
Longitudinal 3D Study of Anterior Tooth Wear from Adolescence to Adulthood in Modern Humans

 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Sample
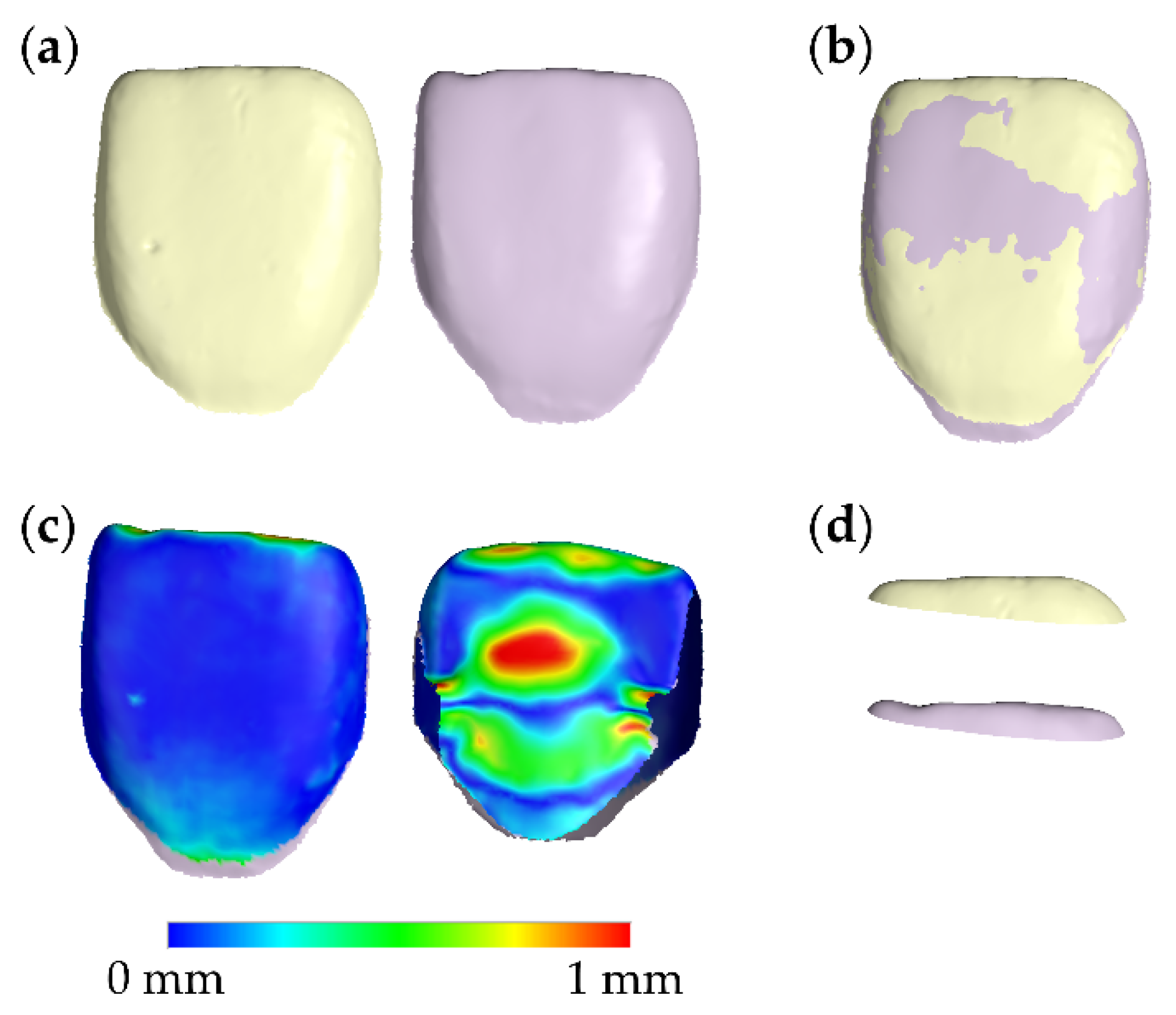
2.3. Tooth Wear Assessment Workflow
2.4. Method Error
2.5. Statistical Analysis
3. Results
3.1. Method Error
3.2. Tooth Wear Differences between Contralateral Sides
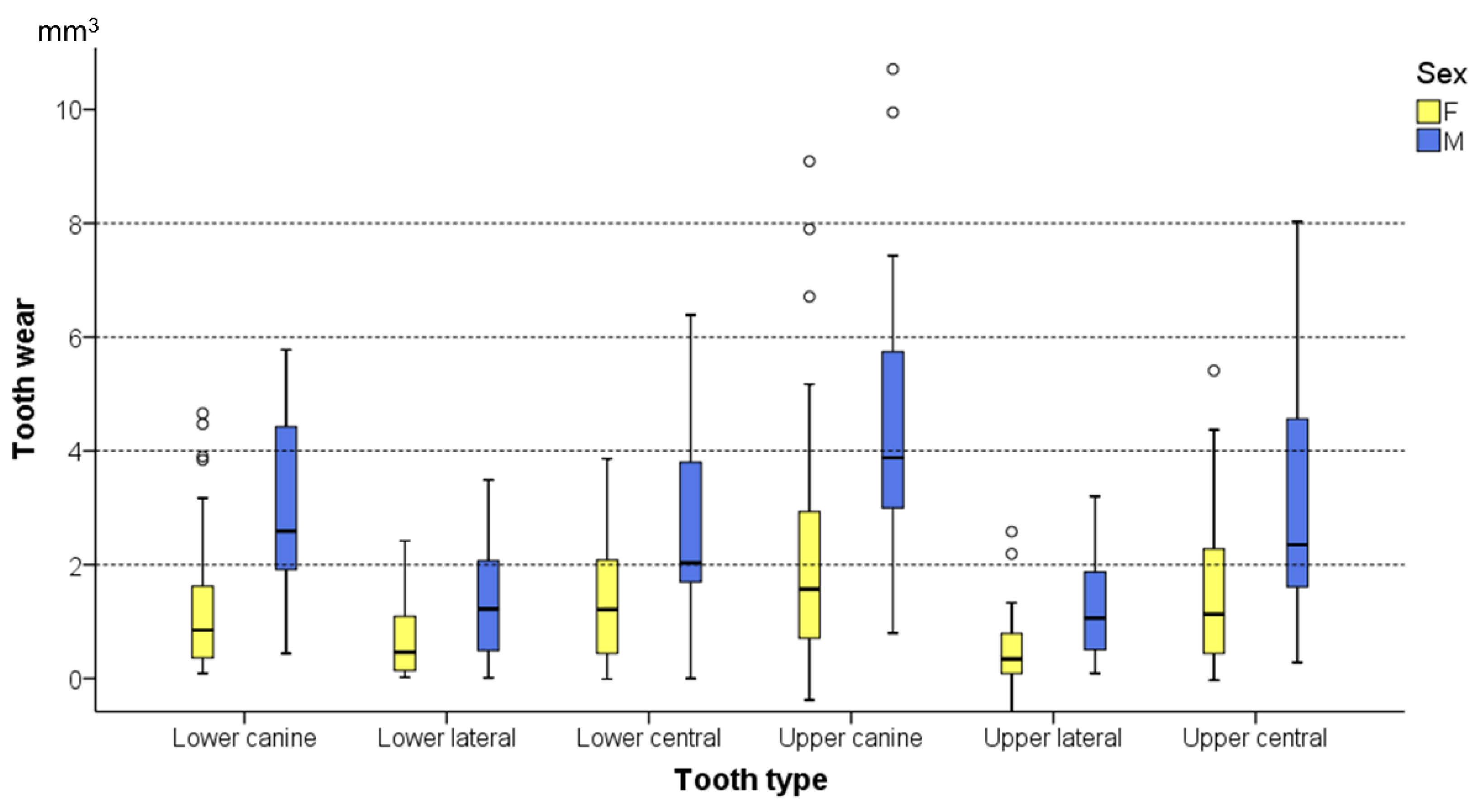
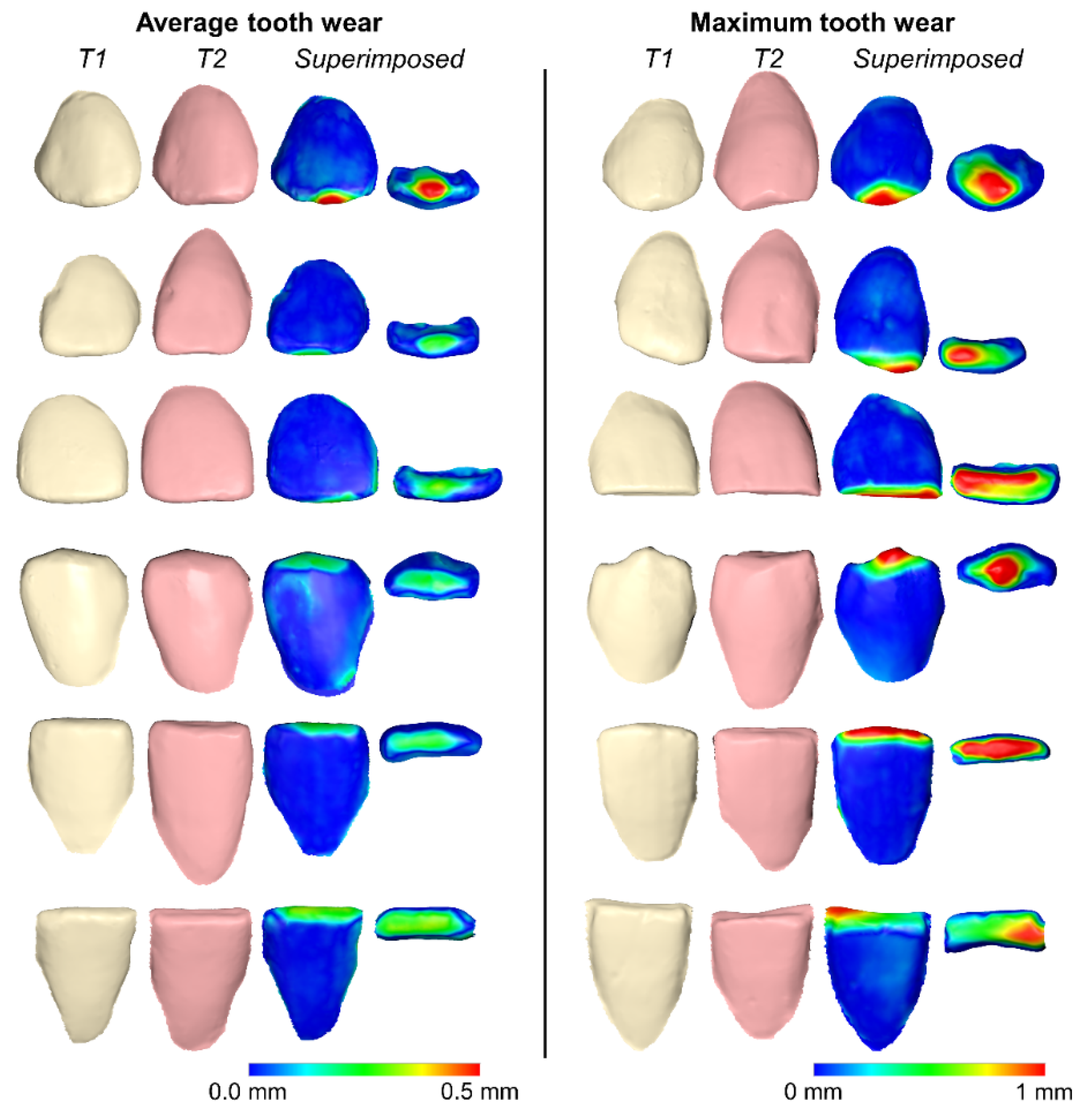
3.3. Tooth Wear among Tooth Types and between Sexes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cunha-Cruz, J.; Pashova, H.; Packard, J.D.; Zhou, L.; Hilton, T.J.; Northwest PRECEDENT. Tooth wear: Prevalence and associated factors in general practice patients. Community Dent. Oral Epidemiol. 2010, 38, 228–234. [Google Scholar] [CrossRef] [Green Version]
- Schierz, O.; Dommel, S.; Hirsch, C.; Reissmann, D.R. Occlusal tooth wear in the general population of Germany: Effects of age, sex, and location of teeth. J. Prosthet. Dent. 2014, 112, 465–471. [Google Scholar] [CrossRef]
- Kuijpers, M.A.; Kiliaridis, S.; Renkema, A.; Bronkhorst, E.M.; Kuijpers-Jagtman, A.M. Anterior tooth wear and retention type until 5 years after orthodontic treatment. Acta Odontol. Scand. 2009, 67, 176–181. [Google Scholar] [CrossRef]
- Kitasako, Y.; Sasaki, Y.; Takagaki, T.; Sadr, A.; Tagami, J. Age-specific prevalence of erosive tooth wear by acidic diet and gastroesophageal reflux in Japan. J. Dent. 2015, 43, 418–423. [Google Scholar] [CrossRef]
- Goldfarb, M.B.; Hara, A.T.; Hirsh, A.T.; Carvalho, J.C.; Maupome, G. Are dental patients able to perceive erosive tooth wear on anterior teeth?: An internet-based survey assessing awareness and related action. J. Am. Dent. Assoc. 2020, 151, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Zhang, M.; Chen, Y.; Yao, Y. Tooth wear in aging people: An investigation of the prevalence and the influential factors of incisal/occlusal tooth wear in northwest China. BMC Oral Health 2014, 14, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, K.E.; Whitters, J.; Ju, X.; Pierce, S.G.; MacLeod, C.N.; Murray, C.A. Clinical Monitoring of Tooth Wear Progression in Patients over a Period of One Year Using CAD/CAM. Int. J. Prosthodont. 2017, 30, 153–155. [Google Scholar] [CrossRef] [Green Version]
- Marro, M.L.; Aranguiz, V.; Ramirez, V.; Lussi, A. Prevalence of erosive tooth wear in Chilean adults, 2016: A cross-sectional study. J. Oral Rehabil. 2020, 47, 467–472. [Google Scholar] [CrossRef]
- Awad, M.A.; El Kassas, D.; Al Harthi, L.; Abraham, S.B.; Al-Khalifa, K.S.; Khalaf, M.E.; Al Habashneh, R.; Bartlett, D. Prevalence, severity and explanatory factors of tooth wear in Arab populations. J. Dent. 2019, 80, 69–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olley, R.C.; Moazzez, R.; Bartlett, D. The relationship between incisal/occlusal wear, dentine hypersensitivity and time after the last acid exposure in vivo. J. Dent. 2015, 43, 248–252. [Google Scholar] [CrossRef]
- Van’t Spijker, A.; Kreulen, C.M.; Bronkhorst, E.M.; Creugers, N.H. Occlusal wear and occlusal condition in a convenience sample of young adults. J. Dent. 2015, 43, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Oltramari-Navarro, P.V.; Janson, G.; de Oliveira, R.B.; Quaglio, C.L.; Castanha Henriques, J.F.; de Carvalho Sales-Peres, S.H.; McNamara, J.A., Jr. Tooth-wear patterns in adolescents with normal occlusion and Class II Division 2 malocclusion. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 730.e1–730.e5. [Google Scholar] [CrossRef]
- Janson, G.; Oltramari-Navarro, P.V.; de Oliveira, R.B.; Quaglio, C.L.; Sales-Peres, S.H.; Tompson, B. Tooth-wear patterns in subjects with Class II Division 1 malocclusion and normal occlusion. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 14.e1–14.e7; discussion 14–15. [Google Scholar] [CrossRef]
- Meng, M.; Zhang, Q.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.; Ma, C.; Zhang, S. Occlusal tooth wear in patients of a dental school’s prosthodontic department in Xi’an, China. Int. J. Prosthodont. 2014, 27, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Wazani, B.E.; Dodd, M.N.; Milosevic, A. The signs and symptoms of tooth wear in a referred group of patients. Br. Dent. J. 2012, 213, E10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, A.W.; Moon, W.; Gandini, L.G., Jr. Influence of maxillary incisor edge asymmetries on the perception of smile esthetics among orthodontists and laypersons. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 658–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betrine Ribeiro, J.; Alecrim Figueiredo, B.; Wilson Machado, A. Does the presence of unilateral maxillary incisor edge asymmetries influence the perception of smile esthetics? J. Esthet. Restor. Dent. 2017, 29, 291–297. [Google Scholar] [CrossRef]
- Sobral, M.C.; Crusoe-Rebello, I.M.; Machado, A.W. Does the presence of maxillary central incisor edge asymmetry influence the perception of dentofacial esthetics in video analysis? Angle Orthod. 2019, 89, 775–780. [Google Scholar] [CrossRef] [Green Version]
- Al-Allaq, T.; Feng, C.; Saunders, R.H. Anterior tooth wear and quality of life in a nursing home population. Spec. Care Dent. 2018, 38, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Loomans, B.; Opdam, N. A guide to managing tooth wear: The Radboud philosophy. Br. Dent. J. 2018, 224, 348–356. [Google Scholar] [CrossRef]
- Hasselkvist, A.; Johansson, A.; Johansson, A.K. A 4 year prospective longitudinal study of progression of dental erosion associated to lifestyle in 13-14 year-old Swedish adolescents. J. Dent. 2016, 47, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Omiri, M.K.; Sghaireen, M.G.; Alzarea, B.K.; Lynch, E. Quantification of incisal tooth wear in upper anterior teeth: Conventional vs new method using toolmakers microscope and a three-dimensional measuring technique. J. Dent. 2013, 41, 1214–1221. [Google Scholar] [CrossRef] [PubMed]
- Wulfman, C.; Koenig, V.; Mainjot, A.K. Wear measurement of dental tissues and materials in clinical studies: A systematic review. Dent. Mater. 2018, 34, 825–850. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Dritsas, K.; Katsaros, C.; Halazonetis, D.; Ren, Y. 3D Method for Occlusal Tooth Wear Assessment in Presence of Substantial Changes on Other Tooth Surfaces. J. Clin. Med. 2020, 9, 3937. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Dritsas, K.; Ren, Y.; Halazonetis, D.; Katsaros, C. An accurate and efficient method for occlusal tooth wear assessment using 3D digital dental models. Sci. Rep. 2020, 10, 10103. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, S.; Osnes, C.; Bartlett, D.; Keeling, A. Investigation into the validity of WearCompare, a purpose-built software to quantify erosive tooth wear progression. Dent. Mater. 2019, 35, 1408–1414. [Google Scholar] [CrossRef]
- Gkantidis, N.; Dritsas, K.; Katsaros, C.; Halazonetis, D.; Ren, Y. 3D Occlusal Tooth Wear Assessment in Presence of Limited Changes in Non-Occlusal Surfaces. Diagnostics 2021, 11, 1033. [Google Scholar] [CrossRef]
- Korkut, B.; Tagtekin, D.; Murat, N.; Yanikoglu, F. Clinical Quantitative Evaluation of Tooth Wear: A 4-year Longitudinal Study. Oral Health Prev. Dent. 2020, 18, 719–729. [Google Scholar] [CrossRef]
- O’Toole, S.; Lau, J.S.; Rees, M.; Warburton, F.; Loomans, B.; Bartlett, D. Quantitative tooth wear analysis of index teeth compared to complete dentition. J. Dent. 2020, 97, 103342. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [Green Version]
- Gebistorf, M.; Mijuskovic, M.; Pandis, N.; Fudalej, P.S.; Katsaros, C. Gingival recession in orthodontic patients 10 to 15 years posttreatment: A retrospective cohort study. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Besl, P.J.; Mckay, N.D. A Method for Registration of 3-D Shapes. IEEE T Pattern Anal. 1992, 14, 239–256. [Google Scholar] [CrossRef]
- Ray, D.S.; Wiemann, A.H.; Patel, P.B.; Ding, X.; Kryscio, R.J.; Miller, C.S. Estimation of the rate of tooth wear in permanent incisors: A cross-sectional digital radiographic study. J. Oral Rehabil. 2015, 42, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Stucki, S.; Gkantidis, N. Assessment of techniques used for superimposition of maxillary and mandibular 3D surface models to evaluate tooth movement: A systematic review. Eur. J. Orthod. 2019. [Google Scholar] [CrossRef]
- Winkler, J.; Gkantidis, N. Trueness and precision of intraoral scanners in the maxillary dental arch: An in vivo analysis. Sci. Rep. 2020, 10, 1172. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Canines | Lateral Incisors | Central Incisors | |||
|---|---|---|---|---|---|
| Upper | Lower | Upper | Lower | Upper | Lower |
| n = 71 | n = 65 | n = 67 | n = 61 | n = 65 | n = 56 |
| 53F, 18M | 50F, 15M | 51F, 16M | 47F, 14M | 51F, 14M | 41F, 15M |
| 67R, 68L | 60R, 63L | 58R, 63L | 55R, 51L | 54R, 58L | 49R, 45L |
| T1 | T2 | ||
|---|---|---|---|
| Angle Class 1 | Class I | 70 | 61 |
| Class II | 2 (unilateral) | 11 (9 unilateral, 2 bilateral) | |
| Overjet 2 | Normal | 72 | 70 |
| Increased | 0 | 2 | |
| Overbite 3 | Normal | 65 | 58 |
| Reduced * | 7 | 14 |
| Source | df | F | Sig. |
|---|---|---|---|
| Corrected Model | 13 | 16.35 | 0.000 |
| Intercept | 1 | 0.08 | 0.782 |
| Patient | 1 | 3.45 | 0.064 |
| Assessment period | 1 | 11.37 | 0.001 |
| Tooth type | 5 | 20.76 | 0.000 |
| Sex | 1 | 74.57 | 0.000 |
| Tooth type × Sex | 5 | 2.77 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkantidis, N.; Dritsas, K.; Gebistorf, M.; Halazonetis, D.; Ren, Y.; Katsaros, C. Longitudinal 3D Study of Anterior Tooth Wear from Adolescence to Adulthood in Modern Humans. Biology 2021, 10, 660. https://doi.org/10.3390/biology10070660
Gkantidis N, Dritsas K, Gebistorf M, Halazonetis D, Ren Y, Katsaros C. Longitudinal 3D Study of Anterior Tooth Wear from Adolescence to Adulthood in Modern Humans. Biology. 2021; 10(7):660. https://doi.org/10.3390/biology10070660
Chicago/Turabian StyleGkantidis, Nikolaos, Konstantinos Dritsas, Meret Gebistorf, Demetrios Halazonetis, Yijin Ren, and Christos Katsaros. 2021. "Longitudinal 3D Study of Anterior Tooth Wear from Adolescence to Adulthood in Modern Humans" Biology 10, no. 7: 660. https://doi.org/10.3390/biology10070660
APA StyleGkantidis, N., Dritsas, K., Gebistorf, M., Halazonetis, D., Ren, Y., & Katsaros, C. (2021). Longitudinal 3D Study of Anterior Tooth Wear from Adolescence to Adulthood in Modern Humans. Biology, 10(7), 660. https://doi.org/10.3390/biology10070660