
Transvenous Lead Extraction in Patients with Cardiac Implantable Device: The Impact of Systemic and Local Infection on Clinical Outcomes—An ESC-EHRA ELECTRa (European Lead Extraction Controlled) Registry Substudy

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. The ELECTRa Registry
2.2. Sub-Study Characteristics: Patient Selection, Endpoints
2.3. Statistical Analysis
3. Results
3.1. Patient Population and Baseline Clinical Characteristics
3.2. CIED History and Characteristics
3.3. History of Infection and Investigations
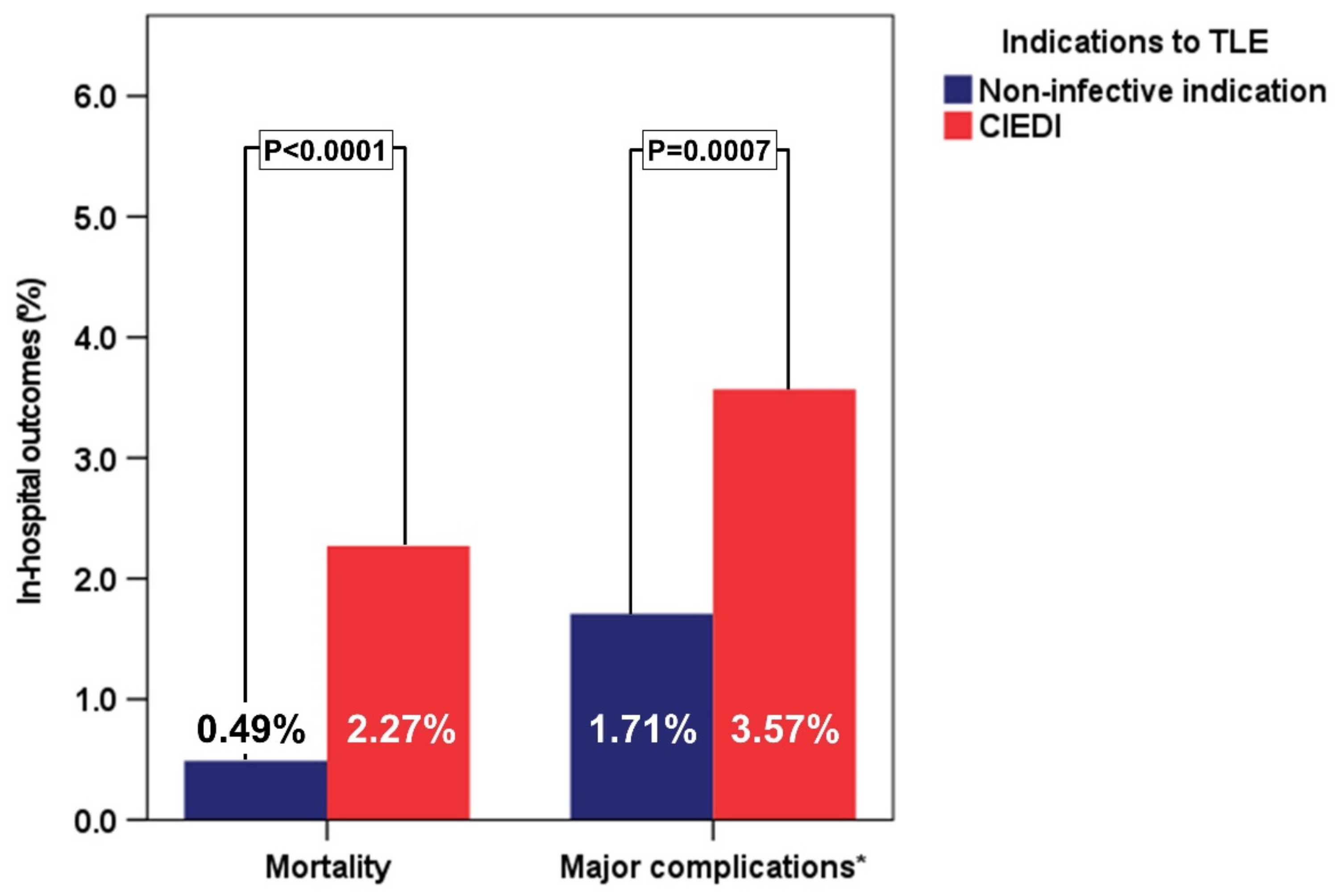
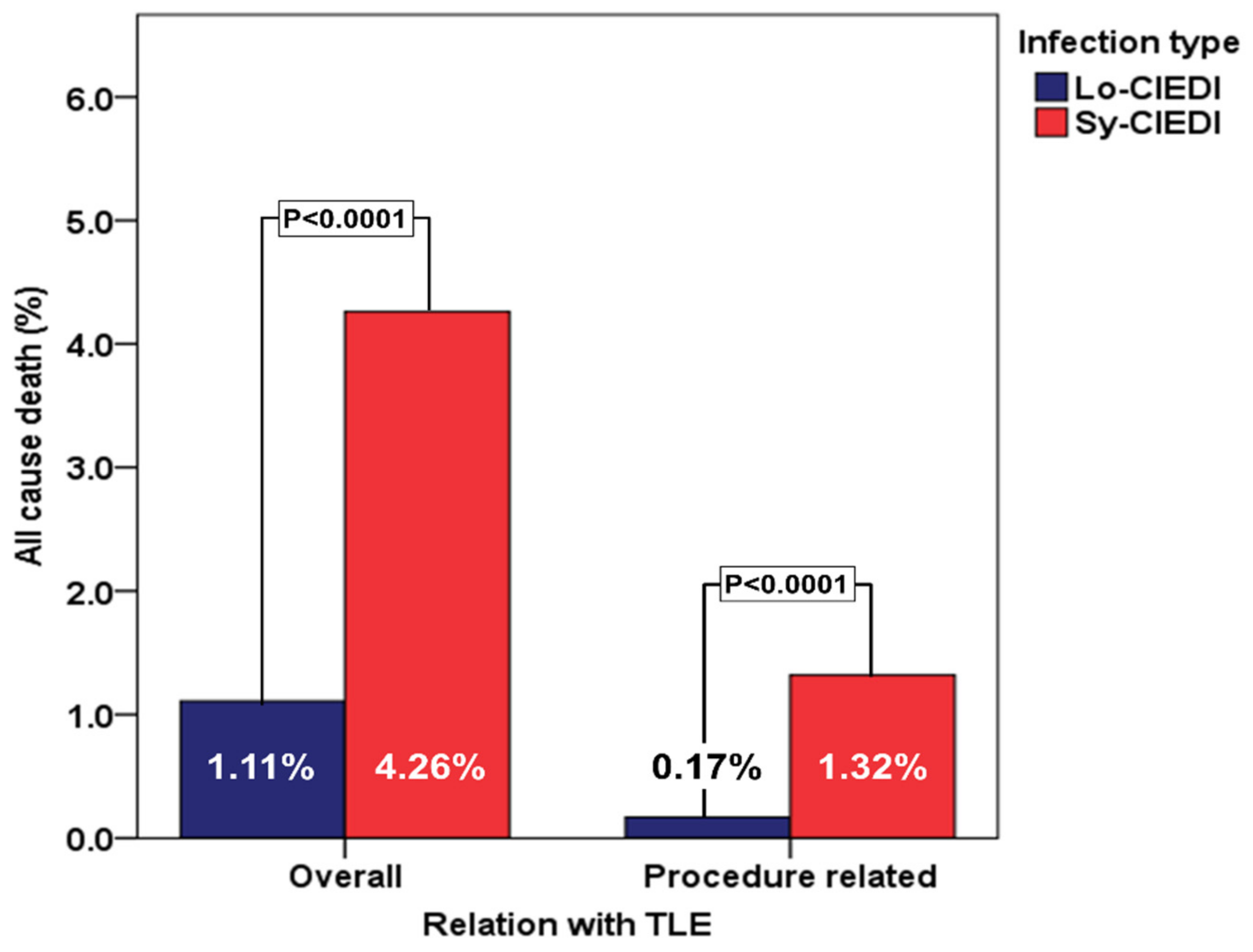
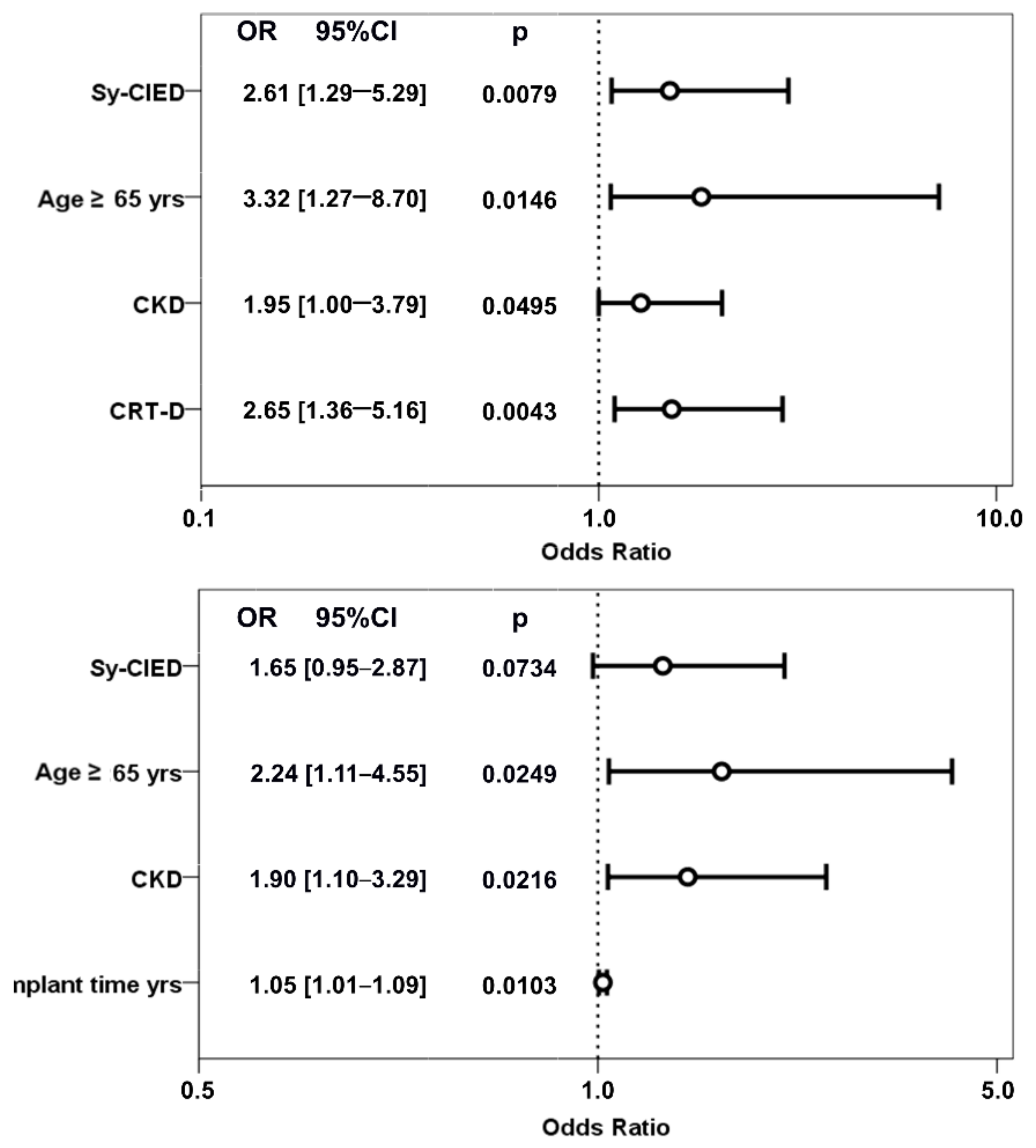
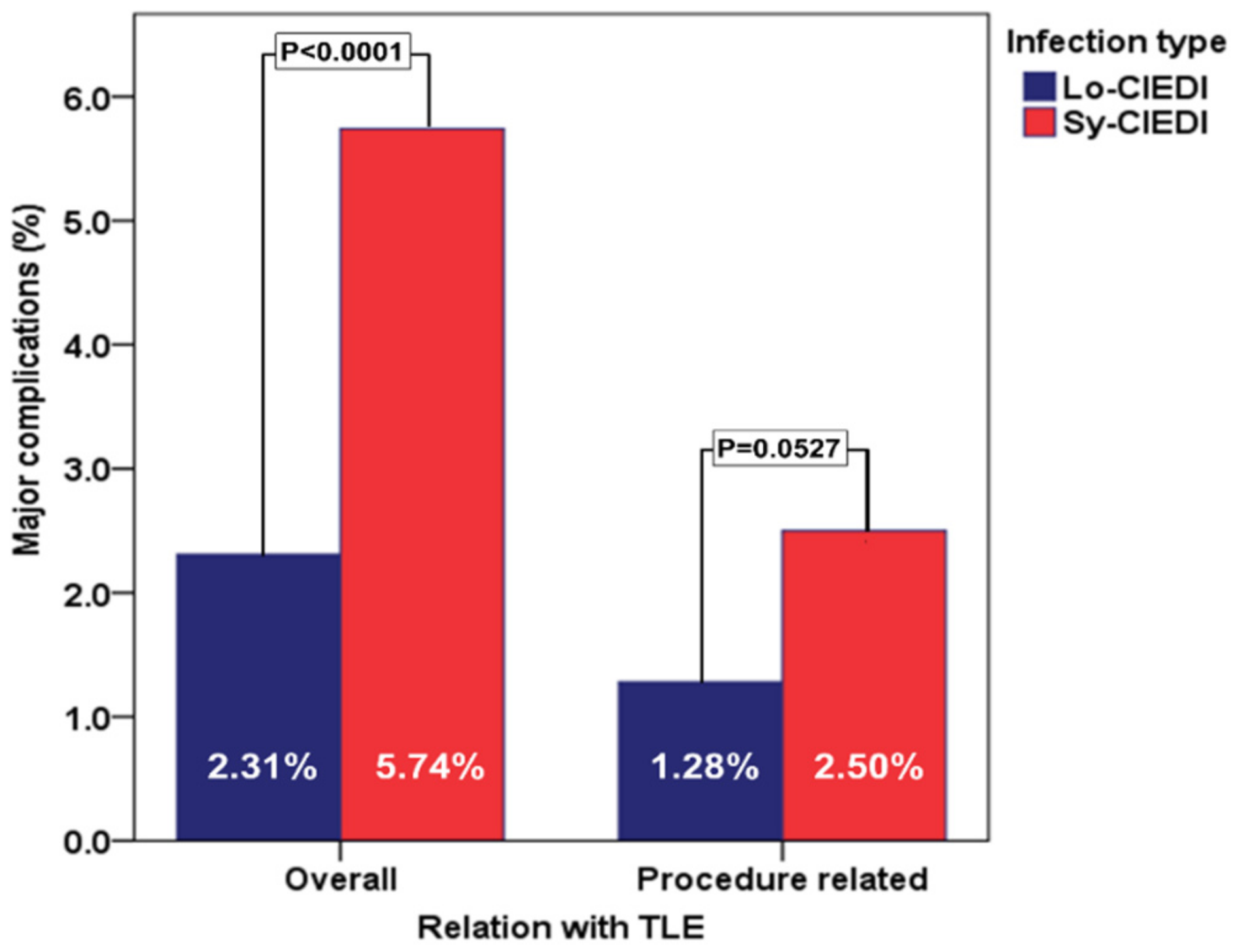
3.4. In-Hospital Mortality and Major Complications
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Banks, H.; Torbica, A.; Valzania, C.; Varabyova, Y.; Prevolnik Rupel, V.; Taylor, R.S.; Hunger, T.; Walker, S.; Boriani, G.; Fattore, G.; et al. Five year trends (2008–2012) in cardiac implantable electrical device utilization in five European nations: A case study in cross-country comparisons using administrative databases. Europace 2018, 20, 643–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boriani, G.; Elsner, C.; Diemberger, I. The struggle against infections of cardiac implantable electrical devices: The burden of costs requires new personalized solutions. Europace 2018, 20, 1877–1879. [Google Scholar] [CrossRef] [PubMed]
- Bongiorni, M.G.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarski, A.; Rinaldi, C.A.; Romano, S.L.; Maggioni, A.P.; Andarala, M.; Auricchio, A.; et al. The European Lead Extraction ConTRolled (ELECTRa) study: A European Heart Rhythm Association (EHRA) Registry of Transvenous Lead Extraction Outcomes. Eur. Heart J. 2017, 38, 2995–3005. [Google Scholar] [CrossRef] [PubMed]
- Diemberger, I.; Migliore, F.; Biffi, M.; Cipriani, A.; Bertaglia, E.; Lorenzetti, S.; Massaro, G.; Tanzarella, G.; Boriani, G. The “Subtle” connection between development of cardiac implantable electrical device infection and survival after complete system removal: An observational prospective multicenter study. Int. J. Cardiol. 2018, 250, 146–149. [Google Scholar] [CrossRef]
- Bongiorni, M.G.; Romano, S.L.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarsky, A.; Rinaldi, C.A.; Maggioni, A.P.; Blomstrom-Lundqvist, C.; Auricchio, A. ELECTRa (European Lead Extraction ConTRolled) Registry–shedding light on transvenous lead extraction real-world practice in Europe. Herzschrittmacherther. Elektrophysiol. 2013, 24, 171–175. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef]
- Kusumoto, F.M.; Schoenfeld, M.H.; Wilkoff, B.L.; Berul, C.I.; Birgersdotter-Green, U.M.; Carrillo, R.; Cha, Y.M.; Clancy, J.; Deharo, J.C.; Ellenbogen, K.A.; et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm 2017, 14, e503–e551. [Google Scholar] [CrossRef] [Green Version]
- Sandoe, J.A.; Barlow, G.; Chambers, J.B.; Gammage, M.; Guleri, A.; Howard, P.; Olson, E.; Perry, J.D.; Prendergast, B.D.; Spry, M.J.; et al. Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Report of a joint Working Party project on behalf of the British Society for Antimicrobial Chemotherapy (BSAC, host organization), British Heart Rhythm Society (BHRS), British Cardiovascular Society (BCS), British Heart Valve Society (BHVS) and British Society for Echocardiography (BSE). J. Antimicrob. Chemother. 2015, 70, 325–359. [Google Scholar] [CrossRef]
- Diemberger, I.; Biffi, M.; Lorenzetti, S.; Martignani, C.; Raffaelli, E.; Ziacchi, M.; Rapezzi, C.; Pacini, D.; Boriani, G. Predictors of long-term survival free from relapses after extraction of infected CIED. Europace 2018, 20, 1018–1027. [Google Scholar] [CrossRef]
- Polewczyk, A.; Jachec, W.; Polewczyk, A.M.; Tomasik, A.; Janion, M.; Kutarski, A. Infectious complications in patients with cardiac implantable electronic devices: Risk factors, prevention, and prognosis. Pol. Arch. Intern. Med. 2017, 127, 597–607. [Google Scholar] [CrossRef] [Green Version]
- Diemberger, I.; Mazzotti, A.; Giulia, M.B.; Cristian, M.; Matteo, M.; Letizia, Z.M.; Reggiani, B.; Battistini, P.; Boriani, G. From lead management to implanted patient management: Systematic review and meta-analysis of the last 15 years of experience in lead extraction. Expert Rev. Med. Devices 2013, 10, 551–573. [Google Scholar] [CrossRef] [PubMed]
- Younis, A.; Beinart, R.; Nehoray, N.; Asher, E.; Matetzky, S.; Beigel, R.; Wieder, A.; Glikson, M.; Nof, E. Characterization of a previously unrecognized clinical phenomenon: Delayed shock after cardiac implantable electronic device extraction. Heart Rhythm 2017, 14, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Regoli, F.; Bongiorni, M.G.; Rordorf, R.; Santamaria, M.; Klersy, C.; Segreti, L.; De Regibus, V.; Moccetti, T.; Conte, G.; Caputo, M.L.; et al. High recurrence of device-related adverse events following transvenous lead extraction procedure in patients with cardiac resynchronization devices. Eur. J. Heart Fail. 2016, 18, 1270–1277. [Google Scholar] [CrossRef] [PubMed]
- Butter, C.; Tosetti, A. Re-Implantation Strategy After Lead Extraction for Cardiac Device Infection. In Infections of Cardiac Implantable Devices: A Comprehensive Guide; Diemberger, I., Boriani, G., Eds.; Springer: Cham, Switzerland, 2020; pp. 109–126. [Google Scholar]
- Viani, S.; Migliore, F.; Tola, G.; Pisano, E.C.L.; Russo, A.D.; Luzzi, G.; Sartori, P.; Piro, A.; Rordorf, R.; Forleo, G.B.; et al. Use and outcomes of subcutaneous implantable cardioverter-defibrillator (ICD) after transvenous ICD extraction: An analysis of current clinical practice and a comparison with transvenous ICD reimplantation. Heart Rhythm 2019, 16, 564–571. [Google Scholar] [CrossRef]
- Deharo, J.C.; Martignani, C. Prevention of Device Infection: New Implantable Devices In Infections of Cardiac Implantable Devices: A Comprehensive Guide; Diemberger, I., Boriani, G., Eds.; Springer: Cham, Switzerland, 2020; pp. 153–176. [Google Scholar]
- Olmos, C.; Vilacosta, I.; Fernandez, C.; Lopez, J.; Sarria, C.; Ferrera, C.; Revilla, A.; Silva, J.; Vivas, D.; Gonzalez, I.; et al. Contemporary epidemiology and prognosis of septic shock in infective endocarditis. Eur. Heart J. 2013, 34, 1999–2006. [Google Scholar] [CrossRef]
- Polewczyk, A.; Jachec, W.; Tomaszewski, A.; Brzozowski, W.; Czajkowski, M.; Polewczyk, A.M.; Janion, M.; Kutarski, A. Lead-related infective endocarditis: Factors influencing the formation of large vegetations. Europace 2017, 19, 1022–1030. [Google Scholar] [CrossRef]
- Greenspon, A.J.; Prutkin, J.M.; Sohail, M.R.; Vikram, H.R.; Baddour, L.M.; Danik, S.B.; Peacock, J.; Falces, C.; Miro, J.M.; Blank, E.; et al. Timing of the most recent device procedure influences the clinical outcome of lead-associated endocarditis results of the MEDIC (Multicenter Electrophysiologic Device Infection Cohort). J. Am. Coll. Cardiol. 2012, 59, 681–687. [Google Scholar] [CrossRef] [Green Version]
- Diemberger, I.; Bonfiglioli, R.; Martignani, C.; Graziosi, M.; Biffi, M.; Lorenzetti, S.; Ziacchi, M.; Nanni, C.; Fanti, S.; Boriani, G. Contribution of PET imaging to mortality risk stratification in candidates to lead extraction for pacemaker or defibrillator infection: A prospective single center study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 194–205. [Google Scholar] [CrossRef]
- Kolodzinska, K.; Kutarski, A.; Grabowski, M.; Jarzyna, I.; Malecka, B.; Opolski, G. Abrasions of the outer silicone insulation of endocardial leads in their intracardiac part: A new mechanism of lead-dependent endocarditis. Europace 2012, 14, 903–910. [Google Scholar] [CrossRef]
- Tarakji, K.G.; Mittal, S.; Kennergren, C.; Corey, R.; Poole, J.E.; Schloss, E.; Gallastegui, J.; Pickett, R.A.; Evonich, R.; Philippon, F.; et al. Antibacterial Envelope to Prevent Cardiac Implantable Device Infection. N. Engl. J. Med. 2019, 380, 1895–1905. [Google Scholar] [CrossRef]
- Mittal, S.; Shaw, R.E.; Michel, K.; Palekar, R.; Arshad, A.; Musat, D.; Preminger, M.; Sichrovsky, T.; Steinberg, J.S. Cardiac implantable electronic device infections: Incidence, risk factors, and the effect of the AigisRx antibacterial envelope. Heart Rhythm 2014, 11, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Burri, H.; Starck, C.; Auricchio, A.; Biffi, M.; Burri, M.; D’Avila, A.; Deharo, J.C.; Glikson, M.; Israel, C.; Lau, C.P.; et al. EHRA expert consensus statement and practical guide on optimal implantation technique for conventional pacemakers and implantable cardioverter-defibrillators: Endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), and the Latin-American Heart Rhythm Society (LAHRS). Europace 2021, 23, 983–1008. [Google Scholar] [CrossRef] [PubMed]
- Biffi, M. The never-ending story of CIED infection prevention: Shall we WRAP-IT and go? J. Cardiovasc. Electrophysiol. 2019, 30, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Barletta, V.; Morolla, D.; Della Tommasina, V.; Segreti, L.; Di Cori, A.; Zucchelli, G.; Bongiorni, M.G. Cardiac Device Infections: A Lesson from the Registries. In Infections of Cardiac Implantable Devices: A Comprehensive Guide; Diemberger, I., Boriani, G., Eds.; Springer: Cham, Switzerland, 2020; pp. 47–64. [Google Scholar]
- Diemberger, I.; Lorenzetti, S.; Bonfiglioli, R. Building Up the Diagnosis of Cardiac Device Infections: The Role of Imaging. In Infections of Cardiac Implantable Devices: A Comprehensive Guide; Diemberger, I., Boriani, G., Eds.; Springer: Cham, Switzerland, 2020; pp. 65–94. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient characteristics | Lo-CIEDI (1170 pts.) | Sy-CIEDI (680 pts.) | p |
|---|---|---|---|
| General characteristics, N/Total N (%) | |||
| Male sex | 922/1170 (78.80%) | 520/680 (76.47%) | 0.2432 |
| Age ≥ 65 years | 830/1170 (70.94%) | 451/680 (66.32%) | 0.0380 |
| BMI > 25 Kg/m2 | 725/1152 (62.93%) | 375/656 (57.16%) | 0.0156 |
| Hi-vol centre | 964/1170 (82.39%) | 545/680 (80.15%) | 0.2296 |
| LVEF ≤ 35% | 323/1089 (29.66%) | 223/645 (34.57%) | 0.0332 |
| Anticoagulation pre-TLE | 428/1170 (36.58%) | 309/680 (45.44%) | 0.0001 |
| Heart disease N/Total N (%) | |||
| Coronary artery disease | 451/1160 (38.88%) | 282/670 (42.09%) | 0.1769 |
| Valvular heart disease | 179/1167 (15.34%) | 124/678 (18.29%) | 0.0990 |
| Dilated cardiomyopathy | 313/1165 (26.87%) | 184/673 (27.34%) | 0.8258 |
| Hypertrophic cardiomyopathy | 40/1168 (3.42%) | 32/678 (4.72%) | 0.1658 |
| Primary electrical disease | 362/1164 (31.10%) | 182/675 (26.96%) | 0.0610 |
| CHF | 475/1162 (40.88%) | 309/675 (45.78%) | 0.0406 |
| Comorbidities N/Total N (%) | |||
| Hypertension | 697/1162 (59.98%) | 392/673 (58.25%) | 0.4655 |
| Diabetes | 278/1162 (23.92%) | 229/674 (33.98%) | <0.0001 |
| COPD | 115/1162 (9.90%) | 76/673 (11.29%) | 0.3453 |
| Chronic kidney disease | 208/1164 (17.87%) | 209/676 (30.92%) | <0.0001 |
| CIED Characteristics | Lo-CIEDI (1170 pts.) | Sy-CIEDI (680 pts.) | p |
|---|---|---|---|
| General characteristics, N/Total N (%) | |||
| ICD | 470/1170 (40.17%) | 305/680 (44.85%) | 0.0490 |
| CRT-D | 239/1170 (20.43%) | 144/680 (21.18%) | 0.7014 |
| PM dependency | 318/1170 (27.18%) | 157/680 (23.09%) | 0.0521 |
| Patients with >2 target leads | 393/1170 (33.59%) | 212/680 (31.18%) | 0.2860 |
| CIED history, N/Total N (%) | |||
| Previous CIED complication: overall | 526/1170 (44.96%) | 207/680 (30.44%) | <0.0001 |
| Previous CIED complication: infective | 337/526 (64.07%) | 126/207 (60.87%) | 0.4189 |
| Previous CIED complication: malfunction | 192/526 (36.50%) | 85/207 (41.06%) | 0.2516 |
| Previous CIED complication: thrombotic | 9/526 (1.71%) | 6/207 (2.90%) | 0.3066 |
| Last procedure: CIED implant | 287/1170 (24.53%) | 294/680 (43.24%) | <0.0001 |
| Last procedure: CIED replacement | 208/1170 (17.77%) | 143/680 (21.03%) | 0.0855 |
| Previous CIED revision | 575/1170 (49.15%) | 191/680 (28.09%) | <0.0001 |
| Previous CIED upgrade | 175/1170 (14.96%) | 87/680 (12.79%) | 0.1982 |
| Infection Chacracteristics | Lo-CIEDI (1170 pts.) | Sy-CIEDI (680 pts.) | p |
|---|---|---|---|
| Instrumental examination, N/Total N (%) or Median [IQR] | |||
| Masses at TTE/TEE * | 121/1170 (10.34%) | 445/680 (65.44%) | <0.0001 |
| WBC count (x10e9/L) | 7.20 (5.99–8.63) (N = 1095) | 8.08 (6.30–10.60) (N = 629) | <0.0001 |
| C-reactive protein (mg/L) | 4.00 (1.40–12.00) (N = 977) | 17.00 (4.50–65.00) (N = 581) | <0.0001 |
| Blood cultures, N/Total N (%) | |||
| Positive culture ** | 328/958 (34.24%) | 544/659 (82.55%) | <0.0001 |
| Coagulase-negative Staphylococcus | 140/328 (42.68%) | 185/544 (34.01%) | 0.0102 |
| Staphylococcus Aureus | 109/328 (33.23%) | 233/544 (42.83%) | 0.0049 |
| Other agents | 99/328 (30.18%) | 161/544 (29.60%) | 0.8542 |
| Infection history and antibiotic treatment, N/Total N (%) or Median [IQR] | |||
| Time 1st sign of infection —enrolment (days) | 45.00 (17.00–115.00) (N = 1113) | 34.00 (15.00–87.00) (N = 663) | 0.0027 |
| Time from last lead implanted to 1st sign of infection (months) | 47 (14–96) (N = 1094) | 43 (13–87) (N = 649) | 0.0768 |
| Antibiotic pre-TLE | 854/1170 (72.99%) | 636/680 (93.53%) | <0.0001 |
| Empirical antibiotic treatment | 645/854 (75.53%) | 186/636 (29.25%) | <0.0001 |
| Blood Culture-guided antibiotic treatment | 81/854 (9.48%) | 430/636 (67.61%) | <0.0001 |
| Duration of pre-TLE antibiotic | 10.00 (4.00–20.00) (N = 791) | 12.00 (7.00–23.00) (N = 596) | <0.0001 |
| Covariable | Mortality | Major Complications |
|---|---|---|
| Hazard-Ratio [95% CI] | ||
| Age ≥ 65 years | 2.64 (1.17–6.00) | 2.23 (1.21–4.12) |
| LVEF ≤ 35% | 2.06 (1.12–3.81) | n.s. |
| Chronic Heart Failure | 1.98 (1.05–3.73) | n.s. |
| Chronic kidney disease | 2.94 (1.60–5.42) | 2.23 (1.36–3.65) |
| PM dependency | n.s. | 2.06 (1.26–3.36) |
| CRT-D | 2.45 (1.32–4.53) | n.s. |
| Oldest lead dwelling time (years) | n.s. | 1.06 (1.02–1.10) |
| Number of leads ≥ 3 | 2.21 (1.19–4.10) | n.s. |
| Sy-CIEDI | 2.82 (1.45–5.48) | 1.79 (1.08–2.97) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diemberger, I.; Segreti, L.; Rinaldi, C.A.; Svendsen, J.H.; Kutarski, A.; Younis, A.; Laroche, C.; Leclercq, C.; Małecka, B.; Mitkowski, P.; et al. Transvenous Lead Extraction in Patients with Cardiac Implantable Device: The Impact of Systemic and Local Infection on Clinical Outcomes—An ESC-EHRA ELECTRa (European Lead Extraction Controlled) Registry Substudy. Biology 2022, 11, 615. https://doi.org/10.3390/biology11040615
Diemberger I, Segreti L, Rinaldi CA, Svendsen JH, Kutarski A, Younis A, Laroche C, Leclercq C, Małecka B, Mitkowski P, et al. Transvenous Lead Extraction in Patients with Cardiac Implantable Device: The Impact of Systemic and Local Infection on Clinical Outcomes—An ESC-EHRA ELECTRa (European Lead Extraction Controlled) Registry Substudy. Biology. 2022; 11(4):615. https://doi.org/10.3390/biology11040615
Chicago/Turabian StyleDiemberger, Igor, Luca Segreti, Christopher A. Rinaldi, Jesper Hastrup Svendsen, Andrzej Kutarski, Arwa Younis, Cécile Laroche, Christophe Leclercq, Barbara Małecka, Przemyslaw Mitkowski, and et al. 2022. "Transvenous Lead Extraction in Patients with Cardiac Implantable Device: The Impact of Systemic and Local Infection on Clinical Outcomes—An ESC-EHRA ELECTRa (European Lead Extraction Controlled) Registry Substudy" Biology 11, no. 4: 615. https://doi.org/10.3390/biology11040615
APA StyleDiemberger, I., Segreti, L., Rinaldi, C. A., Svendsen, J. H., Kutarski, A., Younis, A., Laroche, C., Leclercq, C., Małecka, B., Mitkowski, P., Bongiorni, M. G., & On behalf of the ELECTRa Investigators. (2022). Transvenous Lead Extraction in Patients with Cardiac Implantable Device: The Impact of Systemic and Local Infection on Clinical Outcomes—An ESC-EHRA ELECTRa (European Lead Extraction Controlled) Registry Substudy. Biology, 11(4), 615. https://doi.org/10.3390/biology11040615