The Surface Anodization of Titanium Dental Implants Improves Blood Clot Formation Followed by Osseointegration

 ,
, 
 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
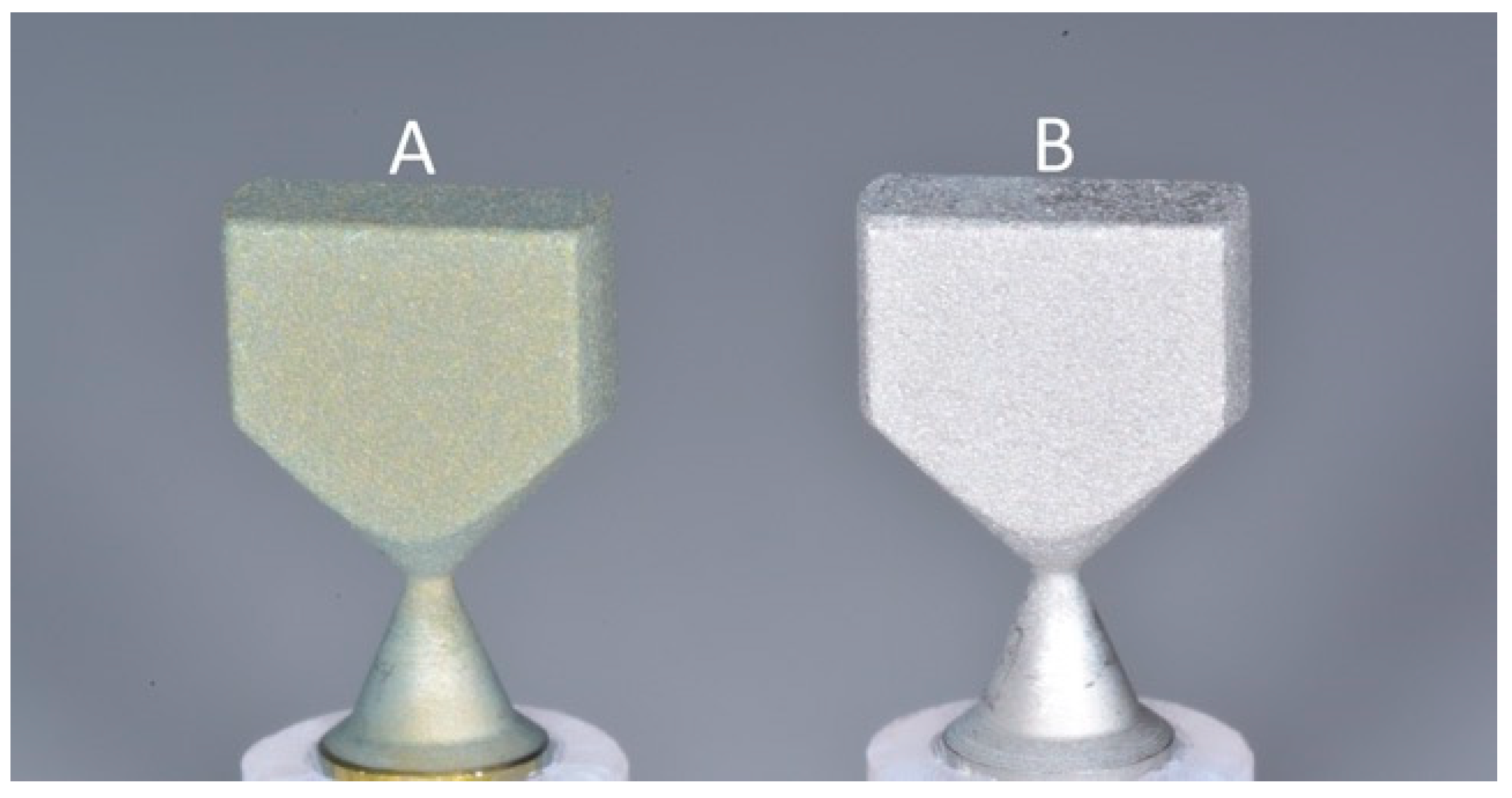
2.1. Specimen Preparation
2.2. Contact Angle (θ) Measurement
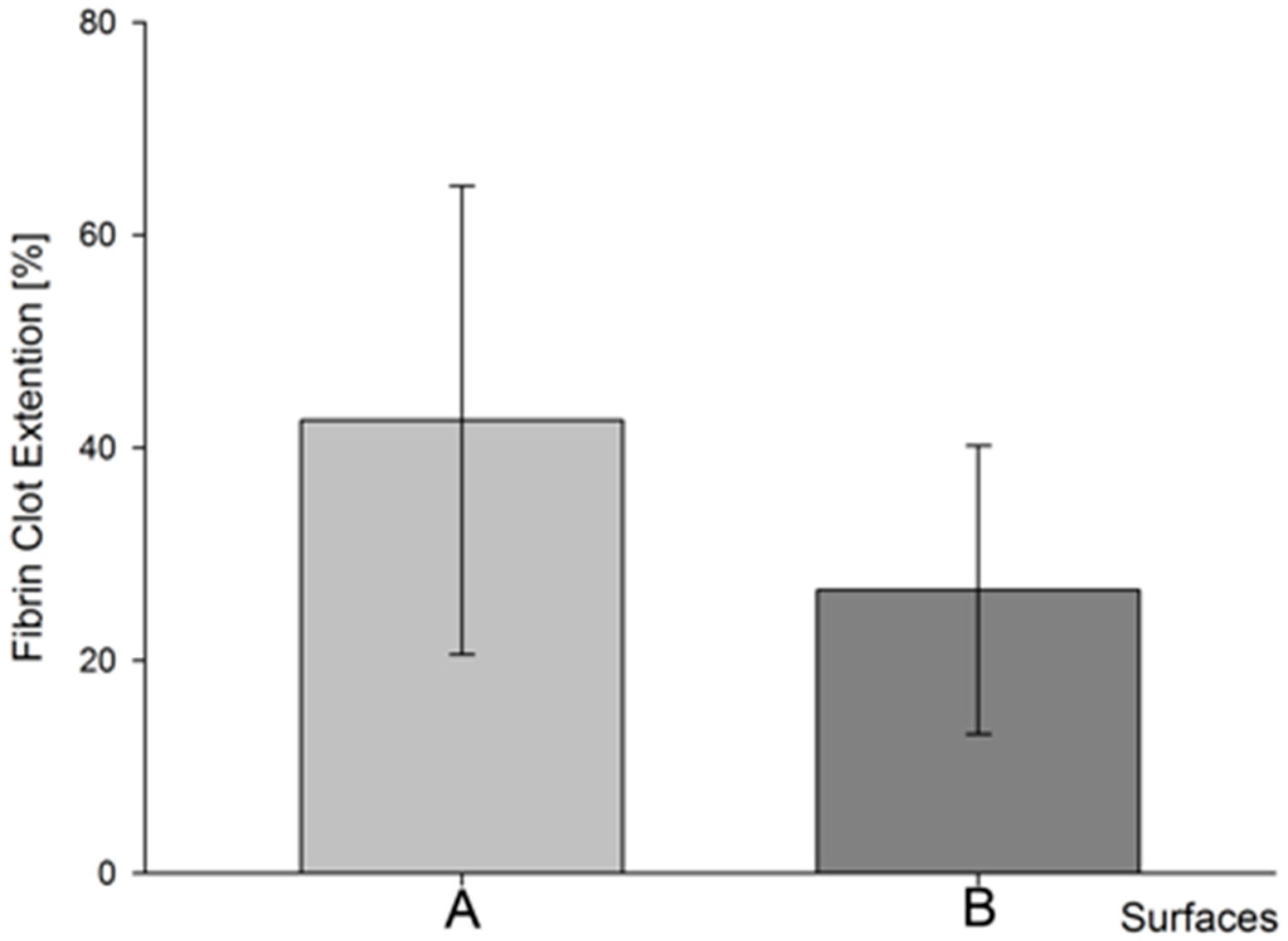
2.3. Blood Clot Extension (bce) Measurament
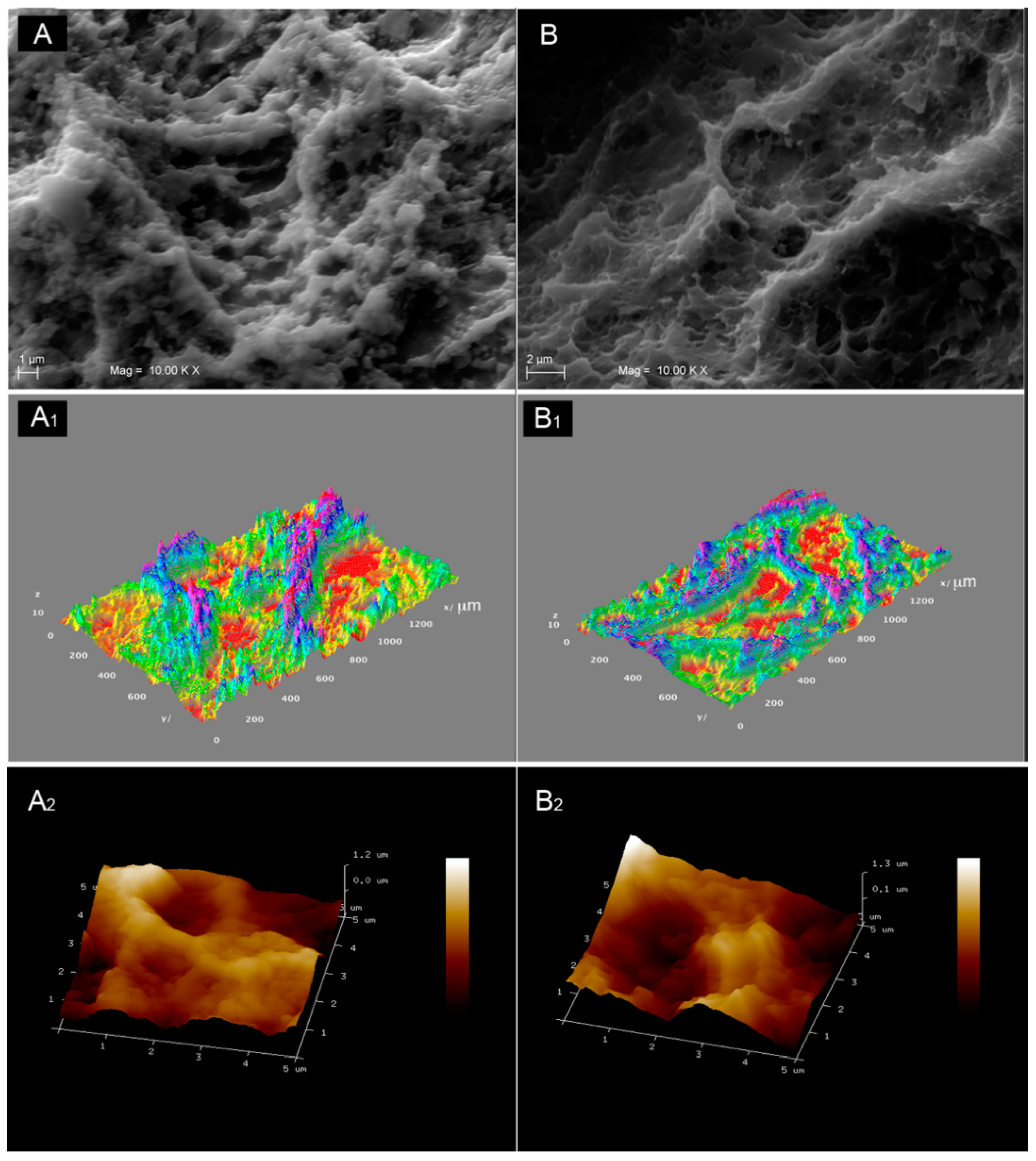
2.4. SEM Observation
2.5. Surface Micro-Roughness (Ra)
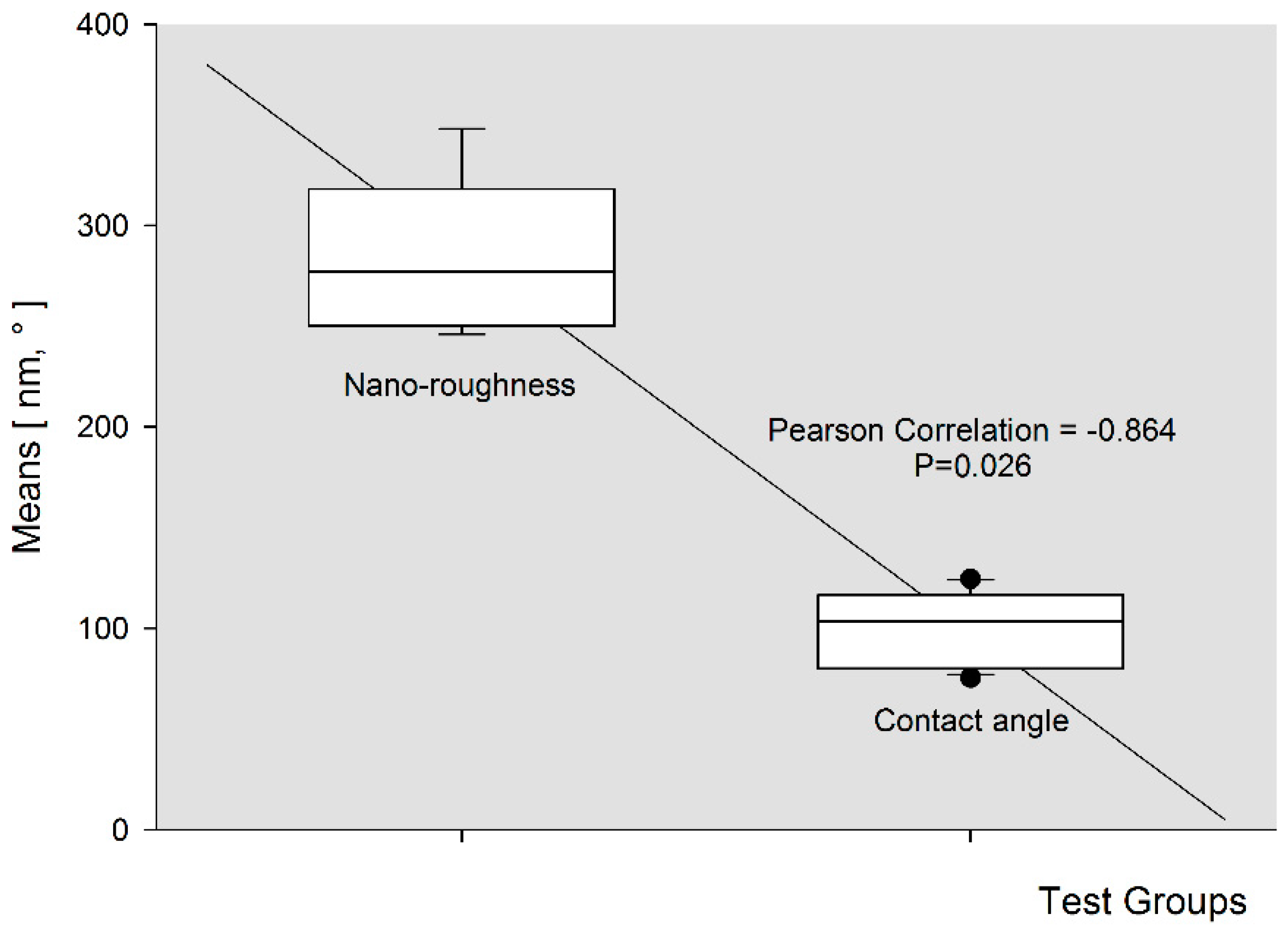
2.6. Surface Nano-Roughness (Ra)
2.7. Implant Retrieval and Evaluation
2.8. Specimen Processing
2.9. Statistics
3. Results
3.1. Contact Angle
3.2. Micro-Roughness
3.3. Nano-Roughness
3.4. Blood Clot Extension
3.5. Bivariate Pearson Correlation
3.6. Histomorphometric Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Davies, J.E. Mechanisms of endosseous integration. Int. J. Prosthodont. 1998, 11, 391–401. [Google Scholar] [PubMed]
- Anderson, J.M. Biological Responses to Materials. Annu. Rev. Mater. Res. 2001, 31, 81–110. [Google Scholar] [CrossRef]
- Arvidsson, S.; Askendal, A.; Tengvall, P. Blood plasma contact activation on silicon, titanium and aluminium. Biomaterials 2007, 28, 1346–1354. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Branemark, P.I.; Hansson, H.A.; Lindstrom, J. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Magnani, A.; Priamo, A.; Pasqui, D.; Barbucci, R. Cell behaviour on chemically microstructured surfaces. Mater. Sci. Eng. C 2003, 23, 315–328. [Google Scholar] [CrossRef]
- Riehle, M.O.; Dalby, M.J.; Johnstone, H.; MacIntosh, A.; Affrossman, S. Cell behaviour of rat calvaria bone cells on surfaces with random nanometric features. Mater. Sci. Eng. C 2003, 23, 337–340. [Google Scholar] [CrossRef]
- Karacs, A.; Joob Fancsaly, A.; Divinyi, T.; Pető, G.; Kovách, G. Morphological and animal study of titanium dental implant surface induced by blasting and high intensity pulsed Nd-glass laser. Mater. Sci. Eng. C 2003, 23, 431–435. [Google Scholar] [CrossRef]
- Lange, R.; Lüthen, F.; Beck, U.; Rychly, J.; Baumann, A.; Nebe, B. Cell-extracellular matrix interaction and physico-chemical characteristics of titanium surfaces depend on the roughness of the material. Biomol. Eng. 2002, 19, 255–261. [Google Scholar] [CrossRef]
- Keselowsky, B.G.; Collard, D.M.; García, A.J. Surface chemistry modulates focal adhesion composition and signaling through changes in integrin binding. Biomaterials 2004, 25, 5947–5954. [Google Scholar] [CrossRef] [PubMed]
- Gorbet, M.B.; Sefton, M.V. Biomaterial-associated thrombosis: Roles of coagulation factors, complement, platelets and leukocytes. Biomaterials 2004, 25, 5681–5703. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.R.; Rinder, H.M.; Rinder, C.S. Interaction of blood and artificial surfaces. In Thrombosis and Hemorrhage, 3rd ed.; Loscalzo, J., Schafer, A.I., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2003; pp. 865–900. [Google Scholar]
- Nygren, H.; Tengvall, P.; Lundstrom, I. The initial reactions of TiO2 with blood. J. Biomed. Mater. Res. 1997, 34, 487–492. [Google Scholar] [CrossRef]
- Horbett, T.A. Chapter 13 Principles underlying the role of adsorbed plasma proteins in blood interactions with foreign materials. Cardiovasc. Pathol. 1993, 2, 137–148. [Google Scholar] [CrossRef]
- Vroman, L. Problems in the development of materials that are compatible with blood. Biomater. Med. Devices Artif. Organs 1984, 12, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Eaton, J.W. Fibrin(ogen) mediates acute inflammatory responses to biomaterials. J. Exp. Med. 1993, 178, 2147–2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bangham, A.D. A Correlation between Surface Charge and Coagulant Action of Phospholipids. Nature 1961, 192, 1197–1198. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.M.; Nemerson, Y. Blood coagulation. Annu. Rev. Biochem. 1980, 49, 765–811. [Google Scholar] [CrossRef] [PubMed]
- Drummond, R.K.; Peppas, N.A. Fibrinolytic behaviour of streptokinaseimmobilized poly(methacrylic acid-g-ethylene oxide). Biomaterials 1991, 12, 356–360. [Google Scholar] [CrossRef]
- Siemssen, P.A.; Garred, P.; Olsen, J.; Aasen, A.O.; Mollnes, T.E. Activation of Complement Kallikrein-kinin, Fibrinolysis and Coagulation Systems by Urinary Catheters. Effect of Time and Temperature in Biocompatibility Studies. Br. J. Urol. 1991, 67, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J. Complement activation during extracorporeal therapy: Biochemistry, cell biology and clinical relevance. Nephrol. Dial. Transplant. 1994, 9, 36–45. [Google Scholar] [PubMed]
- Mosesson, M.W. Fibrinogen functions and fibrin assembly. Fibrinolysis Proteolysis 2000, 14, 182–186. [Google Scholar] [CrossRef]
- Kawase, T.; Okuda, K.; Wolff, L.F.; Yoshie, H. Platelet-rich plasma-derived fibrin clot formation stimulates collagen synthesis in periodontal ligament and osteoblastic cells in vitro. J. Periodontol. 2003, 74, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Schmoekel, H.; Schense, J.C.; Weber, F.E.; Grätz, K.W.; Gnägi, D.; Müller, R.; Hubbell, J.A. Bone healing in the rat and dog with nonglycosylated BMP-2 demonstrating low solubility in fibrin matrices. J. Orthop. Res. 2004, 22, 376–381. [Google Scholar] [CrossRef]
- Yucel, E.A.; Oral, O.; Olgac, V.; Oral, C.K. Effects of fibrin glue on wound healing in oral cavity. J. Dent. 2003, 31, 569–575. [Google Scholar] [CrossRef]
- Chen, J.Y.; Leng, Y.X.; Tian, X.B.; Wang, L.P.; Huang, N.; Chua, P.K.; Yang, P. Antithrombogenic investigation of surface energy and optical bandgap and hemocompatibility mechanism of Ti(Ta+5)O2 thin films. Biomaterials 2002, 23, 2545–2552. [Google Scholar] [CrossRef]
- Park, J.Y.; Gemmell, C.H.; Davies, J.E. Platelet interactions with titanium: Modulation of platelet activity by surface topography. Biomaterials 2001, 22, 2671–2682. [Google Scholar] [CrossRef]
- Di Iorio, D.; Traini, T.; Degidi, M.; Caputi, S.; Neugebauer, J.; Piattelli, A. Quantitative evaluation of the fibrin clot extension on different implant surfaces: An in vitro study. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 74, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Koak, J.Y.; Chang, I.T.; Wennerberg, A.; Heo, S.J. A histomorphometric analysis of the effects of various surface treatment methods on osseointegration. Int. J. Oral Maxillofac. Implant. 2003, 18, 349–356. [Google Scholar]
- Buser, D.; Schenk, R.K.; Steinemann, S.; Fiorellini, J.P.; Fox, C.H.; Stich, H. Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J. Biomed. Mater. Res. 1991, 25, 889–902. [Google Scholar] [CrossRef] [PubMed]
- Larsson, C.; Thomsen, P.; Lausmaa, J.; Rodahl, M.; Kasemo, B.; Ericson, L.E. Bone response to surface modified titanium implants: Studies on electropolished implants with different oxide thicknesses and morphology. Biomaterials 1994, 15, 1062–1074. [Google Scholar] [CrossRef]
- Albrektsson, T.; Johansson, C.; Lundgren, A.; Sul, Y.; Gottlow, J. Experimental studies on oxidized implants. A histomorphometrical and biomechanical analysis. Appl. Osseointegr. Res. 2000, 1, 21–24. [Google Scholar]
- Nishiguchi, S.; Kato, H.; Fujita, H.; Kim, H.M.; Miyaji, F.; Kokubo, T.; Nakamura, T. Enhancement of bone-bonding strengths of titanium alloy implants by alkali and heat treatments. J. Biomed. Mater. Res. Part A 1999, 48, 689–696. [Google Scholar] [CrossRef]
- Larsson, C.; Thomsen, P.; Aronsson, B.-O.; Rodahl, M.; Lausmaa, J.; Kasemo, B.; Ericson, L.E. Bone response to surface-modified titanium implants: Studies on the early tissue response to machined and electropolished implants with different oxide thicknesses. Biomaterials 1996, 17, 605–616. [Google Scholar] [CrossRef]
- Hazan, R.; Brener, R.; Oron, U. Bone growth to metal implants is regulated by their surface chemical properties. Biomaterials 1993, 14, 570–574. [Google Scholar] [CrossRef]
- Fini, M.; Cigada, A.; Rondelli, G.; Chiesa, R.; Giardino, R.; Giavaresi, G.; Nicoli Aldini, N.; Torricelli, P.; Vicentini, B. In vitro and in vivo behaviour of Ca-and P-enriched anodized titanium. Biomaterials 1999, 20, 1587–1594. [Google Scholar] [CrossRef]
- Sul, Y.-T.; Johansson, C.B.; Röser, K.; Albrektsson, T. Qualitative and quantitative observations of bone tissue reactions to anodised implants. Biomaterials 2002, 23, 1809–1817. [Google Scholar] [CrossRef]
- Durual, S.; Pernet, F.; Rieder, P.; Mekki, M.; Cattani-Lorente, M.; Wiskott, H.W. Titanium nitride oxide coating on rough titanium stimulates the proliferation of human primary osteoblasts. Clin. Oral Implant. Res. 2011, 22, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Massa, M.A.; Covarrubias, C.; Bittner, M.; Fuentevilla, I.A.; Capetillo, P.; Von Marttens, A.; Carvajal, J.C. Synthesis of new antibacterial composite coating for titanium based on highly ordered nanoporous silica and silver nanoparticles. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 45, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Souza, F.A.; Queiroz, T.P.; Sonoda, C.K.; Okamoto, R.; Margonar, R.; Guastaldi, A.C.; Nishioka, R.S.; Garcia Júnior, I.R. Histometric analysis and topographic characterization of cp Ti implants with surfaces modified by laser with and without silica deposition. J. Biomed. Mater. Res. B Appl. Biomater. 2014, 102, 1677–1688. [Google Scholar] [CrossRef] [PubMed]
- Mazzola, L.; Bemporad, E.; Misiano, C.; Pepe, F.; Santini, P.; Scandurra, R. Surface analysis and osteoblasts response of a titanium oxi-carbide film deposited on titanium by ion plating plasma assisted (IPPA). J. Nanosci. Nanotechnol. 2011, 11, 8754–8762. [Google Scholar] [CrossRef] [PubMed]
- Maho, A.; Linden, S.; Arnould, C.; Detriche, S.; Delhalle, J.; Mekhalif, Z. Tantalum oxide/carbon nanotubes composite coatings on titanium, and their functionalization with organophosphonic molecular films: A high quality scaffold for hydroxyapatite growth. J. Colloid Interface Sci. 2012, 371, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Eibl, O.; Scheideler, L.; Geis-Gerstorfer, J. Characterization of nano hydroxyapatite/collagen surfaces and cellular behaviors. J. Biomed. Mater. Res. A 2006, 79, 114–127. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, Y. Anodic Oxide Films; Academic Press: London, UK, 1961. [Google Scholar]
- Kim, K.; Lee, B.-A.; Piao, X.-H.; Chung, H.-J.; Kim, Y.-J. Surface characteristics and bioactivity of an anodized titanium surface. J. Periodontal Implant Sci. 2013, 43, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.-J.; Lee, J.-H.; Jeong, Y.; Kim, Y.-J.; Chi, C.-S. Microstructural characterization of biomedical titanium oxide film fabricated by electrochemical method. Surf. Coat. Technol. 2005, 198, 247–252. [Google Scholar] [CrossRef]
- Yao, C.; Webster, T.J. Anodization: A promising nano-modification technique of titanium implants for orthopedic applications. J. Nanosci. Nanotechnol. 2006, 6, 2682–2692. [Google Scholar] [CrossRef] [PubMed]
- Balasundaram, G.; Yao, C.; Webster, T.J. TiO2 nanotubes functionalized with regions of bone morphogenetic protein-2 increases osteoblast adhesion. J. Biomed. Mater. Res. A 2008, 84, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Ueno, T.; Minamikawa, H.; Ikeda, T.; Nakagawa, K.; Ogawa, T. Early-stage osseointegration capability of a submicrofeatured titanium surface created by microroughening and anodic oxidation. Clin. Oral Implant. Res. 2013, 24, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- El-Wassefy, N.A.; Hammouda, I.M.; Habib, A.N.; El-Awady, G.Y.; Marzook, H.A. Assessment of anodized titanium implants bioactivity. Clin. Oral Implant. Res. 2014, 25, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Le Guehennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, R.N. Resistance of solid surfaces to wetting by water. Ind. Eng. Chem. 1936, 28, 988–994. [Google Scholar] [CrossRef]
- Herminghaus, S. Roughness-induced non-wetting. EPL 2000, 52, 165. [Google Scholar] [CrossRef]
- Marmur, A. From hygrophilic to superhygrophobic: Theoretical conditions for making high-contact-angle surfaces from low-contact-angle materials. Langmuir 2008, 24, 7573–7579. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Wieland, M.; Schwartz, Z.; Zhao, G.; Rupp, F.; Geis-Gerstorfer, J.; Schedle, A.; Broggini, N.; Bornstein, M.M.; Buser, D.; et al. Potential of chemically modified hydrophilic surface characteristics to support tissue integration of titanium dental implants. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 88, 544–557. [Google Scholar] [CrossRef] [PubMed]
- Wennerberg, A.; Galli, S.; Albrektsson, T. Current knowledge about the hydrophilic and nanostructured SLActive surface. Clin. Cosmet. Investig. Dent. 2011, 3, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Sista, S.; Nouri, A.; Li, Y.; Wen, C.; Hodgson, P.D.; Pande, G. Cell biological responses of osteoblasts on anodized nanotubular surface of a titanium-zirconium alloy. J. Biomed. Mater. Res. A 2013, 101, 3416–3430. [Google Scholar] [CrossRef] [PubMed]









© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Traini, T.; Murmura, G.; Sinjari, B.; Perfetti, G.; Scarano, A.; D’Arcangelo, C.; Caputi, S. The Surface Anodization of Titanium Dental Implants Improves Blood Clot Formation Followed by Osseointegration. Coatings 2018, 8, 252. https://doi.org/10.3390/coatings8070252
Traini T, Murmura G, Sinjari B, Perfetti G, Scarano A, D’Arcangelo C, Caputi S. The Surface Anodization of Titanium Dental Implants Improves Blood Clot Formation Followed by Osseointegration. Coatings. 2018; 8(7):252. https://doi.org/10.3390/coatings8070252
Chicago/Turabian StyleTraini, Tonino, Giovanna Murmura, Bruna Sinjari, Giorgio Perfetti, Antonio Scarano, Camillo D’Arcangelo, and Sergio Caputi. 2018. "The Surface Anodization of Titanium Dental Implants Improves Blood Clot Formation Followed by Osseointegration" Coatings 8, no. 7: 252. https://doi.org/10.3390/coatings8070252
APA StyleTraini, T., Murmura, G., Sinjari, B., Perfetti, G., Scarano, A., D’Arcangelo, C., & Caputi, S. (2018). The Surface Anodization of Titanium Dental Implants Improves Blood Clot Formation Followed by Osseointegration. Coatings, 8(7), 252. https://doi.org/10.3390/coatings8070252