 15, 617–618. [Google Scholar] [CrossRef]
- Alibi, S.; Ferjani, A.; Boukadida, J.; Cano, M.E.; Fernández-Martínez, M.; Martínez-Martínez, L.; Navas, N. Occurrence of Corynebacterium striatum as an emerging antibioticresistant nosocomial pathogen in a Tunisian hospital. Sci. Rep. 2017, 7, 9704. [Google Scholar] [CrossRef] [Green Version]
- Coman, G.; Brumariu, O.; Petraru, E.; Cucer, F.; Munteanu, M. Corynebacterium urealyticum in urinary infections in children. Bacteriol. Virusol. Parazitol. Epidemiol. 1998, 43, 47–51. [Google Scholar]
- Diculencu, D.; Aramă, S.; Răutu, F.; Coman, G. Empyema caused by Corynebacterium striatum. Pneumoftiziologia 1998, 47, 37–39. [Google Scholar]
- Serban, R.I.; Dan, M.; Pânzaru, C.V.; Anghel, D.; Dăscălescu, D.M.; Ciucu, L.; Serban, I.; Tinică, G. Etiology of ventilator-associated pneumonia at the Cardiovascular Surgery Clinic of Iaşi. Rev. Med. Chir. Soc. Med. Nat. Iasi 2012, 116, 15–21. [Google Scholar] [PubMed]
- Sierra, J.M.; Martinez-Martinez, L.; Vazquez, F.; Giralt, E.; Vila, J. Relationship between Mutations in the gyrA Gene and Quinolone Resistance in Clinical Isolates of Corynebacterium striatum and Corynebacterium amycolatum. Antimicrob. Agents Chemother. 2005, 49, 1714–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical and Laboratory Standards Institute (CLSI). Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria. Propos. Guidel. M45-A2 2012, 30, 18. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically, 7th ed.; Approv. Stand. M7-A7; CLSI: Wayne, PA, USA, 2006; Volume 26, p. 2. [Google Scholar]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 4.0. 2014. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/Breakpoint_table_v_4.0.pdf (accessed on 16 October 2019).
- Suciu, G.; Suciu, V.; Martian, A.; Craciunescu, R.; Vulpe, A.; Marcu, I.; Halunga, S.; Fratu, O. Big data, internet of things and cloud convergence–an architecture for secure e-health applications. J. Med. Syst. 2015, 39, 141. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No. | Sample | Species | P | CXM | CRO | E | CN | C | CIP | RA | TE | VA | TEC | DA | LNZ |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1/2G | Blood culture I | C. amycolatum | R | R | R | R | R | S | R | R | R | S | S | R | S |
| 2 | Blood culture II | C. afermentans | R | R | R | R | S | R | R | R | R | S | S | R | S |
| 3 | Blood culture III | C. afermentans | R | R | R | R | S | R | R | R | R | S | S | R | S |
| 4/5G | Blood culture IV | C. striatum | R | R | R | R | R | R | R | R | R | S | S | R | S |
| 5/GD | Blood culture V | C. striatum | R | R | R | R | R | R | R | R | R | S | S | R | S |
| 6/8G | Blood culture VI | C. amycolatum | R | R | R | R | S | R | R | R | R | S | S | R | S |
| 7/9G | Peritoneal fluid I | C. amycolatum | R | R | R | R | R | R | R | S | R | S | S | R | S |
| 8/10G | Peritoneal fluid II | C. amycolatum | R | R | R | S | R | R | R | R | R | S | S | S | S |
| 9/45G | Catheter | C. striatum | R | R | R | R | R | R | R | R | R | S | S | R | S |
| 10/11G | Osteomyelitis | C. amycolatum | R | R | R | R | S | R | R | R | R | S | S | R | S |
| 11/12G | Perirectal abcess | C. amycolatum | R | R | R | R | R | R | R | R | R | S | S | S | S |
| 12 | Urine I | C. urealyticum | S | S | S | S | R | S | S | S | S | S | S | R | S |
| 13 | Urine II | C. amycolatum | R | R | R | R | R | R | R | S | R | S | S | S | S |
| 14 | Urine III | C. urealyticum | R | R | R | R | R | R | R | R | R | S | S | R | S |
| 15/130G | Wound I | C. striatum | S | S | S | S | S | R | S | S | S | S | S | S | S |
| 16 | Wound II | C. striatum | R | R | R | R | R | R | R | R | R | S | S | R | S |
| 17 | Wound III | C. urealyticum | R | R | R | R | R | R | R | R | R | S | S | R | S |
| 18 | Wound IV | C. striatum | R | R | R | R | R | R | R | R | R | S | S | R | S |
| 19 | Wound V | C. striatum | R | R | R | R | R | R | R | R | R | S | S | R | S |
| 20 | Conjunctival secretion | C. pseudodiphtheriticum | S | S | S | S | S | S | S | S | S | S | S | S | S |
| Antibiotic | MIC (µg/mL) Criteria for the Interpretation of Antimicrobial Activity | Minimal Concentration (µg/mL) | Maximal Concentration (µg/mL) | ||
|---|---|---|---|---|---|
| S µg/mL | I µg/mL | R µg/mL | µg/mL | µg/mL | |
| Penicillin G | ≤1 | 2 | ≥4 | 0.25 | 8 |
| Cefuroxime | ≤1 | 2 | ≥4 | 0.25 | 8 |
| Ceftriaxone | ≤1 | 2 | ≥4 | 0.25 | 8 |
| Erythromycin | ≤0.5 | 1 | ≥2 | 0.12 | 4 |
| Gentamicin | ≤4 | 8 | ≥16 | 1 | 32 |
| Ciprofloxacin | ≤1 | 2 | ≥4 | 0.25 | 8 |
| Tetracycline | ≤4 | 8 | ≥16 | 1 | 32 |
| Rifampin | ≤1 | 2 | ≥4 | 0.25 | 8 |
| Chloramphenicol | ≤8 | - | ≥8 | 1 | 32 |
| Vancomycin | ≤4 | - | - | 0.25 | 8 |
| Teicoplanin | ≤8 | 16 | ≥32 | 0.16 | 258 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dragomirescu, C.C.; Lixandru, B.E.; Coldea, I.L.; Corneli, O.N.; Pana, M.; Palade, A.M.; Cristea, V.C.; Suciu, I.; Suciu, G.; Manolescu, L.S.C.; et al. Antimicrobial Susceptibility Testing for Corynebacterium Species Isolated from Clinical Samples in Romania. Antibiotics 2020, 9, 31. https://doi.org/10.3390/antibiotics9010031
Dragomirescu CC, Lixandru BE, Coldea IL, Corneli ON, Pana M, Palade AM, Cristea VC, Suciu I, Suciu G, Manolescu LSC, et al. Antimicrobial Susceptibility Testing for Corynebacterium Species Isolated from Clinical Samples in Romania. Antibiotics. 2020; 9(1):31. https://doi.org/10.3390/antibiotics9010031
Chicago/Turabian StyleDragomirescu, Cristiana Cerasella, Brandusa Elena Lixandru, Ileana Luminita Coldea, Olguta Nicoleta Corneli, Marina Pana, Andi Marian Palade, Violeta Corina Cristea, Ioana Suciu, George Suciu, Loredana Sabina Cornelia Manolescu, and et al. 2020. "Antimicrobial Susceptibility Testing for Corynebacterium Species Isolated from Clinical Samples in Romania" Antibiotics 9, no. 1: 31. https://doi.org/10.3390/antibiotics9010031
APA StyleDragomirescu, C. C., Lixandru, B. E., Coldea, I. L., Corneli, O. N., Pana, M., Palade, A. M., Cristea, V. C., Suciu, I., Suciu, G., Manolescu, L. S. C., Popa, L. G., & Popa, M. I. (2020). Antimicrobial Susceptibility Testing for Corynebacterium Species Isolated from Clinical Samples in Romania. Antibiotics, 9(1), 31. https://doi.org/10.3390/antibiotics9010031