Best Helicobacter pylori Eradication Strategy in the Era of Antibiotic Resistance


Abstract
:1. Introduction
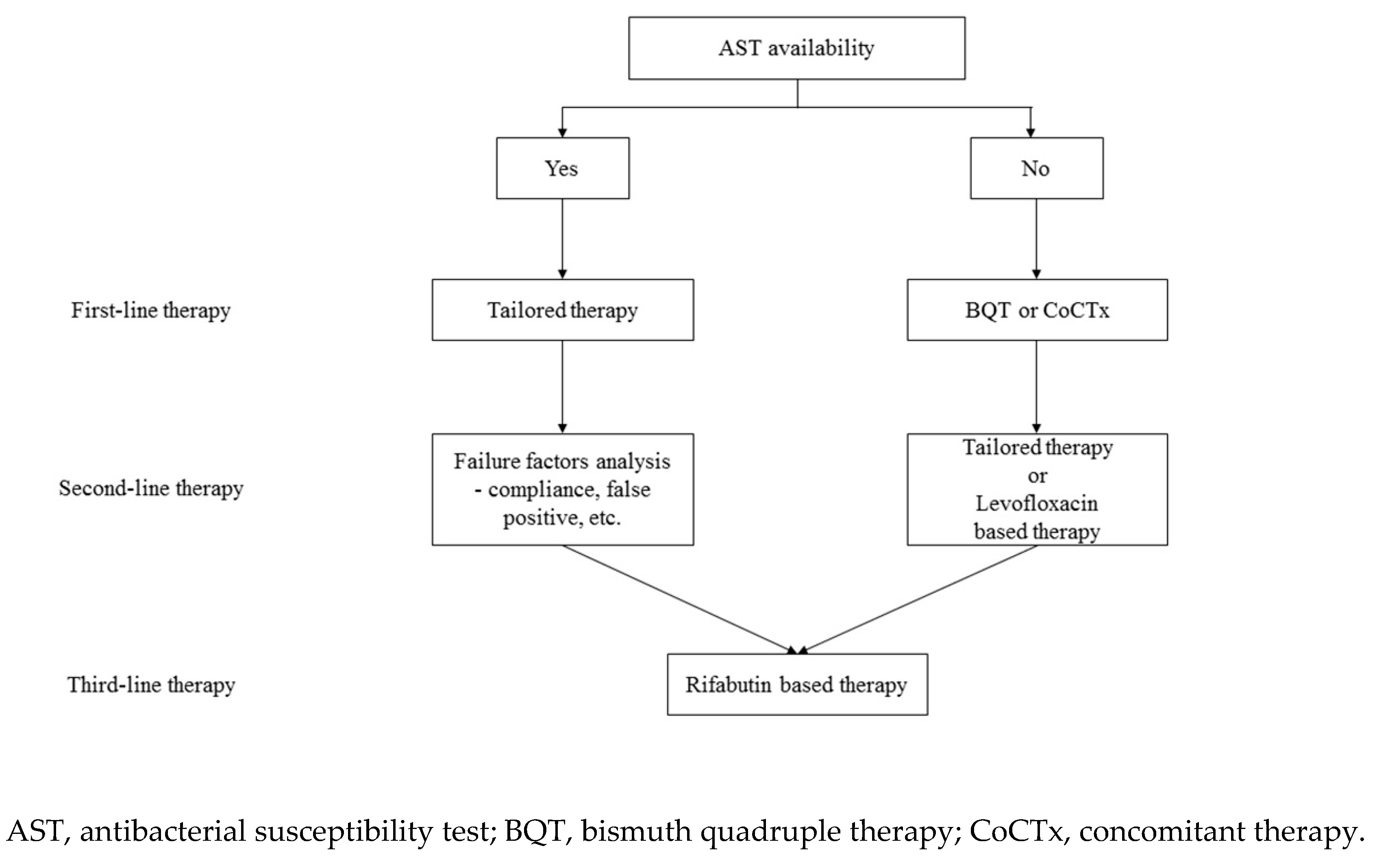
2. H. Pylori Treatment Based on AST Results
3. Bismuth Quadruple Therapy
4. Concomitant Therapy
5. Hybrid Therapy
6. Levofloxacin-Based Therapy
7. Rifabutin-Based Therapy
8. Potassium-Competitive Acid Blocker-Based Therapy
9. Treatments When Primary Therapy Fails
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kandulski, A.; Selgrad, M.; Malfertheiner, P. Helicobacter pylori infection: A clinical overview. Dig. Liver. Dis. 2008, 40, 619–626. [Google Scholar] [CrossRef] [PubMed]
- McColl, K.E. Clinical practice. Helicobacter pylori infection. N. Engl. J. Med. 2010, 362, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Plummer, M.; Franceschi, S.; Vignat, J.; Forman, D.; de Martel, C. Global burden of gastric cancer attributable to Helicobacter pylori. Int. J. Cancer 2015, 136, 487–490. [Google Scholar] [CrossRef]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef]
- Testerman, T.L.; Morris, J. Beyond the stomach: An updated view of Helicobacter pylori pathogenesis, diagnosis, and treatment. World J. Gastroenterol. 2014, 20, 12781–12808. [Google Scholar] [CrossRef]
- Lee, Y.C.; Chiang, T.H.; Chou, C.K.; Tu, Y.K.; Liao, W.C.; Wu, M.S.; Graham, D.Y. Association Between Helicobacter pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-analysis. Gastroenterology 2016, 150, 1113–1124. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Nishizawa, T.; Hibi, T. Helicobacter pylori eradication therapy. Future. Microbiol. 2010, 5, 639–648. [Google Scholar] [CrossRef]
- Kim, S.G.; Jung, H.K.; Lee, H.L.; Jang, J.Y.; Lee, H.; Kim, C.G.; Shin, W.G.; Shin, E.S.; Lee, Y.C. Korean College of Helicobacter and Upper Gastrointestinal Research. Korean J. Gastroenterol. 2013, 62, 3–26. [Google Scholar] [CrossRef] [Green Version]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology 2016, 151, 51–69. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Gisbert, J.P.; Gonzalez, L.; Calvet, X.; Garcia, N.; Lopez, T.; Roque, M.; Gabriel, R.; Pajares, J.M. Proton pump inhibitor, clarithromycin and either amoxycillin or nitroimidazole: A meta-analysis of eradication of Helicobacter pylori. Aliment. Pharmacol. Ther. 2000, 14, 1319–1328. [Google Scholar] [CrossRef]
- Current European concepts in the management of Helicobacter pylori infection The Maastricht Consensus Report. European Helicobacter pylori Study Group. Gut 1997, 41, 8–13. [CrossRef] [PubMed]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Choi, D.J.; Chung, J.W. Antibiotic treatment for Helicobacter pylori: Is the end coming? World J. Gastrointest. Pharmacol. Ther. 2015, 6, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2016, 43, 514–533. [Google Scholar] [CrossRef] [Green Version]
- Woo, H.Y.; Park, D.I.; Park, H.; Kim, M.K.; Kim, D.H.; Kim, I.S.; Kim, Y.J. Dual-priming oligonucleotide-based multiplex PCR for the detection of Helicobacter pylori and determination of clarithromycin resistance with gastric biopsy specimens. Helicobacter 2009, 14, 22–28. [Google Scholar] [CrossRef]
- Liou, J.M.; Chang, C.Y.; Chen, M.J.; Chen, C.C.; Fang, Y.J.; Lee, J.Y.; Wu, J.; Luo, J.; Liou, T.; Chang, W.; et al. The Primary Resistance of Helicobacter pylori in Taiwan after the National Policy to Restrict Antibiotic Consumption and Its Relation to Virulence Factors-A Nationwide Study. PLoS ONE 2015, 10, e0124199. [Google Scholar] [CrossRef]
- Lee, J.Y.; Park, K.S. Optimal First-Line Treatment for Helicobacter pylori Infection: Recent Strategies. Gastroenterol. Res. Pract. 2016, 2016, 9086581. [Google Scholar] [CrossRef]
- Alba, C.; Blanco, A.; Alarcon, T. Antibiotic resistance in Helicobacter pylori. Curr. Opin. Infect. Dis. 2017, 30, 489–497. [Google Scholar] [CrossRef]
- Hwang, T.J.; Kim, N.; Kim, H.B.; Lee, B.H.; Nam, R.H.; Park, J.H.; Lee, M.K.; Park, Y.S.; Lee, D.H.; Jung, H.C.; et al. Change in antibiotic resistance of Helicobacter pylori strains and the effect of A2143G point mutation of 23S rRNA on the eradication of H. pylori in a single center of Korea. J. Clin. Gastroenterol. 2010, 44, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Gerrits, M.M.; van Vliet, A.H.; Kuipers, E.J.; Kusters, J.G. Helicobacter pylori and antimicrobial resistance: Molecular mechanisms and clinical implications. Lancet Infect. Dis. 2006, 6, 699–709. [Google Scholar] [CrossRef]
- Megraud, F. H pylori antibiotic resistance: Prevalence, importance, and advances in testing. Gut 2004, 53, 1374–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulten, K.; Gibreel, A.; Skold, O.; Engstrand, L. Macrolide resistance in Helicobacter pylori: Mechanism and stability in strains from clarithromycin-treated patients. Antimicrob. Agents. Chemother. 1997, 41, 2550–2553. [Google Scholar] [CrossRef] [Green Version]
- Stone, G.G.; Shortridge, D.; Versalovic, J.; Beyer, J.; Flamm, R.K.; Graham, D.Y.; Ghoneim, A.T.; Tanaka, S.K. A PCR-oligonucleotide ligation assay to determine the prevalence of 23S rRNA gene mutations in clarithromycin-resistant Helicobacter pylori. Antimicrob. Agents Chemother. 1997, 41, 712–714. [Google Scholar] [CrossRef] [Green Version]
- Alarcon, T.; Domingo, D.; Prieto, N.; Lopez-Brea, M. Clarithromycin resistance stability in Helicobacter pylori: Influence of the MIC and type of mutation in the 23S rRNA. J. Antimicrob. Chemother. 2000, 46, 613–616. [Google Scholar] [CrossRef] [Green Version]
- Van Doorn, L.J.; Glupczynski, Y.; Kusters, J.G.; Megraud, F.; Midolo, P.; Maggi-Solca, N.; Queiroz, D.M.; Nouhan, N.; Stet, E.; Quint, W.G. Accurate prediction of macrolide resistance in Helicobacter pylori by a PCR line probe assay for detection of mutations in the 23S rRNA gene: Multicenter validation study. Antimicrob. Agents Chemother. 2001, 45, 1500–1504. [Google Scholar] [CrossRef] [Green Version]
- Kato, S.; Fujimura, S.; Udagawa, H.; Shimizu, T.; Maisawa, S.; Ozawa, K.; Iinuma, K. Antibiotic resistance of Helicobacter pylori strains in Japanese children. J. Clin. Microbiol. 2002, 40, 649–653. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.H.; Wong, B.C.; Mukhopadhyay, A.K.; Berg, D.E.; Cho, C.H.; Lai, K.C.; Hu, W.H.; Fung, F.M.; Hui, W.M.; Lam, S.K. High prevalence of Helicobacter pylori infection with dual resistance to metronidazole and clarithromycin in Hong Kong. Aliment. Pharmacol. Ther. 2000, 14, 901–910. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Kim, J.I.; Cheung, D.Y.; Kim, T.H.; Jun, E.J.; Oh, J.H.; Chung, W.C.; Kim, B.; Kim, S.S.; Park, S.; et al. Eradication of Helicobacter pylori according to 23S ribosomal RNA point mutations associated with clarithromycin resistance. J. Infect. Dis. 2013, 208, 1123–1130. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.H.; Jeon, S.R.; Kim, H.G.; Jin, S.Y.; Park, S. Cost-effectiveness of a tailored Helicobacter pylori eradication strategy based on the presence of a 23S ribosomal RNA point mutation that causes clarithromycin resistance in Korean patients. J. Gastroenterol. Hepatol. 2019, 34, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Papastergiou, V.; Mathou, N.; Licousi, S.; Evgenidi, A.; Paraskeva, K.D.; Giannakopoulos, A.; Stavrou, P.; Platsouka, E.; Karagiannis, J.A. Seven-day genotypic resistance-guided triple Helicobacter pylori eradication therapy can be highly effective. Ann. Gastroenterol. 2018, 31, 198–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosme, A.; Montes, M.; Ibarra, B.; Tamayo, E.; Alonso, H.; Mendarte, U.; Lizasoan, J.; Herreros-Villanueva, M.; Bujanda, L. Antimicrobial susceptibility testing before first-line treatment for Helicobacter pylori infection in patients with dual or triple antibiotic resistance. World J. Gastroenterol. 2017, 23, 3367–3373. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Kim, N.; Nam, R.H.; Lee, S.M.; Kwon, Y.H.; Sohn, S.D.; Kim, J.M.; Lee, D.H.; Jung, H.C. Favorable outcomes of culture-based Helicobacter pylori eradication therapy in a region with high antimicrobial resistance. Helicobacter 2019, 24, e12561. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Long, X.; Ji, Y.; Liang, X.; Li, D.; Gao, H.; Xu, B.; Liu, M.; Chen, Y.; Sun, Y. Randomised controlled trial: Susceptibility-guided therapy versus empiric bismuth quadruple therapy for first-line Helicobacter pylori treatment. Aliment. Pharmacol. Ther. 2019, 49, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Blumel, B.; Goelz, H.; Kist, M.; Glocker, E.O. Retrospective study on outcome of salvage Helicobacter pylori eradication therapies based on molecular genetic susceptibility testing. Helicobacter 2018, 23, e12494. [Google Scholar] [CrossRef]
- Bhakta, D.; Graham, D.Y.; Chan, J.; El-Serag, H.B. Lessons From Using Culture-Guided Treatment After Referral for Multiple Treatment Failures for Helicobacter pylori Infection. Clin. Gastroenterol. Hepatol. 2018, 16, 1531–1532. [Google Scholar] [CrossRef]
- Baylina, M.; Munoz, N.; Sanchez-Delgado, J.; Lopez-Gongora, S.; Calvet, X.; Puig, I. Systematic review: Would susceptibility-guided treatment achieve acceptable cure rates for second-line Helicobacter pylori therapy as currently practiced? Helicobacter 2019, 24, e12584. [Google Scholar] [CrossRef]
- Liou, J.M.; Chen, P.Y.; Luo, J.C.; Lee, J.Y.; Chen, C.C.; Fang, Y.J.; Yang, T.H.; Chang, C.Y.; Bair, M.J.; Chenet, M.J.; et al. Efficacies of Genotypic Resistance-Guided vs Empirical Therapy for Refractory Helicobacter pylori Infection. Gastroenterology 2018, 155, 1109–1119. [Google Scholar] [CrossRef]
- Li, B.Z.; Threapleton, D.E.; Wang, J.Y.; Xu, J.M.; Yuan, J.Q.; Zhang, C.; Li, P.; Ye, Q.L.; Guo, B.; Mao, C.; et al. Comparative effectiveness and tolerance of treatments for Helicobacter pylori: Systematic review and network meta-analysis. BMJ 2015, 351, h4052. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.S.; Hung, I.F.; Seto, W.K.; Tong, T.; Hsu, A.S.; Lam, F.Y.; But, D.Y.K.; Wong, S.Y.; Leung, W.K. Ten day sequential versus 10 day modified bismuth quadruple therapy as empirical firstline and secondline treatment for Helicobacter pylori in Chinese patients: An open label, randomised, crossover trial. Gut 2014, 63, 1410–1415. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.I.; Tsay, F.W.; Graham, D.Y.; Tsai, T.J.; Tsai, K.W.; Kao, J.Y.; Peng, N.J.; Kuo, C.H.; Kao, S.S.; Wang, H.M.; et al. Equivalent Efficacies of Reverse Hybrid and Bismuth Quadruple Therapies in Eradication of Helicobacter pylori Infection in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2018, 16, 1427–1433. [Google Scholar] [CrossRef] [PubMed]
- Macias-Garcia, F.; Baston-Rey, I.; de la Iglesia-Garcia, D.; Calvino-Suarez, C.; Nieto-Garcia, L.; Dominguez-Munoz, J.E. Bismuth-containing quadruple therapy versus concomitant quadruple therapy as first-line treatment for Helicobacter pylori infection in an area of high resistance to clarithromycin: A prospective, cross-sectional, comparative, open trial. Helicobacter 2019, 24, e12546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.J.; Chung, J.W.; Woo, H.S.; Kim, S.Y.; Kim, J.H.; Kim, Y.J.; Kim, K.O.; Kwon, K.A.; Park, D.K. Two-week bismuth-containing quadruple therapy and concomitant therapy are effective first-line treatments for Helicobacter pylori eradication: A prospective open-label randomized trial. World. J. Gastroenterol. 2019, 25, 6790–6798. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Lee, S.Y.; Kim, J.H.; Sung, I.K.; Park, H.S. Efficacy and safety of twice a day, bismuth-containing quadruple therapy using high-dose tetracycline and metronidazole for second-line Helicobacter pylori eradication. Helicobacter 2020, 25, e12683. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Pan, X.; Li, Y.; Wang, H.; Du, Y.; Xu, J.; Wang, J.; Zeng, Z.; Chen, Y.; Zhang, G.; et al. New single capsule of bismuth, metronidazole and tetracycline given with omeprazole versus quadruple therapy consisting of bismuth, omeprazole, amoxicillin and clarithromycin for eradication of Helicobacter pylori in duodenal ulcer patients: A Chinese prospective, randomized, multicentre trial. J. Antimicrob. Chemother. 2018, 73, 1681–1687. [Google Scholar]
- Fiorini, G.; Zullo, A.; Saracino, I.M.; Gatta, L.; Pavoni, M.; Vaira, D. Pylera and sequential therapy for first-line Helicobacter pylori eradication: A culture-based study in real clinical practice. Eur. J. Gastroenterol. Hepatol. 2018, 30, 621–625. [Google Scholar] [CrossRef]
- Nyssen, O.P.; McNicholl, A.G.; Gisbert, J.P. Meta-analysis of three-in-one single capsule bismuth-containing quadruple therapy for the eradication of Helicobacter pylori. Helicobacter 2019, 24, e12570. [Google Scholar] [CrossRef]
- Kim, S.E.; Roh, J.H.; Park, M.I.; Park, S.J.; Moon, W.; Kim, J.H.; Jung, K.; Heo, J.J. Effect of 7-day Bismuth Quadruple Therapy versus 14-day Moxifloxacin Triple Therapy for Second-line Helicobacter pylori Eradication Therapy. Korean. J. Gastroenterol. 2019, 73, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Boyanova, L.; Mitov, I. Geographic map and evolution of primary Helicobacter pylori resistance to antibacterial agents. Expert. Rev. Anti. Infect. Ther. 2010, 8, 59–70. [Google Scholar] [CrossRef]
- Megraud, F.; Coenen, S.; Versporten, A.; Kist, M.; Lopez-Brea, M.; Hirschl, A.M.; Andersen, L.P.; Goossens, H.; Glupczynski, Y.; Study Group participants. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut 2013, 62, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Fischbach, L.; Evans, E.L. Meta-analysis: The effect of antibiotic resistance status on the efficacy of triple and quadruple first-line therapies for Helicobacter pylori. Aliment. Pharmacol. Ther. 2007, 26, 343–357. [Google Scholar] [CrossRef] [PubMed]
- Venerito, M.; Krieger, T.; Ecker, T.; Leandro, G.; Malfertheiner, P. Meta-analysis of bismuth quadruple therapy versus clarithromycin triple therapy for empiric primary treatment of Helicobacter pylori infection. Digestion 2013, 88, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Mantzaris, G.J.; Petraki, K.; Archavlis, E.; Amberiadis, P.; Christoforidis, P.; Kourtessas, D.; Chiotakakou, E.; Triantafyllou, G. Omeprazole triple therapy versus omeprazole quadruple therapy for healing duodenal ulcer and eradication of Helicobacter pylori infection: A 24-month follow-up study. Eur. J. Gastroenterol. Hepatol. 2002, 14, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Calvet, X. Review article: Non-bismuth quadruple (concomitant) therapy for eradication of Helicobater pylori. Aliment. Pharmacol. Ther. 2011, 34, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Essa, A.S.; Kramer, J.R.; Graham, D.Y.; Treiber, G. Meta-analysis: Four-drug, three-antibiotic, non-bismuth-containing “concomitant therapy” versus triple therapy for Helicobacter pylori eradication. Helicobacter 2009, 14, 109–118. [Google Scholar] [CrossRef] [Green Version]
- Gisbert, J.P.; Calvet, X. Update on non-bismuth quadruple (concomitant) therapy for eradication of Helicobacter pylori. Clin. Exp. Gastroenterol. 2012, 5, 23–34. [Google Scholar]
- Chen, M.J.; Chen, C.C.; Chen, Y.N.; Chen, C.C.; Fang, Y.J.; Lin, J.T.; Wu, M.S.; Liou, J.M.; Taiwan Gastrointestinal Disease Helicobacter Consortium. Systematic Review with Meta-Analysis: Concomitant Therapy vs. Triple Therapy for the First-Line Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2018, 113, 1444–1457. [Google Scholar] [CrossRef]
- Molina-Infante, J.; Pazos-Pacheco, C.; Vinagre-Rodriguez, G.; Perez-Gallardo, B.; Duenas-Sadornil, C.; Hernandez-Alonso, M.; Gonzalez-Garcia, G.; Mateos-Rodriguez, J.M.; Fernandez-Bermejo, M.; Gisbert, J.P. Nonbismuth quadruple (concomitant) therapy: Empirical and tailored efficacy versus standard triple therapy for clarithromycin-susceptible Helicobacter pylori and versus sequential therapy for clarithromycin-resistant strains. Helicobacter 2012, 17, 269–276. [Google Scholar] [CrossRef]
- Jung, Y.S.; Park, C.H.; Park, J.H.; Nam, E.; Lee, H.L. Efficacy of Helicobacter pylori eradication therapies in Korea: A systematic review and network meta-analysis. Helicobacter 2017, 22. [Google Scholar] [CrossRef]
- Chung, J.W.; Han, J.P.; Kim, K.O.; Kim, S.Y.; Hong, S.J.; Kim, T.H.; Kim, C.W.; Kim, J.S.; Kim, B.W.; Bang, B.W.; et al. Ten-day empirical sequential or concomitant therapy is more effective than triple therapy for Helicobacter pylori eradication: A multicenter, prospective study. Dig. Liver. Dis. 2016, 48, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Park, S.M.; Kim, J.S.; Kim, B.W.; Ji, J.S.; Choi, H. Randomized clinical trial comparing 10- or 14-day sequential therapy and 10- or 14-day concomitant therapy for the first line empirical treatment of Helicobacter pylori infection. J. Gastroenterol. Hepatol. 2017, 32, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Lee, S.W.; Choe, J.W.; Jung, S.W.; Hyun, J.J.; Jung, Y.K.; Koo, J.S.; Yim, H.J. Helicobacter pylori eradication rates of concomitant and sequential therapies in Korea. Helicobacter 2017, 22, e12441. [Google Scholar] [CrossRef] [PubMed]
- Ang, T.L.; Fock, K.M.; Song, M.; Ang, D.; Kwek, A.B.; Ong, J.; Tan, J.; Teo, E.K.; Dhamodaran, S. Ten-day triple therapy versus sequential therapy versus concomitant therapy as first-line treatment for Helicobacter pylori infection. J. Gastroenterol. Hepatol. 2015, 30, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- McNicholl, A.G.; Marin, A.C.; Molina-Infante, J.; Castro, M.; Barrio, J.; Ducons, J.; Calvet, X.; Coba, C.; Montoro, M.; Bory, F.; et al. Randomised clinical trial comparing sequential and concomitant therapies for Helicobacter pylori eradication in routine clinical practice. Gut 2014, 63, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Gatta, L.; Vakil, N.; Vaira, D.; Scarpignato, C. Global eradication rates for Helicobacter pylori infection: Systematic review and meta-analysis of sequential therapy. BMJ 2013, 347, f4587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, L.; Deng, T.; Luo, H. Meta-analysis of sequential, concomitant and hybrid therapy for Helicobacter pylori eradication. Intern. Med. 2015, 54, 703–710. [Google Scholar] [CrossRef] [Green Version]
- Zullo, A.; Scaccianoce, G.; De Francesco, V.; Ruggiero, V.; D’Ambrosio, P.; Castorani, L.; Bonfrate, L.; Vannella, L.; Hassan, C.; Portincasa, P. Concomitant, sequential, and hybrid therapy for H. pylori eradication: A pilot study. Clin. Res. Hepatol. Gastroenterol. 2013, 37, 647–650. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lee, S.W.; Hyun, J.J.; Jung, S.W.; Koo, J.S.; Yim, H.J.; Park, J.J.; Chun, H.J.; Choi, J.H. Comparative study of Helicobacter pylori eradication rates with 5-day quadruple “concomitant” therapy and 7-day standard triple therapy. J. Clin. Gastroenterol. 2013, 47, 21–24. [Google Scholar] [CrossRef]
- Lim, J.H.; Lee, D.H.; Choi, C.; Lee, S.T.; Kim, N.; Jeong, S.H.; Kim, J.W.; Hwang, J.H.; Park, Y.S.; Lee, S.H.; et al. Clinical outcomes of two-week sequential and concomitant therapies for Helicobacter pylori eradication: A randomized pilot study. Helicobacter 2013, 18, 180–186. [Google Scholar] [CrossRef]
- Guevara, B.; Cogdill, A.G. Helicobacter pylori: A Review of Current Diagnostic and Management Strategies. Dig. Dis. Sci. 2020, 65, 1917–1931. [Google Scholar] [CrossRef]
- Graham, D.Y.; Lee, Y.C.; Wu, M.S. Rational Helicobacter pylori therapy: Evidence-based medicine rather than medicine-based evidence. Clin. Gastroenterol. Hepatol. 2014, 12, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Wang, Y.H.; Lv, Z.F.; Xiong, H.F.; Wang, H.; Yang, Y.; Xie, Y. Review: Efficacy and safety of hybrid therapy for Helicobacter pylori infection: A systematic review and meta-analysis. Helicobacter 2015, 20, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Molina-Infante, J.; Romano, M.; Fernandez-Bermejo, M.; Federico, A.; Gravina, A.G.; Pozzati, L.; Garcia-Abadia, E.; Vinagre-Rodriguez, G.; Martinez-Alcala, C.; Hernandez-Alonso, M.; et al. Optimized nonbismuth quadruple therapies cure most patients with Helicobacter pylori infection in populations with high rates of antibiotic resistance. Gastroenterology 2013, 145, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Georgopoulos, S.D.; Papastergiou, V.; Martinez-Gonzalez, B.; Xirouchakis, E.; Familias, I.; Sgouras, D.; Mentis, A.; Karatapanis, S. Hybrid therapy as first-line regimen for Helicobacter pylori eradication in a high clarithromycin resistance area: A prospective open-label trial. Ann. Gastroenterol. 2018, 31, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Fu, W.; Zhou, L. Cefuroxime, levofloxacin, esomeprazole, and bismuth as first-line therapy for eradicating Helicobacter pylori in patients allergic to penicillin. BMC Gastroenterol. 2019, 19, 132. [Google Scholar] [CrossRef] [PubMed]
- Auttajaroon, J.; Vilaichone, R.K.; Chotivitayatarakorn, P.; Mahachai, V. Once-daily rabeprazole, levofloxacin, clarithromycin-MR, and bismuth for Helicobacter pylori eradication: A randomized study of 7 or 14 days (ONCE study). Helicobacter 2019, 24, e12615. [Google Scholar] [CrossRef] [PubMed]
- Gan, H.Y.; Peng, T.L.; Huang, Y.M.; Su, K.H.; Zhao, L.L.; Yao, L.Y.; Yang, R.J. Efficacy of two different dosages of levofloxacin in curing Helicobacter pylori infection: A Prospective, Single-Center, randomized clinical trial. Sci. Rep. 2018, 8, 9045. [Google Scholar] [CrossRef]
- Ciccaglione, A.F.; Di Giulio, M.; Di Lodovico, S.; Di Campli, E.; Cellini, L.; Marzio, L. Bovine lactoferrin enhances the efficacy of levofloxacin-based triple therapy as first-line treatment of Helicobacter pylori infection: An in vitro and in vivo study. J. Antimicrob. Chemother. 2019, 74, 1069–1077. [Google Scholar] [CrossRef] [Green Version]
- Basu, P.P.; Rayapudi, K.; Pacana, T.; Shah, N.J.; Krishnaswamy, N.; Flynn, M. A randomized study comparing levofloxacin, omeprazole, nitazoxanide, and doxycycline versus triple therapy for the eradication of Helicobacter pylori. Am. J. Gastroenterol. 2011, 106, 1970–1975. [Google Scholar] [CrossRef] [Green Version]
- Fallone, C.A.; Moss, S.F.; Malfertheiner, P. Reconciliation of Recent Helicobacter pylori Treatment Guidelines in a Time of Increasing Resistance to Antibiotics. Gastroenterology 2019, 157, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Suzuki, H. Update on quinolone-containing rescue therapies for Helicobacter pylori infection. World J. Gastroenterol. 2020, 26, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- Sue, S.; Shibata, W.; Sasaki, T.; Kaneko, H.; Irie, K.; Kondo, M.; Maeda, S. Randomized trial of vonoprazan-based versus proton-pump inhibitor-based third-line triple therapy with sitafloxacin for Helicobacter pylori. J. Gastroenterol. Hepatol. 2019, 34, 686–692. [Google Scholar] [CrossRef]
- Suzuki, H.; Nishizawa, T.; Muraoka, H.; Hibi, T. Sitafloxacin and garenoxacin may overcome the antibiotic resistance of Helicobacter pylori with gyrA mutation. Antimicrob. Agents. Chemother. 2009, 53, 1720–1721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miftahussurur, M.; Waskito, L.A.; Syam, A.F.; Nusi, I.A.; Siregar, G.; Richardo, M.; Bakry, A.F.; Rezkitha, Y.A.A.; Wibawa, I.D.N.; Yamaoka, Y. Alternative eradication regimens for Helicobacter pylori infection in Indonesian regions with high metronidazole and levofloxacin resistance. Infect. Drug. Resist. 2019, 12, 345–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miftahussurur, M.; Aftab, H.; Shrestha, P.K.; Sharma, R.P.; Subsomwong, P.; Waskito, L.A.; Doohan, D.; Fauzia, K.A.; Yamaoka, Y. Effective therapeutic regimens in two South Asian countries with high resistance to major Helicobacter pylori antibiotics. Antimicrob. Resist. Infect. Control 2019, 8, 40. [Google Scholar] [CrossRef] [Green Version]
- Gisbert, J.P.; Calvet, X. Review article: Rifabutin in the treatment of refractory Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2012, 35, 209–221. [Google Scholar] [CrossRef]
- Heep, M.; Beck, D.; Bayerdorffer, E.; Lehn, N. Rifampin and rifabutin resistance mechanism in Helicobacter pylori. Antimicrob. Agents. Chemother. 1999, 43, 1497–1499. [Google Scholar] [CrossRef] [Green Version]
- Ribaldone, D.G.; Fagoonee, S.; Astegiano, M.; Durazzo, M.; Morgando, A.; Sprujevnik, T.; Giordanino, C.; Baronio, M.; Angelis, C.D.; Saracco, G.M.; et al. Rifabutin-Based Rescue Therapy for Helicobacter pylori Eradication: A Long-Term Prospective Study in a Large Cohort of Difficult-to-Treat Patients. J. Clin. Med. 2019, 8, 199. [Google Scholar] [CrossRef] [Green Version]
- Akada, J.K.; Shirai, M.; Fujii, K.; Okita, K.; Nakazawa, T. In vitro anti-Helicobacter pylori activities of new rifamycin derivatives, KRM-1648 and KRM-1657. Antimicrob. Agents. Chemother. 1999, 43, 1072–1076. [Google Scholar] [CrossRef] [Green Version]
- Kunin, C.M. Antimicrobial activity of rifabutin. Clin. Infect. Dis. 1996, 22 (Suppl. 1:S3-13), 30. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.; Kim, N.; Park, Y.H.; Hwang, Y.J.; Kwon, S.; Na, G.; Choi, J.Y.; Kang, J.B.; Kim, H.R.; Kim, J.W.; et al. Rifabutin-based Fourth and Fifth-line Rescue Therapy in Patients with for Helicobacter pylori Eradication Failure. Korean. J. Gastroenterol. 2017, 69, 109–118. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.Y.; Canaan, Y.; Maher, J.; Wiener, G.; Hulten, K.G.; Kalfus, I.N. Rifabutin-Based Triple Therapy (RHB-105) for Helicobacter pylori Eradication: A Double-Blind, Randomized, Controlled Trial. Ann. Intern. Med. 2020, 172, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Bock, H.; Koop, H.; Lehn, N.; Heep, M. Rifabutin-based triple therapy after failure of Helicobacter pylori eradication treatment: Preliminary experience. J. Clin. Gastroenterol. 2000, 31, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Suzuki, H.; Nishizawa, T.; Kaneko, F.; Ootani, S.; Muraoka, H.; Saito, Y.; Kobayashi, I.; Hibi, T. Past rifampicin dosing determines rifabutin resistance of Helicobacter pylori. Digestion 2009, 79, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.Y.; Munson, K.B.; Marcus, E.A.; Lambrecht, N.W.; Sachs, G. The binding selectivity of vonoprazan (TAK-438) to the gastric H+, K+ -ATPase. Aliment. Pharmacol. Ther. 2015, 42, 1315–1326. [Google Scholar] [CrossRef] [Green Version]
- Park, J.Y.; Kim, J.G. [New Helicobacter pylori Eradication Therapies]. Korean. J. Gastroenterol. 2018, 72, 237–244. [Google Scholar] [CrossRef]
- Sachs, G.; Scott, D.R.; Wen, Y. Gastric infection by Helicobacter pylori. Curr. Gastroenterol. Rep. 2011, 13, 540–546. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.Y.; Dore, M.P. Update on the Use of Vonoprazan: A Competitive Acid Blocker. Gastroenterology 2018, 154, 462–466. [Google Scholar] [CrossRef] [Green Version]
- Lyu, Q.J.; Pu, Q.H.; Zhong, X.F.; Zhang, J. Efficacy and Safety of Vonoprazan-Based versus Proton Pump Inhibitor-Based Triple Therapy for Helicobacter pylori Eradication: A Meta-Analysis of Randomized Clinical Trials. Biomed. Res. Int. 2019, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Murakami, K.; Sakurai, Y.; Shiino, M.; Funao, N.; Nishimura, A.; Asaka, M. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: A phase III, randomised, double-blind study. Gut 2016, 65, 1439–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Oshima, T.; Horikawa, T.; Tozawa, K.; Tomita, T.; Fukui, H.; Watari, J.; Miwa, H. Systematic review with meta-analysis: Vonoprazan, a potent acid blocker, is superior to proton-pump inhibitors for eradication of clarithromycin-resistant strains of Helicobacter pylori. Helicobacter 2018, 23, e12495. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, H.; Yoshino, K.; Ando, K.; Nomura, Y.; Ohta, K.; Satoh, K.; Ichiishi, E.; Ishizuka, A.; Otake, T.; Kohgo, Y.; et al. Vonoprazan-based triple therapy is non-inferior to susceptibility-guided proton pump inhibitor-based triple therapy for Helicobacter pylori eradication. Ann. Clin. Microbiol Antimicrob. 2018, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Gotoda, T.; Kusano, C.; Ikehara, H.; Ichijima, R.; Ohyauchi, M.; Ito, H.; Kawamura, M.; Ogata, Y.; Ohtaka, M.; et al. Seven-day vonoprazan and low-dose amoxicillin dual therapy as first-line Helicobacter pylori treatment: A multicentre randomised trial in Japan. Gut 2020, 69, 1019–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.J.; Lee, H.; Lee, Y.C.; Jeon, S.W.; Kim, G.H.; Kim, H.S.; Sung, J.K.; Lee, D.H.; Kim, H.U.; Park, M.I.; et al. Ten-Day Concomitant, 10-Day Sequential, and 7-Day Triple Therapy as First-Line Treatment for Helicobacter pylori Infection: A Nationwide Randomized Trial in Korea. Gut. Liver. 2019, 13, 531–540. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Ye, Z.; Wang, Y.; Zhang, Y.; Tang, Z.; Yan, W.; Jiang, Y.; Huang, Y. Comparison of four different regimens against Helicobacter pylori as a first-line treatment: A prospective, cross-sectional, comparative, open trial in Chinese children. Helicobacter 2020, 25, e12679. [Google Scholar] [CrossRef] [Green Version]
- Bang, C.S.; Lim, H.; Jeong, H.M.; Shin, W.G.; Choi, J.H.; Soh, J.S.; Kang, H.S.; Yang, Y.J.; Hong, J.T.; Shin, S.P.; et al. Amoxicillin or tetracycline in bismuth-containing quadruple therapy as first-line treatment for Helicobacter pylori infection. Gut Microbes 2020, 11, 1314–1323. [Google Scholar] [CrossRef]
- Romano, M.; Gravina, A.G.; Nardone, G.; Federico, A.; Dallio, M.; Martorano, M.; Mucherino, C.; Romiti, A.; Avallone, L.; Granata, L.; et al. Non-bismuth and bismuth quadruple therapies based on previous clarithromycin exposure are as effective and safe in an area of high clarithromycin resistance: A real-life study. Helicobacter 2020, 25, e12694. [Google Scholar] [CrossRef]
- Tai, W.C.; Liang, C.M.; Bi, K.W.; Kuo, C.M.; Lu, L.S.; Wu, C.K.; Yang, S.C.; Kuo, Y.H.; Lee, C.H.; Huang, C.F.; et al. A comparison between dexlansoprazole modified release-based and lansoprazole-based nonbismuth quadruple (concomitant) therapy for first-line Helicobacter pylori eradication: A prospective randomized trial. Infect. Drug. Resist. 2019, 12, 2923–2931. [Google Scholar] [CrossRef] [Green Version]
- Hsu, P.I.; Tsay, F.W.; Kao, J.Y.; Peng, N.J.; Tsai, K.W.; Tsai, T.J.; Kuo, C.H.; Kao, S.S.; Wang, H.M.; Chen, Y.H.; et al. Equivalent efficacies of reverse hybrid and concomitant therapies in first-line treatment of Helicobacter pylori infection. J. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef]
- Myint, N.; Zaw, T.T.; Sain, K.; Waiyan, S.; Danta, M.; Cooper, D.; Aung, N.M.; Kyi, M.M.; Hanson, J. Sequential Helicobacter pylori eradication therapy in Myanmar; a randomized clinical trial of efficacy and tolerability. J. Gastroenterol. Hepatol. 2020, 35, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Zullo, A.; Fiorini, G.; Scaccianoce, G.; Portincasa, P.; De Francesco, V.; Vassallo, R.; Urban, F.; Monica, F.; Mogavero, G.; Amato, A.; et al. Sequential therapy for first-line Helicobacter pylori eradication: 10- or 14-day regimen? J. Gastrointestin. Liver. Dis. 2019, 28, 11–14. [Google Scholar] [CrossRef]
- Tsay, F.W.; Wu, D.C.; Yu, H.C.; Kao, S.S.; Lin, K.H.; Cheng, J.S.; Wang, H.M.; Chen, W.C.; Sun, W.C.; Tsai, K.W.; et al. A Randomized Controlled Trial Shows that both 14-Day Hybrid and Bismuth Quadruple Therapies Cure Most Patients with Helicobacter pylori Infection in Populations with Moderate Antibiotic Resistance. Antimicrob. Agents. Chemother. 2017, 61, e00140-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishida, T.; Tsujii, Y.; Okamoto, A.; Tomita, R.; Higaki, Y.; Osugi, N.; Sugimoto, A.; Takahashi, K.; Mukai, K.; Nakamatsu, D.; et al. A Triple-Drug Blister-Packaged Drug with Vonoprazan Improves First-Line Eradication of Helicobacter pylori in Elderly Patients: A Retrospective Propensity Score-Matched Cohort Study. Digestion 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Huang, Y.; Liang, X.; Ji, Y.; Yu, L.; Lu, H. Susceptibility-guided therapy for Helicobacter pylori-infected penicillin-allergic patients: A prospective clinical trial of first-line and rescue therapies. Helicobacter 2020, 25, e12699. [Google Scholar] [CrossRef]
- Kim, S.G.; Jung, H.K.; Lee, H.L.; Jang, J.Y.; Lee, H.; Kim, C.G.; Shin, W.G.; Shin, E.S.; Lee, Y.C.; Korean College of Helicobacter and Upper Gastrointestinal Research. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. J. Gastroenterol. Hepatol. 2014, 29, 1371–1386. [Google Scholar] [CrossRef]
- Kato, M.; Ota, H.; Okuda, M.; Kikuchi, S.; Satoh, K.; Shimoyama, T.; Suzuki, H.; Handa, O.; Furuta, T.; Mabe, K.; et al. Guidelines for the management of Helicobacter pylori infection in Japan: 2016 Revised Edition. Helicobacter 2019, 24, e12597. [Google Scholar] [CrossRef]


{kind=link}
| Treatment | Regimen | Duration | Recent First-Line Eradication Rate (ITT) | Recommendations According to Guidelines | Notes |
|---|---|---|---|---|---|
| Standard triple therapy (STT) | PPI standard dose bid Amoxicillin 1 g bid Clarithromycin 500 mg bid | 7–14 d | 63.9% [105], 74.1% [106] | First-line: optionally recommended by KCHUGR and JSHR Rescue: limited recommended by MAA | Over the past 20 years, the efficacy of STT has markedly decreased, and STT is generally not recommended as a first-line regimen |
| Bismuth quadruple therapy (BQT) | PPI standard dose bid Bismuth standard dose qid Metronidazole 500 mg tid Tetracycline 500 mg qid | 7–14 d | 82.8% [107], 88.2% [44], 91.5% [108] | First-line: recommended by ACG, MAA, TOR, and KCHUGR (optionally) Rescue: recommended by ACG, MAA, TOR, and KCHUGR | BQT has been suggested as a first-line treatment option in many guidelines, especially for regions with a high clarithromycin resistance. |
| Concomitant therapy (non-bismuth quadruple therapy) | PPI standard dose bid Clarithromycin 500 mg bid Amoxicillin 1g bid Metronidazole 500 mg bid | 10–14 d | 84.6% [106], 90.1% [109], 93.5% [110] | First-line: recommended by ACG, MAA, and TOR Rescue: recommended by ACG and MAA | The eradication rate is superior to that of CTT, and the method of administration is simple compared to that of sequential therapy. But, adverse events may be more likely with concomitant therapy. |
| Sequential therapy | PPI standard dose bid Amoxicillin 1g bid (first half only) Clarithromycin 500 mg bid (for the second half only) Metronidazole 500 mg bid (for the second half only) | 10–14 d | 69.5% [106], 82.0% [111], 87.0% [112] | First-line: optionally recommended (not ideal) by ACG Rescue: not recommended in all guidelines | As first-line therapy, the role is gradually disappearing. It is a cumbersome way to reduce patient compliance. |
| Hybrid therapy | PPI standard dose bid Amoxicillin 1g bid Clarithromycin 500 mg bid (for the second half only) Metronidazole 500 mg bid (for the second half only) | 14 d | 85.8 % [75], 92.8% [113] | First-line: optionally recommended (not ideal) by ACG Rescue: not recommended in all guidelines | It is a method that combines sequential therapy and concomitant therapy. |
| Levofloxacin-based therapy | Levofloxacin can be given as triple therapy or quadruple therapy. | 10–14 d | 85.5% [76], 94.0% [77] | First-line: recommended by ACG Rescue: recommended by ACG, MAA, and TOR | Most guidelines recommend that levofloxacin-based therapy be applied as rescue therapy rather than first-line. It is less effective for areas with high quinolone resistance. |
| Rifabutin-based therapy | PPI standard dose bid Amoxicillin 1g bid Rifabutin 150 mg bid | 10 d | 83.8% [93] | First-line: not recommended in all guidelines Rescue: optionally recommended (third or fourth-line) by MAA and TOR | All guidelines recommend rifabutin-based therapy as rescue therapy. Rifabutin has the rare risk of myelotoxicity; therefore, careful use is required. |
| Potassium-competitive acid blocker based therapy | P-CAB can be given as triple therapy or quadruple therapy by replacing PPI with P-CAB. | 7–14 d | 89.2% [104], 90.2% [114] | Not stated in algorithm of guidelines | The role of potent acid suppression is expected to increase gradually, and more research is needed. |
| H. pylori treatment based on antibacterial susceptibility test | Tailored therapy according to AST results | 7–14 d | 92.7% [31], 92.9% [115] | MAA recommends to perform AST after the failure of second-line treatment. | The results of tailored therapy based on AST are excellent, and it is expected to play a role in improving H. pylori treatment in the future. Efforts to facilitate the application of AST in clinical practice are required. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Chung, J.-W. Best Helicobacter pylori Eradication Strategy in the Era of Antibiotic Resistance. Antibiotics 2020, 9, 436. https://doi.org/10.3390/antibiotics9080436
Kim SY, Chung J-W. Best Helicobacter pylori Eradication Strategy in the Era of Antibiotic Resistance. Antibiotics. 2020; 9(8):436. https://doi.org/10.3390/antibiotics9080436
Chicago/Turabian StyleKim, Su Young, and Jun-Won Chung. 2020. "Best Helicobacter pylori Eradication Strategy in the Era of Antibiotic Resistance" Antibiotics 9, no. 8: 436. https://doi.org/10.3390/antibiotics9080436
APA StyleKim, S. Y., & Chung, J. -W. (2020). Best Helicobacter pylori Eradication Strategy in the Era of Antibiotic Resistance. Antibiotics, 9(8), 436. https://doi.org/10.3390/antibiotics9080436