
Repeatability and Reliability of the Rheumatoid Arthritis Foot Disease Activity Index in Spanish Patients: A Transcultural Adaptation

 ,
,  ,
,  ,
,  , , , and
, , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Procedure
2.3. Translation Procedure
- A. The authors of the original RADAI-F5 clinimetric tool were contacted to request their permission for its translation [16].
- B. Two neutral polyglot Spanish interpreters performed the translation.
- C. The version of the agreement in the following translations was developed by each translator individually.
- D. Three of the authors of this investigation (ENF, MLLI and RBBV), all of them podiatrists, translated the ordered RADAI-F5 into Spanish and translated forward.
- E. The comparison of the final version with the main statement verified conceptual concordance and whether interpretations were already translated, confused or discrepant.
- F. An arrangement was made by the research team (4 podiatrists ENF, DLL, PPL, 2 nurses RBBV; MELI and 1 physiotherapists EMMJ) to finish the translation.
- G. An intellectual evaluation for podiatric medical clinics was developed to provide feasibility and prevent potential misunderstandings [22].
2.4. Statistical Analysis
3. Results
3.1. Translation
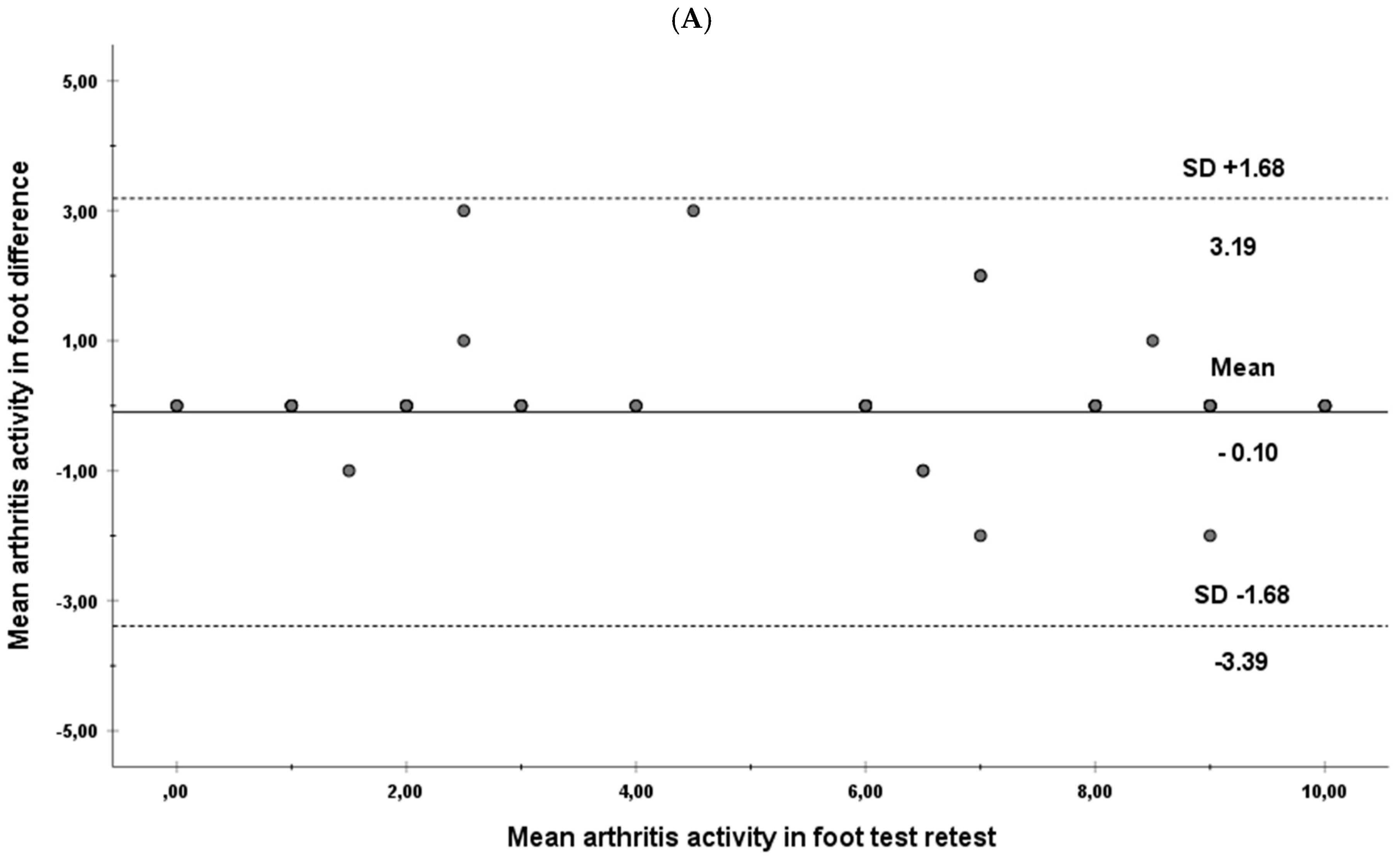
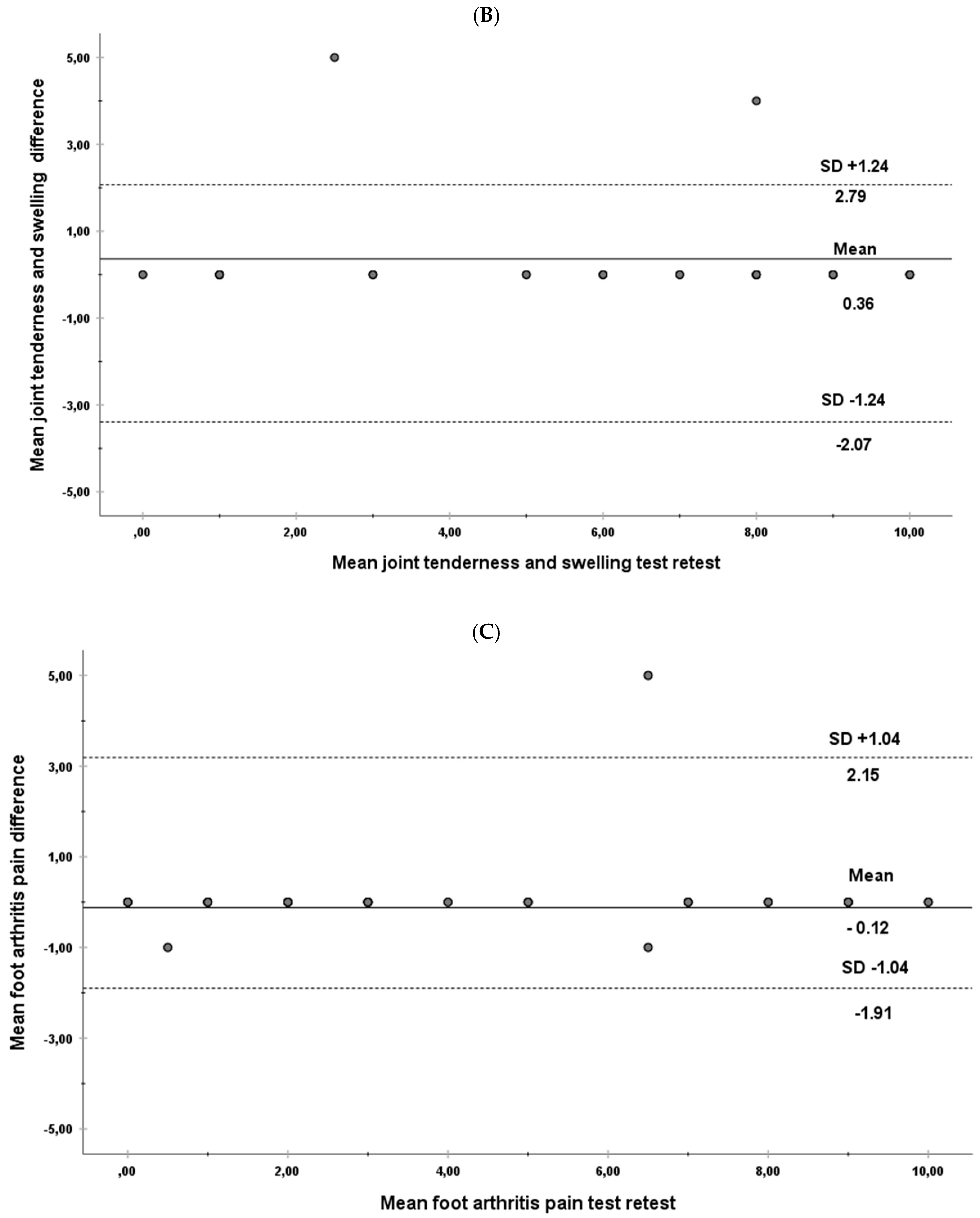
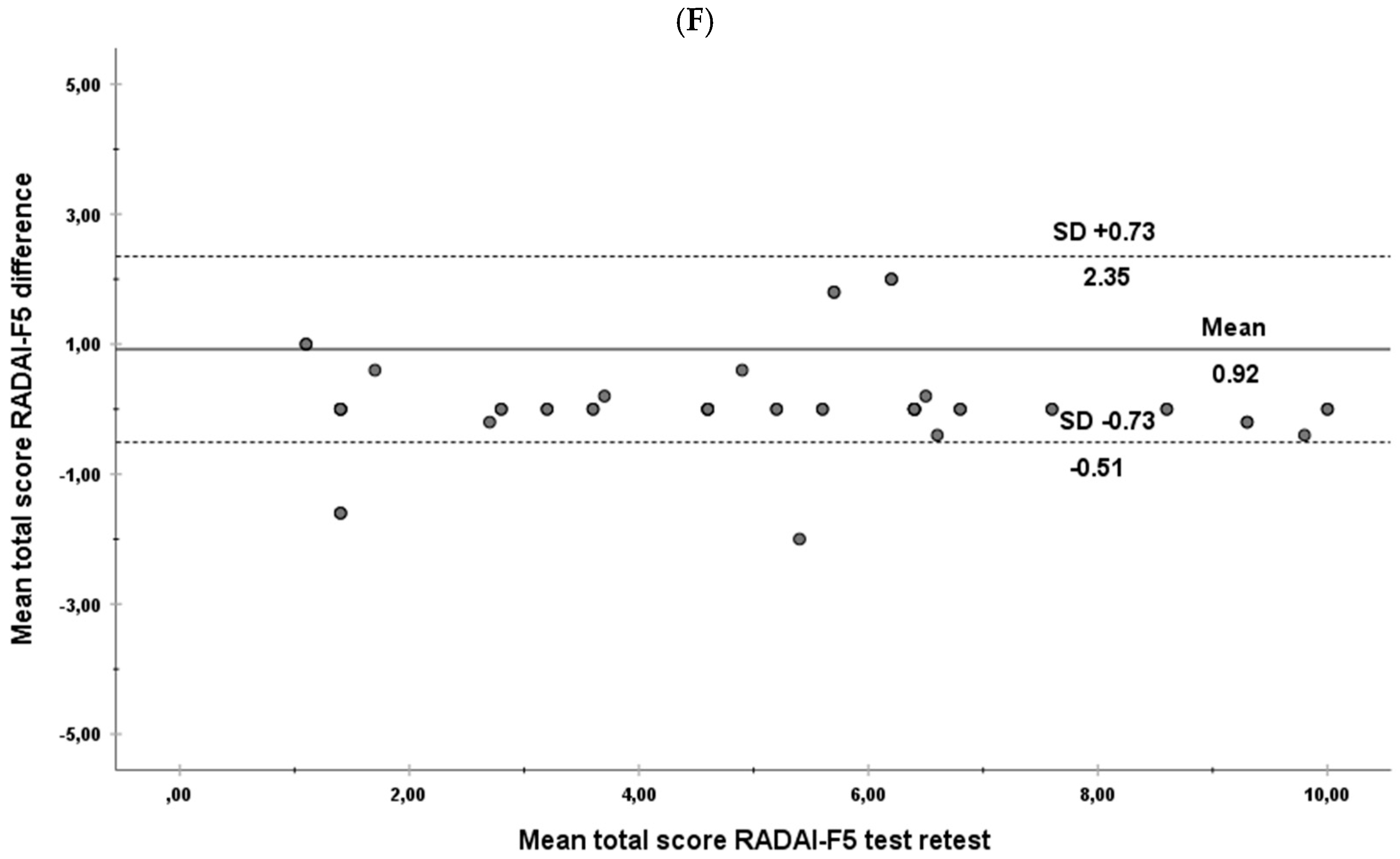
3.2. Test-Retest Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Otter, S.J.; Lucas, K.; Springett, K.; Moore, A.; Davies, K.; Cheek, L.; Young, A.; Walker-Bone, K. Foot pain in rheumatoid arthritis prevalence, risk factors and management: An epidemiological study. Clin. Rheumatol. 2009, 29, 255–271. [Google Scholar] [CrossRef]
- Stolt, M.; Suhonen, R.; Leino-Kilpi, H. Foot health in patients with rheumatoid arthritis—A scoping review. Rheumatol. Int. 2017, 37, 1413–1422. [Google Scholar] [CrossRef]
- Hoque, A.; Gallagher, K.; McEntegart, A.; Porter, D.; Steultjens, M.; Woodburn, J.; Hendry, G.J. Measuring Inflammatory Foot Disease in Rheumatoid Arthritis: Development and Validation of the Rheumatoid Arthritis Foot Disease Activity Index–5. Arthritis Rheum. 2021, 73, 1290–1299. [Google Scholar] [CrossRef] [PubMed]
- Reina-Bueno, M.; Vázquez-Bautista, M.D.C.; Pérez-García, S.; Rosende-Bautista, C.; Sáez-Díaz, A.; Munuera-Martínez, P.V. Effectiveness of custom-made foot orthoses in patients with rheumatoid arthritis: A randomized controlled trial. Clin. Rehabil. 2019, 33, 661–669. [Google Scholar] [CrossRef]
- Reina-Bueno, M.; Munuera-Martínez, P.V.; Pérez-García, S.; Vázquez-Bautista, M.D.C.; Domínguez-Maldonado, G.; Palomo-Toucedo, I.C. Foot Pain and Morphofunctional Foot Disorders in Patients with Rheumatoid Arthritis: A Multicenter Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5042. [Google Scholar] [CrossRef] [PubMed]
- Combe, B.; Landewe, R.; Lukas, C.; Bolosiu, H.D.; Breedveld, F.; Dougados, M.; Emery, P.; Ferraccioli, G.; Hazes, J.M.W.; Klareskog, L.; et al. EULAR recommendations for the management of early arthritis: Report of a task force of the European Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann. Rheum. Dis. 2006, 66, 34–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodkinson, B.; Van Duuren, E.; Pettipher, C.; Kalla, A. South African recommendations for the management of rheumatoid arthritis: An algorithm for the standard of care in 2013. S. Afr. Med. J. 2013, 103, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Walsh, D.A.; Kelly, C.; Bosworth, A.; Price, C.; Burbage, G. Provisional guidelines for applying the Department of Health (England) 18-week-patient pathway to specialist rheumatology care. Rheumatology 2007, 46, 1200–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newsome, G. Guidelines for the Management of Rheumatoid Arthritis 2002 Update. J. Am. Acad. Nurse Pract. 2002, 14, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Mota, L.M.H.D.; Cruz, B.A.; Brenol, C.V.; Pereira, I.A.; Rezende-Fronza, L.S.; Bertolo, M.B.; Freitas, M.V.C.; Silva, N.A.D.; Louzada-Junior, P.; Giorgio, R.D.N.; et al. Diretrizes para o tratamento da artrite reumatoide guidelines for the drug treatment of rheumatoid arthritis. Rev. Bras. Reumatol. 2013, 53, 158–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koike, R.; Takeuchi, T.; Eguchi, K.; Miyasaka, N. Update on the Japanese guidelines for the use of infliximab and etanercept in rheumatoid arthritis. Mod. Rheumatol. 2007, 17, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Leeden, M.V.D.; Steultjens, M.P.; Ursum, J.; Dahmen, R.; Roorda, L.D.; Schaardenburg, D.V.; Dekker, J. Prevalence and course of forefoot impairments and walking disability in the first eight years of rheumatoid arthritis. Arthritis Care Res. 2008, 59, 1596–1602. [Google Scholar] [CrossRef] [PubMed]
- Wickman, A.M.; Pinzur, M.S.; Kadanoff, R.; Juknelis, D. Health-Related Quality of Life for Patients with Rheumatoid Arthritis Foot Involvement. Foot Ankle Int. 2004, 25, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Reeve, B.B.; Wyrwich, K.W.; Wu, A.W.; Velikova, G.; Terwee, C.B.; Snyder, C.F.; Schwartz, C.; Revicki, D.A.; Moinpour, C.M.; McLeod, L.; et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual. Life Res. 2013, 22, 1889–1905. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.; Knol, D.L.; Bouter, L.M.; De Vet, H.C.W. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [Green Version]
- Fransen, J.; Langenegger, T.; Michel, B.A.; Stucki, G.; the members of the Swiss Clinical Quality Management in Rheumatoid Arthritis. Feasibility and validity of the RADAI, a self-administered rheumatoid arthritis disease activity index. Rheumatology 2000, 39, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro-Flores, E.; Losa-Iglesias, M.E.; Becerro-De-Bengoa-Vallejo, R.; López-López, D.; Rodríguez-Sanz, D.; Palomo-López, P.; Calvo-Lobo, C. Translation and Test–Retest of the Spanish Podiatry Health Questionnaire (PHQ-S). Int. J. Environ. Res. Public Health 2018, 15, 2205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorgensen, J.E.; Andreasen, J.; Rathleff, M.S. Translation and validation of the Danish Foot Function Index (FFI-DK). Scand. J. Med. Sci. Sports 2014, 25, e408–e413. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, M.J.; Poniachik, R.; Nuñez, A.; Escudero, M.I.; Carcuro, G.; Cortes, A.A. Cross-cultural adaptation and validation of the Foot and Ankle Outcome Score (FAOS) into Spanish (Chile). Foot Ankle Surg. 2020, 26, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Rintelen, B.; Haindl, P.M.; Sautner, J.; Leeb, B.A.; Deutsch, C.; Leeb, B.F. The Rheumatoid Arthritis Disease Activity Index-5 in Daily Use. Proposal for Disease Activity Categories. J. Rheumatol. 2009, 36, 918–924. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gijon-Nogueron, G.; Ndosi, M.; Luque-Suarez, A.; Alcacer-Pitarch, B.; Munuera-Martínez, P.V.; Garrow, A.; Redmond, A.C. Cross-cultural adaptation and validation of the Manchester Foot Pain and Disability Index into Spanish. Qual. Life Res. 2014, 23, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Scott, N.W.; Fayers, P.M.; Aaronson, N.K.; Bottomley, A.; De Graeff, A.; Groenvold, M.; Gundy, C.; Koller, M.; Petersen, M.A.; Sprangers, M.A.G. The practical impact of differential item functioning analyses in a health-related quality of life instrument. Qual. Life Res. 2009, 18, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Tennant, A.; Penta, M.; Tesio, L.; Grimby, G.; Thonnard, J.-L.; Slade, A.; Lawton, G.; Simone, A.; Carter, J.; Lundgren-Nilsson, Å.; et al. Assessing and Adjusting for Cross-Cultural Validity of Impairment and Activity Limitation Scales Through Differential Item Functioning within the Framework of the Rasch Model. Med. Care 2004, 42, 37–48. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Macran, S.; Kind, P.; Collingwood, J.; Hull, R.; McDonald, I.; Parkinson, L. Evaluating podiatry services: Testing a treatment specific measure of health status. Qual. Life Res. 2003, 12, 177–188. [Google Scholar] [CrossRef]
- Riskowski, J.L.; Hagedorn, T.J.; Hannan, M.T. Measures of foot function, foot health, and foot pain: American Academy of Orthopedic Surgeons Lower Limb Outcomes Assessment: Foot and Ankle Module (AAOS-FAM), Bristol Foot Score (BFS), Revised Foot Function Index (FFI-R), Foot Health Status Questionnair. Arthritis Rheum. 2011, 63, S229–S239. [Google Scholar] [CrossRef]
- Domínguez-Muñoz, F.J.; Garcia-Gordillo, M.A.; Diaz-Torres, R.A.; Hernandez-Mocholi, M.; Villafaina, S.; Collado-Mateo, D.; Jiménez-Fernández, C.; Igual-Fraile, D.; Pérez-Escanilla, F.; Martín-Gómez, G.; et al. Foot Health Status Questionnaire (FHSQ) in Spanish People with Type 2 Diabetes Mellitus: Preliminary Values Study. Int. J. Environ. Res. Public Health 2020, 17, 3643. [Google Scholar] [CrossRef]
- Sirera-Vercher, M.; Sáez-Zamora, P.; Sanz-Amaro, M. Traducción y adaptación transcultural al castellano y al valenciano del Foot Health Status Questionnaire. Rev. Esp. Cir. Ortop. Traumatol. 2010, 54, 211–219. [Google Scholar] [CrossRef]
- Paez-Moguer, J.; Budiman-Mak, E.; Cuesta-Vargas, A.I. Cross-cultural adaptation and validation of the Foot Function Index to Spanish. Foot Ankle Surg. 2014, 20, 34–39. [Google Scholar] [CrossRef]
- Reinoso-Cobo, A.; Gijon-Nogueron, G.; Caliz-Caliz, R.; Ferrer-Gonzalez, M.A.; Vallejo-Velazquez, M.T.; Morales-Asencio, J.M.; Ortega-Avila, A.B. Foot health and quality of life in patients with rheumatoid arthritis: A cross-sectional study. BMJ Open 2020, 10, e036903. [Google Scholar] [CrossRef] [PubMed]
- Matcham, F.; Scott, I.; Rayner, L.; Hotopf, M.; Kingsley, G.H.; Norton, S.; Scott, D.L.; Steer, S. The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2014, 44, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaronson, N.K.; Muller, M.; Cohen, P.D.; Essink-Bot, M.-L.; Fekkes, M.; Sanderman, R.; Sprangers, M.A.; Velde, A.t.; Verrips, E. Translation, Validation, and Norming of the Dutch Language Version of the SF-36 Health Survey in Community and Chronic Disease Populations. J. Clin. Epidemiol. 1998, 51, 1055–1068. [Google Scholar] [CrossRef]
- Linde, L.; Sørensen, J.; Ostergaard, M.; Hørslev-Petersen, K.; Hetland, M.L. Health-related quality of life: Validity, reliability, and responsiveness of SF-36, 15D, EQ-5D, RAQoL, and HAQ in patients with rheumatoid arthritis. J. Rheumatol. 2008, 35, 1528–1537. [Google Scholar]
- Mbada, C.E.; Adeogun, G.A.; Ogunlana, M.; Adedoyin, R.A.; Akinsulore, A.; Awotidebe, T.O.; Idowu, O.A.; Olaoye, O.A. Translation, cross-cultural adaptation and psychometric evaluation of yoruba version of the short-form 36 health survey. Health Qual. Life Outcomes 2015, 13, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pappa, E.; Kontodimopoulos, N.; Niakas, D. Validating and norming of the Greek SF-36 Health Survey. Qual. Life Res. 2005, 14, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Hurst, N.P.; Ruta, D.A.; Kind, P. Comparison of the MOS short form-12 (SF12) health status questionnaire with the SF36 in patients with rheumatoid arthritis. Br. J. Rheumatol. 1998, 37, 862–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dritsaki, M.; Petrou, S.; Williams, M.; Lamb, S.E. An empirical evaluation of the SF-12, SF-6D, EQ-5D and Michigan Hand Outcome Questionnaire in patients with rheumatoid arthritis of the hand. Health Qual. Life Outcomes 2017, 15, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Duong, T.V.; Aringazina, A.; Kayupova, G.; Pham, T.V.; Pham, K.M.; Truong, T.Q.; Nguyen, K.T.; Oo, W.M.; Su, T.T.; Majid, H.A. Development and Validation of a New Short-Form Health Literacy Instrument (HLS-SF12) for the General Public in Six Asian Countries. HLRP Health Lit. Res. Pract. 2019, 3, e91–e102. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Flores, E.; Romero-Morales, C.; De Bengoa-Vallejo, R.B.; Rodríguez-Sanz, D.; Palomo-López, P.; López-López, D.; Losa-Iglesias, M.E.; Calvo-Lobo, C. Sex Differences in Frail Older Adults with Foot Pain in a Spanish Population: An Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 6141. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Flores, E.; Vallejo, R.B.D.B.; Losa-Iglesias, M.E.; Palomo-López, P.; Calvo-Lobo, C.; López-López, D.; Martínez-Jiménez, E.M.; Romero-Morales, C. The reliability, validity, and sensitivity of the Edmonton Frail Scale (EFS) in older adults with foot disorders. Aging 2020, 12, 24623–24632. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Group n 50 Mean ± SD Range N = 79 | Men n 27 Mean ± SD Range N = 24 | Women n 23 Mean ± SD Range N = 55 | p Value | |
|---|---|---|---|---|
| Age, years | 69.220 ± 17.136 (64.349–74.090) | 64.037 ± 18.107 (56.873–72.200) | 42.018 ± 13.959 (69.267–81.340) | 0.029 |
| Weight (kg) | 66.400 ± 15.877 (61.887–70.912) | 67.537 ± 16.053 (61.186–73.887) | 65.065 ± 15.920 (58.180–71.949) | 0.533 |
| Height (cm) | 1.633 ± 0.088 (1.607–1.658) | 1.671 ± 0.066 (1.645–1.697) | 1.587 ± 0.091 (1.548–1.627) | 0.002 |
| BMI (kg/m2) | 24.854 ± 5.541 (23.221–24.428) | 24.074 ± 5.205 (22.014–26.133) | 25.769 ± 5.894 (23.221–28.318) | 0.316 |
| Test (N = 50) | Retest (N = 50) | Correlation Test-Retest | Reliability Test-Retest | Systematic Differences Test-Retest | |||||
|---|---|---|---|---|---|---|---|---|---|
| DOMAIN | Mean ± SD (95% CI) | Item–Total Correlation r (p) * | Alpha If Item Removed | Mean ± SD (95% CI) | Item–Total Correlation r (p) * | Alpha If Item Removed | Item–Total Correlation r (p) * | Alpha If Item Removed | Mean ± SD (95% CI) |
| Arthritis activity in foot | 5.540 ± 3.252 (4.61–6.46) | 0.865 (<0.01) | 0.896 | 5.64–3.30 (4.70–6.57) | 0.839 (<0.01) | 0.885 | 0.858 (<0.01) | 0.953 (0.876–0.960) | 0.812 |
| Joint tenderness and swelling | 6.080 ± 3.306 (5.14–7.019) | 0.898 (<0.01) | 0.894 | 5.72 ± 3.41 (4.75–6.68) | 0.862 (<0.01) | 0.883 | 0.914 (<0.01) | 0.952 (0.938–0.970) | 0.063 |
| Foot arthritis pain | 4.60 ± 3.41 (3.63–5.56) | 0.965 (<0.01) | 0.879 | 4.48 ± 3.26 (3.55–5.40) | 0.932 (<0.01) | 0.878 | 0.965 (<0.01) | 0.951 (0.948–0.969) | 0.914 |
| General foot health | 6.08 ± 2.85 (5.26–6.89) | 0.763 (<0.01) | 0.910 | 6.04 ± 2.59 (5.30–6.77) | 0.671 (<0.01) | 0.915 | 0.865 (<0.01) | 0.959 (0.884–0.961) | 0.916 |
| Joint stiffness on awakening sub-scales | 3.72 ± 3.103 (2.83–4.60) | 0.446 (<0.01) | 0.946 | 3.68 ± 3.22 (2.76–4.59) | 0.427 (<0.01) | 0.948 | 0.935 (<0.01) | 0.965 (0.948–0.970) | 0.557 |
| Total | 5.20 ± 2.60 (4.46–5.94) | N/A | 0.875 | 5.11 ± 2.57 (4.37–5.84) | N/A | 0.871 | 0.933 (<0.01) | 0.951 (0.944–0.988) | 0.347 |
| Total Cronbach alpha test: 0.914 | Total Cronbach alpha retest: 0.918 | ||||||||
| Test (N = 50) | Retest (N = 50) | Correlation Test-Retest | Reliability Test-Retest | Systematic Differences Test-Retest | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Corrected Item-Total Correlation | Cronbach’s Alpha if Item Deleted | r (p) * | ICC (IC95%) | r (p) * | ||||||
| Item | Mean ± SD (95% CI) | Corrected Item-Total Correlation | Cronbach’s Alpha if Item Deleted | Mean ± SD (95% CI) | Corrected Item-Total Correlation | Cronbach’s Alpha if Item Deleted | r (p) * | ICC (IC95%) | r (p) * | 0.812 |
| Item 1: THINKING ONLY OF YOUR FEET How active was your arthritis IN YOUR FEET over the last 6 months? | 5.54 ± 3.25 (4.61–6.46) | 0.865 (<0.01) | 0.896 | 5.64–3.30 (4.70–6.57) | 0.839 (<0.01) | 0.885 | 0.858 (<0.01) | 0.953 (0.876– 0.960) | 0.812 | 0.063 |
| Item 2: THINKING ONLY OF YOUR FEET How active is your FOOT arthritis today with respect to joint tenderness and swelling? | 6.08 ± 3.30 (5.14–7.01) | 0.898 (<0.01) | 0.894 | 5.72 ± 3.41 (4.75–6.68) | 0.862 (<0.01) | 0.883 | 0.914 (<0.01) | 0.952 (0.938–0.970) | 0.063 | 0.914 |
| Item 3: THINKING ONLY OF YOUR FEET How severe is your arthritis pain IN YOUR FEET today? | 4.60 ± 3.41 (3.63–5.56) | 0.965 (<0.01) | 0.879 | 4.48 ± 3.26 (3.55–5.40) | 0.932 (<0.01) | 0.878 | 0.965 (<0.01) | 0.951 (0.948–0.969) | 0.914 | 0.916 |
| Item 4: THINKING ONLY OF YOUR FEET How would you describe your general FOOT health today? | 6.08 ± 2.85 (5.26–6.89) | 0.763(<0.01) | 0.910 | 6.04 ± 2.59 (5.30–6.77) | 0.671 (<0.01) | 0.915 | 0.865 (<0.01) | 0.959 (0.884–0.961) | 0.916 | 0.557 |
| Item 5: THINKING ONLY OF YOUR FEET Did you experience foot joint stiffness on awakening yesterday morning? If yes, how long was this stiffness IN YOUR FEET? | 3.72 ± 3.10 (2.83–4.60) | 0.446 (<0.01) | 0.946 | 3.68 ± 3.22 (2.76–4.59) | 0.427 (<0.01) | 0.948 | 0.935 (<0.01) | 0.965 (0.948–0.970) | 0.557 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Jiménez, E.M.; Pereiro-Buceta, H.; Palomo-López, P.; Navarro-Flores, E.; Jiménez-Cebrián, A.M.; Losa-Iglesias, M.E.; Becerro-De-Bengoa-Vallejo, R.; López-López, D. Repeatability and Reliability of the Rheumatoid Arthritis Foot Disease Activity Index in Spanish Patients: A Transcultural Adaptation. Biology 2022, 11, 30. https://doi.org/10.3390/biology11010030
Martínez-Jiménez EM, Pereiro-Buceta H, Palomo-López P, Navarro-Flores E, Jiménez-Cebrián AM, Losa-Iglesias ME, Becerro-De-Bengoa-Vallejo R, López-López D. Repeatability and Reliability of the Rheumatoid Arthritis Foot Disease Activity Index in Spanish Patients: A Transcultural Adaptation. Biology. 2022; 11(1):30. https://doi.org/10.3390/biology11010030
Chicago/Turabian StyleMartínez-Jiménez, Eva María, Héctor Pereiro-Buceta, Patricia Palomo-López, Emmanuel Navarro-Flores, Ana María Jiménez-Cebrián, Marta Elena Losa-Iglesias, Ricardo Becerro-De-Bengoa-Vallejo, and Daniel López-López. 2022. "Repeatability and Reliability of the Rheumatoid Arthritis Foot Disease Activity Index in Spanish Patients: A Transcultural Adaptation" Biology 11, no. 1: 30. https://doi.org/10.3390/biology11010030
APA StyleMartínez-Jiménez, E. M., Pereiro-Buceta, H., Palomo-López, P., Navarro-Flores, E., Jiménez-Cebrián, A. M., Losa-Iglesias, M. E., Becerro-De-Bengoa-Vallejo, R., & López-López, D. (2022). Repeatability and Reliability of the Rheumatoid Arthritis Foot Disease Activity Index in Spanish Patients: A Transcultural Adaptation. Biology, 11(1), 30. https://doi.org/10.3390/biology11010030