Titanium-Nitride Coating Does Not Result in a Better Clinical Outcome Compared to Conventional Cobalt-Chromium Total Knee Arthroplasty after a Long-Term Follow-Up: A Propensity Score Matching Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Outcome Measurements
2.3. Statistical Methods
3. Results
The Overall Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pabinger, C.; Lothaller, H.; Geissler, A. Utilization rates of knee-arthroplasty in OECD countries. Osteoarthr. Cartil. 2015, 23, 1664–1673. [Google Scholar] [CrossRef] [Green Version]
- Turkiewicz, A.; Petersson, I.F.; Bjork, J.; Hawker, G.; Dahlberg, L.E.; Lohmander, L.S.; Englund, M. Current and future impact of osteoarthritis on health care: A population-based study with projections to year 2032. Osteoarthr. Cartil. 2014, 22, 1826–1832. [Google Scholar] [CrossRef] [Green Version]
- Pabinger, C.; Berghold, A.; Boehler, N.; Labek, G. Revision rates after knee replacement. Cumulative results from worldwide clinical studies versus joint registers. Osteoarthr. Cartil. 2013, 21, 263–268. [Google Scholar] [CrossRef] [Green Version]
- Hawker, G.; Wright, J.; Coyte, P.; Paul, J.; Dittus, R.; Croxford, R.; Freund, D. Health-related quality of life after knee replacement. J. Bone Jt. Surg. Am. 1998, 80, 163–173. [Google Scholar] [CrossRef]
- Van Hove, R.P.; Brohet, R.M.; van Royen, B.J.; Nolte, P.A. No clinical benefit of titanium nitride coating in cementless mobile-bearing total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1833–1840. [Google Scholar] [CrossRef]
- Bravo, D.; Wagner, E.R.; Larson, D.R.; Davis, M.P.; Pagnano, M.W.; Sierra, R.J. No Increased Risk of Knee Arthroplasty Failure in Patients with Positive Skin Patch Testing for Metal Hypersensitivity: A Matched Cohort Study. J. Arthroplasty 2016, 31, 1717–1721. [Google Scholar] [CrossRef]
- Sonntag, R.; Reinders, J.; Kretzer, J.P. What’s next? Alternative materials for articulation in total joint replacement. Acta Biomater. 2012, 8, 2434–2441. [Google Scholar] [CrossRef]
- Hooper, G.; Rothwell, A.; Frampton, C. The low contact stress mobile-bearing total knee replacement: A prospective study with a minimum follow-up of ten years. J. Bone Jt. Surg. Br. 2009, 91, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Chiu, V.; Vail, T.P.; Berry, D.J. The epidemiology of revision total knee arthroplasty in the United States. Clin. Orthop. Relat. Res. 2010, 468, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Galvin, A.; Brockett, C.; Williams, S.; Hatto, P.; Burton, A.; Isaac, G.; Fisher, J. Comparison of wear of ultra-high molecular weight polyethylene acetabular cups against surface-engineered femoral heads. Proc. Inst. Mech. Eng. H 2008, 222, 1073–1080. [Google Scholar] [CrossRef]
- Rostlund, T.; Albrektsson, B.; Albrektsson, T.; McKellop, H. Wear of ion-implanted pure titanium against UHMWPE. Biomaterials 1989, 10, 176–181. [Google Scholar] [CrossRef]
- Hallab, N.J.; Vermes, C.; Messina, C.; Roebuck, K.A.; Glant, T.T.; Jacobs, J.J. Concentration- and composition-dependent effects of metal ions on human MG-63 osteoblasts. J. Biomed. Mater. Res. 2002, 60, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Hallab, N.J.; Caicedo, M.; Epstein, R.; McAllister, K.; Jacobs, J.J. In vitro reactivity to implant metals demonstrates a person-dependent association with both T-cell and B-cell activation. J. Biomed. Mater. Res. A 2010, 92, 667–682. [Google Scholar] [PubMed] [Green Version]
- Van Hove, R.P.; Sierevelt, I.N.; van Royen, B.J.; Nolte, P.A. Titanium-Nitride Coating of Orthopaedic Implants: A Review of the Literature. BioMed Res. Int. 2015, 2015, 485975. [Google Scholar] [CrossRef] [Green Version]
- Eliaz, N. Corrosion of Metallic Biomaterials: A Review. Materials 2019, 12, 407. [Google Scholar] [CrossRef] [Green Version]
- Galea, V.P.; Laaksonen, I.; Matuszak, S.J.; Connelly, J.W.; Muratoglu, O.; Malchau, H. Mid-term changes in blood metal ion levels after Articular Surface Replacement arthroplasty of the hip. Bone Jt. J. 2017, 99 (Suppl. SB), 33–40. [Google Scholar] [CrossRef]
- Beraudi, A.; Catalani, S.; Montesi, M.; Stea, S.; Sudanese, A.; Apostoli, P.; Toni, A. Detection of cobalt in synovial fluid from metal-on-metal hip prosthesis: Correlation with the ion haematic level. Biomarkers 2013, 18, 699–705. [Google Scholar] [CrossRef]
- Akbar, M.; Brewer, J.M.; Grant, M.H. Effect of chromium and cobalt ions on primary human lymphocytes in vitro. J. Immunotoxicol. 2011, 8, 140–149. [Google Scholar] [CrossRef]
- Eltit, F.; Assiri, A.; Garbuz, D.; Duncan, C.; Masri, B.; Greidanus, N.; Wang, R. Adverse reactions to metal on polyethylene implants: Highly destructive lesions related to elevated concentration of cobalt and chromium in synovial fluid. J. Biomed. Mater. Res. A 2017, 105, 1876–1886. [Google Scholar] [CrossRef]
- Hallab, N.; Merritt, K.; Jacobs, J.J. Metal sensitivity in patients with orthopaedic implants. J. Bone Jt. Surg. Am. 2001, 83, 428–436. [Google Scholar] [CrossRef]
- Wang, J.Y.; Wicklund, B.H.; Gustilo, R.B.; Tsukayama, D.T. Prosthetic metals interfere with the functions of human osteoblast cells in vitro. Clin. Orthop. Relat. Res. 1997, 339, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Wawrzynski, J.; Gil, J.A.; Goodman, A.D.; Waryasz, G.R. Hypersensitivity to Orthopedic Implants: A Review of the Literature. Rheumatol. Ther. 2017, 4, 45–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermes, C.; Kuzsner, J.; Bardos, T.; Than, P. Prospective analysis of human leukocyte functional tests reveals metal sensitivity in patients with hip implant. J. Orthop. Surg. Res. 2013, 8, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carossino, A.M.; Carulli, C.; Ciuffi, S.; Carossino, R.; Thyrion, G.D.Z.; Zonefrati, R.; Brandi, M.L. Hypersensitivity reactions to metal implants: Laboratory options. BMC Musculoskelet. Disord. 2016, 17, 486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapaj, L.; Rozwalka, J. Retrieval analysis of TiN (titanium nitride) coated knee replacements: Coating wear and degradation in vivo. J. Biomed. Mater. Res. B Appl. Biomater. 2019. [Google Scholar]
- Fabry, C.; Zietz, C.; Baumann, A.; Ehall, R.; Bader, R. High wear resistance of femoral components coated with titanium nitride: A retrieval analysis. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 2630–2639. [Google Scholar] [CrossRef]
- Gobel, F.; Ulbricht, S.; Hein, W.; Bernstein, A. Radiological mid-term results of total knee arthroplasty with femoral components of different materials. Z. Orthop. Unfall. 2008, 146, 194–199. [Google Scholar]
- Ferreira, M.L.; Zhang, Y.; Metcalf, B.; Makovey, J.; Bennell, K.L.; March, L.; Hunter, D.J. The influence of weather on the risk of pain exacerbation in patients with knee osteoarthritis—A case-crossover study. Osteoarthr. Cartil. 2016, 24, 2042–2047. [Google Scholar] [CrossRef]
- Smedslund, G.; Hagen, K.B. Does rain really cause pain? A systematic review of the associations between weather factors and severity of pain in people with rheumatoid arthritis. Eur. J. Pain 2011, 15, 5–10. [Google Scholar] [CrossRef]
- Vielgut, I.; Leitner, L.; Kastner, N.; Radl, R.; Leithner, A.; Sadoghi, P. Sports Activity after Low-contact-stress Total Knee Arthroplasty—A long term follow-up study. Sci. Rep. 2016, 6, 24630. [Google Scholar] [CrossRef] [Green Version]
- Tegner, Y.; Lysholm, J. Rating systems in the evaluation of knee ligament injuries. Clin. Orthop. Relat. Res. 1985, 198, 43–49. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar] [PubMed]
- Insall, J.N.; Dorr, L.D.; Scott, R.D.; Scott, W.N. Rationale of the Knee Society clinical rating system. Clin. Orthop. Relat. Res. 1989, 248, 13–14. [Google Scholar]
- Hoenig, J.M.; Heise, D.M. The Abuse of Power: The Pervasive Fallacy of Power Calculations for Data Analysis. Am. Stat. 2001, 55, 19–24. [Google Scholar] [CrossRef]
- Thienpont, E. Titanium niobium nitride knee implants are not inferior to chrome cobalt components for primary total knee arthroplasty. Arch. Orthop. Trauma Surg. 2015, 135, 1749–1754. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.; Metcalfe, A.; Woodnutt, D. Medium-term outcome of titanium nitride, mobile bearing total knee replacement. Acta Orthop. Belg. 2014, 80, 269–275. [Google Scholar]
- Australian Orthopaedic Association National Joint Replacement Registry (2019). National Joint Replacement Registry. Annual Report 2019. Australian Orthopaedic Association National Joint Replacement Registry. Available online: https://aoanjrr.sahmri.com/annual-reports-2019 (accessed on 15 March 2020).
- National Joint Registry for England and Wales (2018). National Joint Registry. 15th Annual Report 2018. National Joint Registry for England and Wales. Available online: http://www.njrcentre.org.uk (accessed on 15 March 2020).
- Amstutz, H.C.; Campbell, P.; Kossovsky, N.; Clarke, I.C. Mechanism and clinical significance of wear debris-induced osteolysis. Clin. Orthop. Relat. Res. 1992, 276, 7–18. [Google Scholar] [CrossRef]
- Sadoghi, P.; Liebensteiner, M.; Agreiter, M.; Leithner, A.; Bohler, N.; Labek, G. Revision surgery after total joint arthroplasty: A complication-based analysis using worldwide arthroplasty registers. J. Arthroplasty 2013, 28, 1329–1332. [Google Scholar] [CrossRef]
- Beverland, D. Patient satisfaction following TKA: Bless them all! Orthopedics 2010, 33, 657. [Google Scholar] [CrossRef] [Green Version]
- Ghanem, E.; Pawasarat, I.; Lindsay, A.; May, L.; Azzam, K.; Joshi, A.; Parvizi, J. Limitations of the Knee Society Score in evaluating outcomes following revision total knee arthroplasty. J. Bone Jt. Surg. Am. 2010, 92, 2445–2451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liow, R.Y.; Walker, K.; Wajid, M.A.; Bedi, G.; Lennox, C.M. The reliability of the American Knee Society Score. Acta Orthop. Scand. 2000, 71, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Loth, F.L.; Liebensteiner, M.C.; Giesinger, J.M.; Giesinger, K.; Bliem, H.R.; Holzner, B. What makes patients aware of their artificial knee joint? BMC Musculoskelet. Disord. 2018, 19, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmermans, E.J.; van der Pas, S.; Schaap, L.A.; Sanchez-Martinez, M.; Zambon, S.; Peter, R.; Siviero, P. Self-perceived weather sensitivity and joint pain in older people with osteoarthritis in six European countries: Results from the European Project on OSteoArthritis (EPOSA). BMC Musculoskelet. Disord. 2014, 15, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, J.; Aoyama, M.; Yamazaki, M.; Okumura, S.; Takahashi, K.; Funakubo, M.; Mizumura, K. Artificially produced meteorological changes aggravate pain in adjuvant-induced arthritic rats. Neurosci. Lett. 2004, 354, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Sato, J.; Inagaki, H.; Kusui, M.; Yokosuka, M.; Ushida, T. Lowering barometric pressure induces neuronal activation in the superior vestibular nucleus in mice. PLoS ONE 2019, 14, e0211297. [Google Scholar] [CrossRef]
- Behrend, H.; Zdravkovic, V.; Bosch, M.; Hochreiter, B. No difference in joint awareness after TKA: A matched-pair analysis of a classic implant and its evolutional design. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2124–2129. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
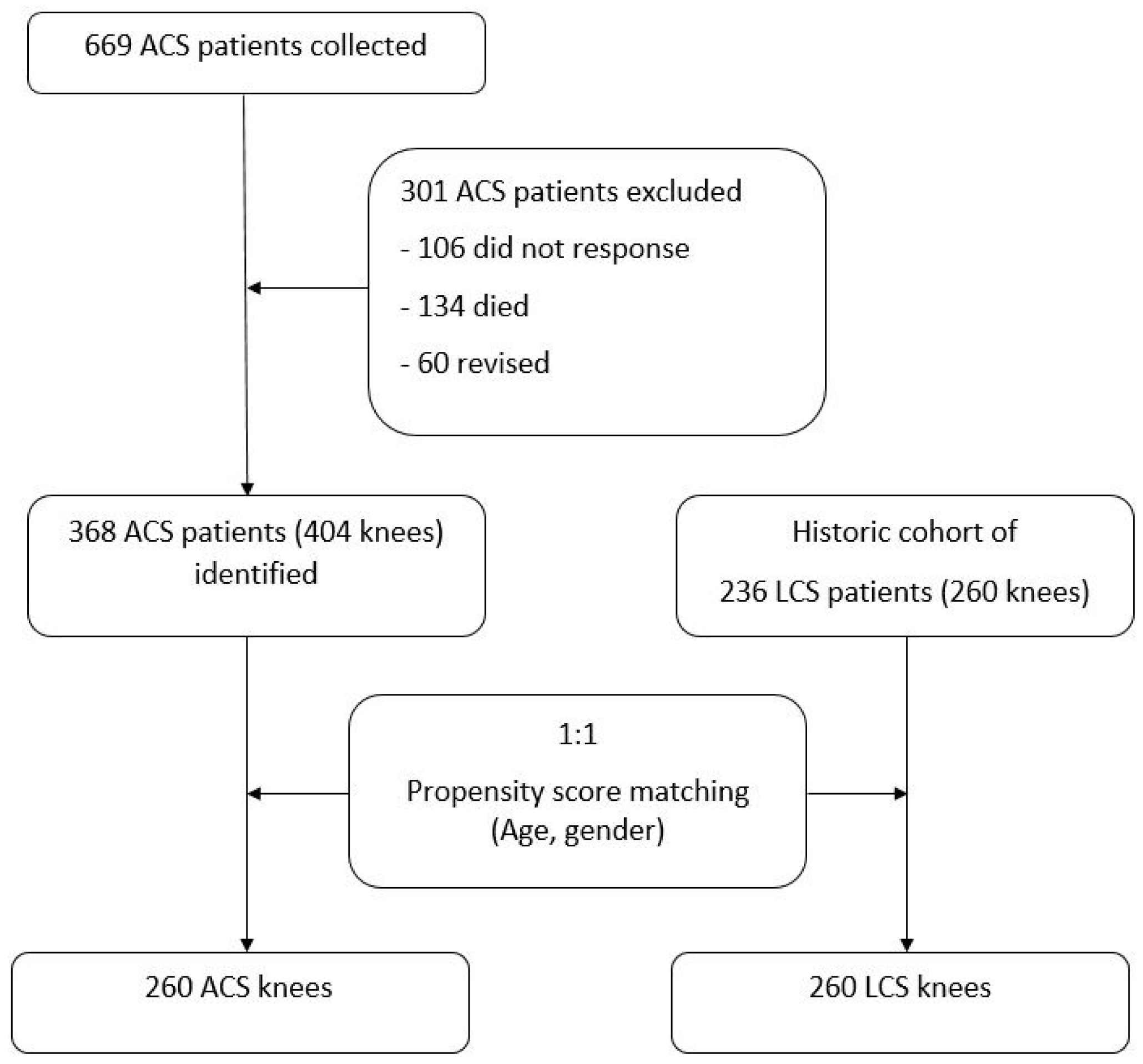
| Patient Characteristics | ACS (n = 404) | LCS (n = 260) | p | Matched ACS (n = 260) | p |
|---|---|---|---|---|---|
| Age, mean ± SD | 65.6 ± 8.2 | 65.8 ± 11.3 | 0.775 | 66.5 ± 9.1 | 0.423 |
| Sex (F:M) | 275:129 | 209:51 | <0.001 | 209:51 | 0.999 |
| – | ACS (n = 260) | LCS (n = 260) | p |
|---|---|---|---|
| KSS Pain (mean ± SD) | 82.6 ± 15.6 | 70.8 ± 21.9 | p < 0.001 |
| KSS Function (mean ± SD) | 61.9 ± 25.4 | 71.1 ± 29.1 | p = 0.011 |
| WOMAC (mean ± SD) | 79.9 ± 15.2 | 81.3 ± 14.6 | p = 0.453 |
| VAS (mean ± SD) Pre-operative Post-operative Change in VAS | |||
| 7.7 ± 1.2 | 6.9 ± 1.8 | p < 0.001 | |
| 2.9 ± 2.0 | 1.4 ± 1.8 | p = 0.002 | |
| 5.6 ± 2.3 | 4.4 ± 3.3 | p < 0.001 | |
| TAS (mean ± SD) Pre-operative Post-operative Change in TAS | |||
| 2.9 ± 1.2 | 3.0 ± 1.5 | p = 0.256 | |
| 2.6 ± 1.1 | 2.2 ± 1.5 | p = 0.001 | |
| 0.3 ± 1.4 | 0.6 ± 1.7 | p = 0.072 | |
| Meteoro-sensitivity (yes) | 150 (58%) | 54 (21%) | p < 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hauer, G.; Leitner, L.; Ackerl, M.C.; Klim, S.; Vielgut, I.; Ehall, R.; Glehr, M.; Leithner, A.; Sadoghi, P. Titanium-Nitride Coating Does Not Result in a Better Clinical Outcome Compared to Conventional Cobalt-Chromium Total Knee Arthroplasty after a Long-Term Follow-Up: A Propensity Score Matching Analysis. Coatings 2020, 10, 442. https://doi.org/10.3390/coatings10050442
Hauer G, Leitner L, Ackerl MC, Klim S, Vielgut I, Ehall R, Glehr M, Leithner A, Sadoghi P. Titanium-Nitride Coating Does Not Result in a Better Clinical Outcome Compared to Conventional Cobalt-Chromium Total Knee Arthroplasty after a Long-Term Follow-Up: A Propensity Score Matching Analysis. Coatings. 2020; 10(5):442. https://doi.org/10.3390/coatings10050442
Chicago/Turabian StyleHauer, Georg, Lukas Leitner, Marc C. Ackerl, Sebastian Klim, Ines Vielgut, Reinhard Ehall, Mathias Glehr, Andreas Leithner, and Patrick Sadoghi. 2020. "Titanium-Nitride Coating Does Not Result in a Better Clinical Outcome Compared to Conventional Cobalt-Chromium Total Knee Arthroplasty after a Long-Term Follow-Up: A Propensity Score Matching Analysis" Coatings 10, no. 5: 442. https://doi.org/10.3390/coatings10050442
APA StyleHauer, G., Leitner, L., Ackerl, M. C., Klim, S., Vielgut, I., Ehall, R., Glehr, M., Leithner, A., & Sadoghi, P. (2020). Titanium-Nitride Coating Does Not Result in a Better Clinical Outcome Compared to Conventional Cobalt-Chromium Total Knee Arthroplasty after a Long-Term Follow-Up: A Propensity Score Matching Analysis. Coatings, 10(5), 442. https://doi.org/10.3390/coatings10050442