Label-Free Electrochemical Microfluidic Chip for the Antimicrobial Susceptibility Testing




Abstract
:1. Introduction
2. Results and Discussion
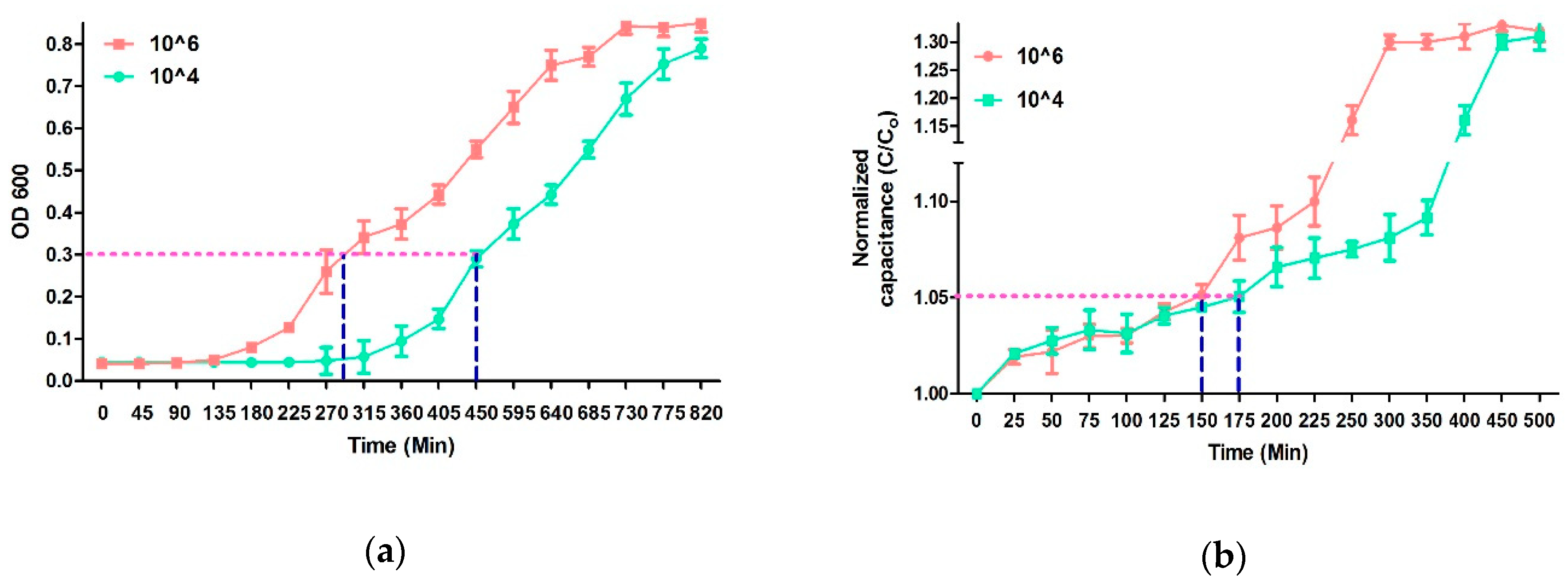
2.1. Bacterial Growth Analysis and MIC
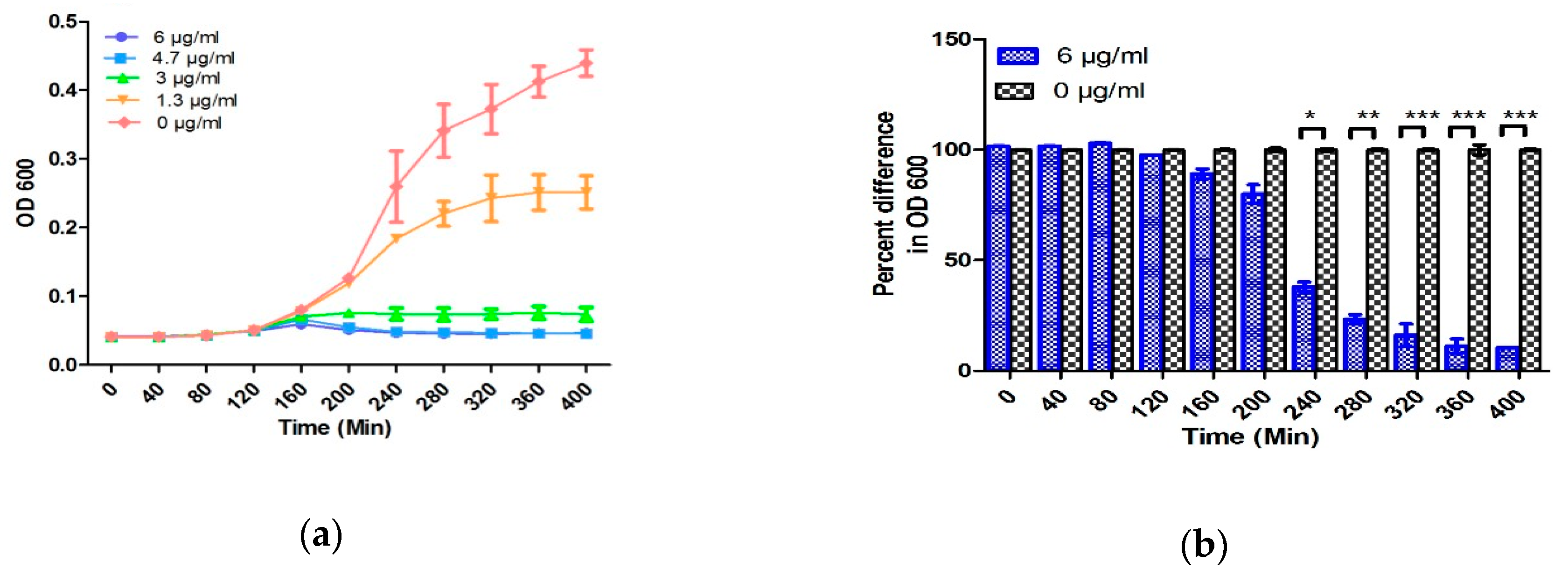
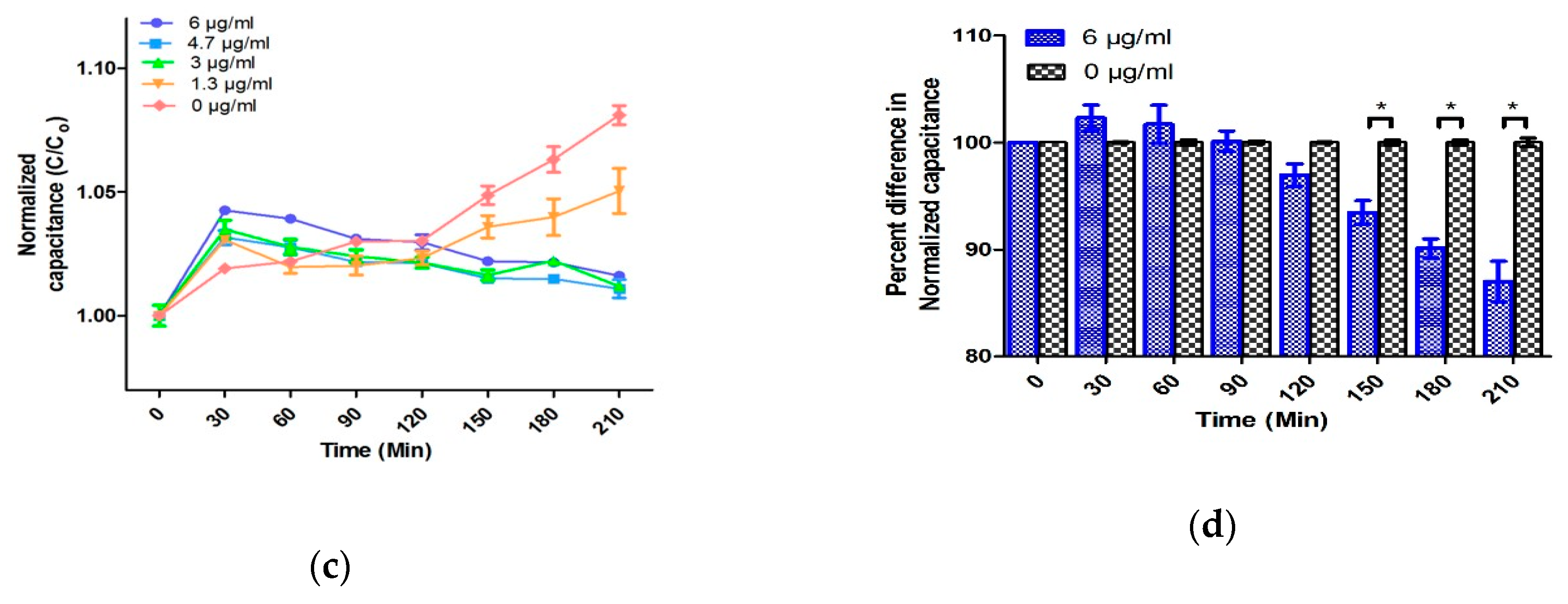
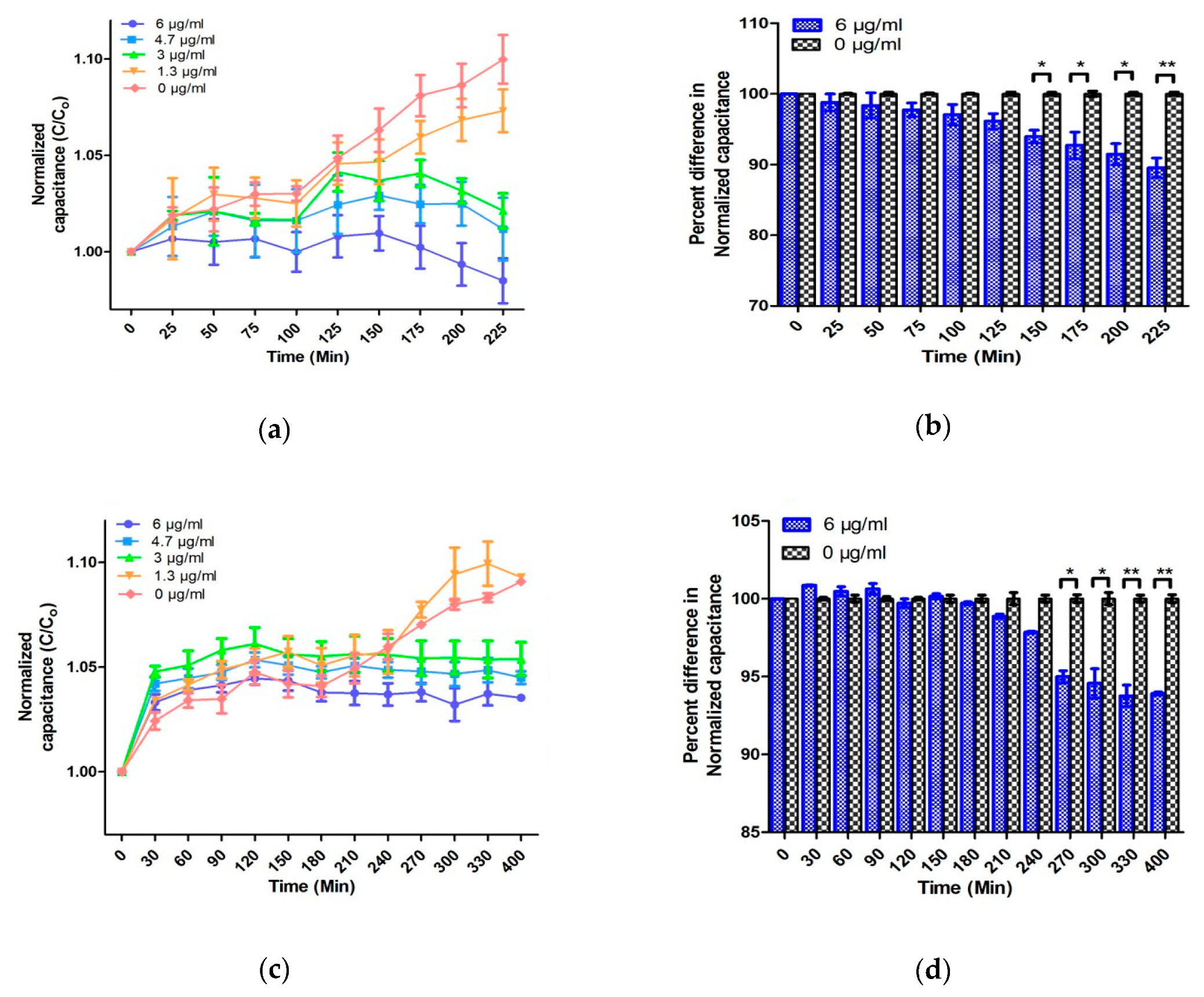
2.2. Analysis of Microplate and Microfluidic Chip-Based AST in TSB
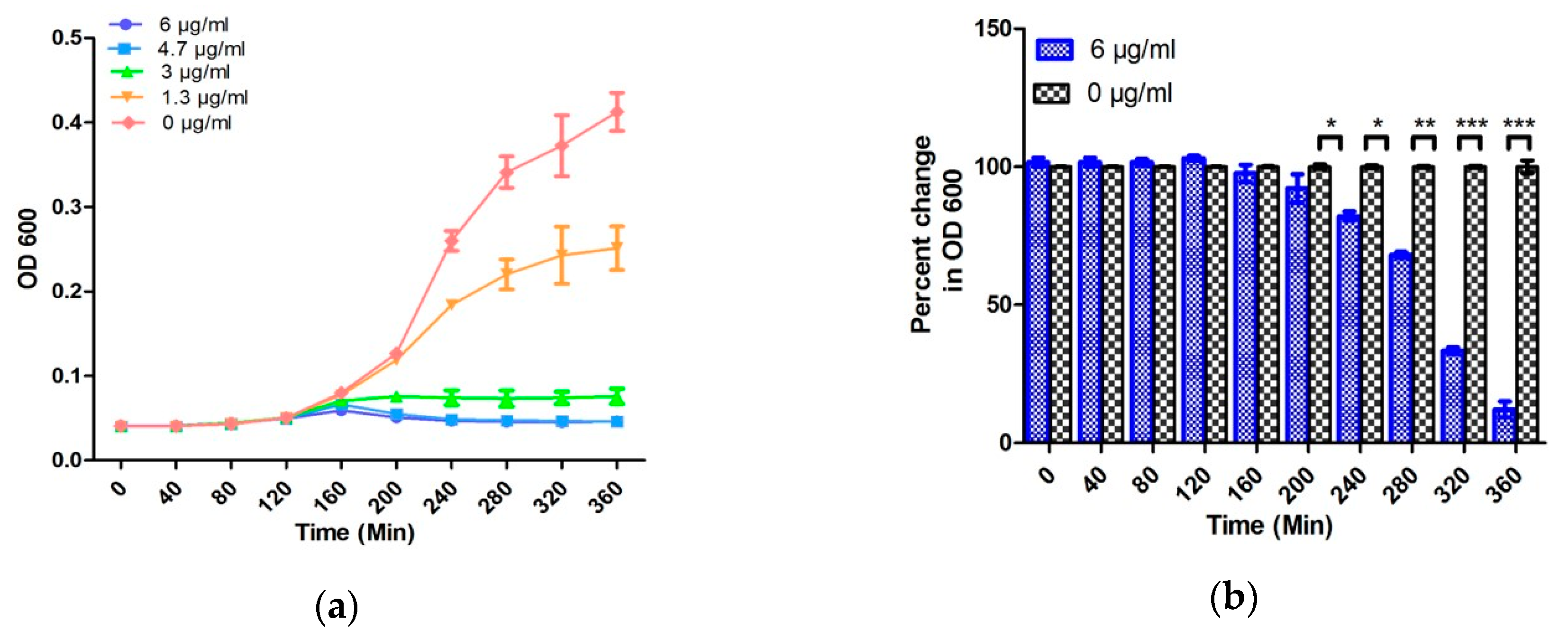
2.3. Antibiotic Susceptibility Testing in Artificial Urine Samples
3. Materials and Methods
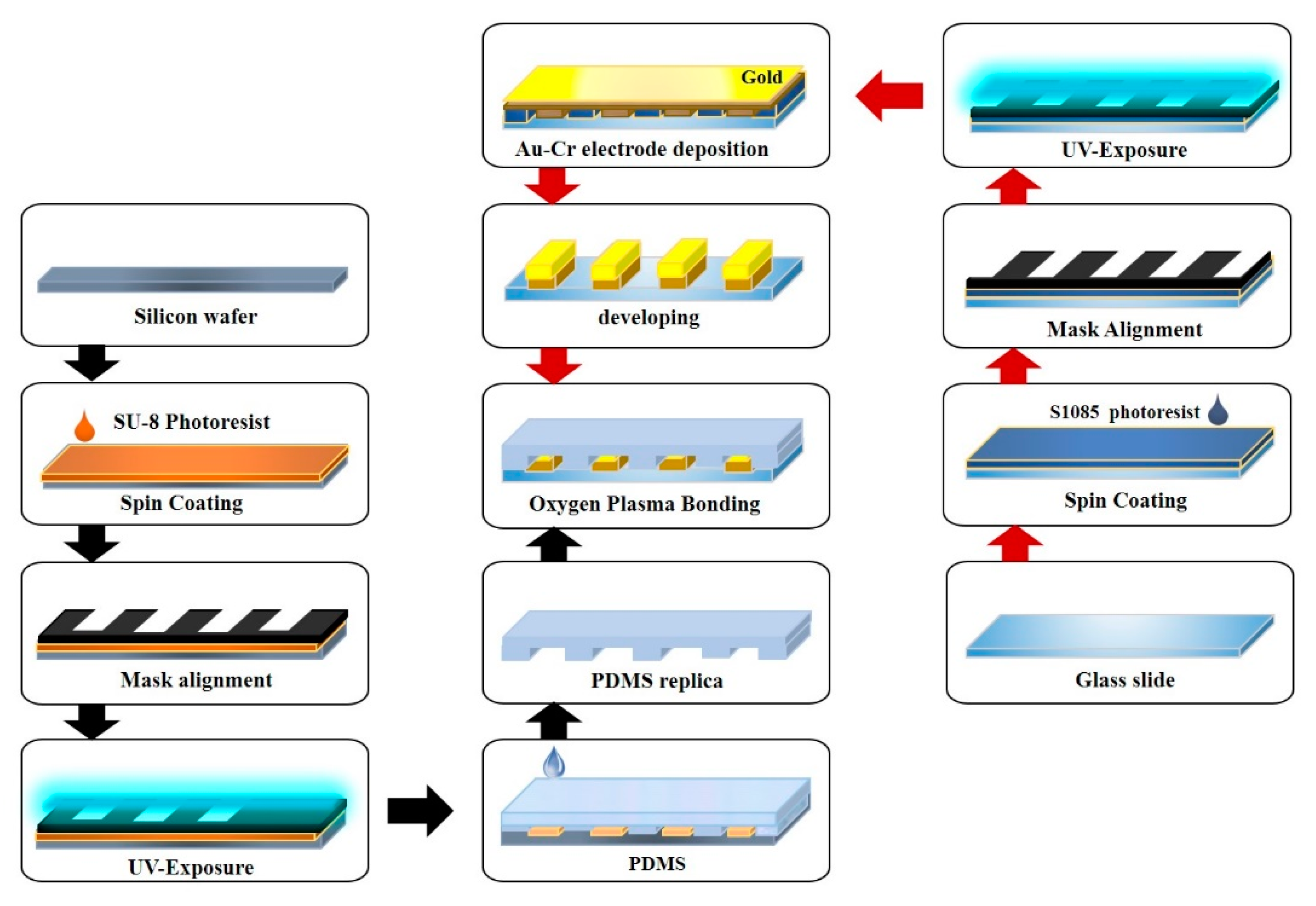
3.1. Fabrication of the EMC
3.2. Operation of EMC
3.3. Bacterial Culture, Growth Analysis, and Antibiotic Susceptibility Testing
3.4. Preparation of Artificial Urine Sample
3.5. Electrical Signal Measurements
3.6. Statistical analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Tadesse, B.T.; Ashley, E.A.; Ongarello, S.; Havumaki, J.; Wijegoonewardena, M.; González, I.J.; Dittrich, S. Antimicrobial resistance in Africa: A systematic review. BMC Infect. Dis. 2017, 17, 616. [Google Scholar] [CrossRef]
- Garcia-Doval, I.; Cohen, A.D.; Cazzaniga, S.; Feldhamer, I.; Addis, A.; Carretero, G.; Ferrándiz, C.; Stern, R.S.; Naldi, L.; Network, P. Risk of serious infections, cutaneous bacterial infections, and granulomatous infections in patients with psoriasis treated with anti–tumor necrosis factor agents versus classic therapies: Prospective meta-analysis of Psonet registries. J. Am. Acad. Dermatol. 2017, 76, 299–308. [Google Scholar] [CrossRef]
- Zhang, R.; Eggleston, K.; Rotimi, V.; Zeckhauser, R.J. Antibiotic resistance as a global threat: Evidence from China, Kuwait and the United States. Glob. Health 2006, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blair, J.M.A.; Webber, M.A.; Baylay, A.J.; Ogbolu, D.O.; Piddock, L.J.V. Molecular mechanisms of antibiotic resistance. Nat. Rev. Microbiol. 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Resistance, R.O.A. Tackling Drug-resistant Infections Globally: Final Report and Recommendations; Review on Antimicrobial Resistance. 2016. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 18 April 2020).
- Foxman, B. The epidemiology of urinary tract infection. Nat. Rev. Urol. 2010, 7, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Ashiru-Oredope, D.; Budd, E.; Bhattacharya, A.; Din, N.; McNulty, C.; Micallef, C. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR). Implementation of antimicrobial stewardship interventions recommended by national toolkits in primary and secondary healthcare sectors in England: TARGET and Start Smart Then Focus. J. Antimicrob. Chemother. 2016, 71, 1408–1414. [Google Scholar]
- Chaplin, S. ESPAUR 2016: Antibiotic and antifungal prescribing in England. Prescriber 2017, 28, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Jafri, S.A.; Qasim, M.; Masoud, M.S. Antibiotic resistance of E. coli isolates from urine samples of urinary tract infection (UTI) patients in Pakistan. Bioinformation 2014, 10, 419–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutter, S.A.; Currie, M.L.; Mitz, L.B.; Greenbaum, L.A. Antibiotic resistance patterns in children hospitalized for urinary tract infections. Arch. Pediatr. Adolesc. Med. 2005, 159, 924–928. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Zhang, X.; Liang, X.; Bloom, G. Addressing antimicrobial resistance in China: Policy implementation in a complex context. Glob. Health 2016, 12, 30. [Google Scholar] [CrossRef] [Green Version]
- Waller, T.A.; Pantin, S.A.L.; Yenior, A.L.; Pujalte, G.G.A. Urinary Tract Infection Antibiotic Resistance in the United States. Prim. Care Clin. Off. Pract. 2018, 45, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. The antibiotic resistance crisis: part 1: Causes and threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Bartlett, J.G.; Gilbert, D.N.; Spellberg, B. Seven ways to preserve the miracle of antibiotics. Clin. Infect. Dis. 2013, 56, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Amidi, S.; Solter, S.; Rashidian, B.; Zokaian, A.-R.; Razmjoian, F. Antibiotic use and abuse among physicians in private practice in Shiraz, Iran. Med. Care 1975, 13, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Lansang, M.A.; Lucas-Aquino, R.; Tupasi, T.E.; Mina, V.S.; Salazar, L.S.; Juban, N.; Limjoco, T.T.; Nisperos, L.E.; Kunin, C.M. Purchase of antibiotics without prescription in Manila, the Philippines. Inappropriate choices and doses. J. clin. epidemiol. 1990, 43, 61–67. [Google Scholar] [CrossRef]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6. [Google Scholar] [CrossRef]
- English, B.K.; Gaur, A.H. The use and abuse of antibiotics and the development of antibiotic resistance. In Hot topics in infection and immunity in children VI; Springer: Berlin, Germany, 2010; pp. 73–82. [Google Scholar]
- Tamma, P.D.; Cosgrove, S.E. Antimicrobial stewardship. Infect. Dis. Clin. 2011, 25, 245–260. [Google Scholar] [CrossRef]
- Niederman, M.S. Principles of appropriate antibiotic use. Int. J. Antimicrob. Agents 2005, 26. [Google Scholar] [CrossRef]
- Gilad, J.; Giladi, M.; Poch, F.; Aharoni, Y.; Schwartz, D. “All-in-one-plate” E-test and disk diffusion susceptibility co-testing for multiresistant Acinetobacter baumannii. Eur. J. Clin. Microbiol. Infect. Dis. 2006, 25, 799–802. [Google Scholar] [CrossRef]
- Khan, Z.A.; Siddiqui, M.F.; Park, S. Current and Emerging Methods of Antibiotic Susceptibility Testing. Diagnostics 2019, 9, 49. [Google Scholar] [CrossRef] [Green Version]
- Hudzicki, J. Kirby-Bauer Disk Diffusion Susceptibility Test Protocol. 2009. Available online: https://www.asm.org/getattachment/2594ce26-bd44-47f6-8287-0657aa9185ad/Kirby-Bauer-Disk-Diffusion-Susceptibility-Test-Protocol-pdf.pdf (accessed on 18 April 2020).
- Reller, L.B.; Weinstein, M.; Jorgensen, J.H.; Ferraro, M.J. Antimicrobial susceptibility testing: a review of general principles and contemporary practices. Clin. Infect. dis. 2009, 49, 1749–1755. [Google Scholar]
- Dickert, H.; Machka, K.; Braveny, I. The uses and limitations of disc diffusion in the antibiotic sensitivity testing of bacteria. Infection 1981, 9, 18–24. [Google Scholar] [CrossRef]
- Wiegand, I.; Hilpert, K.; Hancock, R.E. Agar and broth dilution methods to determine the minimal inhibitory concentration (MIC) of antimicrobial substances. Nat. protoc. 2008, 3, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Syal, K.; Mo, M.; Yu, H.; Iriya, R.; Jing, W.; Guodong, S.; Wang, S.; Grys, T.E.; Haydel, S.E.; Tao, N. Current and emerging techniques for antibiotic susceptibility tests. Theranostics 2017, 7, 1795–1805. [Google Scholar] [CrossRef]
- Khan, Z.A.; Siddiqui, M.F.; Park, S. Progress in antibiotic susceptibility tests: A comparative review with special emphasis on microfluidic methods. Biotechnol. Lett. 2019, 41, 221–230. [Google Scholar] [CrossRef]
- Cornaglia, G.; Akova, M.; Amicosante, G.; Canton, R.; Cauda, R.; Docquier, J.D.; Edelstein, M.; Frere, J.M.; Fuzi, M.; Galleni, M.; et al. Metallo-beta-lactamases as emerging resistance determinants in Gram-negative pathogens: Open issues. Int. J. Antimicrob. Agents 2007, 29, 380–388. [Google Scholar] [CrossRef]
- Burckhardt, I.; Zimmermann, S. Susceptibility Testing of Bacteria Using Maldi-Tof Mass Spectrometry. Front. Microbiol. 2018, 9, 1744. [Google Scholar] [CrossRef] [Green Version]
- Lowe, R.D.; Guild, G.E.; Harpas, P.; Kirkbride, P.; Hoffmann, P.; Voelcker, N.H.; Kobus, H. Rapid drug detection in oral samples by porous silicon assisted laser desorption/ionization mass spectrometry. Rapid Commun. Mass Spectrom. 2009, 23, 3543–3548. [Google Scholar] [CrossRef]
- Flentie, K.; Spears, B.R.; Chen, F.; Purmort, N.B.; DaPonte, K.; Viveiros, E.; Phelan, N.; Krebill, C.; Flyer, A.N.; Hooper, D.C.; et al. Microplate-based surface area assay for rapid phenotypic antibiotic susceptibility testing. Sci. Rep. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Toseland, C.P. Fluorescent labeling and modification of proteins. J. Chem. Biol. 2013, 6, 85–95. [Google Scholar] [CrossRef]
- Krüger, J.; Singh, K.; O’Neill, A.; Jackson, C.; Morrison, A.; O’Brien, P. Development of a microfluidic device for fluorescence activated cell sorting. J. Micromech. Microeng. 2002, 12. [Google Scholar] [CrossRef]
- McDonald, J.C.; Metallo, S.J.; Whitesides, G.M. Fabrication of a configurable, single-use microfluidic device. Anal. Chem. 2001, 73, 5645–5650. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Lu, Y.; Sin, M.L.; Mach, K.E.; Zhang, D.D.; Gau, V.; Liao, J.C.; Wong, P.K. Antimicrobial susceptibility testing using high surface-to-volume ratio microchannels. Anal. Chem. 2010, 82, 1012–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baltekin, Ö.; Boucharin, A.; Tano, E.; Andersson, D.I.; Elf, J. Antibiotic susceptibility testing in less than 30 min using direct single-cell imaging. Proc. Natl. Acad. Sci. USA 2017, 114, 9170–9175. [Google Scholar] [CrossRef] [Green Version]
- Hassanpourfard, M.; Ghosh, R.; Thundat, T.; Kumar, A. Dynamics of bacterial streamers induced clogging in microfluidic devices. Lab. Chip. 2016, 16, 4091–4096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukhopadhyay, R. When microfluidic devices go bad. How does fouling occur in microfluidic devices, and what can be done about it? Anal. Chem. 2005, 77, 429A–432A. [Google Scholar]
- Safavieh, M.; Pandya, H.J.; Venkataraman, M.; Thirumalaraju, P.; Kanakasabapathy, M.K.; Singh, A.; Prabhakar, D.; Chug, M.K.; Shafiee, H. Rapid real-time antimicrobial susceptibility testing with electrical sensing on plastic microchips with printed electrodes. ACS Appl. Mater. Interfaces 2017, 9, 12832–12840. [Google Scholar] [CrossRef] [Green Version]
- Halford, C.; Gonzalez, R.; Campuzano, S.; Hu, B.; Babbitt, J.T.; Liu, J.; Wang, J.; Churchill, B.M.; Haake, D.A. Rapid antimicrobial susceptibility testing by sensitive detection of precursor rRNA using a novel electrochemical biosensing platform. Antimicrob. Agents Chemother. 2013, 57, 936–943. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Lu, Y.; Gau, V.; Liao, J.C.; Wong, P.K. Rapid antimicrobial susceptibility testing with electrokinetics enhanced biosensors for diagnosis of acute bacterial infections. Ann. Biomed. Eng. 2014, 42, 2314–2321. [Google Scholar] [CrossRef] [Green Version]
- Gómez, R.; Bashir, R.; Bhunia, A.K. Microscale electronic detection of bacterial metabolism. Sens. Actuators B Chem. 2002, 86, 198–208. [Google Scholar]
- Patolsky, F.; Filanovsky, B.; Katz, E.; Willner, I. Photoswitchable Antigen−Antibody Interactions Studied by Impedance Spectroscopy. J. Phys. Chem. B 1998, 102, 10359–10367. [Google Scholar] [CrossRef]
- Sezonov, G.; Joseleau-Petit, D.; D’Ari, R. Escherichia coli cell Physiology in Luria-Bertani Broth. J. Bacteriol. 2007, 189, 8746–8749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ur, A.; Brown, D.F. Impedance monitoring of bacterial activity. J. Med. Microbiol. 1975, 8, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fridman, O.; Goldberg, A.; Ronin, I.; Shoresh, N.; Balaban, N.Q. Optimization of lag time underlies antibiotic tolerance in evolved bacterial populations. Nature 2014, 513, 418–421. [Google Scholar] [CrossRef]
- Yourassowsky, E.; Van der Linden, M.P.; Lismont, M.J.; Crokaert, F.; Glupczynski, Y. Correlation between growth curve and killing curve of Escherichia coli after a brief exposure to suprainhibitory concentrations of ampicillin and piperacillin. Antimicrob. Agents Chemother. 1985, 28, 756–760. [Google Scholar] [CrossRef] [Green Version]
- Scheffers, D.-J.; Pinho, M.G. Bacterial cell wall synthesis: new insights from localization studies. Microbiol. Mol. Biol. Rev. 2005, 69, 585–607. [Google Scholar] [CrossRef] [Green Version]
- Chudobova, D.; Dostalova, S.; Blazkova, I.; Michalek, P.; Ruttkay-Nedecky, B.; Sklenar, M.; Nejdl, L.; Kudr, J.; Gumulec, J.; Tmejova, K.; et al. Effect of ampicillin, streptomycin, penicillin and tetracycline on metal resistant and non-resistant Staphylococcus aureus. Int. J. Environ. Res. Public Health 2014, 11, 3233–3255. [Google Scholar] [CrossRef]
- Mason, D.J.; Allman, R.; Stark, J.M.; Lloyd, D. Rapid estimation of bacterial antibiotic susceptibility with flow cytometry. J. Microsc. 1994, 176, 8–16. [Google Scholar] [CrossRef]
- Nguyen, T.; Chidambara Vinayaka, A.; Duong Bang, D.; Wolff, A. A Complete Protocol for Rapid and Low-Cost Fabrication of Polymer Microfluidic Chips Containing Three-Dimensional Microstructures Used in Point-of-Care Devices. Micromachines 2019, 10, 624. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.; Ngo, T.A.; Bang, D.D.; Wolff, A. Optimising the supercritical angle fluorescence structures in polymer microfluidic biochips for highly sensitive pathogen detection: a case study on Escherichia coli. Lab. Chip. 2019, 19, 3825–3833. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, M.F.; Khan, Z.A.; Jeon, H.; Park, S. SPE based soil processing and aptasensor integrated detection system for rapid on-site screening of arsenic contamination in soil. Ecotoxicol. Environ. Saf. 2020, 196. [Google Scholar] [CrossRef] [PubMed]
- Hanif, Z.; Khan, Z.A.; Siddiqui, M.F.; Tariq, M.Z.; Park, S.; Park, S.J. Tannic acid-mediated rapid layer-by-layer deposited non-leaching silver nanoparticles hybridized cellulose membranes for point-of-use water disinfection. Carbohydr. Polym. 2020, 231. [Google Scholar] [CrossRef] [PubMed]
- Prywer, J.; Kozanecki, M.; Mielniczek-Brzóska, E.; Torzewska, A. Solid Phases Precipitating in Artificial Urine in the Absence and Presence of Bacteria Proteus mirabilis—A Contribution to the Understanding of Infectious Urinary Stone Formation. Crystals 2018, 8, 164. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Quantity (g/L) |
|---|---|
| CaCl2·2H2O | 0.651 |
| MgCl2·6H2O | 0.651 |
| NaCl | 4.6 |
| Na2SO4 | 2.3 |
| Na3C6H5O7 | 0.65 |
| Na2C2O4 | 0.023 |
| KH2PO4 | 2.8 |
| KCl | 1.6 |
| NH4Cl | 1.0 |
| CO(NH2)2 | 25.0 |
| C4H9N3O2 | 1.1 |
| Tryptic soy broth | 10.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, H.; A. Khan, Z.; Barakat, E.; Park, S. Label-Free Electrochemical Microfluidic Chip for the Antimicrobial Susceptibility Testing. Antibiotics 2020, 9, 348. https://doi.org/10.3390/antibiotics9060348
Jeon H, A. Khan Z, Barakat E, Park S. Label-Free Electrochemical Microfluidic Chip for the Antimicrobial Susceptibility Testing. Antibiotics. 2020; 9(6):348. https://doi.org/10.3390/antibiotics9060348
Chicago/Turabian StyleJeon, Hyoil, Zeeshan A. Khan, Emad Barakat, and Seungkyung Park. 2020. "Label-Free Electrochemical Microfluidic Chip for the Antimicrobial Susceptibility Testing" Antibiotics 9, no. 6: 348. https://doi.org/10.3390/antibiotics9060348
APA StyleJeon, H., A. Khan, Z., Barakat, E., & Park, S. (2020). Label-Free Electrochemical Microfluidic Chip for the Antimicrobial Susceptibility Testing. Antibiotics, 9(6), 348. https://doi.org/10.3390/antibiotics9060348