Actinomycosis of the Tongue: A Case Report and Review of Literature

 ,
, 
Abstract
:1. Introduction
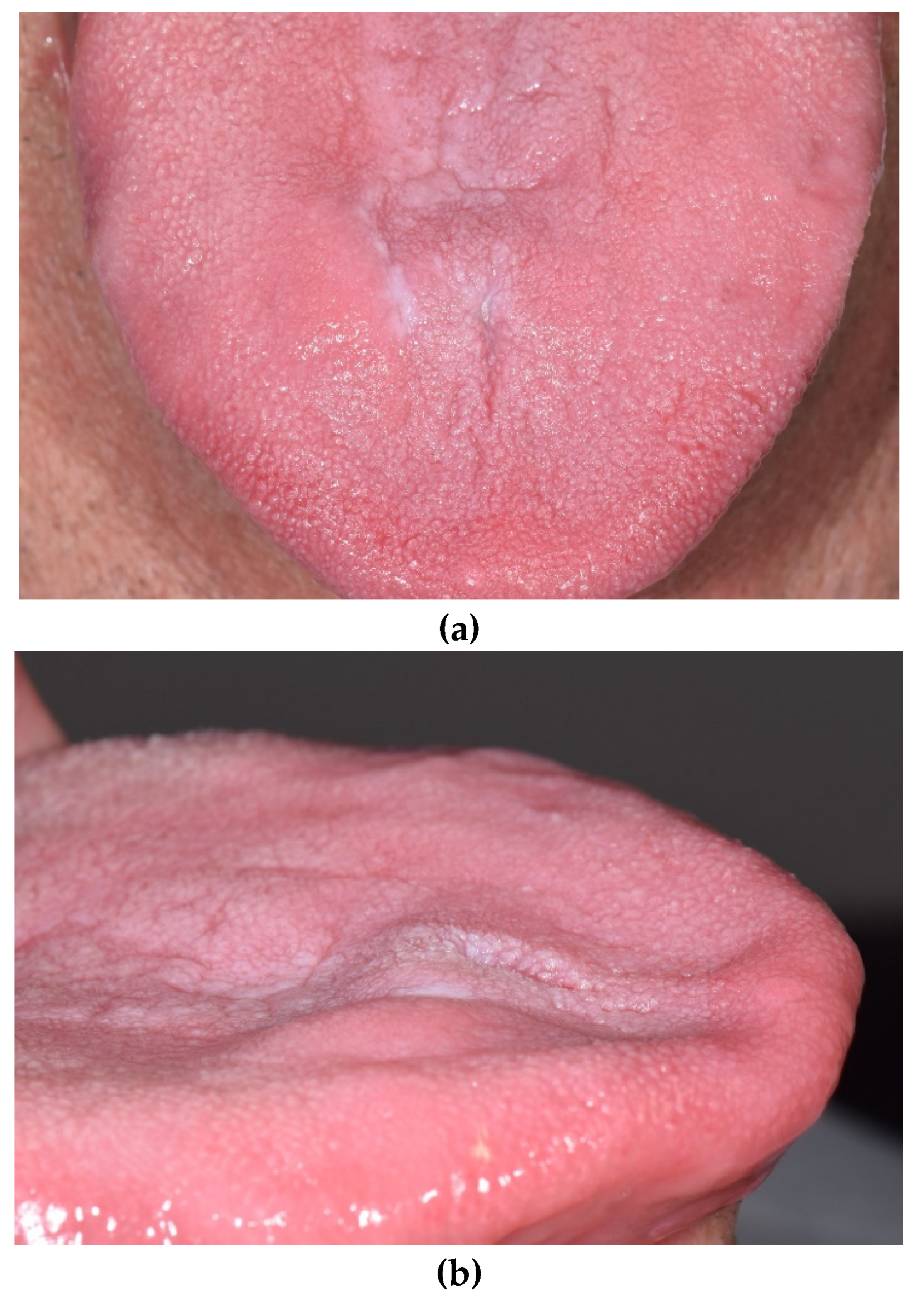
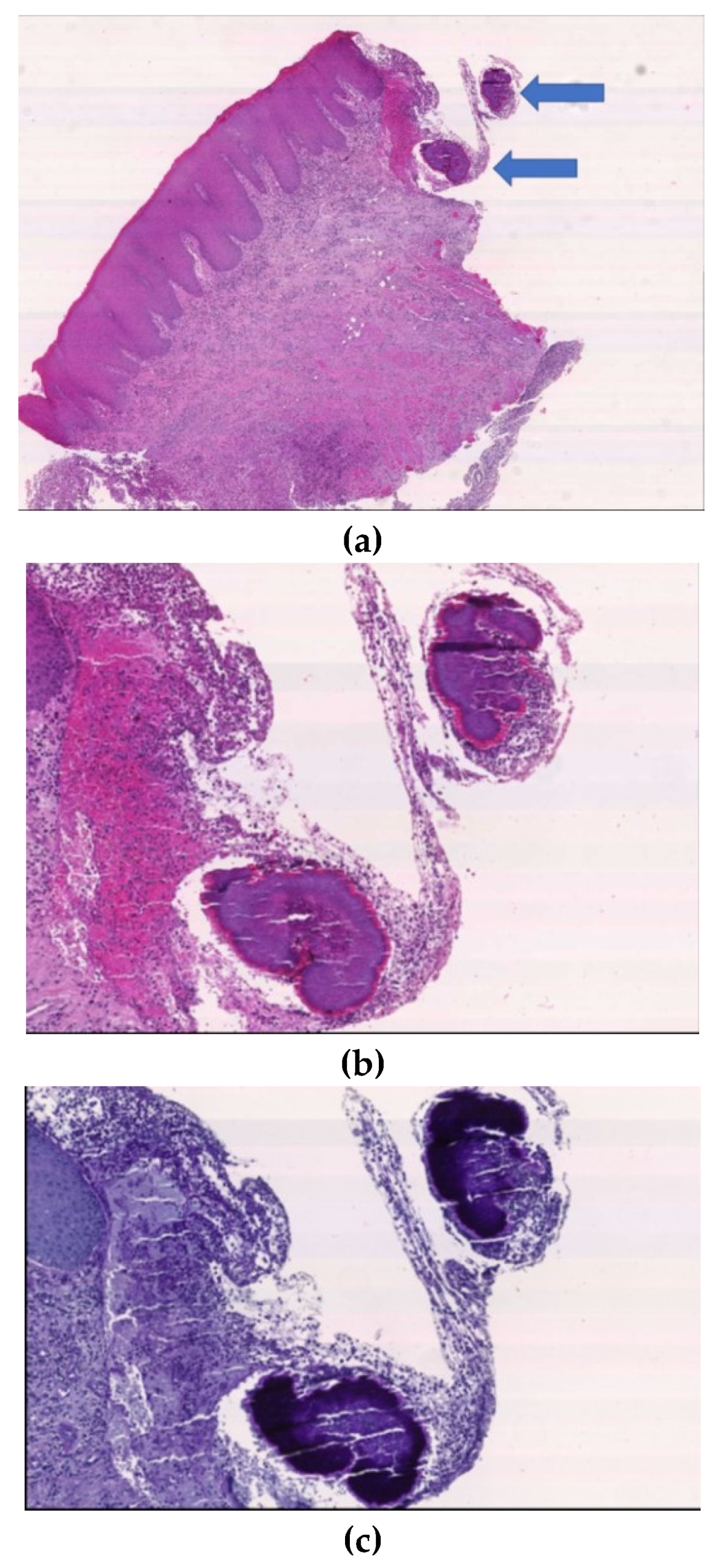
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bronner, M.; Bronner, M. Actinomycosis, 2nd ed.; J. Wright & Son Ltd.: Bristol, UK, 1971. [Google Scholar]
- Valour, F.; Senechal, A. Actinomycosis: Etiology, clinical features, diagnosis, treatment, and management. Infect. Drug Resist. 2014, 7, 183–197. [Google Scholar] [PubMed] [Green Version]
- Lancella, A.; Abbate, G.; Foscolo, A.M.; Dosdegani, R. Two unusual presentations of cervicofacial actinomycosis and review of the literature. Acta Otorhinolaryngol. Ital. 2008, 28, 89–93. [Google Scholar] [PubMed]
- Gerbino, G.; Bernardi, M.; Secco, F.; Sapino, A.; Pacchioni, D. Actinomycosis of the tongue: Report of two cases and review of the literature. Minerva Stomatol. 1998, 47, 95–101. [Google Scholar] [PubMed]
- Cameron, O.J. Primary actinomycosis of the tongue with a report of two cases. J. Am. Med. Assoc. 1932, 99, 1146–1150. [Google Scholar] [CrossRef]
- Kuepper, R.C.; Harrigan, W.F. Actinomycosis of the tongue: Report of case. J. Oral Surg. 1979, 37, 123–125. [Google Scholar]
- Atespare, A.; Keskin, G.; Ercin, C.; Keskin, S.; Camcioglu, A. Actinomycosis of the tongue: A diagnostic dilemma. J. Laryngol. Otol. 2006, 120, 681–683. [Google Scholar] [CrossRef]
- Bennhoff, F. Actinomycosis: Diagnostic and therapeutic considerations and a review of 32 cases. Laryngoscope 1984, 94, 1198–1217. [Google Scholar] [CrossRef]
- Kobayashi, G.S. Actinomycetes: The fungus-like bacteria. In Micro-Biology, 4th ed.; Davis, B.D., Dulbecco, R., Eisen, H.N., Ginsberg, H.S., Eds.; JB Lippincott: Philadelphia, PA, USA, 1990; pp. 665–671. [Google Scholar]
- Reichenbach, J.; Lopatin, U.; Mahlaoui, N.; Beovic, B.; Siler, U.; Zbinden, R.; Seger, R.A.; Galmiche, L.; Brousse, N.; Kayal, S.; et al. Actinomyces in chronic granulomatous disease: An emerging and unanticipated pathogen. Clin. Infect. Dis. 2009, 49, 1703–1710. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.; Haddad, A.J. Cervicofacial actinomycosis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 496–508. [Google Scholar] [CrossRef] [Green Version]
- Pulverer, G.; Schutt-Gerowitt, H.; Schaal, K.P. Human cervicofacial actinomycosis: Microbiological data for 1997 cases. Clin. Infect. Dis. 2003, 37, 490–497. [Google Scholar] [CrossRef]
- Sudhakar, S.S.; Ross, J.J. Short-term treatment of actinomycosis: Two cases and a review. Clin. Infect. Dis. 2004, 38, 444–447. [Google Scholar] [CrossRef] [Green Version]
- Chaudhry, S.I.; Greenspan, J.S. Actinomycosis in HIV infection: A review of a rare complication. Int. J. STD AIDS 2000, 11, 349–355. [Google Scholar] [CrossRef]
- Park, J.K.; Lee, H.K.; Ha, H.K.; Choi, H.Y.; Choi, C.G. Cervicofacial actinomycosis: CT and MR imaging findings in seven patients. Am. J. Neuroradiol. 2003, 24, 331–335. [Google Scholar]
- Volante, M.; Contucci, A.M.; Fantoni, M.; Ricci, R.; Galli, J. Cervicofacial actinomycosis: Still a difficult differential diagnosis. Acta Otorhinolaryngol. Ital. 2005, 25, 116–119. [Google Scholar]
- Balatsouras, D.G.; Kaberos, A.K.; Eliopoulos, P.N.; Kandiloros, D.; Economou, C.N. Cervicofacial actinomycosis presenting as an acute upper respiratory tract obstruction. J. Laryngol. Otol. 1994, 108, 801–803. [Google Scholar] [CrossRef]
- Ahmed, S.; Ali, M.; Adegbite, N.; Vaidhyanath, R.; Avery, C. Actinomycosis of tongue: Rare presentation mimicking malignancy with literature review and imaging features. Radiol. Case Rep. 2018, 14, 190–194. [Google Scholar] [CrossRef]
- Brignall, I.D.; Gilhooly, M. Actinomycosis of the tongue. A diagnostic dilemma. Br. J. Oral Maxillofac. Surg. 1989, 27, 249–253. [Google Scholar] [CrossRef]
- Sodagar, R.; Kohout, E. Actinomycosis of tongue as pseudotumor. Laryngoscope 1972, 82, 2149–2152. [Google Scholar] [CrossRef]
- Isalska, B.J.; Habashi, S.; Stanbridge, T.N. Actinomycosis of the tongue. J. Infect. 1991, 22, 201. [Google Scholar] [CrossRef]
- Kurtaran, H.; Ugur, K.S.; Ark, N.; Vuran, O.; Gunduz, M. Tongue abscess with actinomycosis. J. Craniofac. Surg. 2011, 22, 1107–1109. [Google Scholar] [CrossRef]
- Escoda, M.; Gardiello, M.; Muntané, M.J. Painful tongue ulcers. Actas Dermosifiliogr. 2013, 104, 77–78. [Google Scholar] [CrossRef]
- Sadeghi, S.; Azaïs, M.; Ghannoum, J. Actinomycosis Presenting as Macroglossia: Case Report and Review of Literature. Head Neck Pathol. 2019, 13, 327–330. [Google Scholar] [CrossRef]
- Uhler, I.V.; Dolan, L.A. Actinomycosis of the tongue. Oral Surg. Oral Med. Oral Pathol. 1972, 34, 199–200. [Google Scholar] [CrossRef]
- Rocha, O.K.M.S.; de França, G.M.; Oliveira, P.T.; Santos, J.L.M.; Miguel, M.C.C.; Silveira, É.J.D. Unusual presentation of oral actinomycosis in the tongue: Case report. J. Bras. Patol. Med. Lab. 2017, 53, 330–333. [Google Scholar] [CrossRef]
- Jat, P.S.; Paulose, A.A.; Agarwal, S. Lingual actinomycosis, an uncommon diagnosis of tongue lesions: A case report and review of literature. Ann. Clin. Case Rep. 2017, 2, 1381. [Google Scholar]
- Aneja, T.; Bhat, N.; Chawla, G.; Negi, M. Actinomycosis of tongue: Case report of an atypical presentation. IOSR J. Dental Med. Sci. 2017, 16, 84–86. [Google Scholar]
- Vazquez, A.M.; Marti, C.; Renaga, I.; Salavert, A. Actinomycosis of the tongue associated with human immunodeficiency virus infection: Case report. J. Oral Maxillofac. Surg. 1997, 55, 879–881. [Google Scholar] [CrossRef]
- Ficarra, G.; Di Lollo, S.; Pierleoni, F.; Panzoni, E. Actinomycosis of the tongue: A diagnostic challenge. Head Neck 1993, 15, 53–55. [Google Scholar] [CrossRef]
- Habibi, A.; Salehinejad, J.; Saghafi, S.; Melati, E.; Habibi, M. Actinomycosis of the tongue. Arch. Iran. Med. 2008, 11, 566–568. [Google Scholar]
- Smith, A.J.; Hall, V.; Thakker, B.; Gemmell, C.G. Antimicrobial susceptibility testing of Actinomyces species with 12 antimicrobial agents. J. Antimicrob. Chemother. 2005, 56, 407–409. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Reference | Oral Site (Number of Patients) | Clinical Appearance | Symptoms | Triggering Factors | Other Associated Signs | Treatment |
|---|---|---|---|---|---|---|
| SADEGHI, 2018 [24] | Tongue | Macroglossia | No | No | Dysphagia and speech impairment | Penicillin for 22 weeks |
| ANEJA, 2017 [28] | Tongue | Nodular mass | No | Tongue bite one month before | Difficulty in speech | Excision and amoxicillin–clavulanic acid for 2 weeks |
| JAT, 2017 [27] | Tongue | Nodular mass | No | No | Poor oral hygiene and dental caries | Excision. Doxycycline for 3 weeks |
| ROCHA, 2017 [26] | Tongue | Necrotic tissue with purulent right lateral tongue developed after sclerosing agent injection to treat vascular lesion | No | No | No | Local debridement |
| ESCODA, 2013 [23] | Tongue | Two ulcerated lesions | Pain | No | Erosive lichen asymptomatic | Clyndamicin (unknown posology) and chlorhexidine digluconate for 1 month |
| KURTARAN, 2011 [22] | Tongue | Solid mass | Pain | Dental prosthesis problem 1 month before | Dysphagia and speech impairment | Excision and combination of amoxicillin-clavulanic acid and metronidazole for 5 weeks |
| HABIBI, 2008 [31] | Tongue | Solid mass | No | Tongue bite | No | Excision and intravenus penicillin for 3 weeks |
| ATESPARE, 2006 [7] | Tongue | solid mass | No | No | Speech disturbance | Excision and amoxicillin-clavulanic acid for 3 weeks |
| VAZQUEZ, 1997 [29] | Tongue | Swelling | No | No | No | Amoxicillin for 4 weeks |
| GERBINO, 1996 [4] | Tongue (n = 2) | Nodules | NA | NA | NA | Penicillin V for 1 month |
| FICARRA, 1993 [31] | Tongue | Swelling | No | No | No | Penicillin for 2 weeks |
| ISALSKA, 1991 [21] | Tongue | Swelling | Local discomfort | No | No | Amoxycillin for 6 month |
| BRIGNALL, 1989 [19] | Tongue | Swelling | Acute discomfort | Accidental self-inflicted bite to the tongue 6 months previously | Lost normal movement and dysphagia | Henoxy-methyl-penicillin for 3 month |
| KUEPPER, 1979 [6] | Tongue | Mass | NA | NA | NA | Penicillin for 1 month |
| UHLER, 1972 [25] | Tongue | Nodular mass | NA | NA | NA | Excision and penicillin for 6 months |
| SODAGAR, 1972 [20] * | Tongue | Solid mass | NA | NA | NA | Excision |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Amore, F.; Franchini, R.; Moneghini, L.; Lombardi, N.; Lodi, G.; Sardella, A.; Varoni, E.M. Actinomycosis of the Tongue: A Case Report and Review of Literature. Antibiotics 2020, 9, 124. https://doi.org/10.3390/antibiotics9030124
D’Amore F, Franchini R, Moneghini L, Lombardi N, Lodi G, Sardella A, Varoni EM. Actinomycosis of the Tongue: A Case Report and Review of Literature. Antibiotics. 2020; 9(3):124. https://doi.org/10.3390/antibiotics9030124
Chicago/Turabian StyleD’Amore, Fiorella, Roberto Franchini, Laura Moneghini, Niccolò Lombardi, Giovanni Lodi, Andrea Sardella, and Elena M. Varoni. 2020. "Actinomycosis of the Tongue: A Case Report and Review of Literature" Antibiotics 9, no. 3: 124. https://doi.org/10.3390/antibiotics9030124
APA StyleD’Amore, F., Franchini, R., Moneghini, L., Lombardi, N., Lodi, G., Sardella, A., & Varoni, E. M. (2020). Actinomycosis of the Tongue: A Case Report and Review of Literature. Antibiotics, 9(3), 124. https://doi.org/10.3390/antibiotics9030124