
Failure Rate, Marginal Bone Loss, and Pink Esthetic with Socket-Shield Technique for Immediate Dental Implant Placement in the Esthetic Zone. A Systematic Review and Meta-Analysis


 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Question of Interest
2.3. Databases and Search Strategy
2.4. Study Selection
2.5. Data Extraction and Study Outcomes
2.6. Methodological Quality Assessment
2.7. Quantitative Synthesis—Meta-Analysis
3. Results
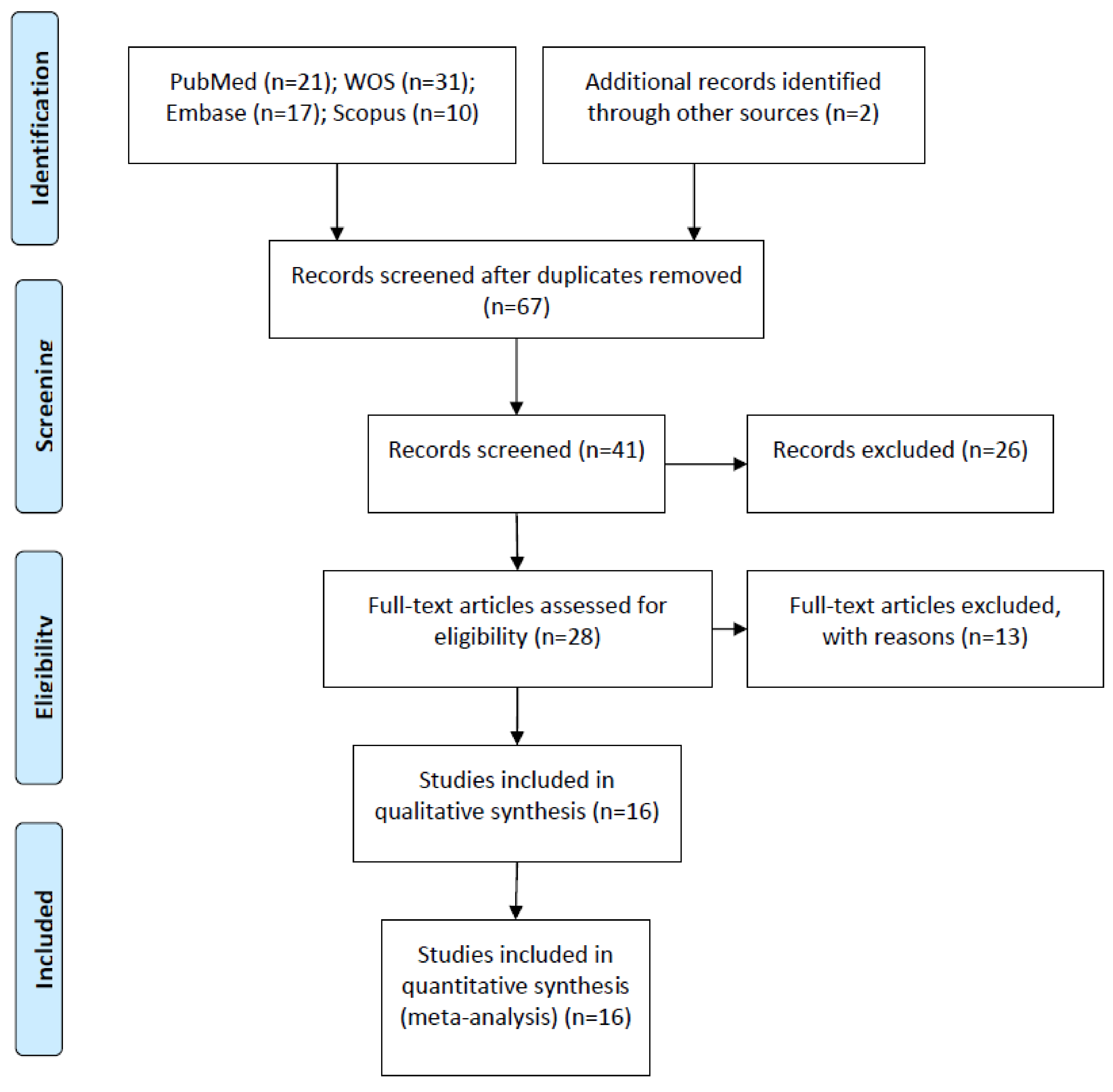
3.1. Flow Diagram
3.2. Qualitative Analysis
3.3. Quality Assessment
3.4. Quantitative Analysis
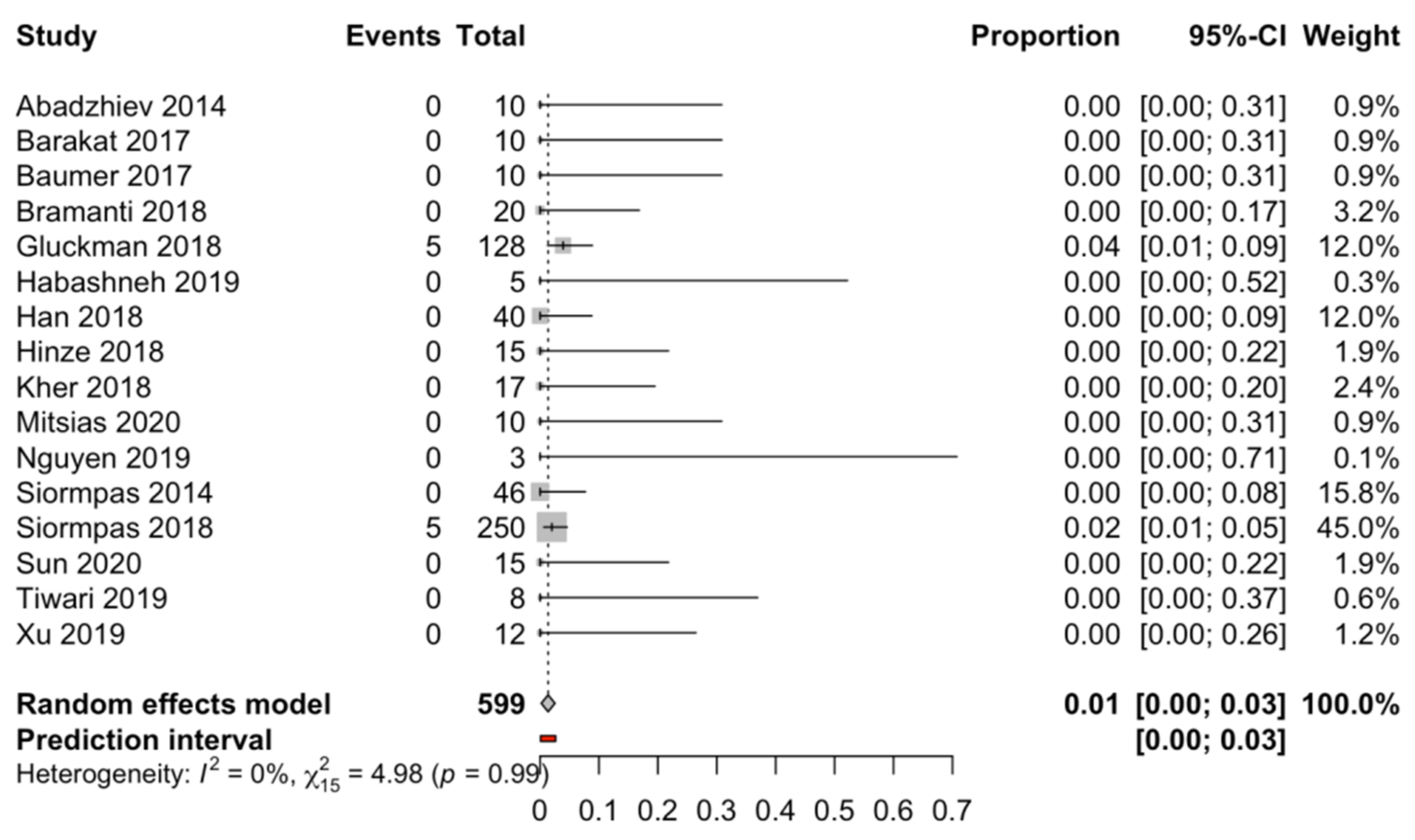
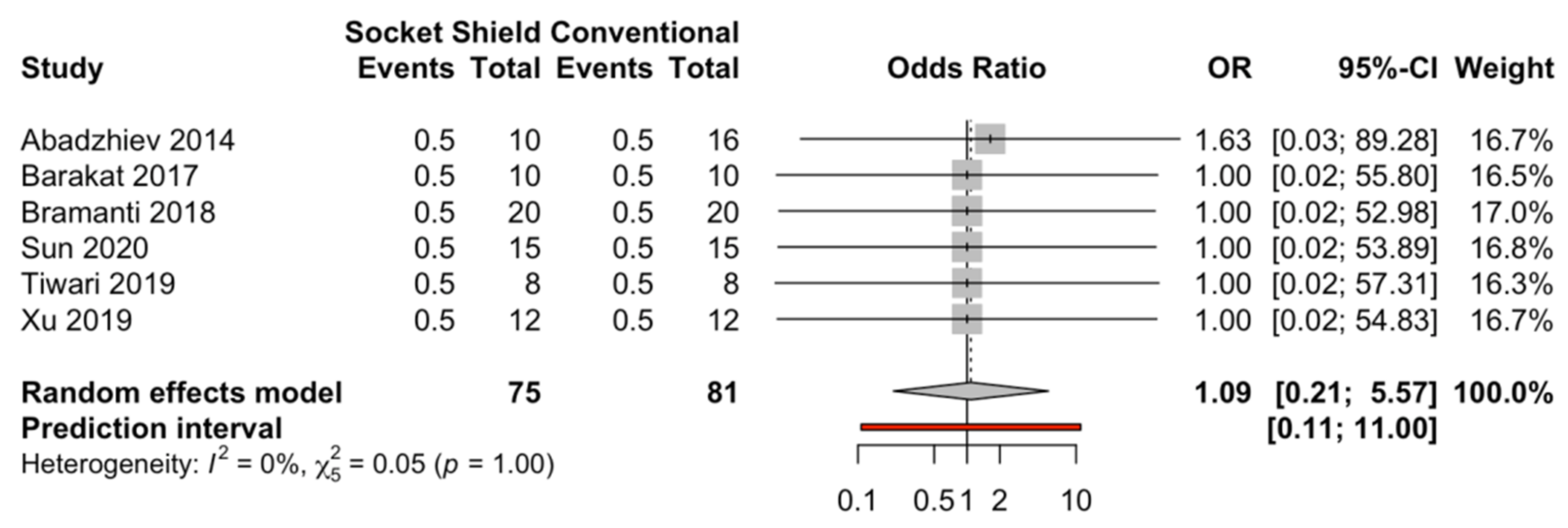
3.4.1. Failure Rate
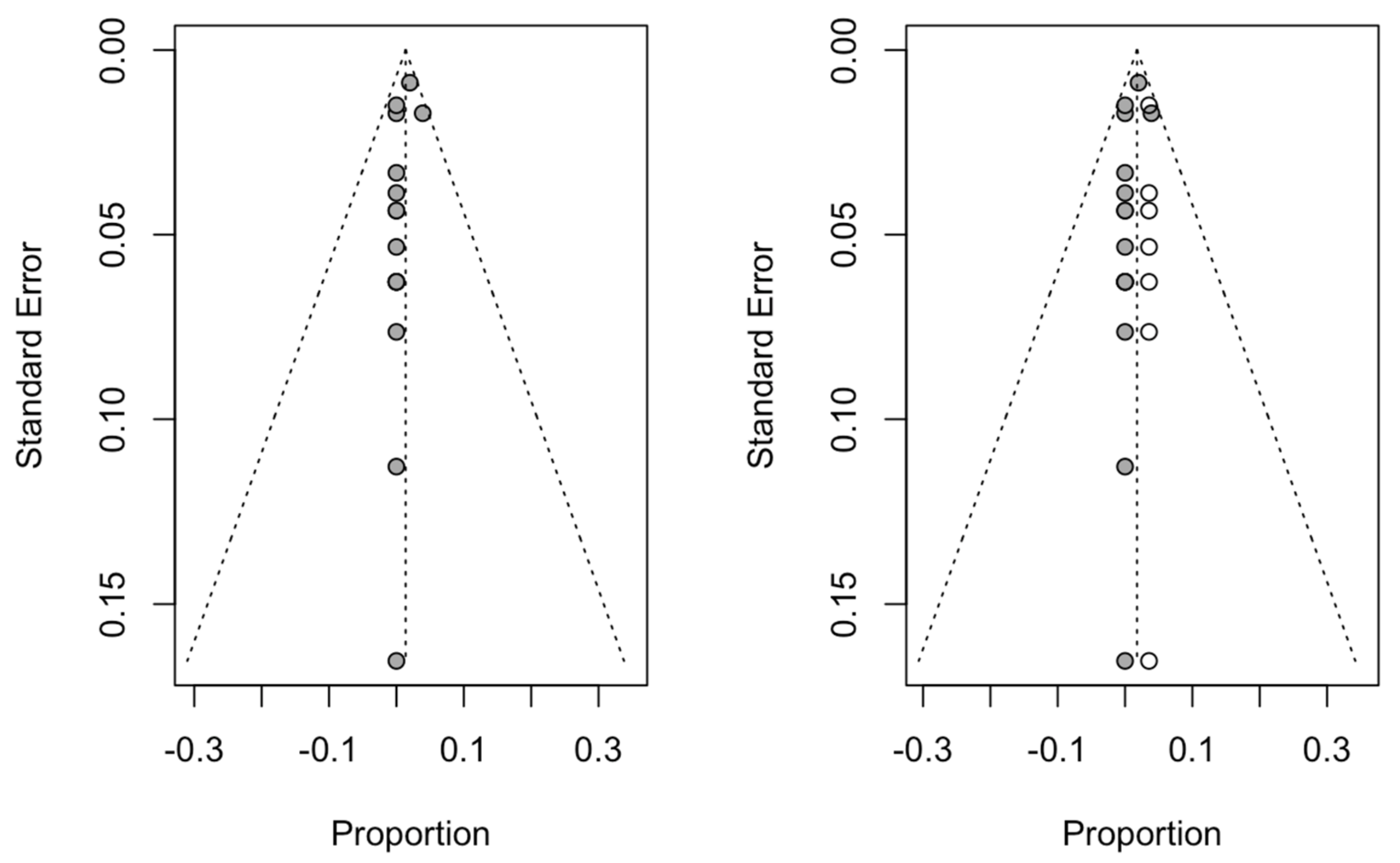
3.4.2. Publication Bias
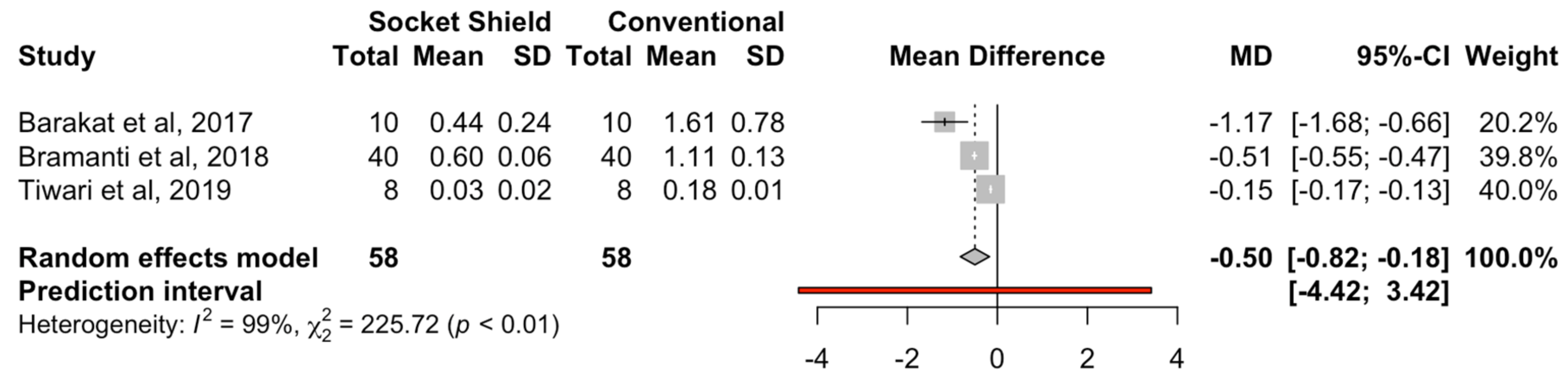
3.4.3. Marginal Bone Loss
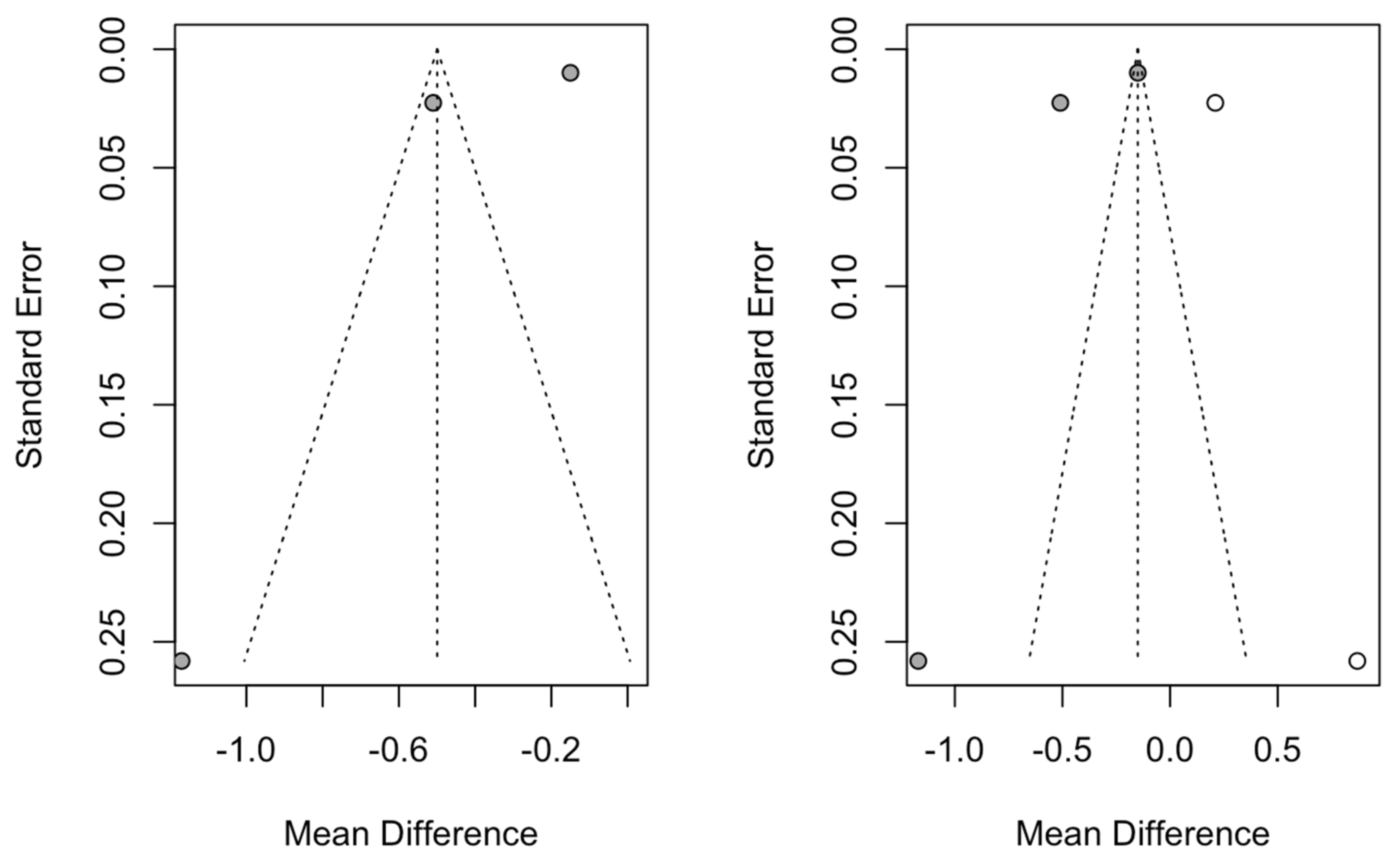
3.4.4. Publication Bias
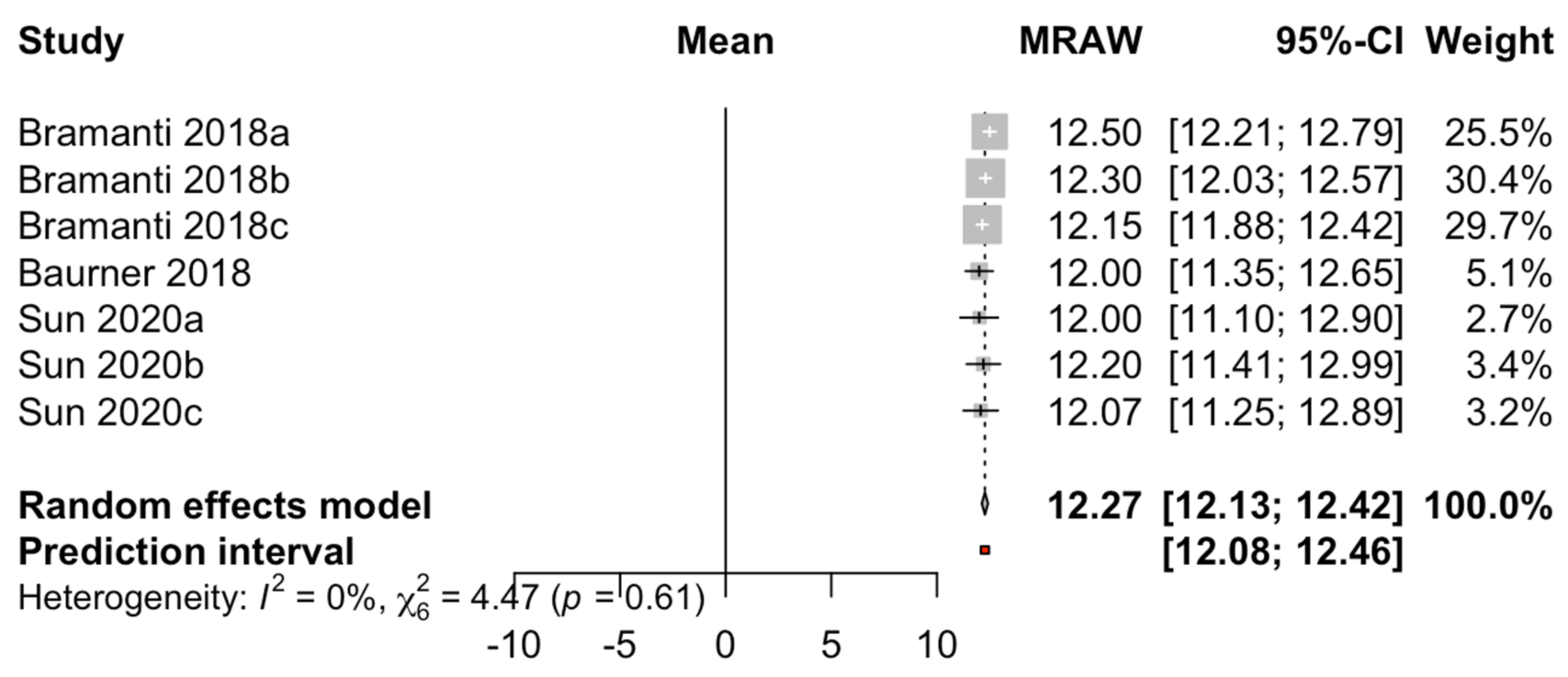
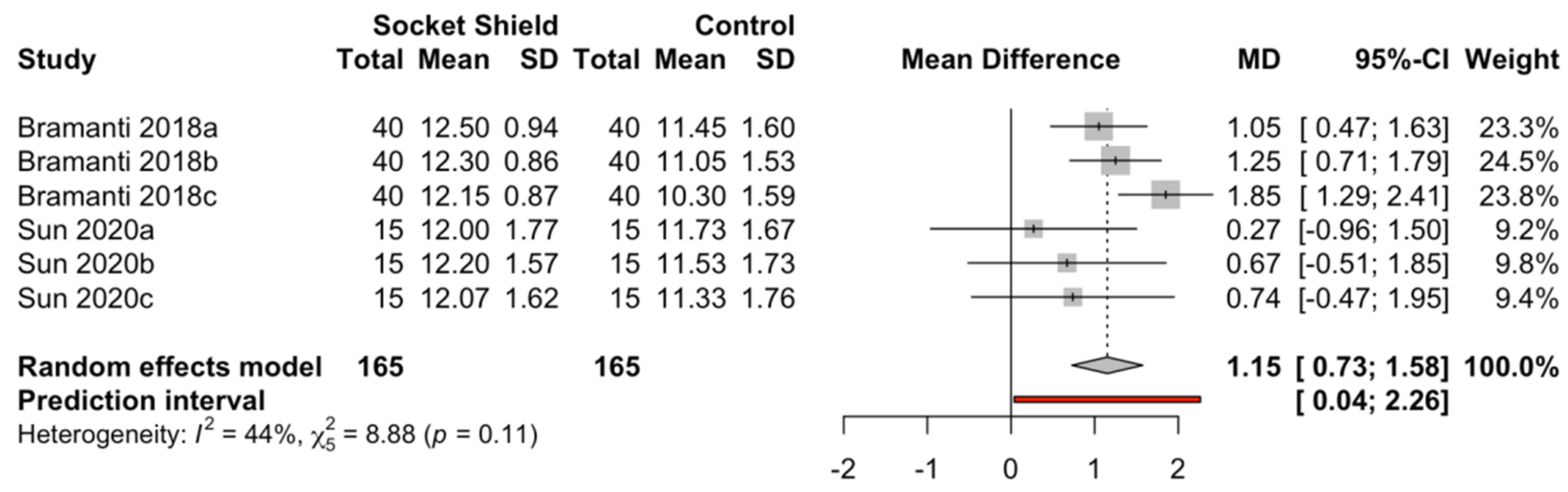
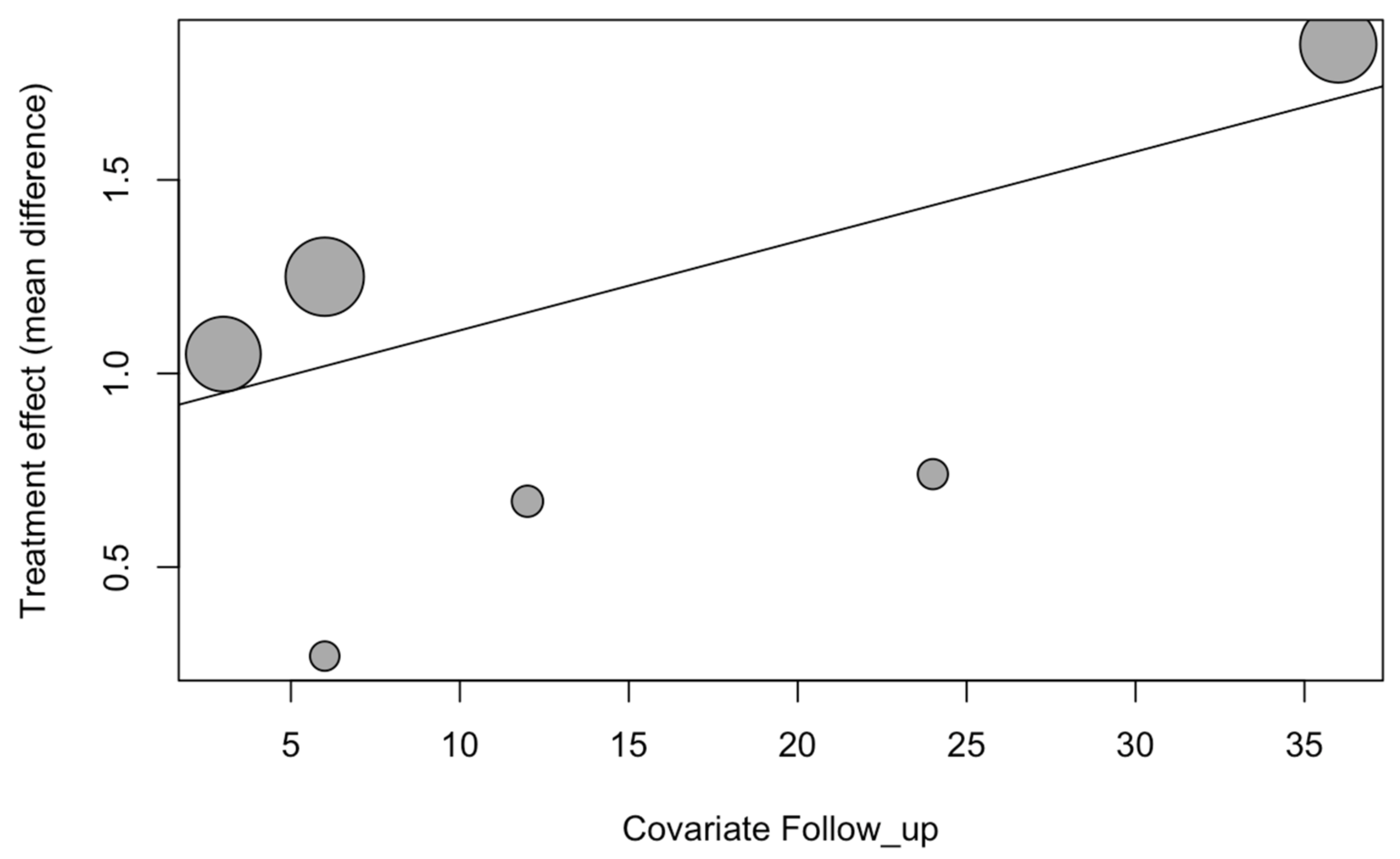
3.4.5. Pink Esthetic Score
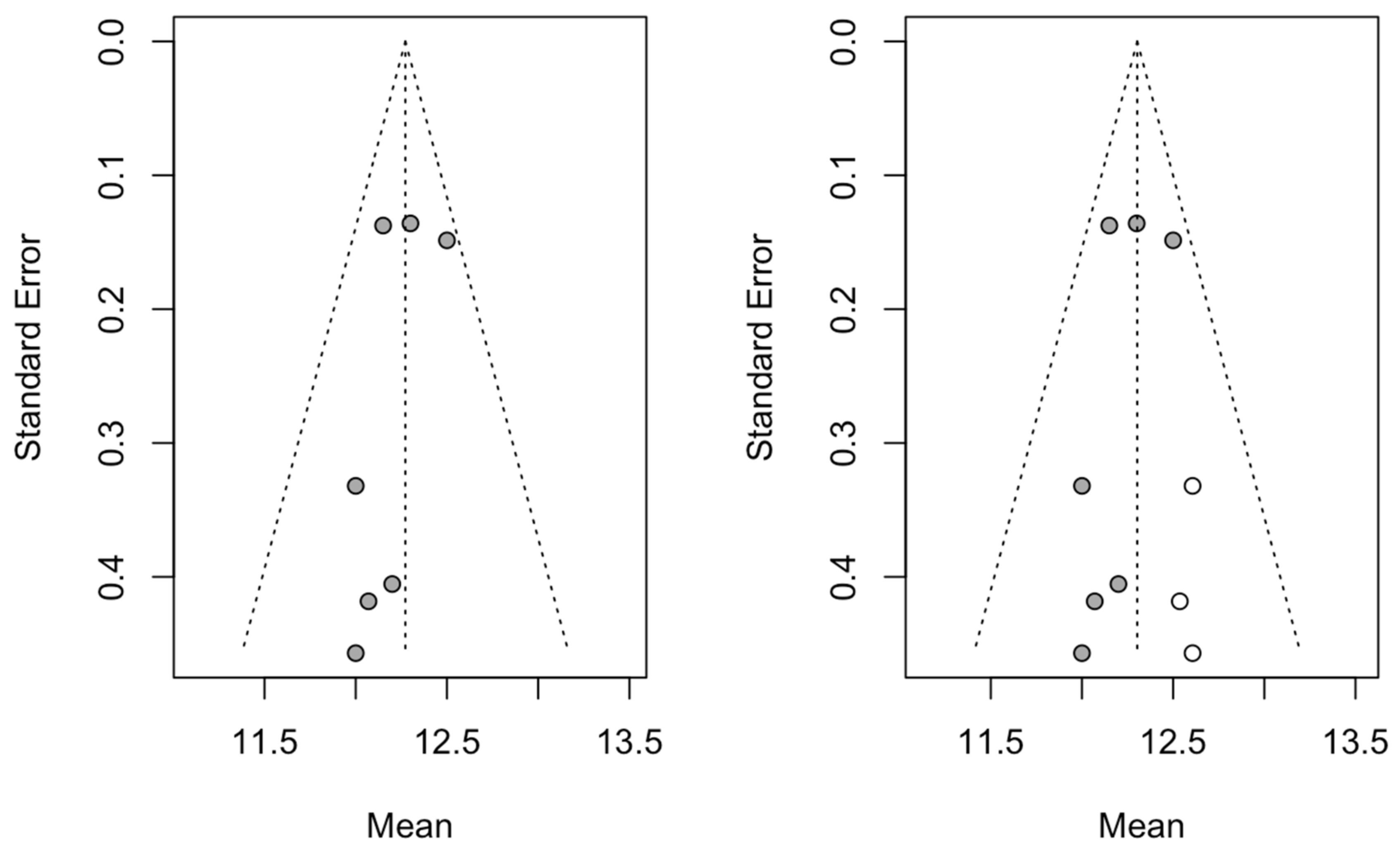
3.4.6. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| CI | Confidence Interval |
| PES | Pink esthetic score |
| OR | Odds ratio |
| NA | Not applicable |
| NAv | Not available |
| CIIP | Conventional immediate dental implant placement |
| SST | Socket-shield technique |
| RCT | Randomized controlled trial |
References
- Abd-Elrahman, A.; Shaheen, M.; Askar, N.; Atef, M. Socket shield technique vs conventional immediate implant placement with immediate temporization. Randomized clinical trial. Clin. Implant Dent. Relat. Res. 2020, 22, 602–611. [Google Scholar] [CrossRef]
- Siormpas, K.D.; Mitsias, M.E.; Kotsakis, G.A.; Tawil, I.; Pikos, M.A.; Mangano, F.G. The Root Membrane Technique: A Retrospective Clinical Study with up to 10 Years of Follow-Up. Implant Dent. 2018, 27, 564–574. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Troiano, M.; López-López, P.J.; Ramírez-Fernandez, M.P.; de Val Sanchze, J.E.; Marin, J.M.; Gehrke, S.A. Different configuration of socket shield technique in peri-implant bone preservation: An experimental study in dog mandible. Ann. Anat. 2016, 208, 109–115. [Google Scholar] [CrossRef]
- Bramanti, E.; Norcia, A.; Cicciù, M.; Matacena, G.; Cervino, G.; Troiano, G.; Zhurakivska, K.; Laino, L. Postextraction Dental Implant in the Aesthetic Zone, Socket Shield Technique Versus Conventional Protocol. J. Craniofac. Surg. 2018, 29, 1037–1041. [Google Scholar] [CrossRef] [PubMed]
- Han, C.H.; Park, K.B.; Mangano, F.G. The Modified Socket Shield Technique. J. Craniofac. Surg. 2018, 29, 2247–2254. [Google Scholar] [CrossRef]
- Barakat, D.A.; Hassan, R.S.; Eldibany, R.M. Evaluation of the shocket shield technique for immediate implantation. Alex. Dent. J. 2017, 42, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Giudice, A.; Bennardo, F.; Antonelli, A.; Barone, S.; Wagner, F.; Fortunato, L.; Traxler, H. Influence of clinician’s skill on primary implant stability with conventional and piezoelectric preparation techniques: An ex-vivo study. J. Biol. Regul. Homeost. Agents 2020, 34, 739–745. [Google Scholar] [PubMed]
- Siormpas, K.D.; Mitsias, M.E.; Kontsiotou-Siormpa, E.; Garber, D.; Kotsakis, G.A. Immediate implant placement in the esthetic zone utilizing the “root-membrane” technique: Clinical results up to 5 years postloading. Int. J. Oral Maxillofac. Implants 2014, 29, 1397–1405. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, V.G.; Flanagan, D.; Syrbu, J.; Nguyen, T.T. Socket Shield Technique Used in Conjunction with Immediate Implant Placement in the Anterior Maxilla: A Case Series. Clin. Adv. Periodontics 2020, 10, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implants Res. 2005, 16, 639–644. [Google Scholar] [CrossRef]
- Liberati, A.; Banzi, R.; Moja, L. Measuring the impact of evidence: The Cochrane systematic review of organized stroke care. Intern. Emerg. Med. 2009, 4, 507–510. [Google Scholar]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Sun, C.; Zhao, J.; Liu, Z.; Tan, L.; Huang, Y.; Zhao, L.; Tao, H. Comparing conventional flap-less immediate implantation and socket-shield technique for esthetic and clinical outcomes: A randomized clinical study. Clin. Oral Implants Res. 2020, 31, 181–191. [Google Scholar] [CrossRef]
- Tiwari, S.; Bedi, R.S.; Wadhwani, P.; Aurora, J.K.; Chauhan, H. Comparison of Immediate Implant Placement Following Extraction with and without Socket-Shield Technique in Esthetic Region. J. Maxillofac. Oral Surg. 2020, 19, 552–560. [Google Scholar] [CrossRef]
- Xu, Y.M.; Huang, H.; Wang, L.; Wu, Q.Q.; Fu, G.; Li, J. Comparison of clinical effects of a modified socket shield technique and the conventional immediate implant placement. Hua Xi Kou Qiang Yi Xue Za Zhi 2019, 37, 490–495. [Google Scholar]
- Kher, U.; Tunkiwala, A.; Shanbag, S. A graftless socket- shield technique for immediate implant placement in the esthetic zone. Clin. Oral Implants Res. 2018, 29, 451. [Google Scholar] [CrossRef] [Green Version]
- Bäumer, D.; Zuhr, O.; Rebele, S.; Hürzeler, M. Socket Shield Technique for immediate implant placement—Clinical, radiographic and volumetric data after 5 years. Clin. Oral Implants Res. 2017, 28, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, H.; Salama, M.; Du Toit, J. A retrospective evaluation of 128 socket-shield cases in the esthetic zone and posterior sites: Partial extraction therapy with up to 4 years follow-up. Clin. Implant Dent. Relat. Res. 2018, 20, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Hinze, M.; Janousch, R.; Goldhahn, S.; Schlee, M. Volumetric alterations around single-tooth implants using the socket-shield technique: Preliminary results of a prospective case series. Int. J. Esthet Dent. 2018, 13, 146–170. [Google Scholar] [PubMed]
- Habashneh, R.A.; Walid, M.A.; Abualteen, T.; Abukar, M. Socket-shield Technique and Immediate Implant Placement for Ridge Preservation: Case Report Series with 1-year Follow-up. J. Contemp. Dent. Pract. 2019, 20, 1108–1117. [Google Scholar] [CrossRef] [PubMed]
- Hürzeler, M.B.; Zuhr, O.; Schupbach, P.; Rebele, S.F.; Emmanouilidis, N.; Fickl, S. The socket-shield technique: A proof-of-principle report. J. Clin. Periodontol. 2010, 37, 855–862. [Google Scholar] [CrossRef]
- Araújo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontol. 2000 2015, 68, 122–134. [Google Scholar] [CrossRef]
- Tsigarida, A.; Toscano, J.; de Brito Bezerra, B.; Geminiani, A.; Barmak, A.B.; Caton, J.; Papaspyridakos, P.; Chochlidakis, K. Buccal bone thickness of maxillary anterior teeth: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 1326–1343. [Google Scholar] [CrossRef]
- Monje, A.; Chappuis, V.; Monje, F.; Muñoz, F.; Wang, H.L.; Urban, I.A.; Buser, D. The Critical Peri-implant Buccal Bone Wall Thickness Revisited: An Experimental Study in the Beagle Dog. Int. J. Oral Maxillofac. Implants 2019, 34, 1328–1336. [Google Scholar] [CrossRef]
- Mitsias, M.E.; Siormpas, K.D.; Kotsakis, G.A.; Ganz, S.D.; Mangano, C.; Iezzi, G. The Root Membrane Technique: Human Histologic Evidence after Five Years of Function. Biomed. Res. Int. 2017, 2017, 7269467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bäumer, D.; Zuhr, O.; Rebele, S.; Schneider, D.; Schupbach, P.; Hürzeler, M. The socket-shield technique: First histological, clinical, and volumetrical observations after separation of the buccal tooth segment—A pilot study. Clin. Implant Dent. Relat. Res. 2015, 17, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Blaschke, C.; Schwass, D.R. The socket-shield technique: A critical literature review. Int. J. Implant Dent. 2020, 6, 52. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Sitalaksmi, R.M.; Miyashita, M.; Maekawa, K.; Ryu, M.; Kimura-Ono, A.; Suganuma, T.; Kikutani, T.; Fujisawa, M.; Tamaki, K.; et al. Effectiveness of the Socket Shield Technique in Dental Implant: A Systematic Review. J. Prosthodont. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hof, M.; Umar, N.; Budas, N.; Seemann, R.; Pommer, B.; Zechner, W. Evaluation of implant esthetics using eight objective indices-Comparative analysis of reliability and validity. Clin. Oral Implants Res. 2018, 29, 697–706. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Jadad Criteria | ||||||
|---|---|---|---|---|---|---|
| Author/Year | Is the Study Described as Randomized? | Is the Study Described as Double-Blinded? | Was There a Description of Withdrawals and Dropouts? | Was the Method of Randomization Adequate? | Was the Method of Blinding Appropriate? | Score |
| Abadzhiev et al., 2014 [15] | 0 | 0 | 0 | 0 | 0 | 0 |
| Barakat et al., 2017 [6] | 1 | 0 | 0 | NAv | 0 | 1 |
| Baumer et al., 2017 [19] | NA | NA | NA | NA | NA | NA |
| Bramanti et al., 2018 [4] | 1 | 1 | 0 | 1 | 1 | 4 |
| Gluckman et al., 2018 [20] | NA | NA | NA | NA | NA | NA |
| Habasneh et al., 2019 [22] | NA | NA | NA | NA | NA | NA |
| Han et al., 2018 [5] | 0 | 0 | 0 | 0 | 0 | 0 |
| Hinze et al., 2018 [21] | NA | NA | NA | NA | NA | NA |
| Kher et al., 2018 [18] | 0 | 0 | 0 | 0 | 0 | 0 |
| Mitsias et al., 2020 [16] | 0 | 0 | 0 | 0 | 0 | 0 |
| Nguyen et al., 2019 [8] | NA | NA | NA | NA | NA | NA |
| Siormpas et al., 2014 [7] | NA | NA | NA | NA | NA | NA |
| Siormpas et al., 2018 [2] | NA | NA | NA | NA | NA | NA |
| Sun et al., 2020 [12] | 1 | 1 | 0 | 1 | 1 | 4 |
| Tiwari et al., 2019 [13] | 1 | 0 | 0 | Nav | 0 | 1 |
| Xu et al., 2019 [14] | NAv | NAv | NAv | NAv | NAv | NAv |
| Author/Year | Study Type | Sample (n) | Follow-Up Time (Months) | Dental Implant Failure Rate | Marginal Bone Loss | Soft Tissue Results and Pink Esthetic |
|---|---|---|---|---|---|---|
| Abadzhiev et al., 2014 [15] | Prospective clinical trial | 26 dental implants (25 patients 20–64 years old) | 24 | 0/16 CIIP 0/10 SST | CIIP: 12% bone loss (5 mm) SST: 2% bone loss (0.8 mm) | CIIP: 12% attached gingiva loss (5 mm) SST: 2% attached gingiva loss (0.8 mm) |
| Barakat et al., 2017 [6] | RCT | 20 dental implants (20 patients 20–50 years old) | 7 | 0/10 CIIP 0/10 SST | CIIP: 1.61 ± 0.78 mm vertical bone loss SST: 0.44 ± 0.24 mm vertical bone loss | CIIP: 2.12 ± 0.64 mm probing depth SST: 1.73 ± 0.28 mm probing depth |
| Baumer et al., 2017 [19] | Retrospective study | 10 dental implants (10 patients) | 51–63 | 0/10 SST | 0.33 ± 0.43 mm mesial and 0.17 ± 0.36 mm distal marginal bone loss | SST: −0.37 ± 0.18 mm loss of buccal tissue and −0.33 ± 0.23 mm mid-facial recession Pink aesthetic score: 12 |
| Bramanti et al., 2018 [4] | RCT | 40 dental implants (40 patients) | 36 | 0/20 CIIP 0/20 SST | CIIP: 1.11 ± 0.13 mm marginal bone loss SST: 0.60 ± 0.06 mm marginal bone loss | CIIP: Pink aesthetic score: 10.30 ± 2.53 SST: Pink aesthetic score: 12.15 ± 0.76 |
| Gluckman et al., 2018 [20] | Retrospective study | 128 dental implants (128 patients 24–71 years old) | 48 | 5/128 SST | NAv | NAv |
| Habasneh et al., 2019 [22] | Case series | 5 dental implants (5 patients 20–54 years old) | 12 | 0/5 SST | NAv | NAv |
| Han et al., 2018 [5] | Prospective clinical trial | 40 dental implants (30 patients 20–82 years old) | 12 | 0/40 SST | NAv | 0/40 SST |
| Hinze et al., 2018 [21] | Case series | 17 dental implants (15 patients 26–66 years old) | 3 | 0/17 SST | NAv | SST: 0.17 ± 0.67 mm change in the gingival margin SST: 8/15 patients suffer recession SST: 0.31 ± 0.64 mm mesial papilla height change and −0.38 ± 0.57 mm distal papilla height change |
| Kher et al., 2018 [18] | Prospective clinical trial | 21 dental implants (17 patients 26–66 years old) | 12–42 | 0/21 SST | NAv | SST: Pink aesthetic score: 12 |
| Mitsias et al., 2020 [16] | Prospective clinical trial | 10 dental implants (10 patients) | 42 | 0/10 SST | NAv | SST: 0.19 mm (0.10–0.28 mm) mid-facial recession |
| Nguyen et al., 2019 [8] | Case series | 4 dental implants (3 patients 62–87 years old) | 24–72 | 0/4 SST | 0.1 ± 0.2 mm marginal bone loss | SST: No changes in soft tissue dimensions |
| Siormpas et al., 2014 [7] | Retrospective study | 46 dental implants (46 patients 28–70 years old) | 24–60 | 0/46 SST | 0.18 ± 0.09 mm mesial and 0.21 ± 0.09 mm distal marginal bone loss | NAv |
| Siormpas et al., 2018 [2] | Retrospective study | 250 dental implants (182 patients 18–83 years old) | 120 | 5/250 SST | NAv | NAv |
| Sun et al., 2020 [12] | RCT | 30 dental implants (30 patients | 24 | 0/15 CIIP 0/15 SST | NAv | CIIP: Pink aesthetic score: 11.33 ± 1.76 SST: Pink aesthetic score: 12.07 ± 1.62 |
| Tiwari et al., 2019 [13] | RCT | 16 dental implants (16 patients) | 12 | 0/8 CIIP 0/8 SST | CIIP: 0.188 ± 0.013 mm marginal bone loss SST: 0.030 ± 0.025 mm marginal bone loss | CIIP: Labial bone thickness: 0.988 ± 0.173 mm SST: Labial bone thickness: 1.145 ± 0.277 mm |
| Xu et al., 2019 [14] | Prospective clinical trial | 24 dental implants (24 patients) | 12 | 0/12 CIIP 0/12 SST | NAv | SST higher PES than CIIP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velasco Bohórquez, P.; Rucco, R.; Zubizarreta-Macho, Á.; Montiel-Company, J.M.; de la Vega Buró, S.; Madroño, E.C.; Marín, L.S.H.; Hernández Montero, S. Failure Rate, Marginal Bone Loss, and Pink Esthetic with Socket-Shield Technique for Immediate Dental Implant Placement in the Esthetic Zone. A Systematic Review and Meta-Analysis. Biology 2021, 10, 549. https://doi.org/10.3390/biology10060549
Velasco Bohórquez P, Rucco R, Zubizarreta-Macho Á, Montiel-Company JM, de la Vega Buró S, Madroño EC, Marín LSH, Hernández Montero S. Failure Rate, Marginal Bone Loss, and Pink Esthetic with Socket-Shield Technique for Immediate Dental Implant Placement in the Esthetic Zone. A Systematic Review and Meta-Analysis. Biology. 2021; 10(6):549. https://doi.org/10.3390/biology10060549
Chicago/Turabian StyleVelasco Bohórquez, Pilar, Roberta Rucco, Álvaro Zubizarreta-Macho, José María Montiel-Company, Susana de la Vega Buró, Esther Cáceres Madroño, Lara San Hipólito Marín, and Sofía Hernández Montero. 2021. "Failure Rate, Marginal Bone Loss, and Pink Esthetic with Socket-Shield Technique for Immediate Dental Implant Placement in the Esthetic Zone. A Systematic Review and Meta-Analysis" Biology 10, no. 6: 549. https://doi.org/10.3390/biology10060549
APA StyleVelasco Bohórquez, P., Rucco, R., Zubizarreta-Macho, Á., Montiel-Company, J. M., de la Vega Buró, S., Madroño, E. C., Marín, L. S. H., & Hernández Montero, S. (2021). Failure Rate, Marginal Bone Loss, and Pink Esthetic with Socket-Shield Technique for Immediate Dental Implant Placement in the Esthetic Zone. A Systematic Review and Meta-Analysis. Biology, 10(6), 549. https://doi.org/10.3390/biology10060549