High-Value Plant Species Used for the Treatment of “Fever” by the Karen Hill Tribe People



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
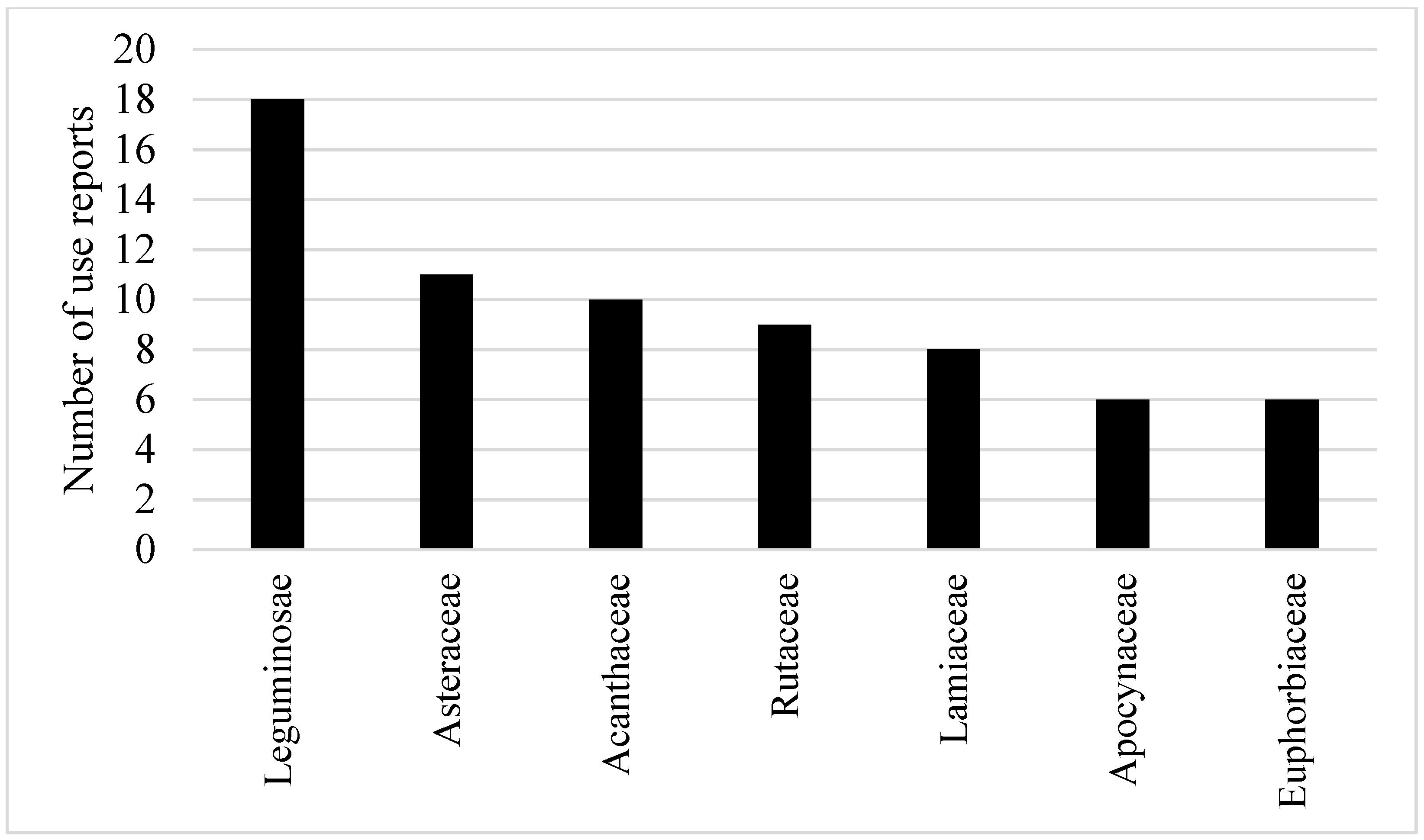
2. Results
3. Discussion
3.1. Ethnobotanical Significance
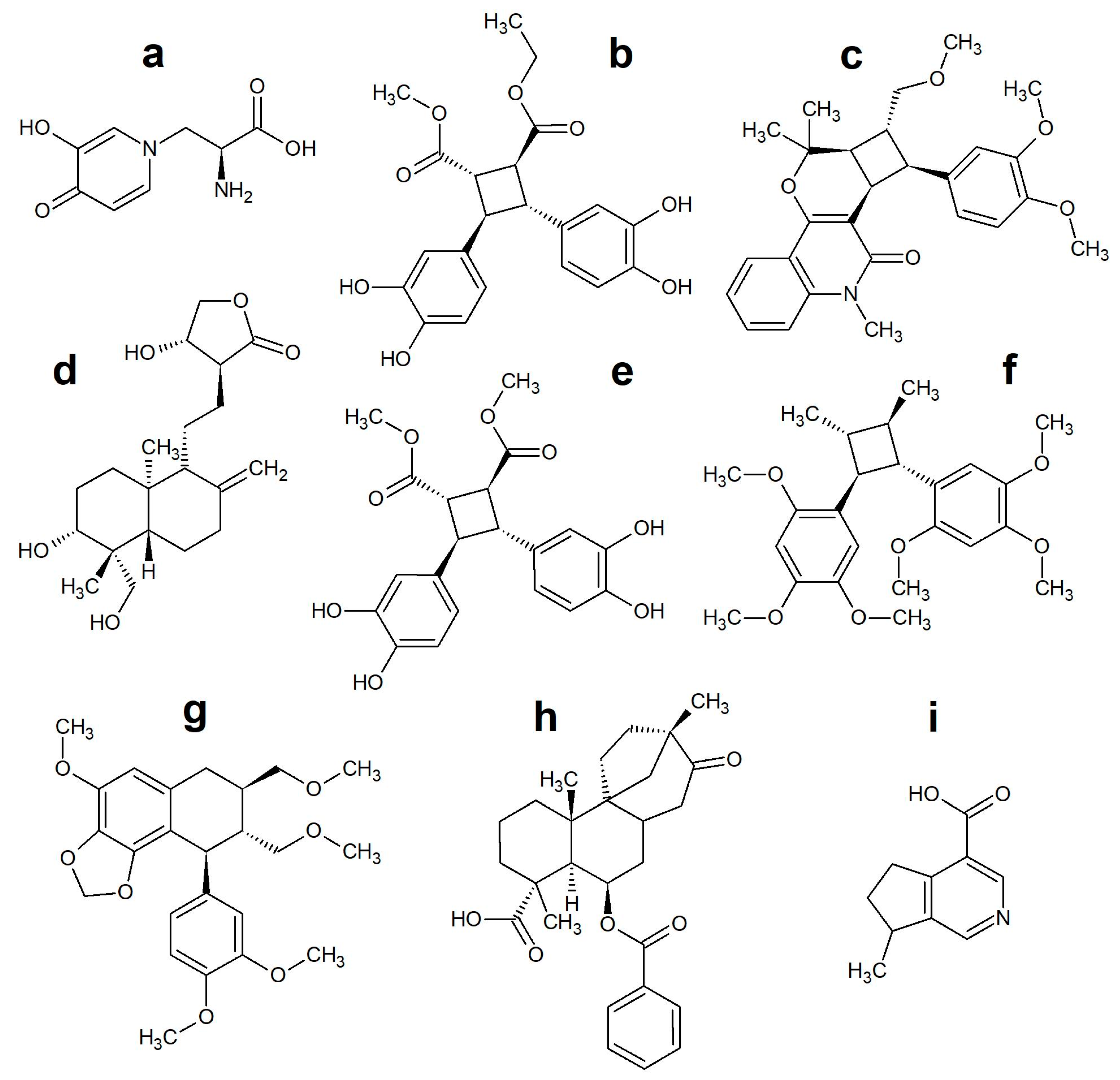
3.2. Ethnopharmacological Significance
4. Materials and Methods
Plants with High Potential
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bryan, C.S. Fever, Famine, and War: William Osler as an infectious disease specialist. Clin. Infect. Dis. 1996, 23, 1139–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, E.J.; Henna-Jumma, S.; Carraretto, M.; Forni, L. The pathophysiological basis and consequences of fever. Crit. Care 2016, 20, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mungmonphoncharoen, S.; Apidechkul, T.; Dokmaingam, P. Factors associated with the recurrence of dengue fever in villages in Chian Rai, Thailand: A community-based case-control study. J. Health Res. 2019, 33, 438–449. [Google Scholar] [CrossRef]
- Luxemburger, C.; Thwai, K.L.; White, N.J.; Webster, H.K.; Kyle, D.E.; Maelankirri, L.; Chongsuphajaisiddhi, T.; Nosten, F. The epidemiology of malaria in a Karen population on the western border of Thailand. Trans. R. Soc. Trop. Med. Hyg. 1996, 90, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci. Trends 2020. [Google Scholar] [CrossRef] [Green Version]
- Schieber, A.M.P.; Ayres, J.S. Thermoregulation as a disease tolerance defense strategy. Pathog. Dis. 2016, 74, ftw106. [Google Scholar] [CrossRef] [Green Version]
- Atkins, E. Pathogenesis of Fever. Physiol. Rev. 1960, 40, 580–646. [Google Scholar] [CrossRef]
- Solecki, R.S. Shanidar IV, a Neanderthal Flower Burial in Northern Iraq. Science 1975, 190, 880–881. [Google Scholar] [CrossRef]
- WHO. WHO traditional medicine strategy 2002–2005; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Fabricant, D.S.; Farnsworth, N.R. The value of plants used in traditional medicine for drug discovery. Environ. Health Persp. 2001, 109, 69–75. [Google Scholar]
- Tu, Y. The discovery of artemisinin (qinghaosu) and gifts from Chinese medicine. Nat. Med. 2011, 17, 1217. [Google Scholar] [CrossRef]
- Pooma, R.; Suddee, S. Tem Smitinand’s Thai Plant Names, revised; The Office of the Forest Herbarium: Bangkok, Thailand, 2014. [Google Scholar]
- Premsrirat, S. Ethnolinguistic Maps of Thailand; Ministry of Culture and Mahidol University: Bangkok, Thaialnd, 2004. [Google Scholar]
- Hidayati, S.; Franco, F.M.; Bussmann, R.W. Ready for phase 5-current status of ethnobiology in Southeast Asia. J. Ethnobiol. Ethnomed. 2015, 11. [Google Scholar] [CrossRef] [Green Version]
- Sanoprai, S.; Meeprom, K. Karen. Available online: https://www.sac.or.th/databases/ethnic-groups/ethnicGroups/79 (accessed on 19 March 2020).
- Tipraqsa, P.; Schreinemachers, P. Agricultural commercialization of Karen Hill tribes in northern Thailand. Agric. Econ. 2009, 40, 43–53. [Google Scholar] [CrossRef]
- Kaewsangsai, K. Ethnobotany of Karen in Khun Tuen Noi Village; Chiang Mai University: Chiang Mai, Thailand, 2017. [Google Scholar]
- Kamwong, K. Ethnobotany of Karens at Ban Mai Sawan and Ban Huay Pu Ling, Ban Luang Sub-District, Chom Thong District. Master’s Thesis, Chiang Mai University, Chiang Mai Province, Thailand, 2010. [Google Scholar]
- Phumthum, M.; Srithi, K.; Inta, A.; Junsongduang, A.; Tangjitman, K.; Pongamornkul, W.; Trisonthi, C.; Balslev, H. Ethnomedicinal plant diversity in Thailand. J. Ethnopharmacol. 2018, 214, 90–98. [Google Scholar] [CrossRef]
- Srithi, K. Comparative ethnobotany in Nan Province, Thailand. Ph.D. Thesis, Chiang Mai University, Chiang Mai Province, Thailand, 2012. [Google Scholar]
- Charnprasert, C.; Chansuwanit, N. Exploration and collection of medicinal plants in wasted areas of Muang district, Nonthaburi province. Kasetsart J. 1992, 26, 19. [Google Scholar]
- Sukkho, T. A Survey of medicinal plants used by Karen people at Ban Chan and Chaem Luang Subdidtricts, Mae Chaem District. Master’s Thesis, Chiang Mai University, Chiang Mai Province, Thailand, 2008. [Google Scholar]
- Oratai, N. Diversity of medicinal plants for fever healing from Khao Phanom Benja National Park, Krabi Province. KKU Sci. J. 2014, 42, 313–326. [Google Scholar]
- Apidechkul, T. Seroprevalence and factors associated with hepatitis B virus infection among the hill tribe youths, northern Thailand. BMC Infect. Dis. 2019, 19, 125. [Google Scholar] [CrossRef] [Green Version]
- Tienboon, P.; Wangpakapattanawong, P. Nutritional status, body composition and health conditions of the Karen hill tribe children aged 1–6 years in northern Thailand. Asia-Pac. J. Clin. Nutr. 2007, 16, 279–285. [Google Scholar]
- Anderson, E.F. Plants and People of the Golden Triangle: Ethnobotany of the Hill Tribes of Northern Thailand; Timber Press: Portland, OR, USA, 1993. [Google Scholar]
- Winijchaiyanan, P. Ethnobotany of Karen in Chiang Mai. Master’s Thesis, Chiang Mai University, Chiang Mai Province, Thailand, 1995. [Google Scholar]
- Tangjitman, K.; Trisonthi, C.; Wongsawad, C.; Jitaree, S.; Svenning, J.-C. Potential impact of climatic change on medicinal plants used in the Karen women’s health care in northern Thailand. Songklanakarin J. Sci. Technol 2015, 37, 369–379. [Google Scholar]
- Sutjaritjai, N.; Wangpakapattanawong, P.; Balslev, H.; Inta, A. Traditional uses of Leguminosae among the Karen in Thailand. Plants (Basel) 2019, 8, 600. [Google Scholar] [CrossRef] [Green Version]
- Phumthum, M.; Balslev, H.; Barfod, A.S. Important Medicinal Plant Families in Thailand. Front. Pharmacol. 2019, 10. [Google Scholar] [CrossRef]
- Moerman, D.E. An analysis of the food plants and drug plants of native North America. J. Ethnopharmacol. 1996, 52, 1–22. [Google Scholar] [CrossRef]
- Bennett, B.C.; Husby, C.E. Patterns of medicinal plant use: An examination of the Ecuadorian Shuar medicinal flora using contingency table and binomial analyses. J. Ethnopharmacol. 2008, 116, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Weckerle, C.S.; Cabras, S.; Castellanos, M.E.; Leonti, M. Quantitative methods in ethnobotany and ethnopharmacology: Considering the overall flora—hypothesis testing for over- and underused plant families with the Bayesian approach. J. Ethnopharmacol. 2011, 137, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Saslis-Lagoudakis, C.H.; Williamson, E.M.; Savolainen, V.; Hawkins, J.A. Cross-cultural comparison of three medicinal floras and implications for bioprospecting strategies. J. Ethnopharmacol. 2011, 135, 476–487. [Google Scholar] [CrossRef] [PubMed]
- Phumthum, M.; Balslev, H. Use of Medicinal Plants among Thai Ethnic Groups: A Comparison. Econ. Bot. 2019, 73, 64–75. [Google Scholar] [CrossRef] [Green Version]
- Slater, A.F. Chloroquine: Mechanism of drug action and resistance in Plasmodium falciparum. Pharmacol. Ther. 1993, 57, 203–235. [Google Scholar]
- Keyaerts, E.; Vijgen, L.; Maes, P.; Neyts, J.; Ranst, M.V. In vitro inhibition of severe acut respiratory syndrome coronavirus by chloroquine. Biochem. Bioph. Res. Commun. 2004, 323, 264–268. [Google Scholar] [CrossRef]
- Meshnick, S.R. Artemisinin: Mechanisms of action, resistance and toxicity. Int. J. Prasitology 2002, 32, 1655–1660. [Google Scholar] [CrossRef]
- Aronoff, D.M.; Neilson, E.G. Antipyretics: Mechanisms of action and clinical use in fever suppression. Am. J. Med. 2001, 111, 304–315. [Google Scholar] [CrossRef]
- Sadgrove, N.J.; Jones, G.L. From Petri Dish to Patient: Bioavailability Estimation and Mechanism of Action for Antimicrobial and Immunomodulatory Natural Products. Front. Microbiol. 2019, 10, 2470. [Google Scholar] [CrossRef]
- Chassagne, F.; Hul, S.; Deharo, E.; Bourdy, G. Natural remedies used by Bunong people in Mondulkiri province (Northeast Cambodia) with special reference to the treatment of 11 most common ailments. J. Ethnopharmacol. 2016, 191, 41–70. [Google Scholar] [CrossRef] [PubMed]
- Gandhiraja, N.; Sriram, S.; Meenaa, V.; Srilakshmi, J.K.; Sasikumar, C.; Rajeswari, R. Phytochemical screening and antimicrobial activity of the plant extracts of Mimosa pudica L. against selected microbes. Ethnobot. Leafl. 2009, 2009, 8. [Google Scholar]
- Ahmad, H.; Sehgal, S.; Mishra, A.; Gupta, R. Mimosa pudica L. (Laajvanti): An overview. Pharmacogn. Rev. 2012, 6, 115–124. [Google Scholar] [PubMed] [Green Version]
- Zaware, B.; Chaudhari, S.; Shinde, M. An overview of Mimosa pudica Linn. Chemistry and pharmacological profile. Res. J. Pharm. Biol. Chem. Sci. 2014, 5, 754–761. [Google Scholar]
- Wu, T.; Cui, H.; Cheng, B.; Fang, S.; Xu, F.; Gu, Q. Chemical constituetns from the roots of Elephantopus scaber L. Biochem. Syst. Ecol. 2014, 54, 65–67. [Google Scholar] [CrossRef]
- Wang, J.; Li, P.; Li, B.; Guo, Z.; Kennelly, E.J.; Long, C. Bioactivities of compounds from Elephantopus scaber, an ethnomedicinal plant from southwest china. Evid.-Based Compl. Altern. 2014, 2014, 569594. [Google Scholar]
- George, S.; Venkataraman, R.; Baby, S. Melicodenine I, a new quinolinone alkaloid from Melicope denhamii leaves. Nat. Prod. Res. 2017, 31, 890–895. [Google Scholar] [CrossRef]
- Chen, I.-S.C.; Chen, H.-F.; Cheng, M.-J.; Chang, Y.-L.; Teng, C.-M.; Tsutomu, I.; Chen, J.-J.; Tsai, I.-L. Quinoline alkaloids and other constituents of Melicope semecarpifolia with antiplatelet aggregation activity. J. Nat. Prod. 2001, 64, 1143–1147. [Google Scholar] [CrossRef]
- Achan, J.; Talisuna, A.O.; Erhart, A.; Yeka, A.; Tibenderana, J.K.; Baliraine, F.N.; Rosenthal, P.J.; D’Alessandro, U. Quinine, an old anti-malarial drug in a modern world: Role in the treatment of malaria. Malaria J. 2011, 10, 144. [Google Scholar] [CrossRef] [Green Version]
- Okhuarobo, A.; Falodun, J.E.; Erharuyi, O.; Imieje, V.; Falodun, A.; Langer, P. Harnessing the medicinal properties of Andrographics paniculata for diseases and beyond: A review of its phytochemistry and pharmacology. Asian Pac. J. Trop. Dis. 2014, 4, 213–222. [Google Scholar] [CrossRef]
- Sultana, S.; Asif, H.M.; Akhtar, N.; Ahmad, K. Medicinal plants with potential antipyretic activity: A review. Asian Pac. J. Trop. Dis. 2015, 5, S202–S208. [Google Scholar] [CrossRef]
- Mohammed, A.; Chiruvella, K.K.; Rao, Y.K.; Geethangili, M.; Raghavan, S.C.; Ghanta, R.G. In vitro production of echioidinin, 7-O-methywogonin from callus cultures of Andrographis lineata and their cytotoxicity on cancer cells. PLoS ONE 2015, 10, e0141154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deepa, V.S.; Rajaram, K.; Sureshkumar, P. Dimethyl 3, 3′, 4, 4′-tetrahydroxy-δ-truxinate isolated from the leaves of Andrographis lineata. Wall. ex. Nees suppress adipogenesis in 3T3-L1 preadipocytes for type 2 diabetes. Pak. J. Pharm. Sci. 2015, 28, 443–448. [Google Scholar] [PubMed]
- Raja, A.E.; Vijayalakshmi, M.; Devalarao, G. Acorus calamus Linn.: Chemistry and biology. Res. J. Pharm. Technol. 2009, 2, 256–261. [Google Scholar]
- Kassuya, C.A.L.; Leite, D.F.P.; de Melo, L.V.; Reher, V.L.G.; Calixto, J.B. Anti-inflammatory properties of extracts, fractions and lignans isolated from Phyllanthus amarus. Planta Med. 2005, 71, 721–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thyagarajan, S.P.; Subramanian, S.; Thirunalasundari, T.; Venkateswaran, P.S.; Blumberg, B.S. Effect of Phyllanthus amarus on chronic carriers of hepatitis B virus. Lancet 1988, 2, 764–766. [Google Scholar] [CrossRef]
- Giang, P.M.; Son, P.T.; Matsunami, K.; Otsuka, H. Chemical and biological evaluation on scopadulane-type diterpenoids from Scoparia dulcis of vietnamese origins. Chem. Pharm. Bull. 2006, 54, 546–549. [Google Scholar] [CrossRef]
- Hayashi, T.; Hayashi, K.; Uchida, K.; Niwayama, S.; Morita, N. Antiviral agents of plant origin. 2. Antiviral activity of scopadulcic acid B derivatives. Chem. Pharm. Bull. 1990, 38, 239–242. [Google Scholar] [CrossRef]
- Saptarini, N.M.; Deswita, D.A. Antipyretic activity of plantain (Plantago major L.) leaves extract in yeast-induced mice. Drug Invent. Today 2019. [Google Scholar]
- Adom, M.B.; Taher, M.; Mutalabisin, M.F.; Amri, M.S.; Kudos, M.B.A.; Sulaiman, M.W.A.W.; Sengupta, P.; Susanti, D. Chemical constituents and medical benefits of Plantago major. Biomed. Pharmacother. 2017, 96, 348–360. [Google Scholar] [CrossRef]
- Tardío, J.; Pardo-de-Santayana, M. Cultural Importance Indices: A Comparative Analysis Based on the Useful Wild Plants of Southern Cantabria (Northern Spain). Econ. Bot. 2008, 62, 24–39. [Google Scholar] [CrossRef]
Sample Availability: Samples of the compounds are not available from the authors. |



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phumthum, M.; Sadgrove, N.J. High-Value Plant Species Used for the Treatment of “Fever” by the Karen Hill Tribe People. Antibiotics 2020, 9, 220. https://doi.org/10.3390/antibiotics9050220
Phumthum M, Sadgrove NJ. High-Value Plant Species Used for the Treatment of “Fever” by the Karen Hill Tribe People. Antibiotics. 2020; 9(5):220. https://doi.org/10.3390/antibiotics9050220
Chicago/Turabian StylePhumthum, Methee, and Nicholas J. Sadgrove. 2020. "High-Value Plant Species Used for the Treatment of “Fever” by the Karen Hill Tribe People" Antibiotics 9, no. 5: 220. https://doi.org/10.3390/antibiotics9050220
APA StylePhumthum, M., & Sadgrove, N. J. (2020). High-Value Plant Species Used for the Treatment of “Fever” by the Karen Hill Tribe People. Antibiotics, 9(5), 220. https://doi.org/10.3390/antibiotics9050220