A Review of Topical Phage Therapy for Chronically Infected Wounds and Preparations for a Randomized Adaptive Clinical Trial Evaluating Topical Phage Therapy in Chronically Infected Diabetic Foot Ulcers

Abstract
:1. Introduction
2. A Systematic Review of Topical Bacteriophage Therapy Used in Chronically Infected Ulcers
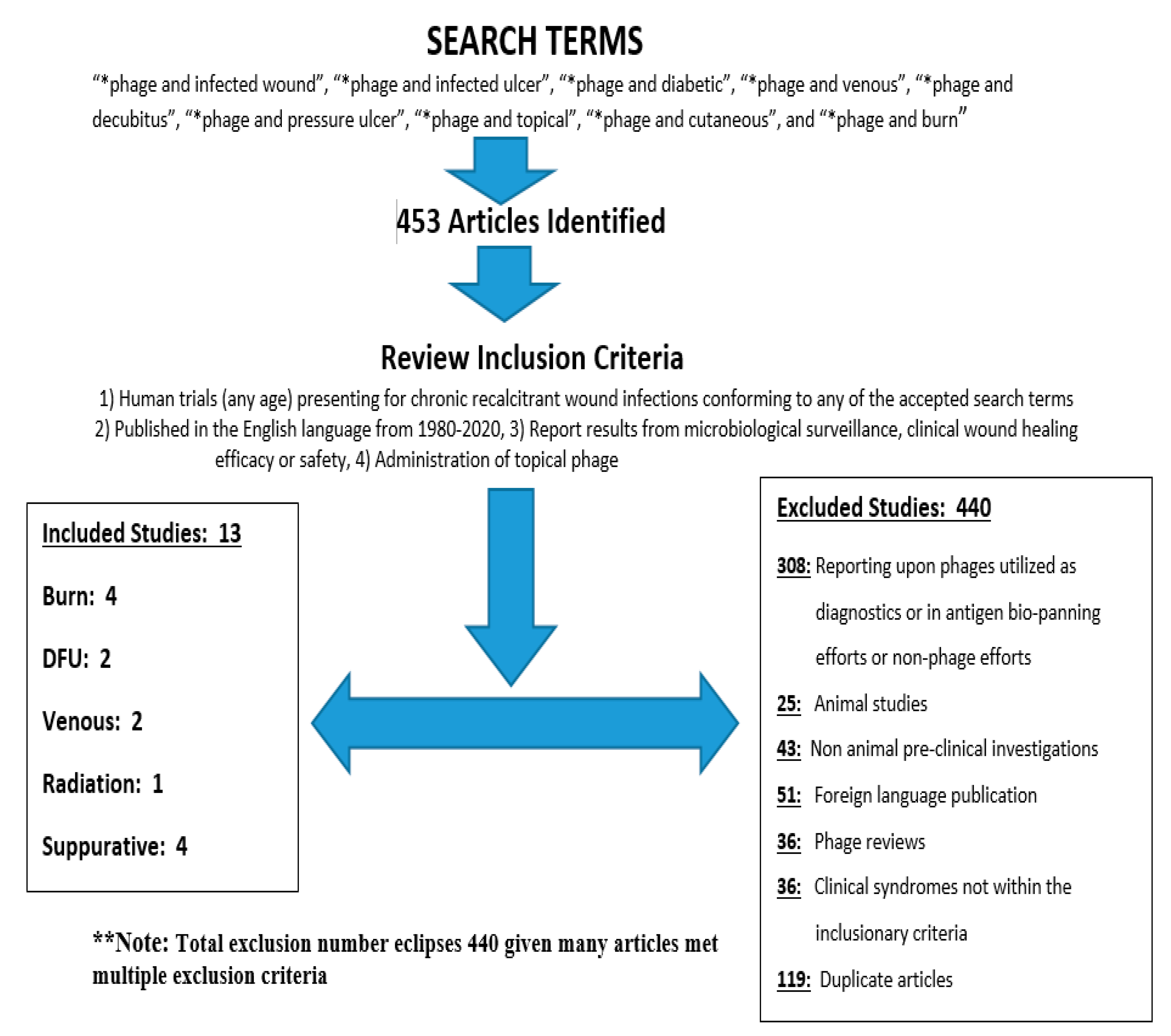
2.1. The Literature Search
2.2. Inclusion/Exclusion Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Data Abstraction
2.4. Analysis
3. Literature Search Results
3.1. Overall Search Results
3.2. Synopses of the Results from Included Articles (See Table 1)
3.2.1. Topical Phage Therapy for Treatment of Infected Venous Stasis Wounds/Ulcers
3.2.2. Topical Phage Therapy for Secondarily Infected Radiation Induced Cutaneous Ulcers
3.2.3. Topical Phage Therapy for Secondarily Infected Burn-Mediated Ulcers
3.2.4. Topical Phage Therapy in the Treatment of Infected Diabetic Foot (Toe) Ulcers
3.2.5. Topical Phage Therapy in Undisclosed (Uncharacterized) Chronically Infected Wounds
4. Discussion
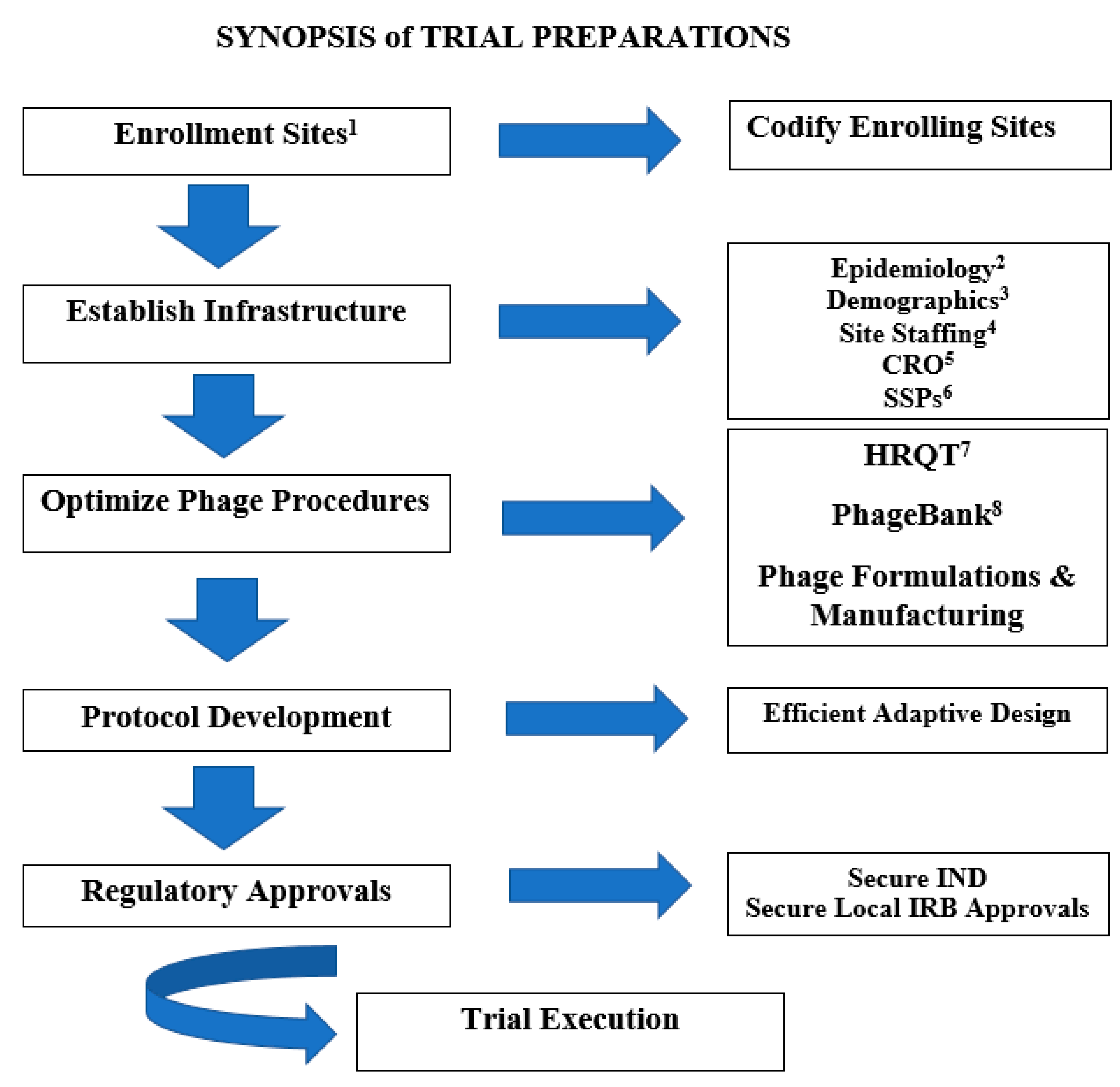
5. Preparations for a Randomized Clinical Trial Evaluating the Safety and Therapeutic Efficacy of Adjunctive Phage Therapy in Infected Diabetic Foot Ulcers
5.1. Background
5.1.1. Diabetic Foot Infections (DFI): A Canonical Paradigm and Model for Complicated Refractory Infected Cutaneous Wounds/Ulcers
5.1.2. Protocol Overview: Phage Therapy for Treatment of Chronic Diabetic Foot Infections (DFI)
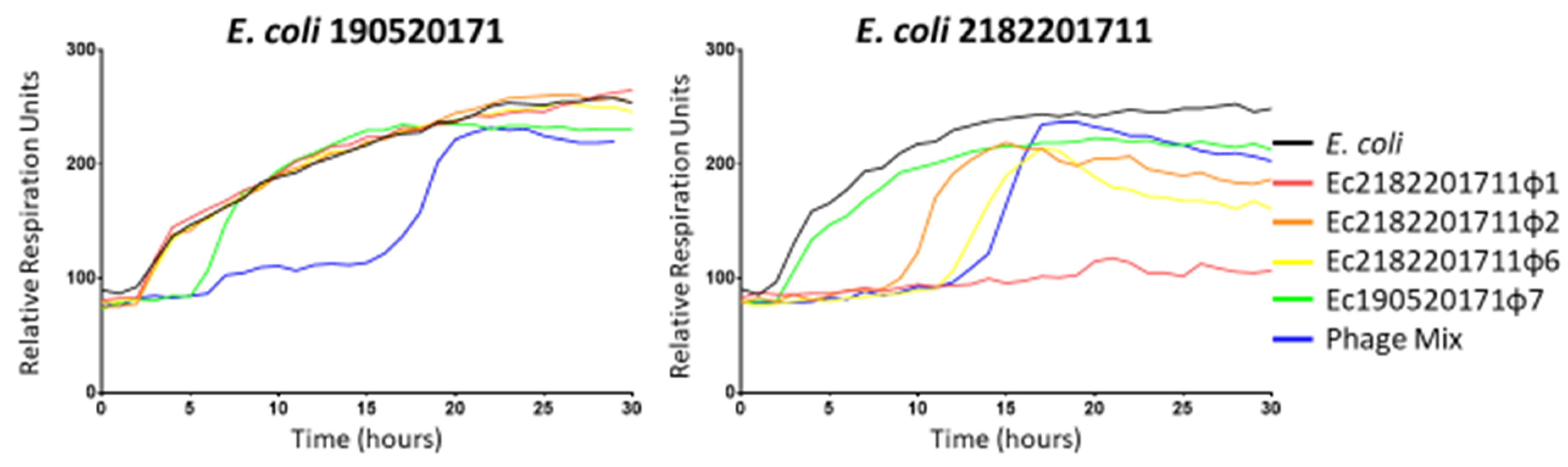
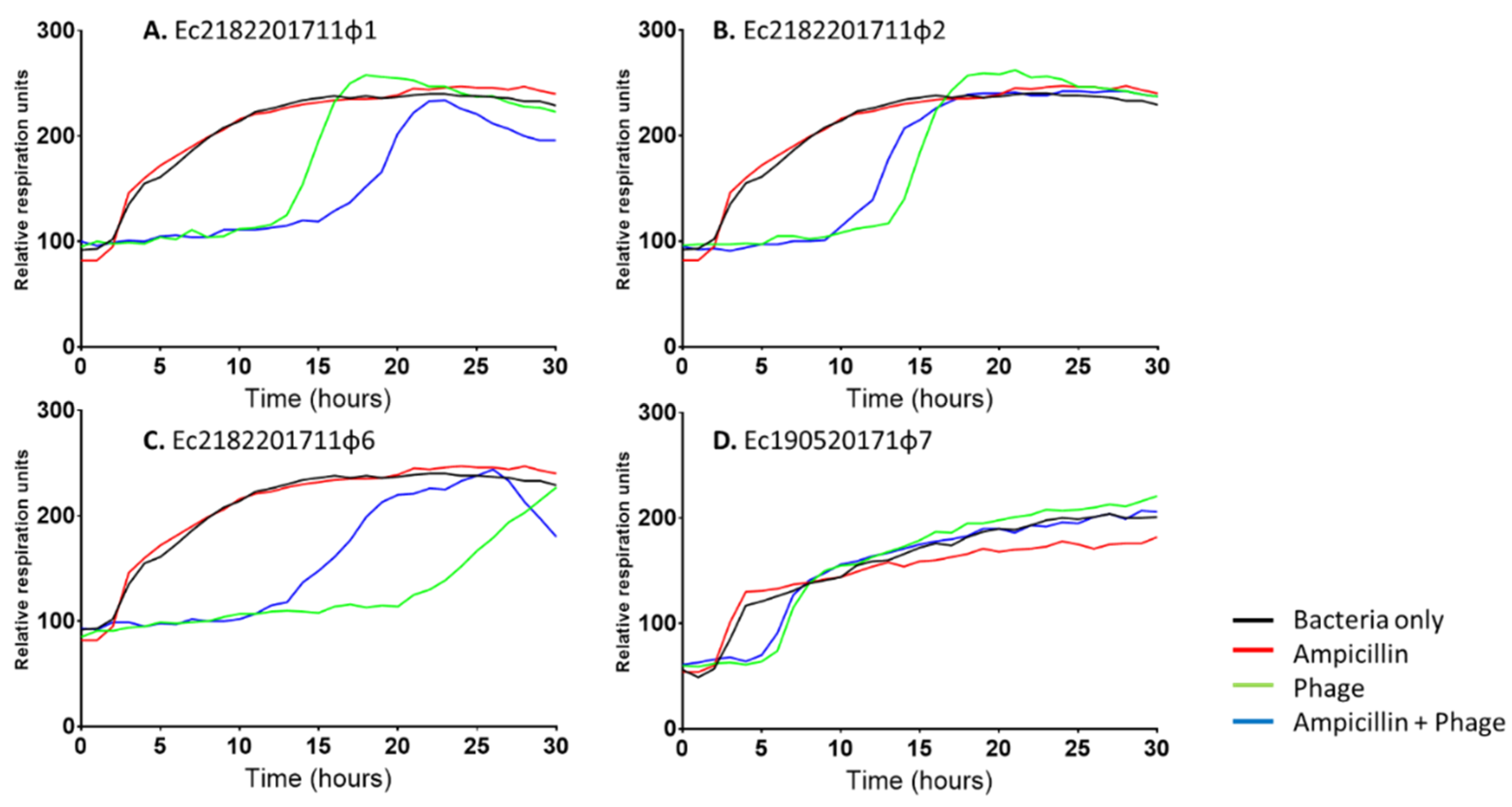
5.2. The HRQT Assay
5.3. PhageBankTM
5.4. Exploratory Insights to Optimizing Adjunctive Phage Therapy
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
Copyright Statement
References
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance; World Health Organization: Geneva, Switzerland, 2014; pp. 1–257. Available online: http://www.who.int (accessed on 1 May 2019).
- El-Shibiny, A.; El-Sahhar, S. Bacteriophages: The possible solution to treat infections caused by pathogenic bacteria. Can. J. Microbiol. 2017, 63, 865–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, E.V.; James, C.E.; Williams, D.; O’Brien, S.; Fothergill, J.L.; Haldenby, S.; Paterson, S.; Winstanley, C.; Brockhurst, M.A. Temperate phages both mediate and drive adaptive evolution in pathogen biofilms. Proc. Natl. Acad. Sci. USA 2016, 113, 8266–8271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debarbieux, L.; Pimay, J.P.; Verbeken, G.; DeVos, D.; Merabishvili, M.; Huys, I.; Patey, O.; Schoonjans, D.; Vaneechoutte, M.; Zizi, M.; et al. A bacteriophage journey at the European Medicines Agency. FEMS Microbiol. Lett. 2016, 363, fnv225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauser, A.R.; Mecsas, J.; Moir, D.T. Beyond Antibiotics: New Therapeutic Approaches for Bacterial Infections. Clin. Infect. Dis. 2016, 63, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Drulis-Kawa, Z.; Majkowska-Skrobek, G.; Maciejewska, B. Bacteriophages and phage-derived proteins- application approaches. Curr. Med. Chem. 2015, 22, 1757–1773. [Google Scholar] [CrossRef] [PubMed]
- El Haddad, L.; Harb, C.P.; Gebrara, M.A.; Stibich, M.A.; Chemaly, R.F. A systematic and critical review of bacteriophage therapy against multi drug resistant ESKAPE organisms in humans. Clin. Infect. Dis. 2018, 69, 167–178. [Google Scholar] [CrossRef]
- Furfaro, L.; Change, B.J.; Payne, M. Applications for Bacteriophage Therapy during Pregnancy and the Perinatal Period. Front Microbiol. 2017, 8, 2660. [Google Scholar] [CrossRef] [Green Version]
- Chaudhry, W.N.; Concepcion-Acevedo, J.; Park, T.; Anleeb, S.; Bull, J.J.; Levin, B.R. Synergy and Order Effects of Antibiotics and Phages in Killing Pseudomonas aeruginosa Biofilms. PLoS ONE 2017, 12, e0168615. [Google Scholar] [CrossRef]
- Tzeng, A.; Tzeng, T.H.; Vasdev, S.; Korth, K.; Healey, T.; Parvizi, J.; Saleh, K.J. Treating periprosthetic joint infections as biofilms: Key diagnosis and management strategies. Diagn. Microbiol. Infect. Dis. 2015, 81, 192–200. [Google Scholar] [CrossRef]
- Chibeu, A.; Lingohr, E.J.; Masson, L.; Manges, A.; Harel, J.; Ackermann, H.; Kropinski, A.; Boerlin, P. Bacteriophages with the Ability to Degrade Uropathogenic Escherichia coli Biofilms. Viruses 2012, 4, 471–487. [Google Scholar] [CrossRef] [Green Version]
- Weber-Dabrowska, B.; Mulczyk, M.; Górski, A. Bacteriophages as an efficient therapy for antibiotic-resistant septicemia in man. Transplant. Proc. 2003, 35, 1385–1386. [Google Scholar] [CrossRef]
- Kutter, E.M.; Kuhl, S.J.; Abedon, S.T. Re-establishing a place for phage therapy in western medicine. Future Microbiol. 2015, 10, 685–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duplessis, C.; Stockelman, M.; Hamilton, T.; Merril, G.; Brownstein, M.; Bishop-lilly, K.; Schooley, R.; Henry, M.; Horne, B.; Sisson, B.; et al. A Case Series of Emergency Investigational New Drug Applications for Bacteriophages Treating Recalcitrant Multi-drug Resistant Bacterial Infections: Confirmed Safety and a Signal of Efficacy. J. Intensive Crit. Care 2019, 5, 11. [Google Scholar]
- Markoishvili, K.; Tsitlanadze, G.; Katsarava, R.; Morris, J.G., Jr.; Sulakvelidze, A. A novel sustained-release matrix based on biodegradable poly (ester amide)s and impregnated with bacteriophages and an antibiotic shows promise in management of infected venous stasis ulcers and other poorly healing wounds. Int. J. Dermatol. 2002, 41, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Rhoads, D.D.; Wolcott, R.D.; Kuskowski, M.A.; Wolcott, B.M.; Ward, L.S.; Sulakvelidze, A. Bacteriophage therapy of venous leg ulcers in humans: Results of a phase I safety trial. J. Wound Care. 2009, 18, 237–238. [Google Scholar] [CrossRef] [PubMed]
- Jikia, D.; Chkhaidze, N.; Imedashvili, E.; Mgaloblishvili, I.; Tsitlanadze, G.; Katsarava, R.; Glenn Morris, J., Jr.; Sulakvelidze, A. The use of a novel biodegradable preparation capable of the sustained release of bacteriophages and ciprofloxacin, in the complex treatment of multidrug-resistant Staphylococcus aureus-infected local radiation injuries caused by exposure to Sr90. Clin. Exp. Dermatol. 2005, 30, 23–26. [Google Scholar] [CrossRef]
- Marza, J.; Soothill, J.; Boydell, P.; Collyns, T. Multiplication of therapeutically administered bacteriophages in Pseudomonas aeruginosa infected patients. Burns 2006, 32, 644–666. [Google Scholar] [CrossRef]
- Abdul-Hassan, H.S.; El-Tahan, K.; Massoud, B.; Gomaa, R. Bacteriophage therapy of Pseudomonas burn wound sepsis. Ann. Med. Burn. Club. 1990, 3, 262–264. [Google Scholar]
- Rose, T.; Verbeken, G.; Vos, D.; Merabishvili, M.; Vaneechoutte, M.; Lavigne, R.; Jennes, S.; Zizi, M.; Pirnay, J. Experimental phage therapy of burn wound infection: Difficult first steps. Int. J. Burns. Trauma. 2014, 4, 66–73. [Google Scholar]
- Jault, P.; Leclerc, T.; Jennes, S.; Pirnay, J.; Que, Y.; Resch, G.; Rousseau, A.; Ravat, F.; Carsini, H.; LeFloch, R.; et al. Efficacy and tolerability of a cocktail of bacteriophages to treat burn wounds infected by Pseudomonas aeruginosa (PhagoBurn): A randomized, controlled, double-blind phase ½ trial. Lancet. Infect Dis. 2019, 19, 35–45. [Google Scholar] [CrossRef]
- Weber-Dabrowska, B.; Mulczyk, M.; Gorski, A. Bacteriophage therapy of bacterial infections: An update of our institute’s experience. Arch. Immunol. Ther. Exp. (Warsz) 2000, 48, 547–551. [Google Scholar]
- Morozova, V.V.; Kozlova, Y.N.; Ganichev, D.A.; Tikunova, N.V. Bacteriophage Treatment of Infected Diabetic Foot Ulcers. Methods Mol. Biol. 2018, 1693, 151–158. [Google Scholar] [PubMed]
- Fish, R.; Kutter, E.; Wheat, G.; Blasdel, B.; Kutateladze, M.; Kuhl, S. Compassionate Use of Bacteriophage Therapy for Foot Ulcer Treatment as an Effective Step for Moving Toward Clinical Trials. Methods Mol. Biol. 2018, 1693, 159–170. [Google Scholar] [PubMed]
- Fish, R.; Kutter, E.; Wheat, G.; Blasdel, B.; Kutateladze, M.; Kuhl, S. Bacteriophage treatment of intransigent diabetic toe ulcers: A case series. J. Wound Care 2016, 25, S27–S33. [Google Scholar] [CrossRef]
- Gupta, P.; Singh, H.; Shukla, V.; Nath, G.; Bhartiva, S. Bacteriophage Therapy of Chronic Nonhealing Wound: Clinical Study. Int. J. Low. Extrem. Wounds 2019, 18, 171–175. [Google Scholar] [CrossRef]
- Cisło, M.; Dabrowski, M.; Weber-Dabrowska, B.; Woytoń, A. Bacteriophage treatment of suppurative skin infections. Arch. Immunol. Ther. Exp. (Warsz) 1987, 35, 175–183. [Google Scholar]
- Slopek, S.; Durlakowa, I.; Weber-Dabrowska, B.; Kucharewicz-Krukowska, A.; Dabrowski, M.; Biskikewicz, R. Results of bacteriophage treatment of suppurative bacterial infections. I. General evaluation of the results. Arch. Immunol. Ther. Exp. (Warsz) 1983, 31, 267–291. [Google Scholar]
- Patel, D.; Bhartiva, S.; Kumar, R.; Shukla, V.; Nath, G. Use of Customized bacteriophages in the treatment of chronic nonhealing wounds: A prospective study. Int. J. Low Extrem. Wounds 2019. (Online ahead of print). [Google Scholar] [CrossRef]
- Henry, M.; Biswas, B.; Vincent, L.; Mokashi, V.; Schuch, R.; Bishop-Lilly, K.A.; Sozhamannan, S. Development of a high throughput assay for indirectly measuring phage growth using the OmniLog™ system. Bacterophage 2012, 2, 159–167. [Google Scholar] [CrossRef] [Green Version]
- Phillipson, C.; Voegtly, L.; Lueder, M.; Long, K.; Rice, G.; Frey, K.; Biswas, B.; Cer, R.; Hamilton, T.; Bishop-Lilly, K. Characterizing phage genomes for therapeutic applications. Viruses 2018, 10, 188. [Google Scholar] [CrossRef] [Green Version]
- Doss, J.; Culbertson, K.; Hahn, D.; Camacho, J.; Barekzi, N. A review of phage therapy against bacterial pathogens of aquatic and terrestrial organisms. Viruses 2017, 9, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Barcelo, C.; Arias-Sanchez, F.; Vasse, M.; Ramsayer, J.; Kaltz, O.; Hochberg, M.E. A window of opportunity to control the bacterial pathogen Pseudomonas aeruginosa combining antibiotics and phages. PLoS ONE 2014, 9, e106628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumaran, D.; Taha, M.; Yi, Q.; Ramirez-Arcos, S.; Diallo, J.S.; Carli, A.; Abdelbary, H. Does treatment order matter? Investigating the ability of bacteriophage to augment antibiotic activity against Staphylococcus aureus biofilms. Front Microbiol. 2018, 9, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.; Jo, Y.; Hwang, Y.J.; Hong, H.W.; Hong, S.S.; Park, K.; Myung, H. Phage-antibiotic synergy via delayed lysis. Appl. Environ. Microbiol. 2018, 84, e02085-18. [Google Scholar] [CrossRef] [Green Version]
- Kaur, P.; Gondil, V.; Chibber, S. A novel wound dressing consisting of PVA-SA hybrid hydrogel membrane for topical delivery of bacteriophages and antibiotics. Int. J. Pharm. 2019, 15, 572. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year Published | Wound Classification | Microbiology | Phage Characterization | Patient-# | Phage && Regimen (a). Dose ((b). Frequency (c). Duration | Follow-up | Efficacy Results Reported && (a). Clinical Healing (b). Microbiological Eradication (c). Safety Evaluation |
|---|---|---|---|---|---|---|---|---|
| (1). Slopek | 1983 | Skin infections (furunculosis, abscesses, and decubitus ulcers) | Numerous virulent infections | Unknown, but phages were personalized and targeted patient’s bacterial isolate in vitro. Additionally, phages administered orally | 20 | (a). Unk (b). Topically: TID Orally: TID (c). Unk | Unk1 | (a). An outstanding result manifest by complete recovery was achieved in 5 patients --14 patients achieving complete healing (accompanied by “liquidation of the suppurative process”). (b). Microbiological results mirror the clinical (c). Safety established overall. One adverse event, an allergic reaction was reported from local wound application |
| (2). Cislo | 1987 | Purulent Ulcers | Staphylococcus, Pseudomonas, Klebsiella, Proteus spp. and E. coli | Unknown, but phages were personalized and targeted patient’s bacterial isolate in vitro. Additionally, phages administered orally | 31 | (a). Unk 1 Dose (b). TID-QID 2 (c). 2–16 weeks | 2–16 weeks | (a). Outstanding therapeutic effect (wound healing) in 16 patients; Marked and transitory clinical improvement in 7 and 2 patients, respectively. (b). Microbiological results mirror the clinical (c). Safety established overall. Potential attributable adverse events ascribed to phage therapy included intensified local pain and eczematous changes. |
| (3). Abul-Hassan | 1990 | Burn-Mediated | Pseudomonas aeruginosa (PsA) | Unknown | 30 | (a). 1010 pfu/mL 3 (Impregnated Gauze) (b). TID (c). 5–17 days | 5–17 days | (a). Improvement in 15, slight improvement in 9, and no improvement in 6 patients respectively --Graft purchase in 18/30 patients (b). Sterile cultures in 12/30 patients (c). Safety established |
| (4). Weber-Dabrowska | 2000 | Burn-Mediated | S. aureus, and E. coli, Klebsiella, Proteus, and Pseudomonas spp. | Unknown, but phages were personalized and targeted patient’s bacterial isolate in vitro. Additionally, phages administered orally | 49 | (a). Unk (b). Unk topical Oral delivery TID (c). Unk | Unk | (a). Clinical resolution in 42/49 (86%) Improvement in the balance (7 patients) (b). Microbiological clearance in 42/49 (86%) Reduced bacterial burden in the balance (c). Safety established |
| (5). Markoishvilli | 2002 | Venous Stasis and uncharacterized “ulcers/wounds” | E. coli Proteus spp. Pseudomonas spp. Staphylococcus spp. | PhagoBioDerm Phages (106 pfu/cm2) targeting [PsA, E. coli, (S. aureus), Streptococcus, and Proteus spp.] | 96 | (a). # Dressings applied varied (based on wound size) (b). Reapplied PRN 4 (typically 3–7 days) (c). N/A | 6 days–15 months | (a). Clinical efficacy in 67/96 (70%) patients. Improvement (reduced ulcer size and elimination of purulent drainage in another 24 patients. (b). All 22 patients for whom microbiological data had been collected were in the completely healed group. (c). Safety established |
| (6). Jikia | 2005 | Radiation Injury | S. aureus | PhagoBioDerm The S. aureus isolates were susceptible to the phage preparation in this product | 2 | (a). # Dressings applied varied (based on wound size) (b). Reapplied PRN (c). N/A | 7 days | (a). Clinical wound healing in 2/2 (100%) subjects, both failing antecedent antibiotics (b). Microbiological eradication in 2/2 (100%) (c). Safety established |
| (7). Marza | 2006 | Burn-mediated | PsA | Derived by Dr. Soothill | 1 | (a). ~2 × 103 pfu Applied via 2 sterile paper discs (25 mm), then application to entire surface (b). × 2 doses (c). Unk | 3 days | (a). Clinical wound healing (partial) (b). Infectious eradication of PsA Facilitating a successful graft (c). Safety established |
| (8). Rhoades | 2009 | Venous Stasis Ulcers (infected or uninfected) | N/A5 [Wounds were not cultured to assess susceptibility to the phage constituents] | 8-phage cocktail (109 pfu/mL per phage) targeting Pseudomonas spp., E. coli spp., and S. aureus “WPP-201” | 39 (18 received phages) | (a). 4 mL Impregnated Dressing (b). Weekly (c). 12-weeks | 24 weeks | (a). Wound epithelialization achieved in 17/21 control patients and 12/18 treated patients (non-significant) (b). Microbiological Outcomes: N/A 5 (a phase I safety evaluation) (c). Safety established |
| (9). Rose | 2014 | Burn-mediated | MDR PsA or S. aureus | 3-phage cocktail targeting PsA and S. aureus “BFC-1” Please note that this cocktail was active against the strain populating the burn wound center | 9 patients (10 burn applications) | (a). 107 phages/cm2 (average dose) (b). × 1 dose (c). × 1 dose | 2 to 5 h | (a)/(b). Microbiological and Clinical Outcomes: [No change in the microbiological (bacterial) load from pre to post-biopsy wound sampling] (c). Safety established |
| (10). Fish | 2018 | Diabetic toe ulcers | S. aureus | S. aureus targeting phage “Sb-1” | 6 | (a). 107 to 108 pfu/mL Impregnated Dressings (b). Weekly (c). Variable | 7 week median | (a). Clinical wound healing in 6/6 (100%) patients (b). Microbiological data N/A (c). Safety established |
| (11). Jault | 2019 | Burn-mediated | PsA | 12-phage cocktail targeting PsA “PP1131” | 12-treated 13-placebo “efficacy population” | (a). 102 pfu/mL (b). Daily (c). 7 days | 21 days (14 days follow-up) | (a). Clinical Healing: N/A (b). Microbiological Endpoint: Reduced bacterial burden HR 6: 0.29, 95% CI 7 0.10–0.79; p = 0.018 favoring SOC 9 (1% sulfadiazine silver emulsion cream) for microbial burden (c). Safety established |
| (12). Gupta | 2019 | Purulent ulcers | E. coli, S. aureus, or PsA | Unknown (however, a personalized 3-phage cocktail was identified to target the organism in all cases). | 20 | (a). 109 pfu/mL (total pfu dependent upon wound area) (b). QOD 8 (c). 6–10 days | 3-months | (a). Clinical healing in 7/20 (35%) patients -20/20 patients experienced improvement (b). Microbiological sterility achieved in 20/20 (100%) patients (c). Safety established |
| (13). Patel | 2019 | Heterogeneous Diabetic ulcers (>50%) | Bacteria recovered at >10% E. coli (37.5%) PsA (31%) S. aureus (31%) Klebsiella pnuemonia (12.5%) | A personalized phage cocktail was identified to target the organism in all cases. Some were polyvalent targeting the multivalent bacterial wound infection. | 48 | (a). 500 µL/cm2 (109 pfu/mL) (b). QOD (c). 5 to 7 treatments | 3-months | (a). 39/48 (81%) cure (b). Microbiological eradication established in 48/48 (100%) (c). Safety established Increased lymphocytes observed |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duplessis, C.A.; Biswas, B. A Review of Topical Phage Therapy for Chronically Infected Wounds and Preparations for a Randomized Adaptive Clinical Trial Evaluating Topical Phage Therapy in Chronically Infected Diabetic Foot Ulcers. Antibiotics 2020, 9, 377. https://doi.org/10.3390/antibiotics9070377
Duplessis CA, Biswas B. A Review of Topical Phage Therapy for Chronically Infected Wounds and Preparations for a Randomized Adaptive Clinical Trial Evaluating Topical Phage Therapy in Chronically Infected Diabetic Foot Ulcers. Antibiotics. 2020; 9(7):377. https://doi.org/10.3390/antibiotics9070377
Chicago/Turabian StyleDuplessis, Christopher Anthony, and Biswajit Biswas. 2020. "A Review of Topical Phage Therapy for Chronically Infected Wounds and Preparations for a Randomized Adaptive Clinical Trial Evaluating Topical Phage Therapy in Chronically Infected Diabetic Foot Ulcers" Antibiotics 9, no. 7: 377. https://doi.org/10.3390/antibiotics9070377
APA StyleDuplessis, C. A., & Biswas, B. (2020). A Review of Topical Phage Therapy for Chronically Infected Wounds and Preparations for a Randomized Adaptive Clinical Trial Evaluating Topical Phage Therapy in Chronically Infected Diabetic Foot Ulcers. Antibiotics, 9(7), 377. https://doi.org/10.3390/antibiotics9070377