
Bright Light Therapy for Parkinson Disease: A Literature Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:Simple Summary
Abstract
1. Introduction
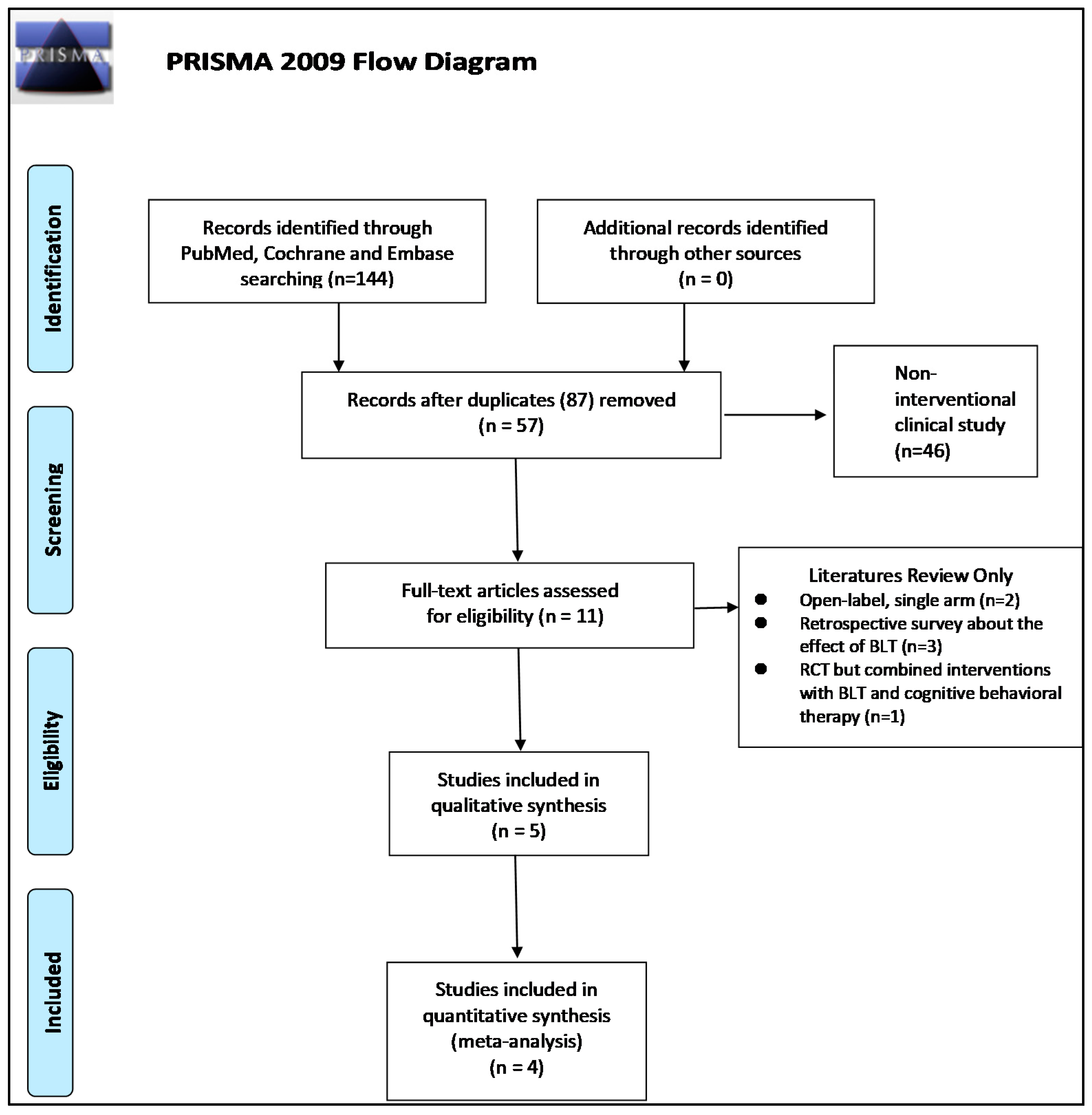
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Literature Search Strategy
2.3. Data Extraction
2.4. Outcomes
2.5. Appraisal of Methodological Quality
2.6. Statistical Analysis
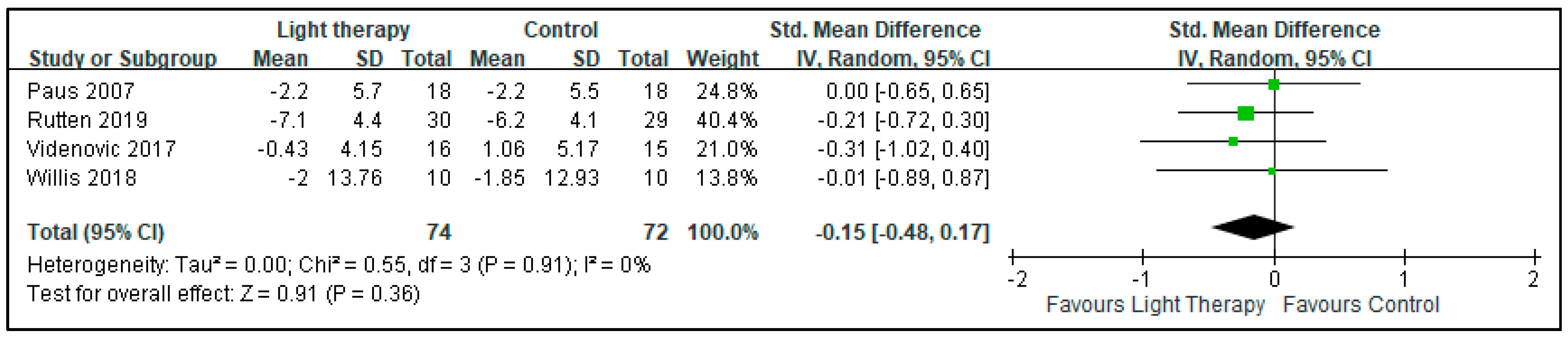
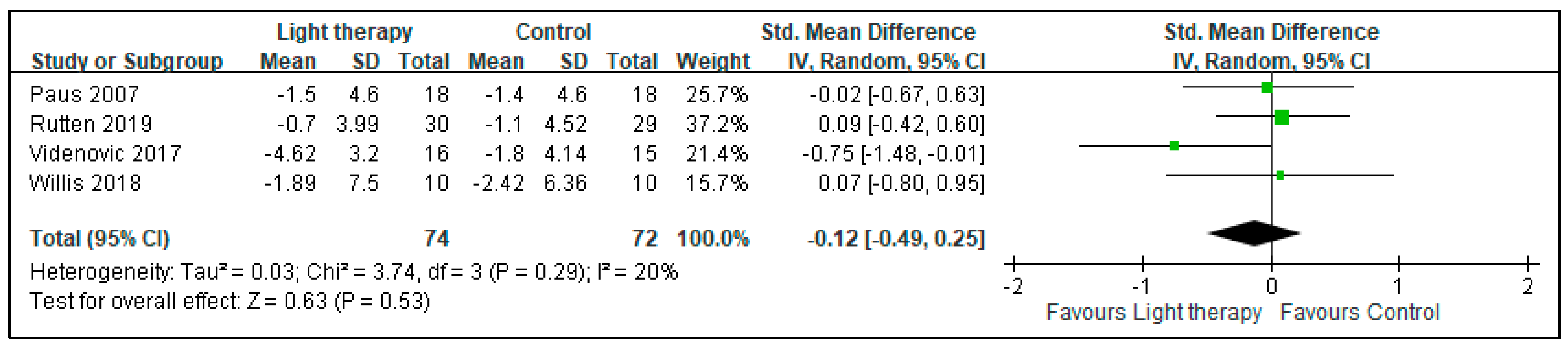
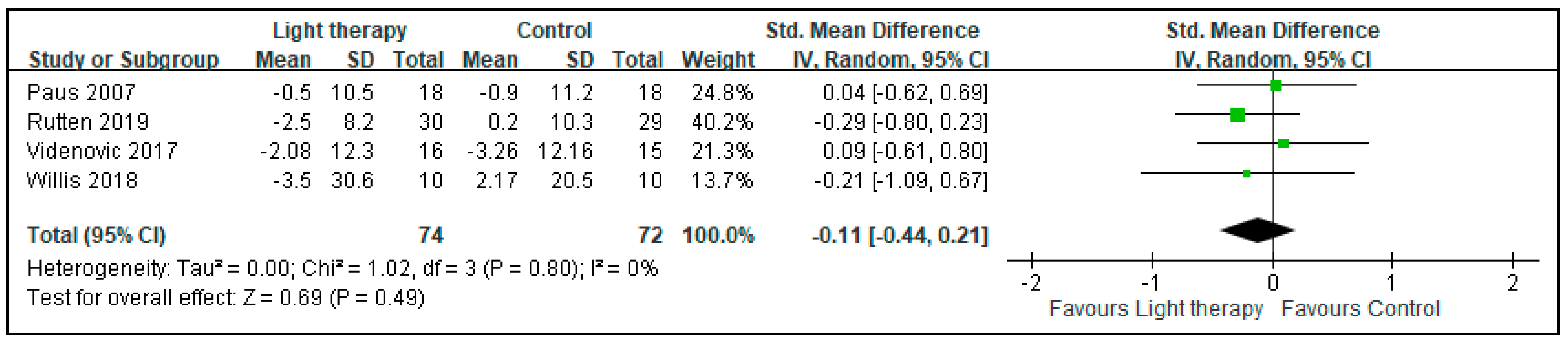
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kalia, L.V.; Lang, A.E. Parkinson’s disease. Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.-E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 3, 17013. [Google Scholar] [CrossRef] [PubMed]
- Aarsland, D.; Marsh, L.; Schrag, A. Neuropsychiatric symptoms in Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2009, 24, 2175–2186. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Nabi, G.; Yao, L.; Siddique, R.; Sajjad, W.; Kumar, S.; Duan, P.; Hou, H. Health risks associated with genetic alterations in internal clock system by external factors. Int. J. Biol. Sci. 2018, 14, 791–798. [Google Scholar] [CrossRef] [Green Version]
- Pail, G.; Huf, W.; Pjrek, E.; Winkler, D.; Willeit, M.; Praschak-Rieder, N.; Kasper, S. Bright-light therapy in the treatment of mood disorders. Neuropsychobiology 2011, 64, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Blume, C.; Garbazza, C.; Spitschan, M. Effects of light on human circadian rhythms, sleep and mood. Somnologie 2019, 23, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cajochen, C.; Kräuchi, K.; Wirz-Justice, A. Role of melatonin in the regulation of human circadian rhythms and sleep. J. Neuroendocrinol. 2003, 15, 432–437. [Google Scholar] [CrossRef] [Green Version]
- Figueiro, M.G. Light, sleep and circadian rhythms in older adults with Alzheimer’s disease and related dementias. Neurodegener. Dis. Manag. 2017, 7, 119–145. [Google Scholar] [CrossRef] [Green Version]
- Faulkner, S.M.; Bee, P.E.; Meyer, N.; Dijk, D.-J.; Drake, R.J. Light therapies to improve sleep in intrinsic circadian rhythm sleep disorders and neuro-psychiatric illness: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 46, 108–123. [Google Scholar] [CrossRef]
- Maruani, J.; Geoffroy, P.A. Bright Light as a Personalized Precision Treatment of Mood Disorders. Front. Psychiatry 2019, 10, 85. [Google Scholar] [CrossRef]
- Stephenson, K.M.; Schroder, C.M.; Bertschy, G.; Bourgin, P. Complex interaction of circadian and non-circadian effects of light on mood: Shedding new light on an old story. Sleep Med. Rev. 2012, 16, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Tyrer, A.E.; Levitan, R.D.; Houle, S.; Wilson, A.A.; Nobrega, J.N.; Meyer, J.H. Increased Seasonal Variation in Serotonin Transporter Binding in Seasonal Affective Disorder. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2016, 41, 2447–2454. [Google Scholar] [CrossRef] [Green Version]
- Paus, S.; Schmitz-Hübsch, T.; Wüllner, U.; Vogel, A.; Klockgether, T.; Abele, M. Bright light therapy in Parkinson’s disease: A pilot study. Mov. Disord. 2007, 22, 1495–1498. [Google Scholar] [CrossRef] [PubMed]
- Rutten, S.; Vriend, C.; Smit, J.H.; Berendse, H.W.; Van Someren, E.J.W.; Hoogendoorn, A.W.; Twisk, J.W.R.; Van Der Werf, Y.D.; Van Den Heuvel, O.A. Bright light therapy for depression in Parkinson disease: A randomized controlled trial. Neurology 2019, 92, E1145–E1156. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raymackers, J.M.; Andrade, M.; Baey, E.; Vanneste, M.; Evrard, F. Bright light therapy with a head-mounted device for anxiety, depression, sleepiness and fatigue in patients with Parkinson’s disease. Acta Neurol. Belg. 2019, 119, 607–613. [Google Scholar] [CrossRef]
- Rios Romenets, S.; Creti, L.; Fichten, C.; Bailes, S.; Libman, E.; Pelletier, A.; Postuma, R.B. Doxepin and cognitive behavioural therapy for insomnia in patients with Parkinson’s disease—A randomized study. Parkinsonism Relat. Disord. 2013, 19, 670–675. [Google Scholar] [CrossRef]
- Rutten, S.; Vriend, C.; Smit, J.H.; Berendse, H.W.; Hoogendoorn, A.W.; van den Heuvel, O.A.; van der Werf, Y.D. A double-blind randomized controlled trial to assess the effect of bright light therapy on depression in patients with Parkinson’s disease. BMC Psychiatry 2016, 16, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Videnovic, A.; Klerman, E.B.; Wang, W.; Marconi, A.; Kuhta, T.; Zee, P.C. Timed light therapy for sleep and daytime sleepiness associated with Parkinson disease a randomized clinical trial. JAMA Neurol. 2017, 74, 411–418. [Google Scholar] [CrossRef]
- Willis, G.L.; Boda, J.; Freelance, C.B. Polychromatic light exposure as a therapeutic in the treatment and management of Parkinson’s disease: A controlled exploratory trial. Front. Neurol. 2018, 9, 741. [Google Scholar] [CrossRef]
- Willis, G.L.; Turner, E.J. Primary and secondary features of Parkinson’s disease improve with strategic exposure to bright light: A case series study. Chronobiol. Int. 2007, 24, 521–537. [Google Scholar] [CrossRef]
- Martino, J.K.; Freelance, C.B.; Willis, G.L. The effect of light exposure on insomnia and nocturnal movement in Parkinson’s disease: An open-label, retrospective, longitudinal study. Sleep Med. 2018, 44, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Smilowska, K.; van Wamelen, D.J.; Schoutens, A.M.C.; Meinders, M.J.; Bloem, B.R. Blue Light Therapy Glasses in Parkinson’s Disease: Patients’ Experience. Parkinson’s Dis. 2019, 2019, 1906271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endo, T.; Matsumura, R.; Tokuda, I.T.; Yoshikawa, T.; Shigeyoshi, Y.; Node, K.; Sakoda, S.; Akashi, M. Bright light improves sleep in patients with Parkinson’s disease: Possible role of circadian restoration. Sci. Rep. 2020, 10, 7982. [Google Scholar] [CrossRef] [PubMed]
- Willis, G.L.; Moore, C.; Armstrong, S.M. A historical justification for and retrospective analysis of the systematic application of light therapy in Parkinson’s disease. Rev. Neurosci. 2012, 23, 199–226. [Google Scholar] [CrossRef] [PubMed]
- Golden, R.N.; Gaynes, B.N.; Ekstrom, R.D.; Hamer, R.M.; Jacobsen, F.M.; Suppes, T.; Wisner, K.L.; Nemeroff, C.B. The efficacy of light therapy in the treatment of mood disorders: A review and meta-analysis of the evidence. Am. J. Psychiatry 2005, 162, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Streeter, C.C.; Gerbarg, P.L.; Saper, R.B.; Ciraulo, D.A.; Brown, R.P. Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Med. Hypotheses 2012, 78, 571–579. [Google Scholar] [CrossRef]
- Koorengevel, K.M.; Gordijn, M.C.; Beersma, D.G.; Meesters, Y.; den Boer, J.A.; van den Hoofdakker, R.H.; Daan, S. Extraocular light therapy in winter depression: A double-blind placebo-controlled study. Biol. Psychiatry 2001, 50, 691–698. [Google Scholar] [CrossRef] [Green Version]
- Van Maanen, A.; Meijer, A.M.; van der Heijden, K.B.; Oort, F.J. The effects of light therapy on sleep problems: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 29, 52–62. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Inclusion Criteria | No. of Patients (Male, %) | Age, Mean (SD or Range) | Intervention | Main Findings | Reason for Not Including into Meta-Analysis |
|---|---|---|---|---|---|---|
| Willis and Turner (2007) | PD with depression or insomnia | 12 (67) | 66 (46~83) | BLT 1000–1500 lux, 1–1.5 h | Improvement in motor, mood, and sleep | Open-label, single-arm |
| Willis et al. (2012) | PD | 129 (unknown) | 66 (12) | BLT 4000–6000 lux, 1–1.5 h | Improvement in motor, mood, and sleep | Retrospective, open-label study |
| Rios Romenets et al. (2013) | PD with insomnia | BLT + CBT: 6 (100) Placebo: 6 (86) | BLT + CBT: 64.5 (16.3) Placebo: 69.5 (10.5) | BLT 10000 lux, 30 min + weekly CBT | Improvement in sleep and quality of life | Can not clarify the effect of BLT alone |
| Martino et al. (2018) | PD | 140 (65) | 66 (10) | BLT 3000–4000 lux, 1–4 h | Improvement in insomnia and RBD | Retrospective, open-label study |
| Smilowska et al. (2019) | PD | 31 (unknown) | unknown | Blue light glasses, 40 lux, usually 30–60 min, twice a day | Improvement in motor, mood, and sleep | Retrospective survey |
| Endo et al. (2020) | PD | 16 (38) | 65.4(7.1) | BLT, 5000 lux, 2 h, three months | Improvement in sleep | Open-label, single-arm |
| Author (Year) | Inclusion Criteria | No. of Patients (Male, %) | Age, Mean (SD or Range) | Baseline H and Y Stage | Intervention | Outcome |
|---|---|---|---|---|---|---|
| Paus et al. (2007) | Stage I to IV MMSE ≥ 24 | E: 18 (67) C: 18 (61) | E: 63.6 (9.8) C: 63.4 (9.7) | E: 2.7 ± 0.6 C: 2.5 ± 0.4 | BLT 7500 lux for 30 min daily for 14 days | BDI, ESS, UPDRS |
| Videnovic et al. (2017) | Stages I to IV ESS: ≥12 | E: 16 (50) C: 15 (33) | E: 62.3 (10.8) C: 64.0 (8.9) | E: 2.1 ± 0.3 C: 2.3 ± 0.5 | BLT 10,000 lux for 1 h twice/day for 14 days | BDI, ESS, UPDRS |
| Willis (2018) | PD | E: 10 (60) C: 10 (50) | E: 66.9 (54–75) C: 66.3 (53–79) | unknown | Polychromatic light, 3000 lux, 1 h for 2 week | BDI, ESS, UPDRS |
| Rutten et al. (2019) | PD with MDD | E: 35 (57) C: 37 (53) | E: 58.9 (8.5) C: 65.8 (8.6) | E: 2.1 ± 0.6 C: 2.4 ± 0.7 | BLT 10,000 lux for 30 min twice/day for 90 days | BDI, ESS, UPDRS, SCOPA-SLEEP |
| Raymackers et al. (2019) | PD | Cross-over design E-C: 8 (50) C-E:8 (75) | E-C: 66.50 (6.30) C-E: 68.88 (5.89) | unknown | Blue enriched light, average 472.7 lux, 45 min for one month | HADS, ESS |
| Allocation Bias | Performance Bias | Attrition Bias | Measurement Bias | Reporting Bias | |
|---|---|---|---|---|---|
| Paus 2007 | Low risk | Low risk | Low risk | Low risk | Low risk |
| Videnovic 2017 | Some concern | Some concern | Low risk | Low risk | Low risk |
| Willis 2018 | Low risk | Low risk | Low risk | Low risk | Low risk |
| Raymackers 2019 | Low risk | Low risk | Low risk | Low risk | Low risk |
| Rutten 2019 | Low risk | Low risk | Some concern | Low risk | Low risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, H.-T.; Huang, T.-W.; Hong, C.-T. Bright Light Therapy for Parkinson Disease: A Literature Review and Meta-Analysis of Randomized Controlled Trials. Biology 2021, 10, 1205. https://doi.org/10.3390/biology10111205
Huang H-T, Huang T-W, Hong C-T. Bright Light Therapy for Parkinson Disease: A Literature Review and Meta-Analysis of Randomized Controlled Trials. Biology. 2021; 10(11):1205. https://doi.org/10.3390/biology10111205
Chicago/Turabian StyleHuang, Hsu-Tung, Tsai-Wei Huang, and Chien-Tai Hong. 2021. "Bright Light Therapy for Parkinson Disease: A Literature Review and Meta-Analysis of Randomized Controlled Trials" Biology 10, no. 11: 1205. https://doi.org/10.3390/biology10111205
APA StyleHuang, H. -T., Huang, T. -W., & Hong, C. -T. (2021). Bright Light Therapy for Parkinson Disease: A Literature Review and Meta-Analysis of Randomized Controlled Trials. Biology, 10(11), 1205. https://doi.org/10.3390/biology10111205