
Detection of Lymphatic Vessels in Dental Pulp

 ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials
- -
- Extensive destruction of the crown and caries;
- -
- Orthodontic reasons, caries-free teeth.
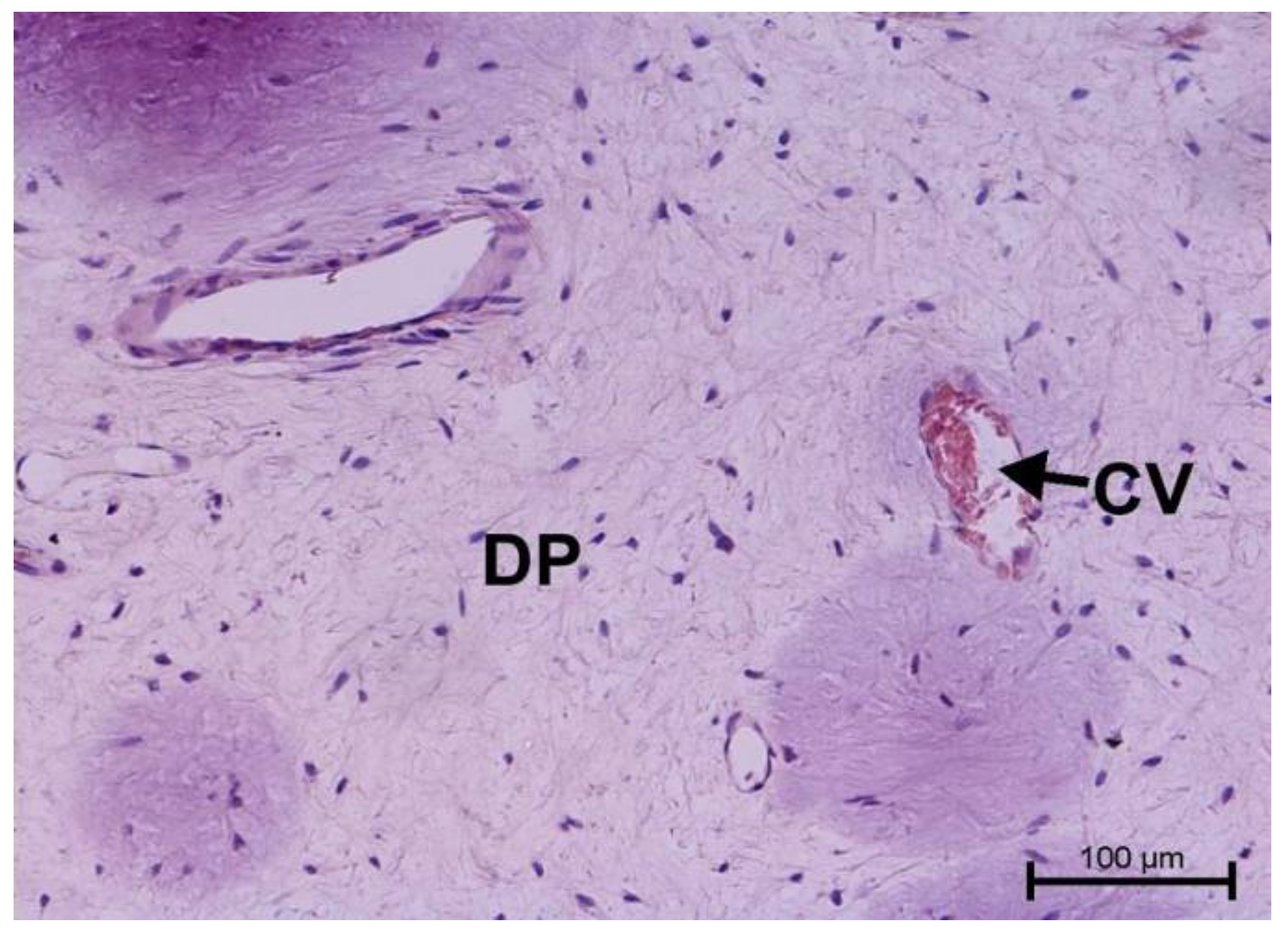
- Group I—healthy teeth.
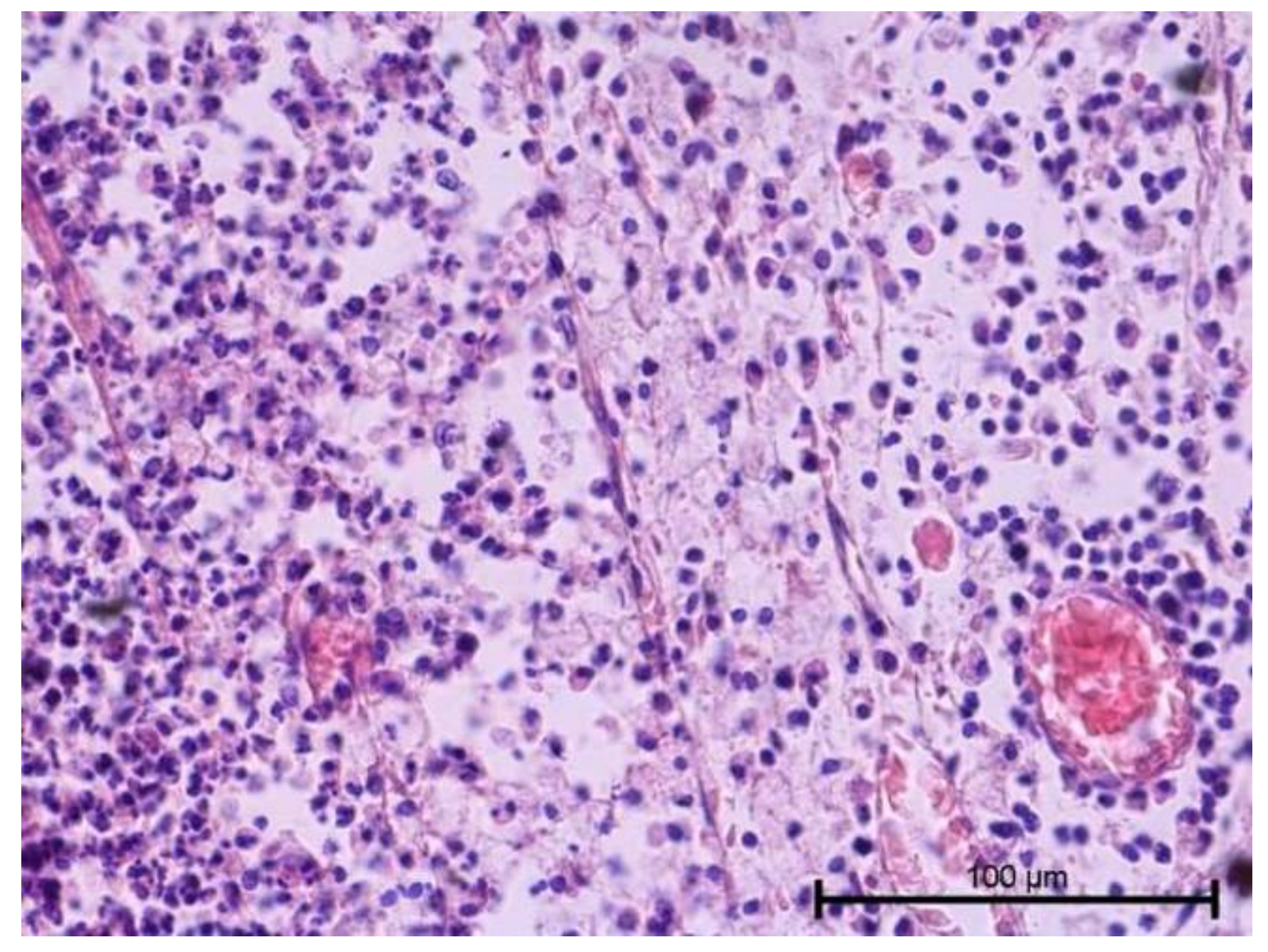
- Group II—teeth with neutrophilic infiltration.
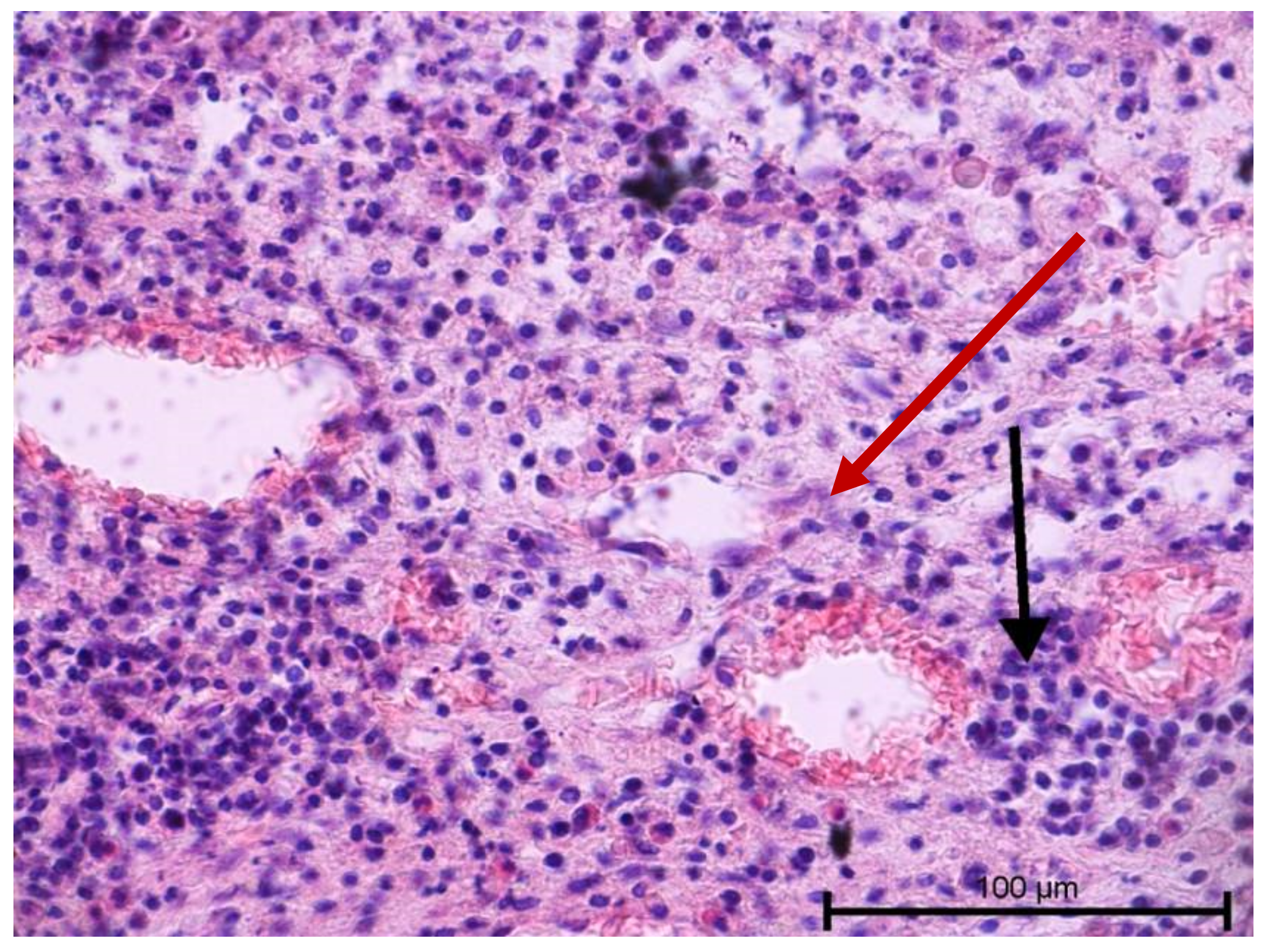
- Group III—teeth with mixed lymphocytic and neutrophilic infiltration.
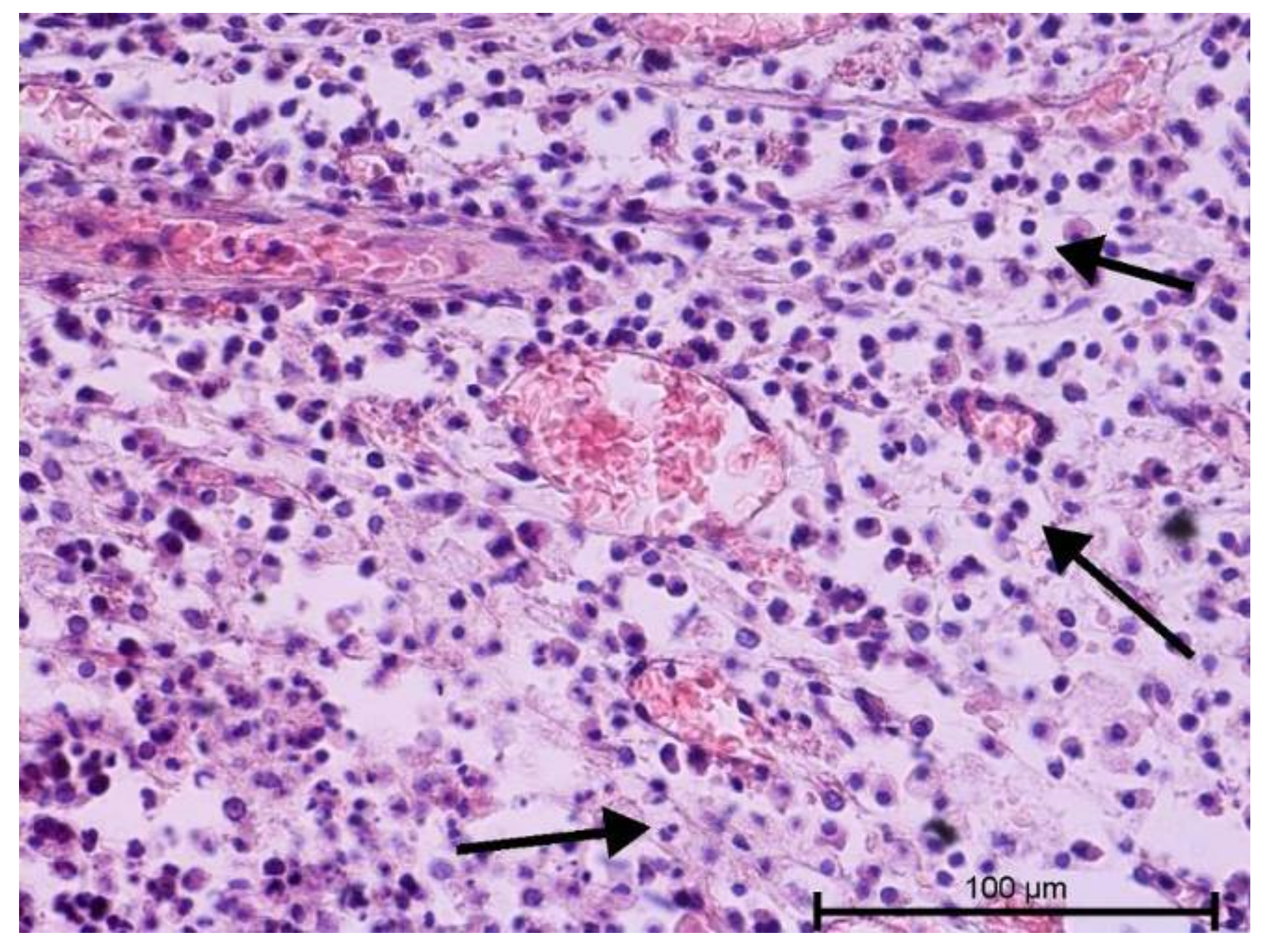
- Group IV—teeth with wide and numerous blood-filled vessels within the dental pulp and without a significant number of inflammatory cells.
3. Methods
3.1. Light and Fluorescence Microscope Examination
3.2. Immunohistochemical Examination
3.3. Scanning Electron Microscope Examination
4. Results
4.1. Light Microscope Examination
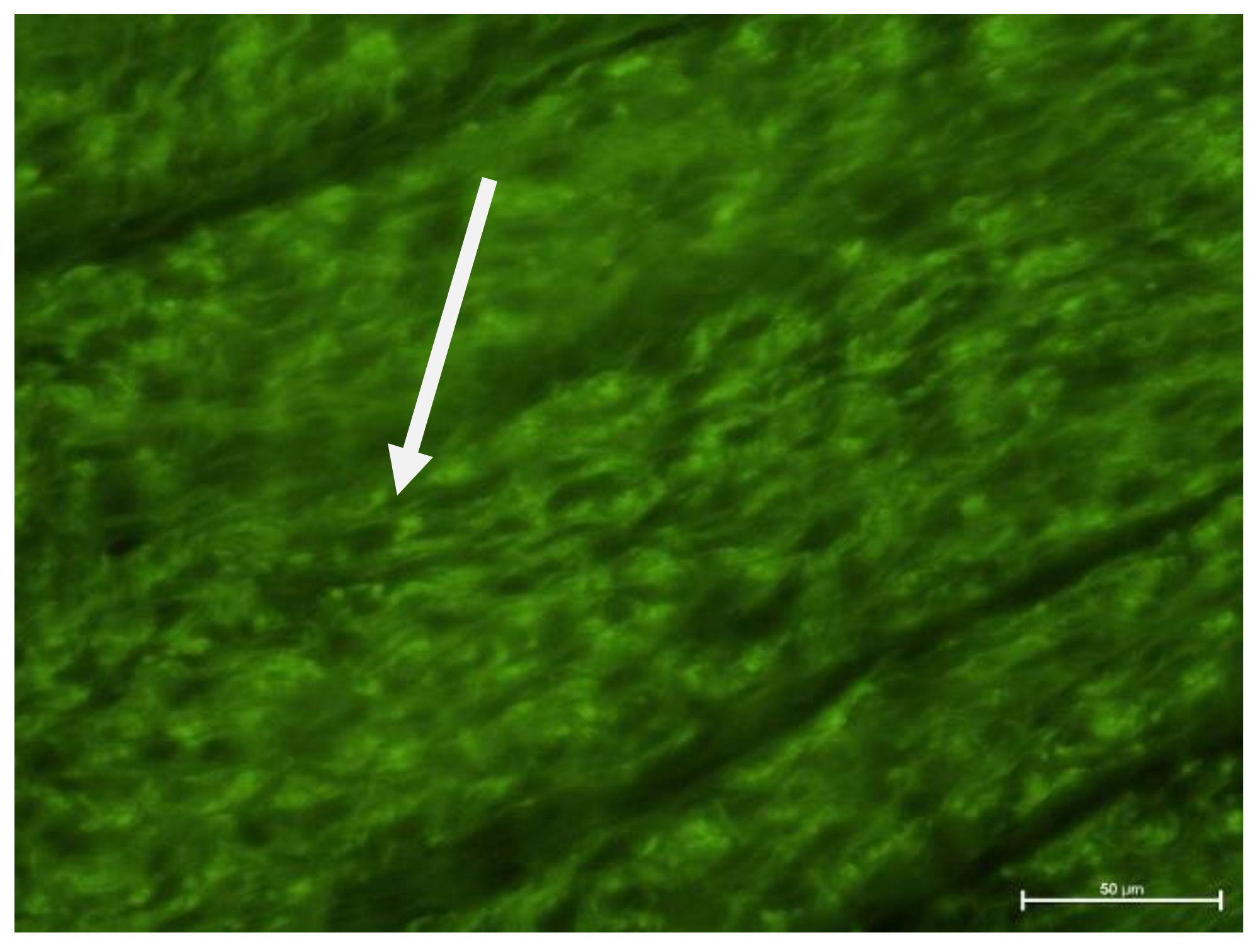
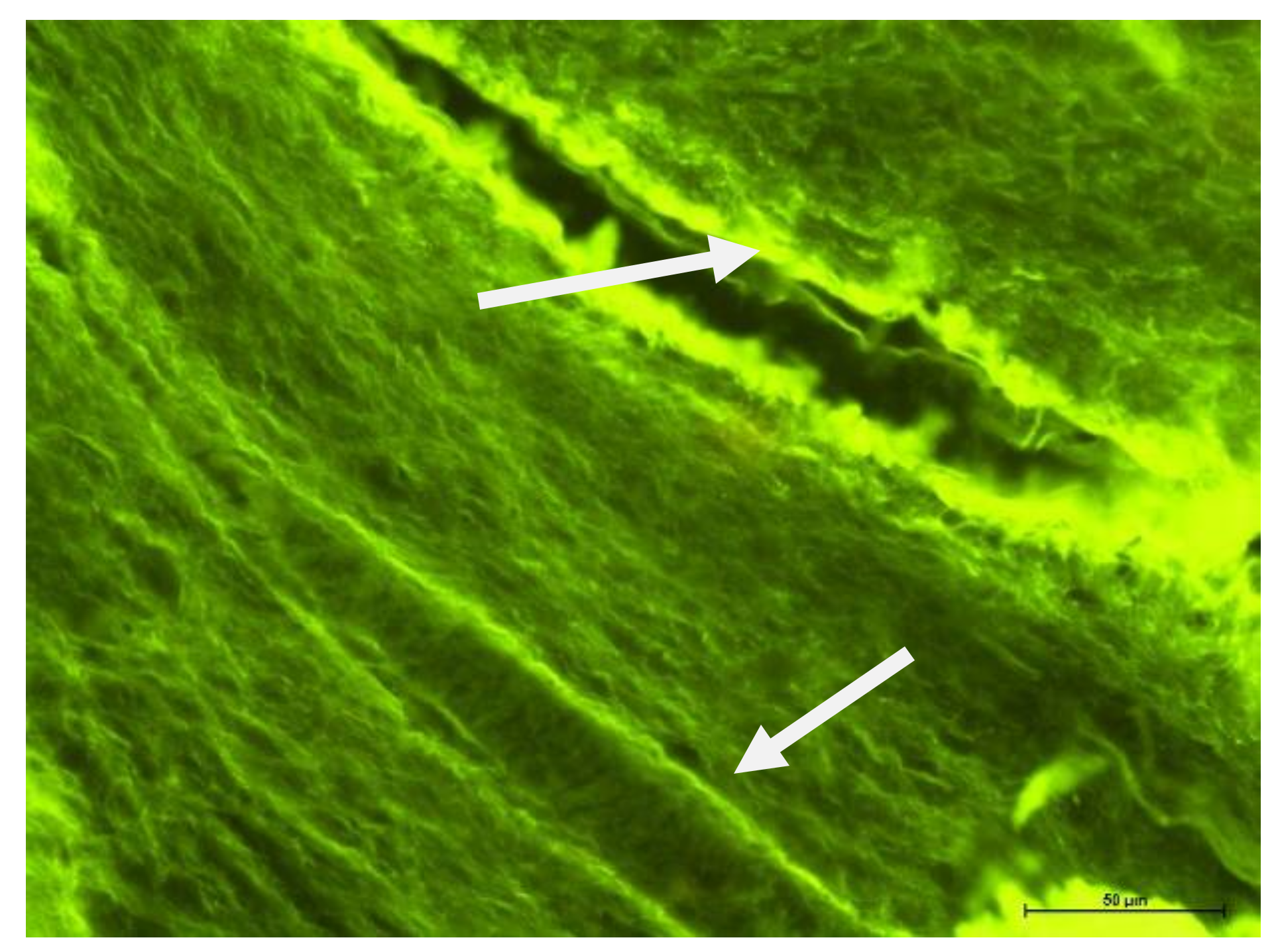
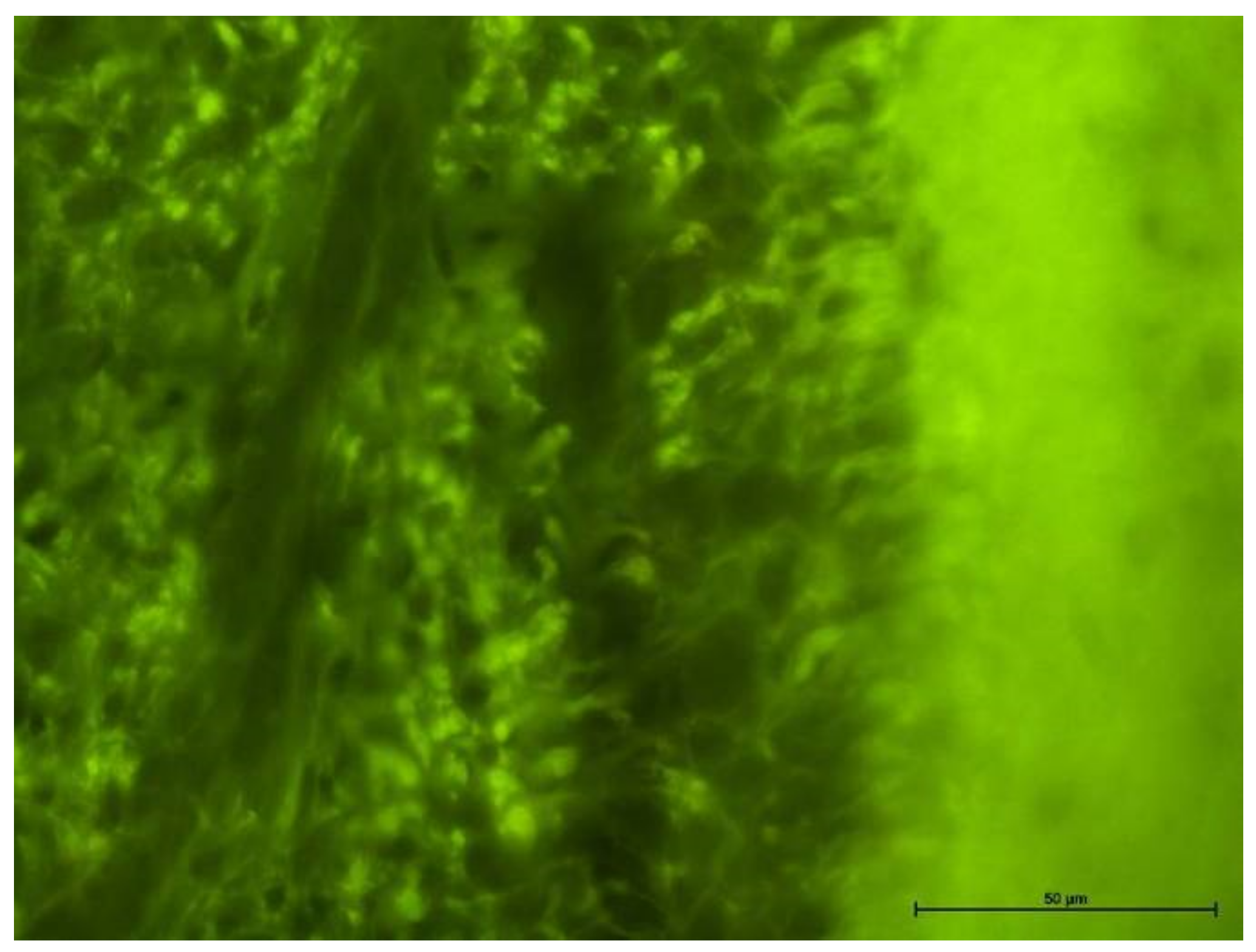
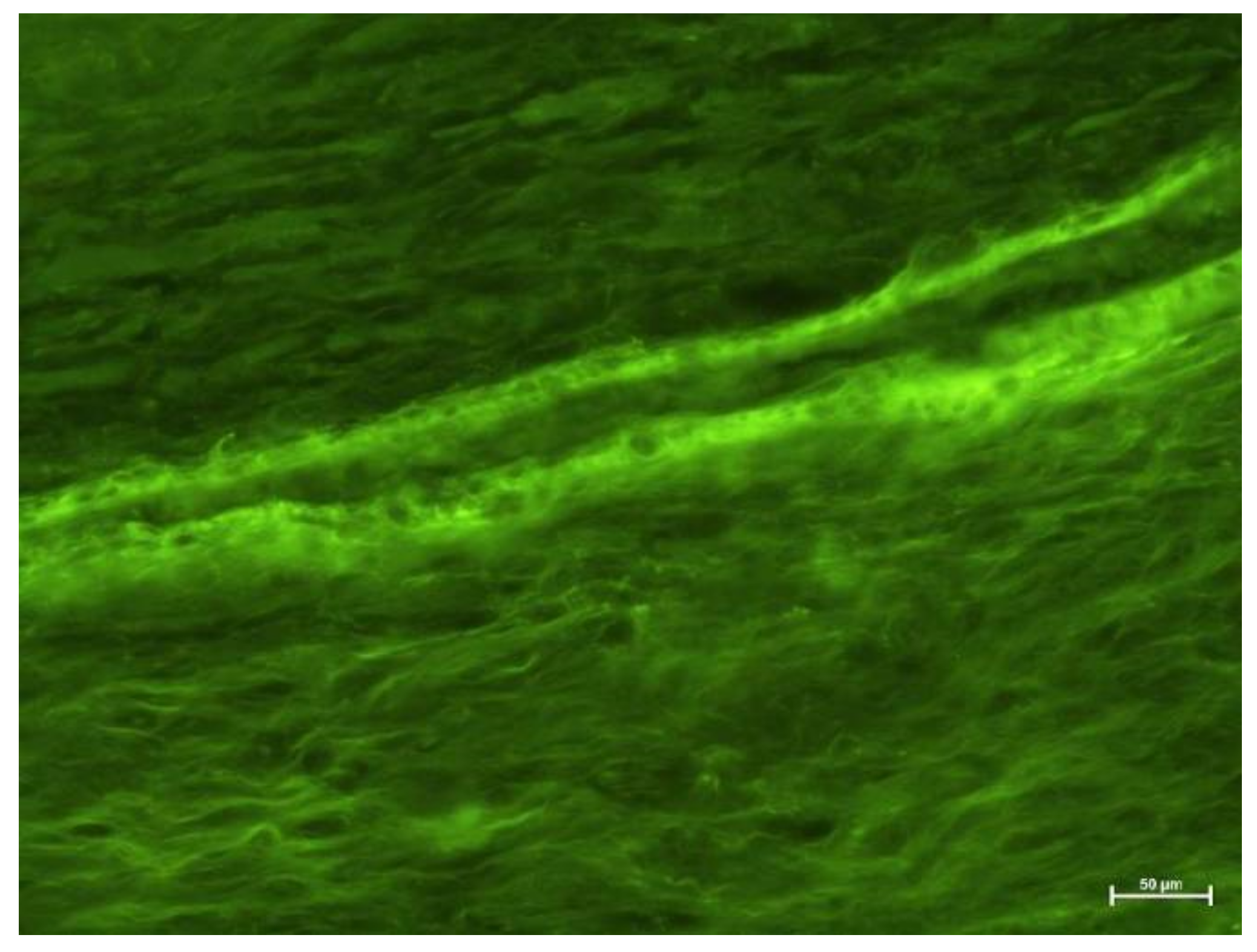
4.2. Fluorescence Microscope Examination
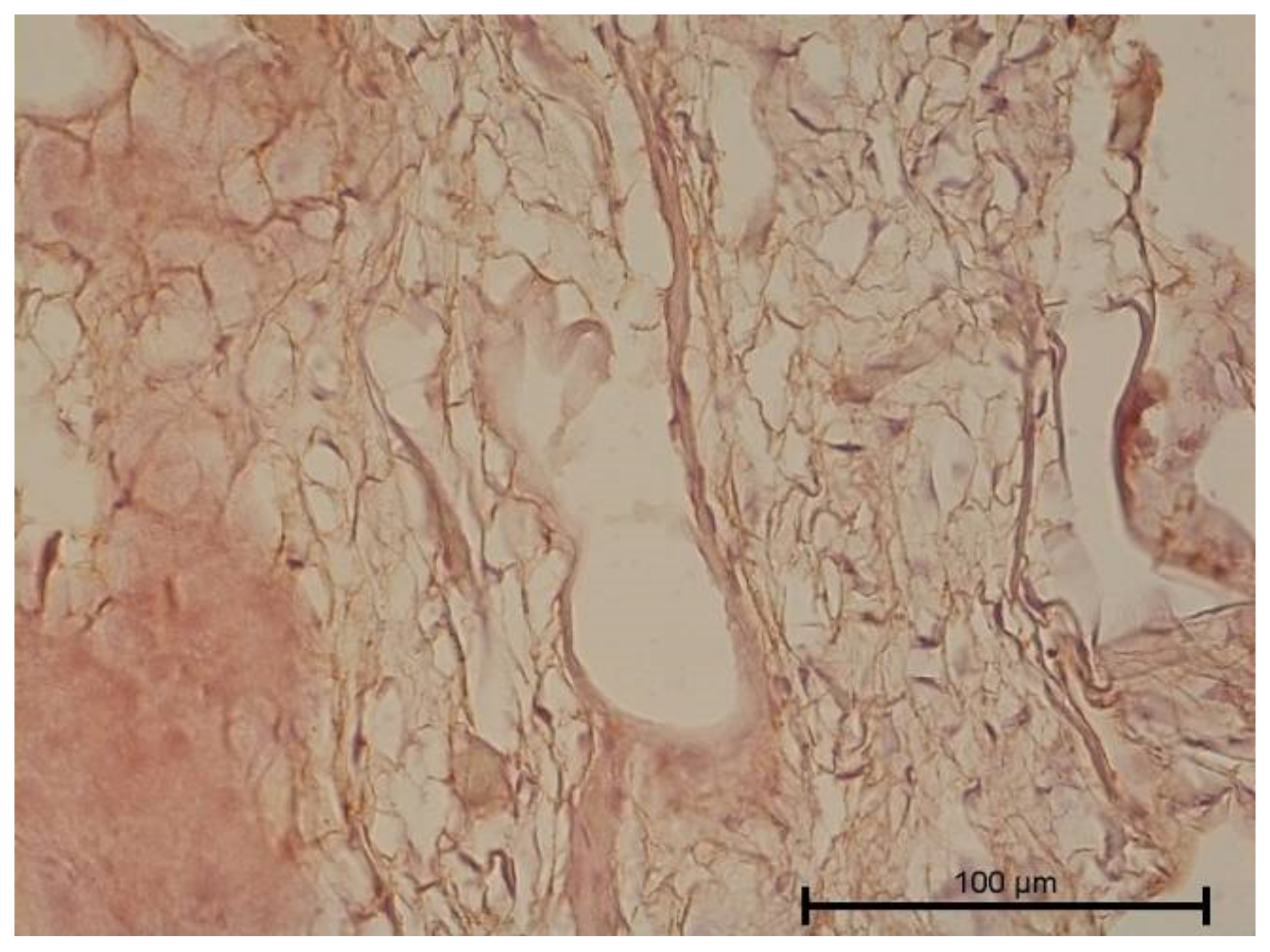
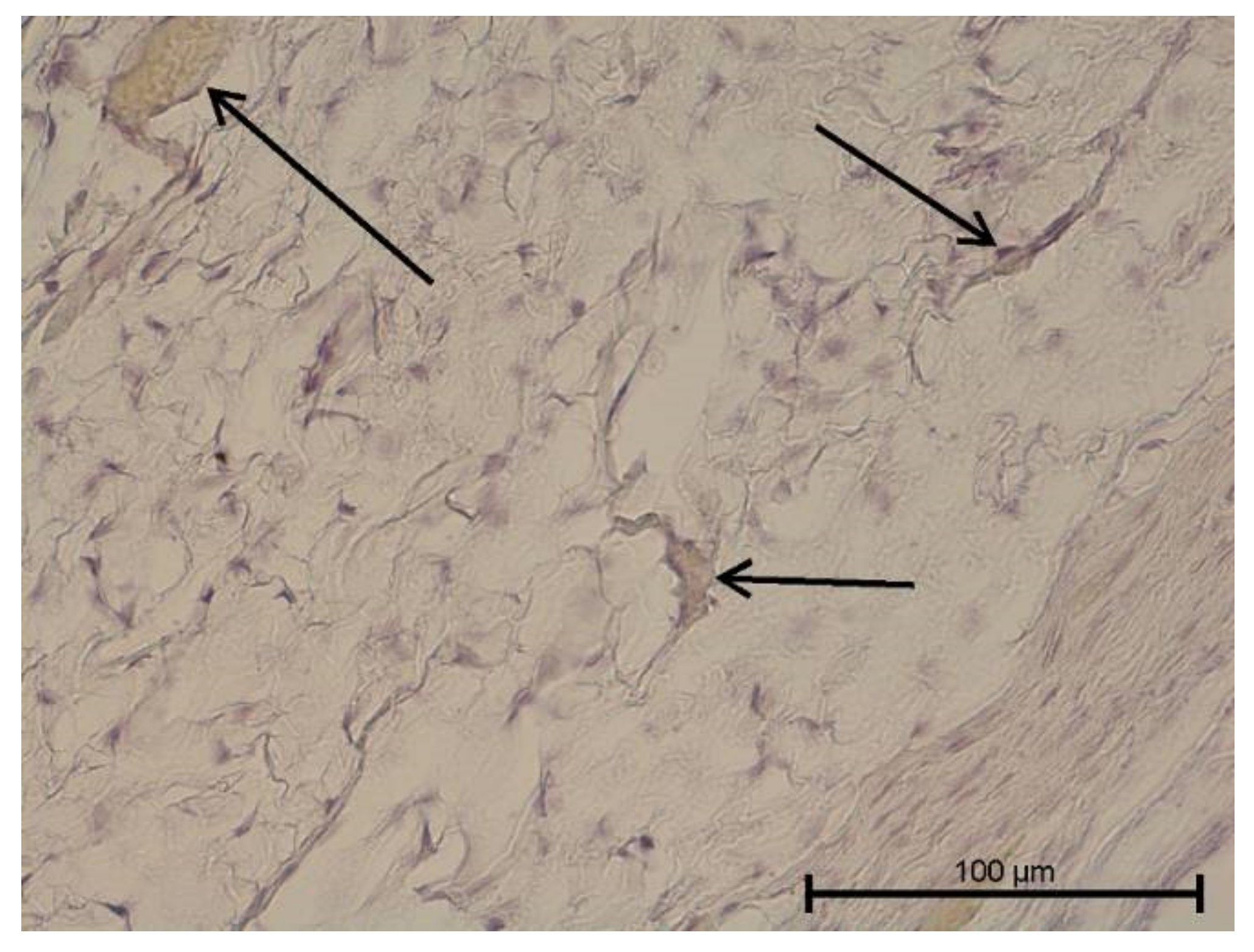
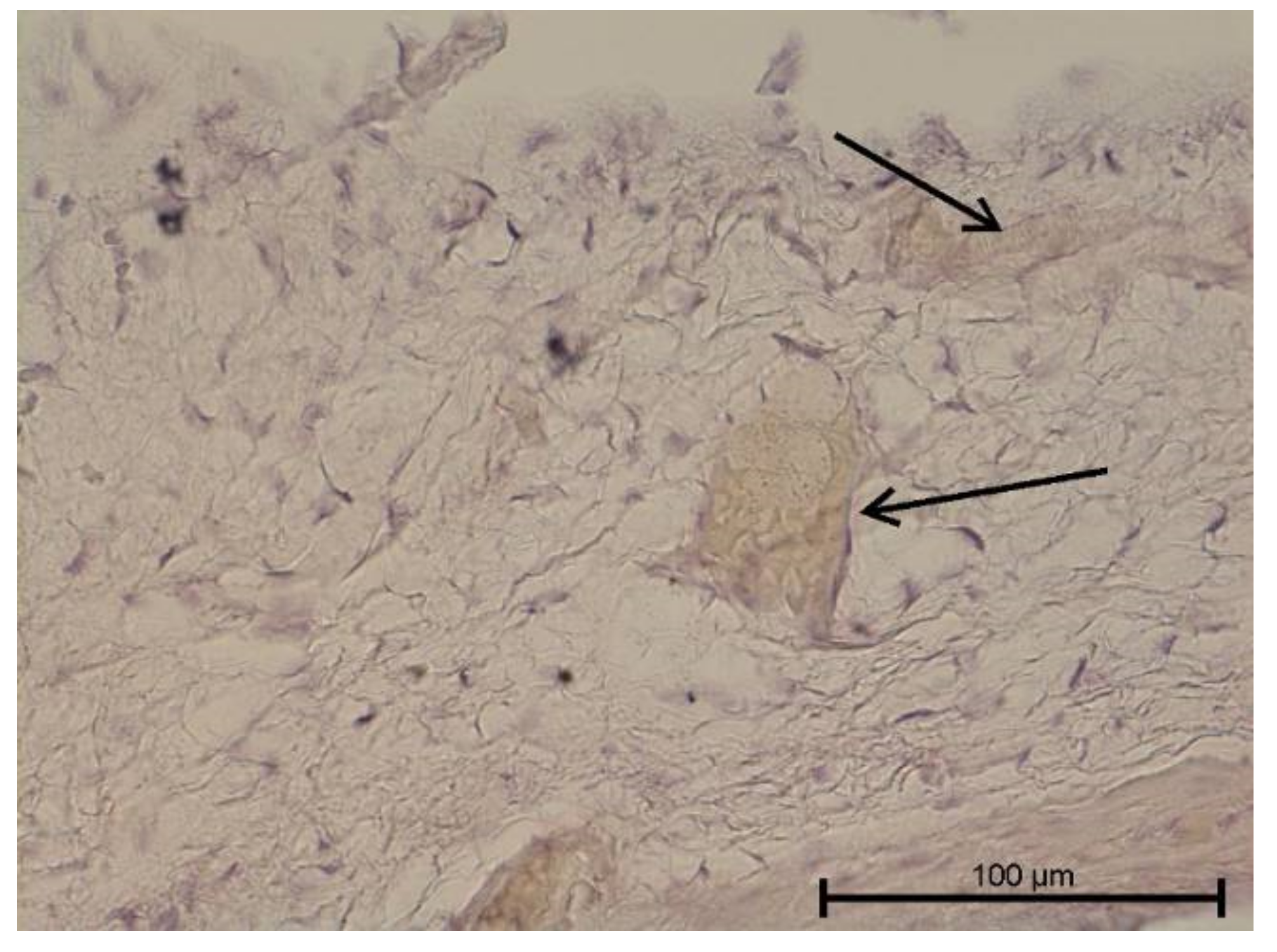
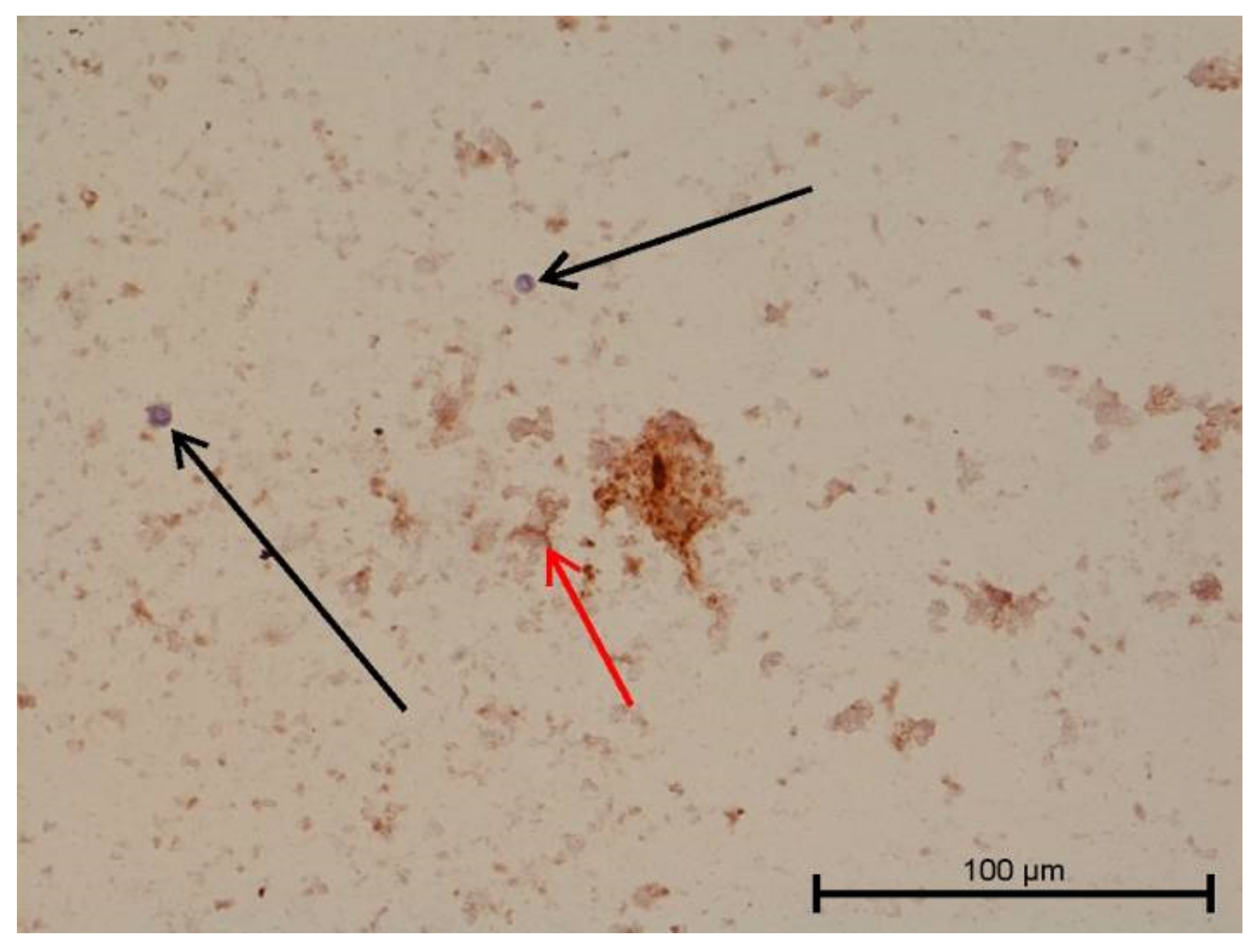
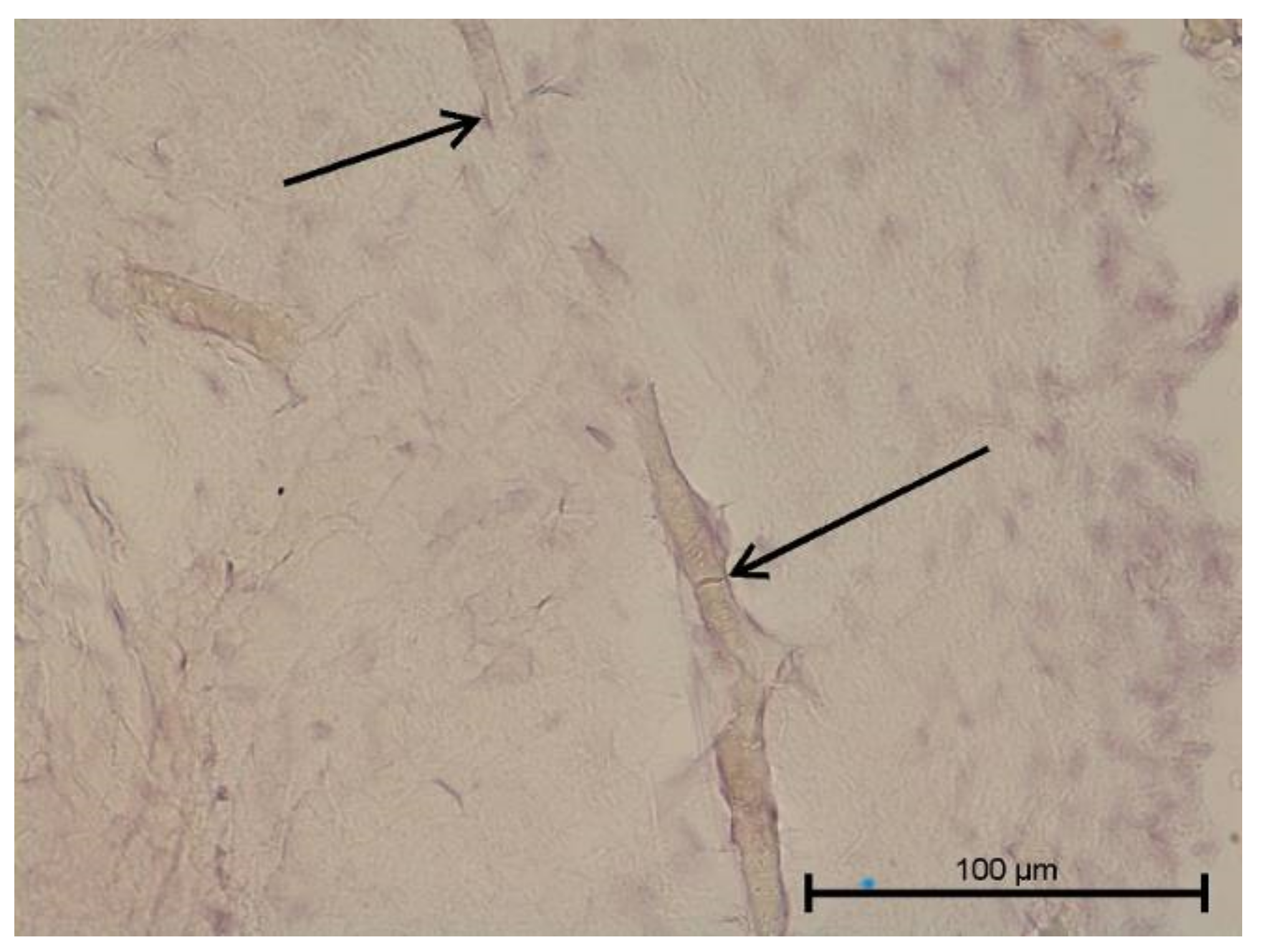
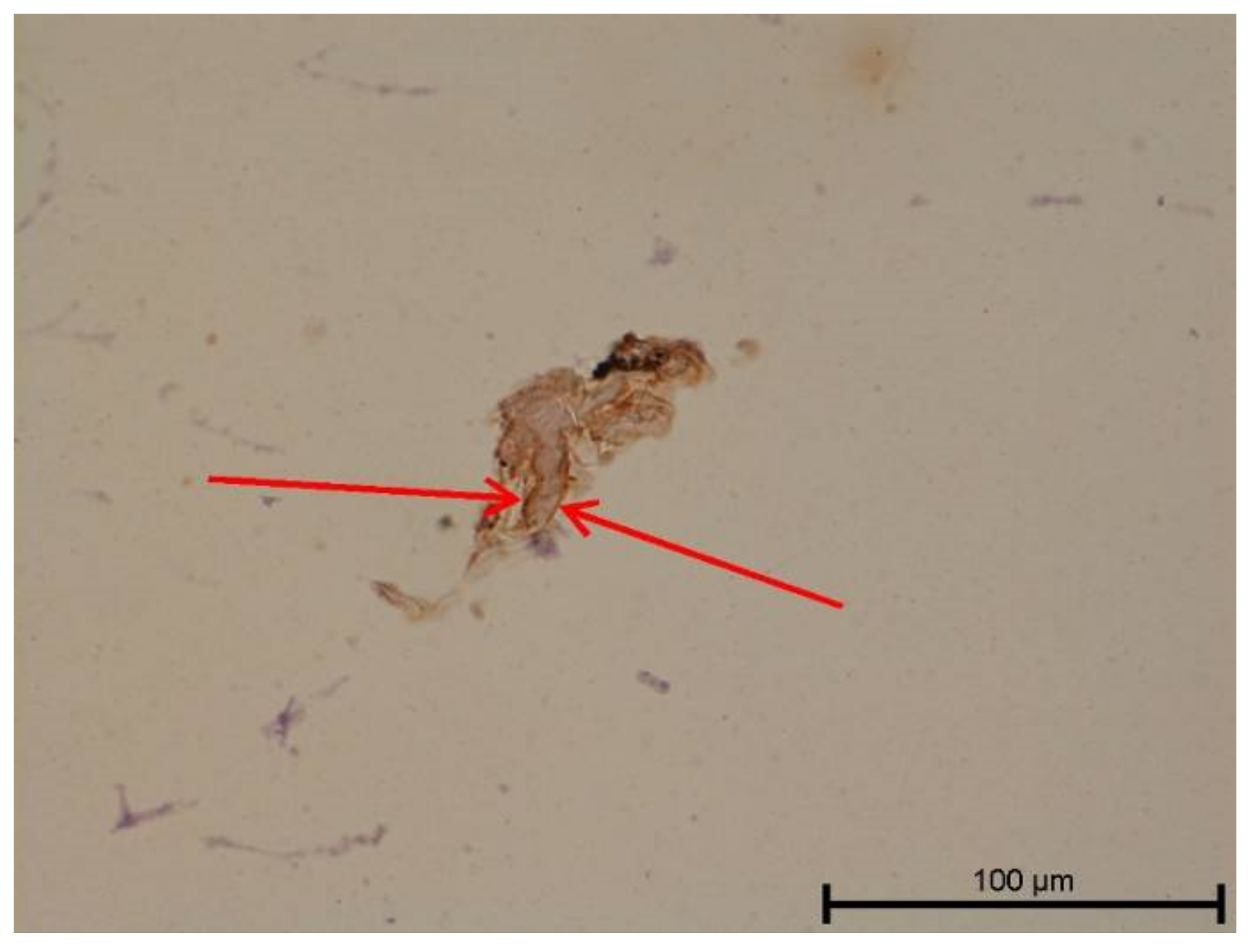
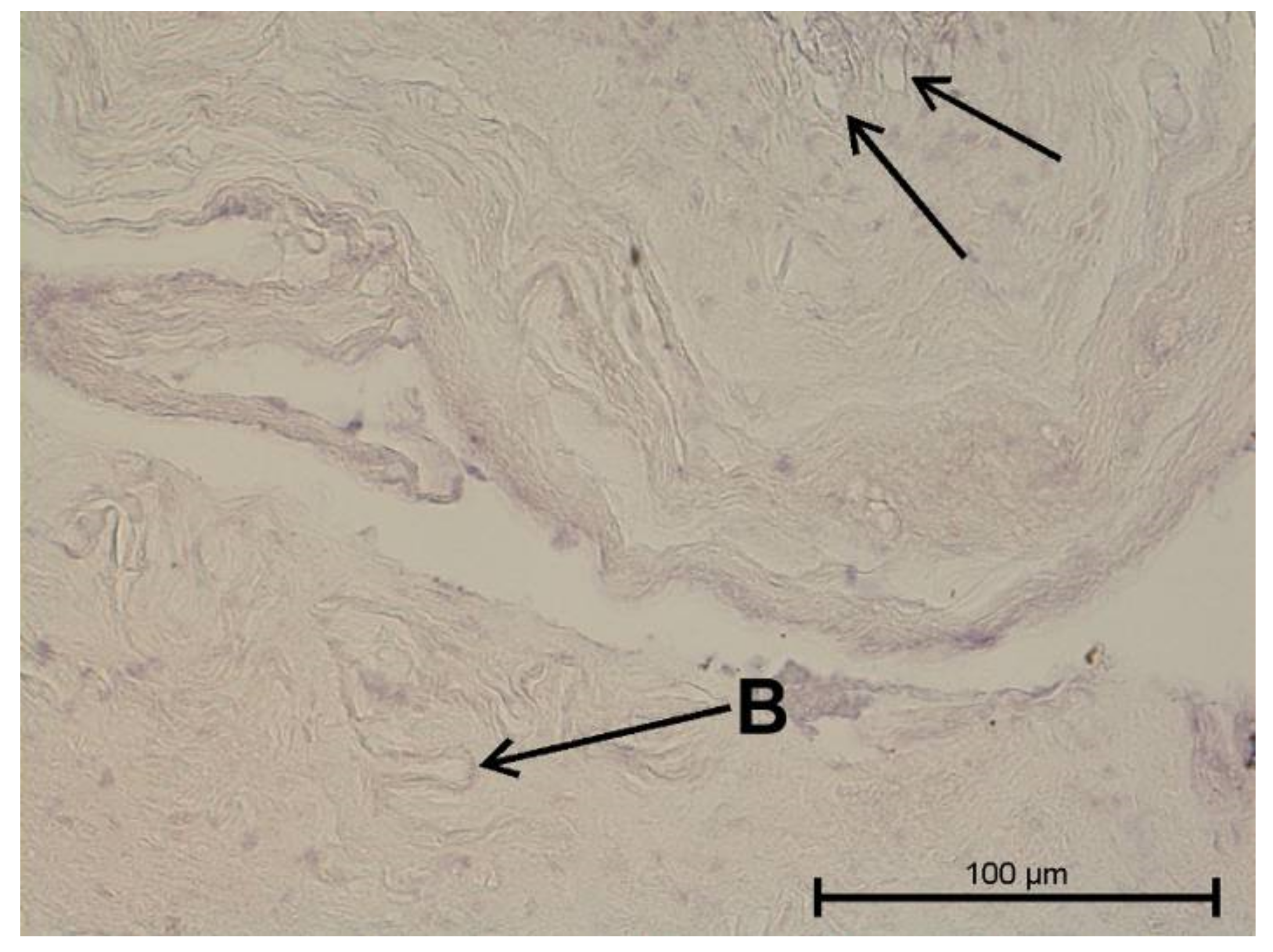
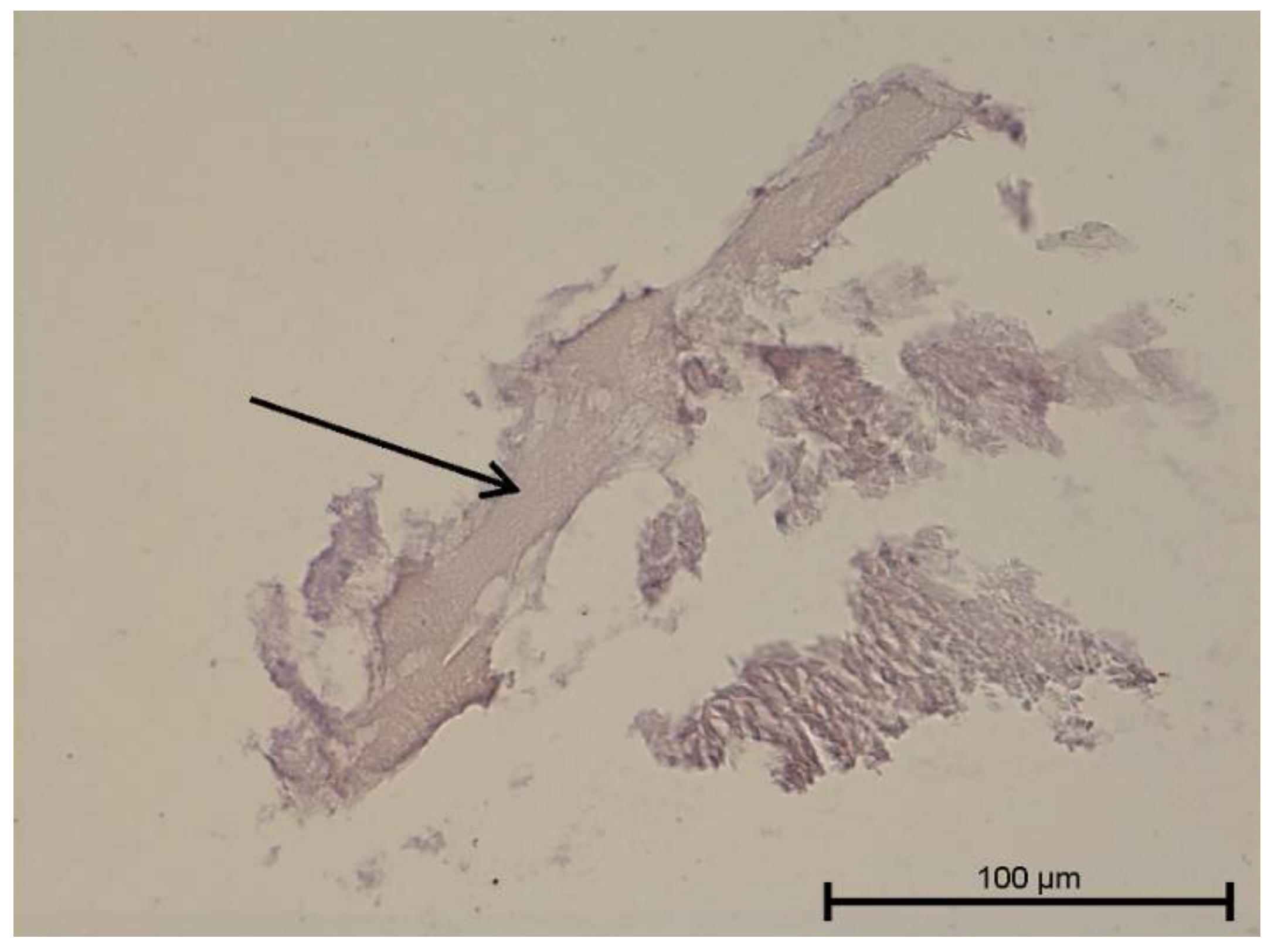
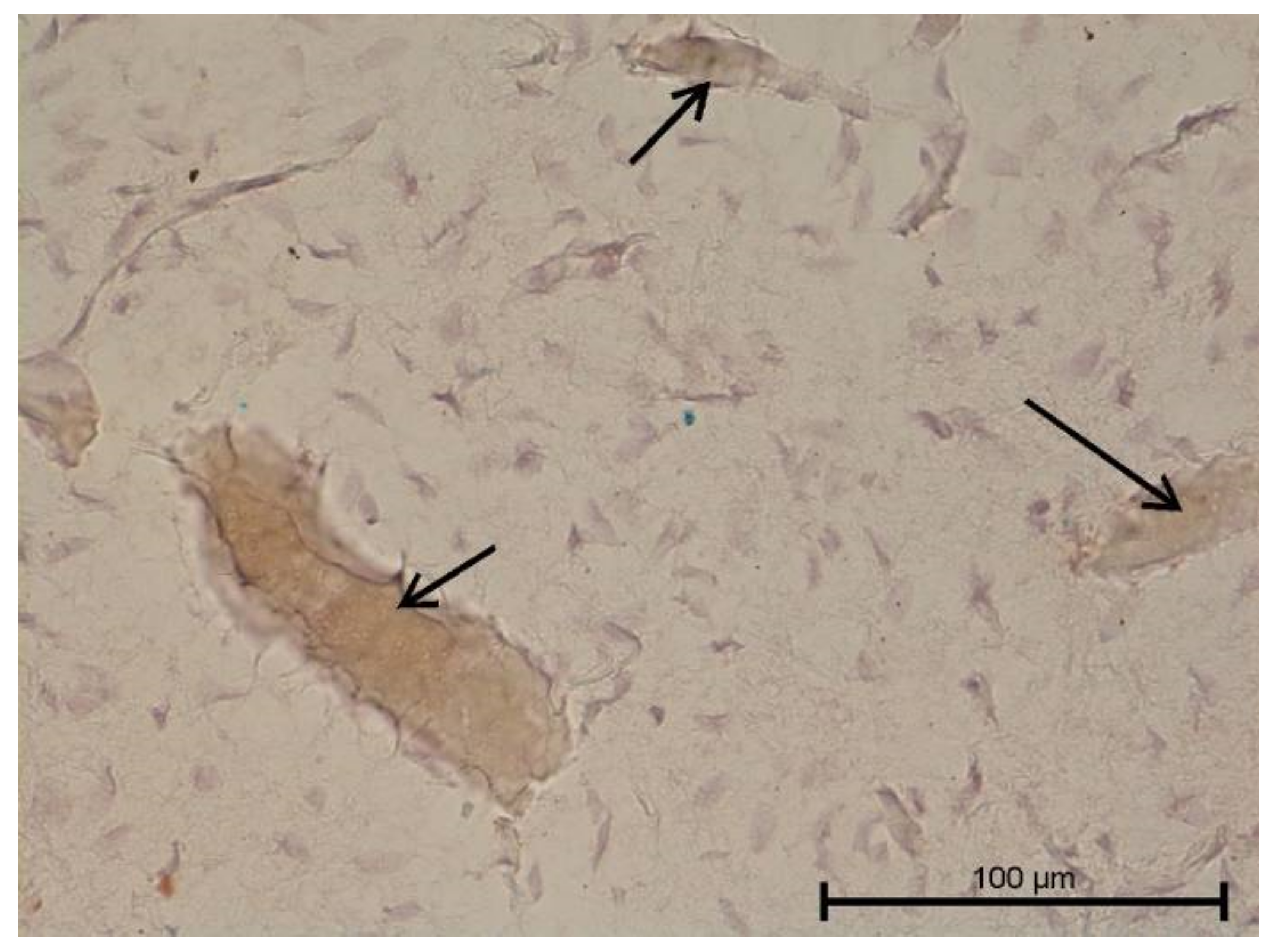
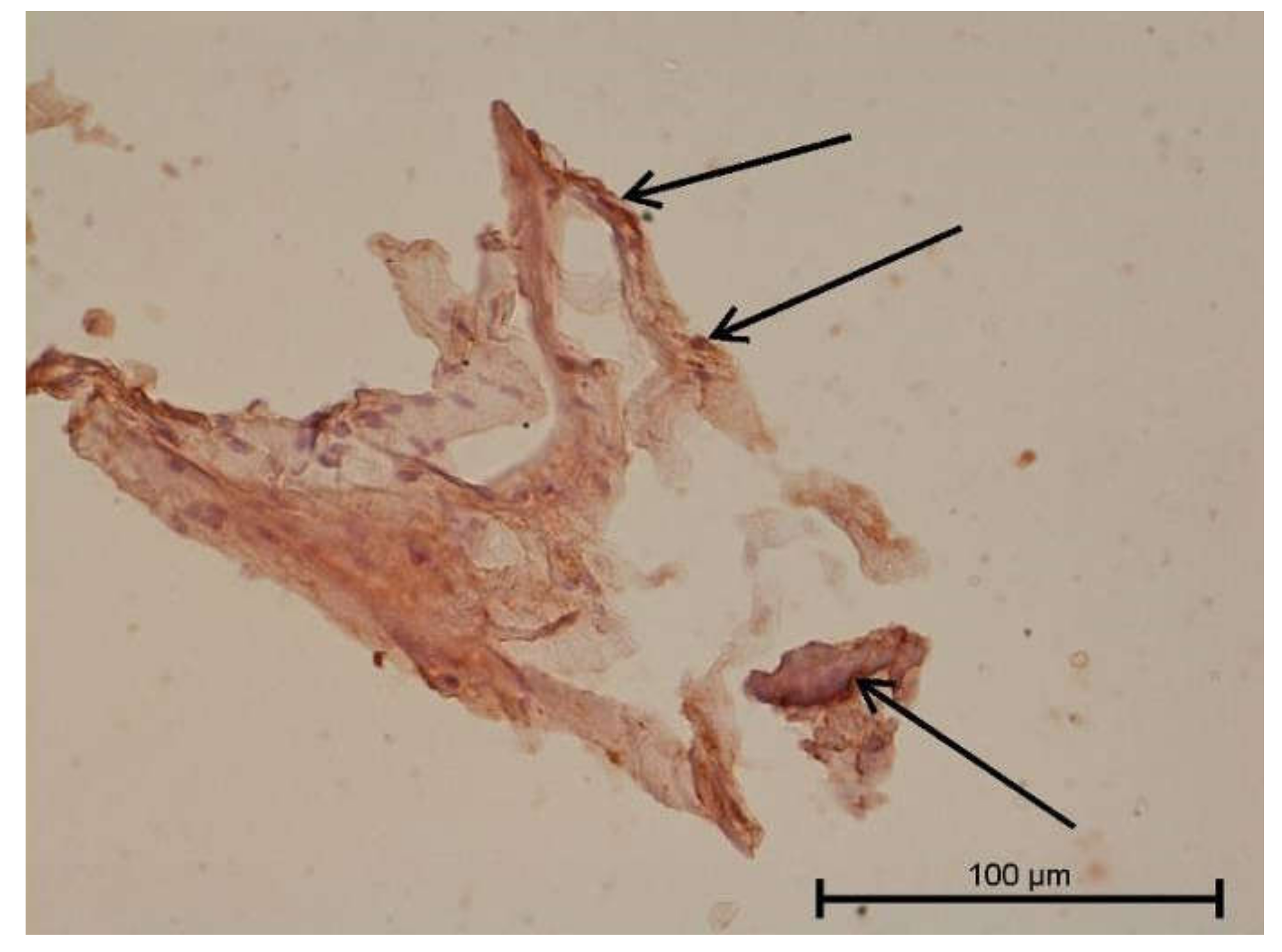
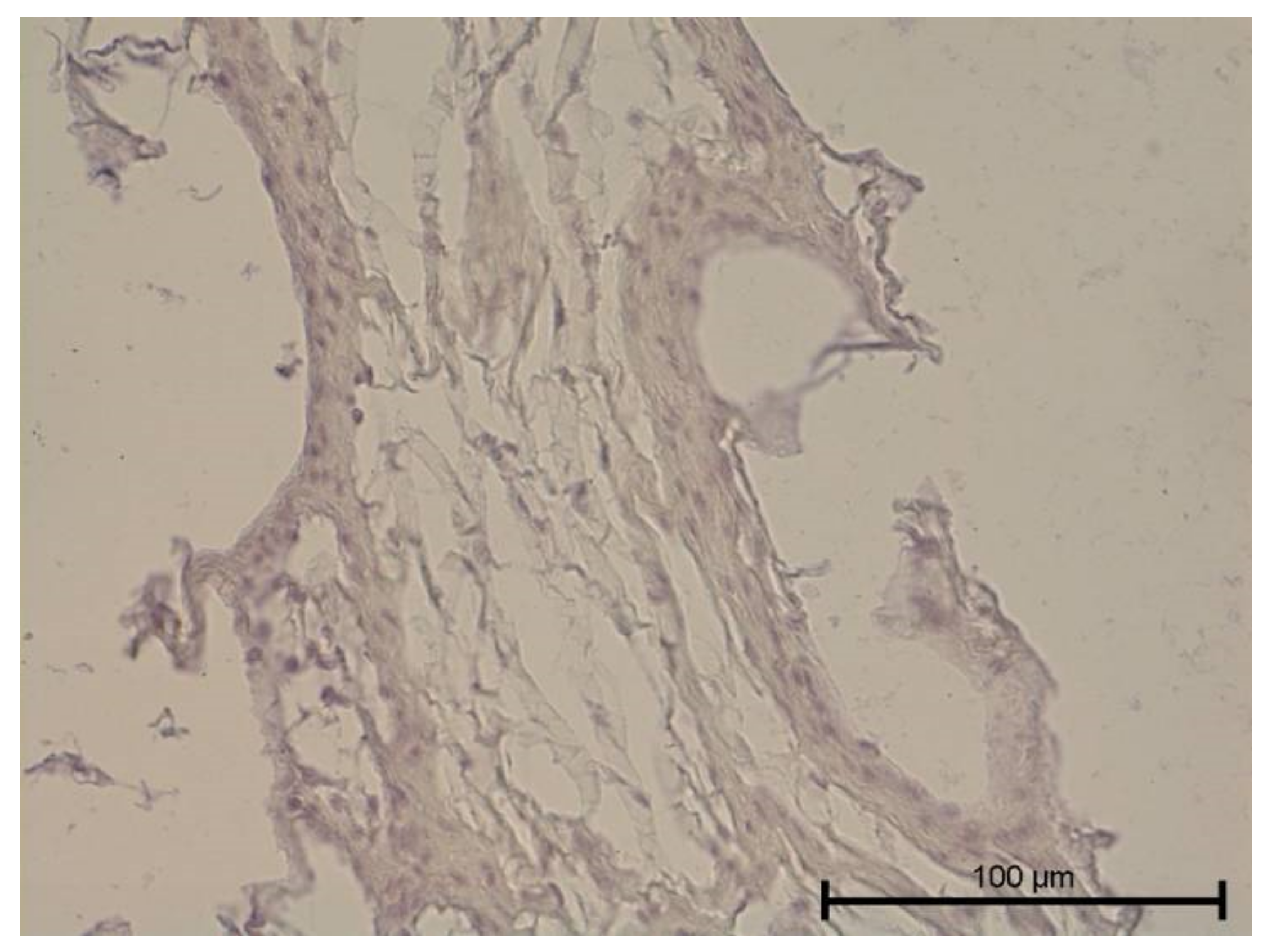
4.3. Immunohistochemical Examination
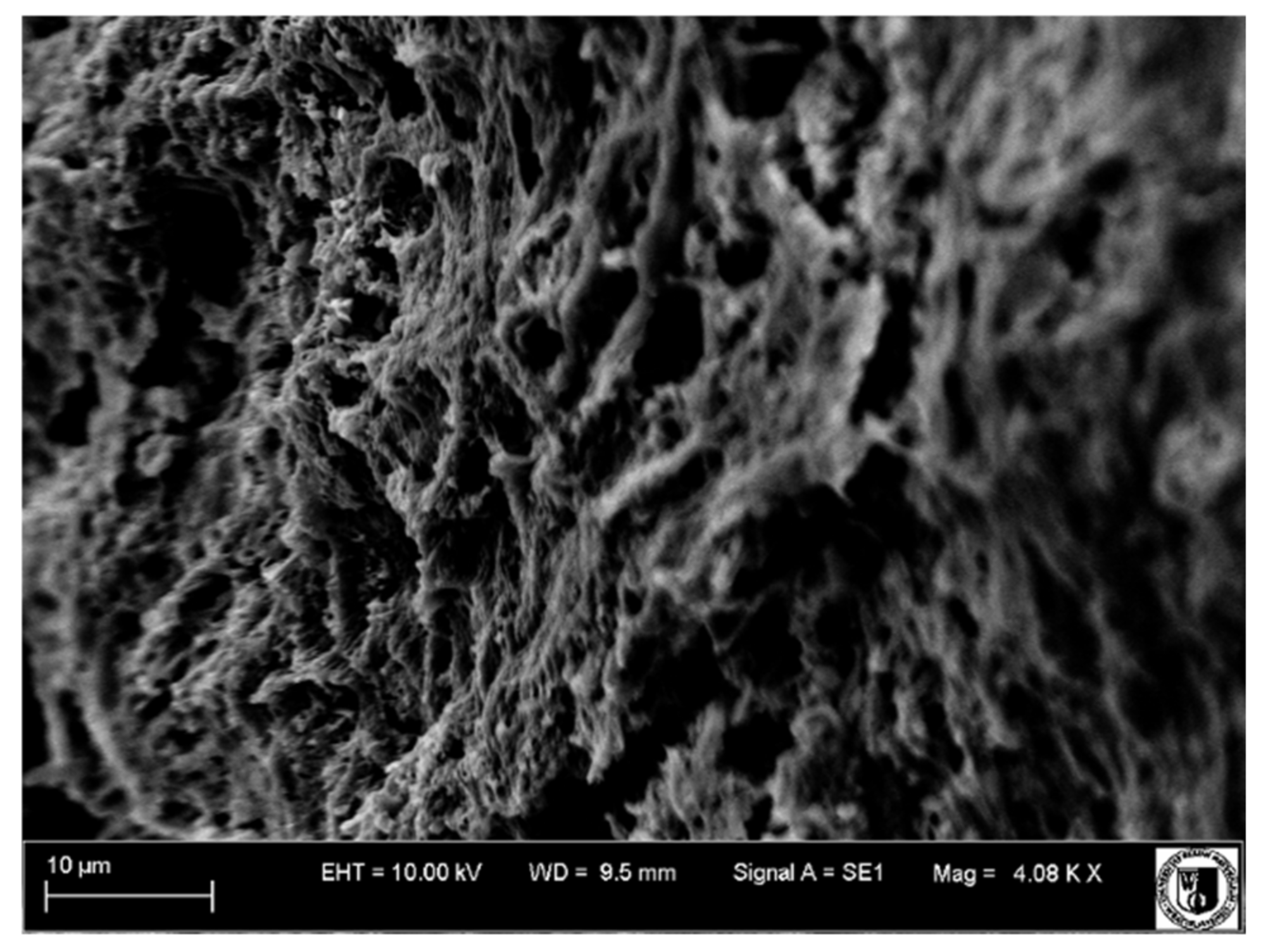
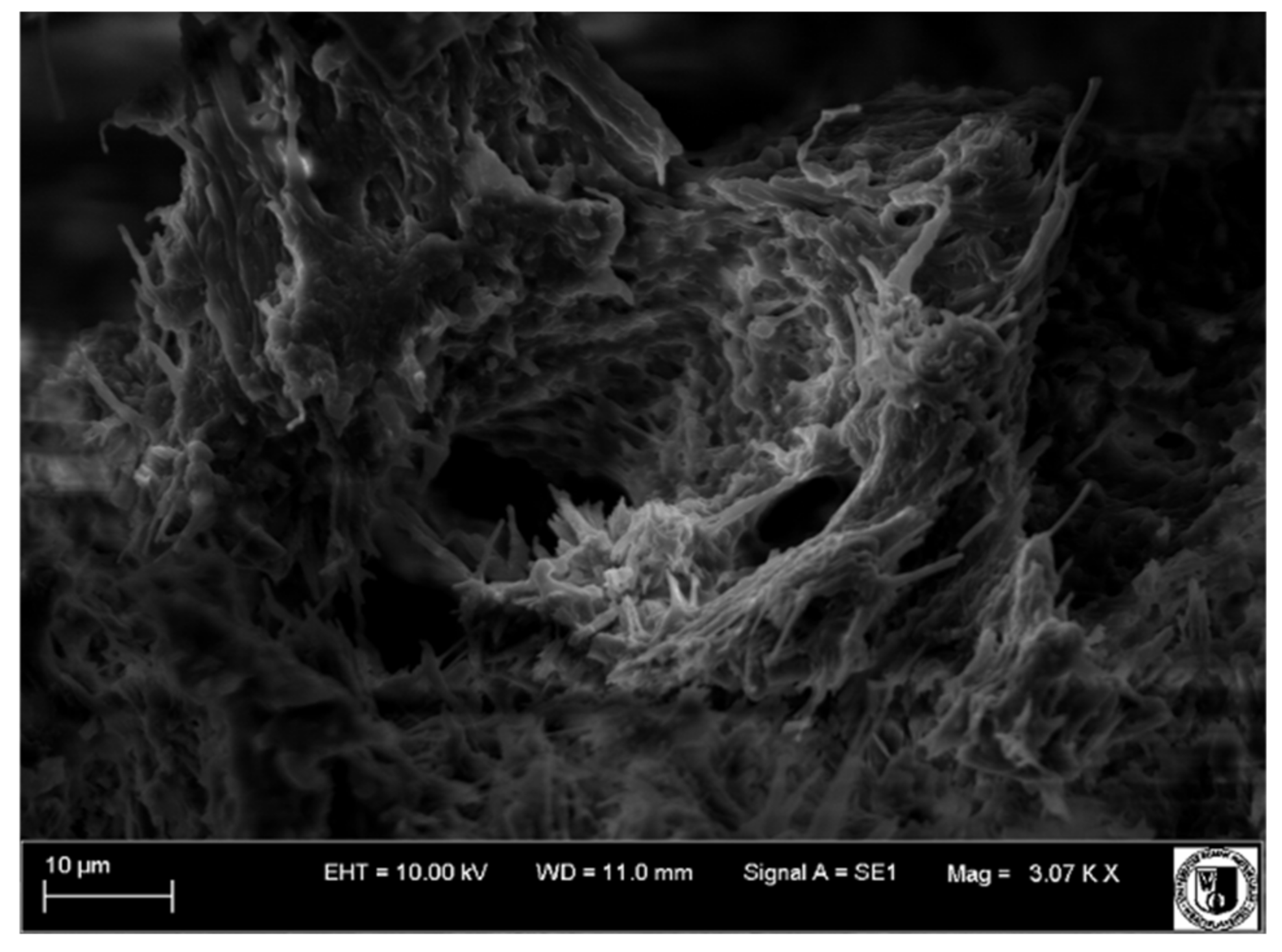
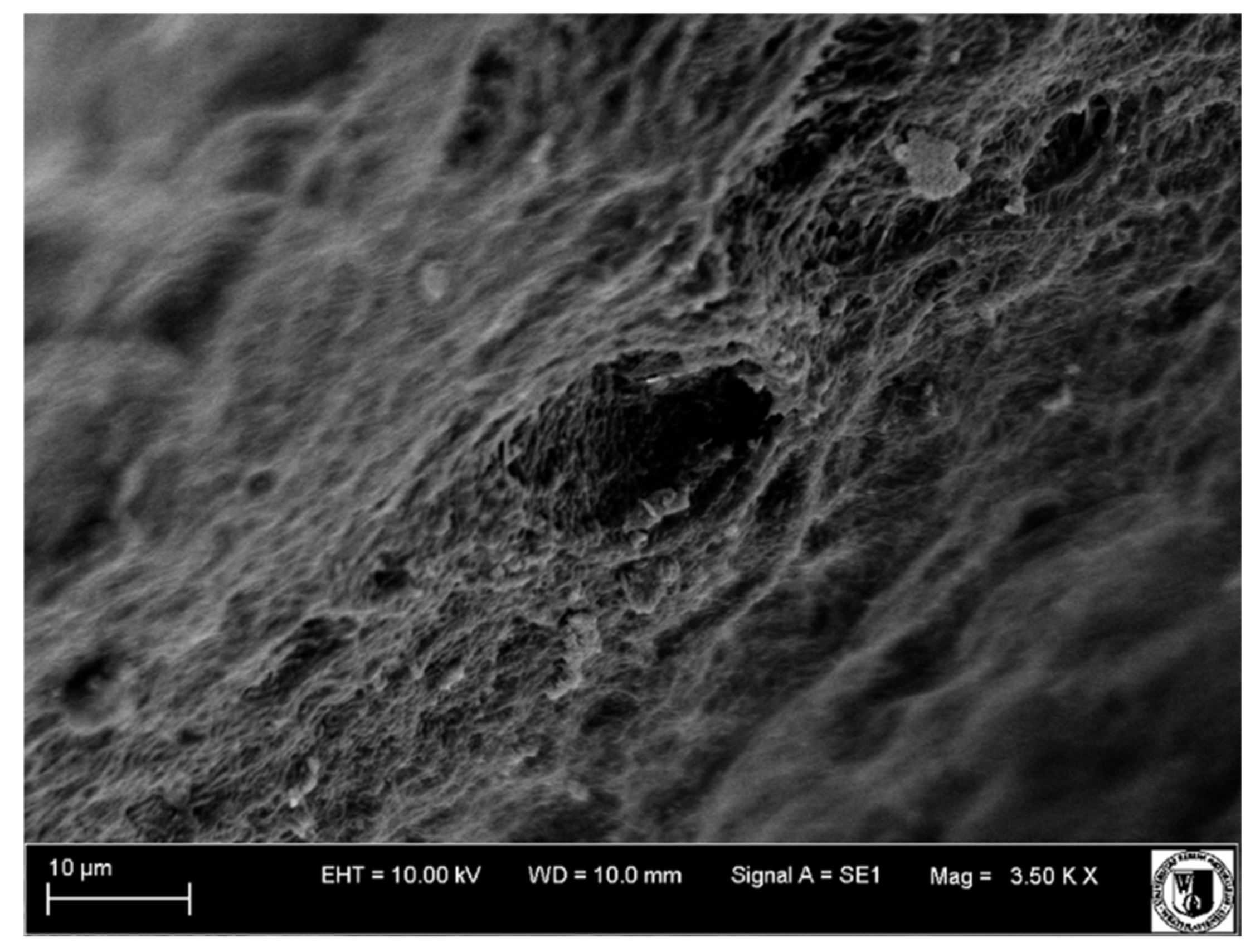
4.4. Scanning Electron Microscope Examination
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mäkinen, T.; Norrmén, C.; Petrova, T.V. Molecular mechanisms of lymphatic vascular development. Cell. Mol. Life Sci. 2007, 64, 1915–1929. [Google Scholar] [CrossRef]
- Al-Rawi, M.A.A.; Mansel, R.E.; Jiang, W.G. Molecular and cellular mechanisms of lymphangiogenesis. Eur. J. Surg. Oncol. 2005, 31, 117–121. [Google Scholar] [CrossRef]
- Martin, A.; Gasse, H.; Staszyk, C. Absence of lymphatic vessels in the dog dental pulp: An immunohistochemical study. J. Anat. 2010, 217, 609–615. [Google Scholar] [CrossRef]
- Staszyk, C.; Duesterdieck, K.F.; Gasse, H.; Bienert, A. lmmunohistochemical ldentification of Lymphatic Vessels in the Periodontium of Equine CheekTeeth. J. Vet. Dent. 2005, 22, 227–232. [Google Scholar] [CrossRef]
- Maruyama, K.; Ii, M.; Cursiefen, C.; Jackson, D.G.; Keino, H.; Tomita, M.; Van Rooijen, N.; Takenaka, H.; D’Amore, P.A.; Stein-Streilein, J.; et al. Inflammation-induced lymphangiogenesis in the cornea arises from CD11b-positive macrophages. J. Clin. Investig. 2005, 115, 2363–2372. [Google Scholar] [CrossRef]
- Wiśniewska, K.; Rybak, Z.; Szymonowicz, M.; Kuropka, P.; Dobrzyński, M. Review on the Lymphatic Vessels in the Dental Pulp. Biology 2021, 10, 1257. [Google Scholar] [CrossRef]
- Bishop, M.A.; Malhotra, M. An investigation of lymphatic vessels in the feline dental pulp. Am. J. Anat. 1990, 187, 247–253. [Google Scholar] [CrossRef]
- Marchetti, C.; Poggi, P.; Calligaro, A.; Casasco, A. Lymphatic Vessels of the Human Dental Pulp in Different Conditions. Anat. Rec. 1992, 33, 27–33. [Google Scholar] [CrossRef]
- Aoyama, Y.; Shigemitsu, Y.; Yoshinobu, N.; Masatsugu, S.; Haruhisa, O. Lymphatic vessels in human dental pulp: An enzymehistochemical study. Jpn. J. Oral Biol. 1995, 37, 437–446. [Google Scholar] [CrossRef] [Green Version]
- Liersch, R.; Detmar, M. Lymphangiogenesis in development and human disease. Thromb. Haemost. 2007, 90, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Berggreen, E.; Haug, S.R.; Mkonyi, L.E.; Bletsa, A. Characterization of the dental lymphatic system and identification of cells immunopositive to specific lymphatic markers. Eur. J. Oral Sci. 2009, 117, 34–42. [Google Scholar] [CrossRef]
- Oehmke, M.J.; Knolle, E.; Oehmke, H.J.; Tranasi, M.; Sberna, M.T.; Zizzari, V.; D’Apolito, G.; Mastrangelo, F.; Salini, L.; Stuppia, L.; et al. Lymph drainage in the human dental pulp. Int. Orthop. 2003, 311, 510–516. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Zhang, B.; Kato, S. Lymphatic networks in the periodontal tissue and dental pulp as revealed by histochemical study. Microsc. Res. Tech. 2002, 56, 50–59. [Google Scholar] [CrossRef]
- Zhang, B.; Miura, M.; Ji, R.C.; Matsumoto, Y.; Yanagisawa, S.; Kato, S. Structural organization and fine distribution of lymphatic vessels in periodontal tissues of the rat and monkey: A histochemical study. Okajimas Folia Anat. Jpn. 2000, 77, 93–107. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, Y.; Kato, S.; Miura, M.; Yanagisawa, S.; Shimizu, M. Fine structure and distribution of lymphatic vessels in the human dental pulp: A study using an enzyme-histochemical method. Cell Tissue Res. 1997, 288, 79–85. [Google Scholar] [CrossRef]
- Heyeraas, K.J. Pulpal hemodynamics and interstitial fluid pressure: Balance of transmicrovascular fluid transport. J. Endod. 1989, 15, 468–472. [Google Scholar] [CrossRef]
- Lohrberg, M.; Wilting, J. The lymphatic vascular system of the mouse head. Cell Tissue Res. 2016, 366, 667. [Google Scholar] [CrossRef] [Green Version]
- Gerli, R.; Secciani, I.; Sozio, F.; Rossi, A.; Weber, E.; Lorenzini, G. Absence of lymphatic vessels in human dental pulp: A morphological study. Eur. J. Oral Sci. 2010, 118, 110–117. [Google Scholar] [CrossRef]
- Xu, H.; Chen, M.; Reid, D.M.; Forrester, J.V. LYVE-1-positive macrophages are present in normal murine eyes. Investig. Ophthalmol. Vis. Sci. 2007, 48, 2162–2171. [Google Scholar] [CrossRef]
- Wilting, J.; Papoutsi, M.; Christ, B.; Nicolaides, K.H.; von Kaisenberg, C.S.; Borges, J.; Stark, G.B.; Alitalo, K.; Tomarev, S.I.; Niemeyer, C.; et al. The transcription factor Prox1 is a marker for lymphatic endothelial cells in normal and diseased human tissues. FASEB J. 2002, 16, 1271–1273. [Google Scholar] [CrossRef]
- Sawa, Y.; Yoshida, S.; Ashikaga, Y.; Kim, T.; Yamaoka, Y.; Suzuki, M. Immunohistochemical demonstration of lymphatic vessels in human dental pulp. Tissue Cell 1998, 30, 510–516. [Google Scholar] [CrossRef]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Examinations | Healthy Teeth [n] | Carious Teeth [n] |
|---|---|---|
| Histological under light microscope | 5 | 10 |
| Immunohistochemical | 5 | 10 |
| Histological under a fluorescence microscope | 5 | 10 |
| Scanning electron microscope | 5 | 10 |
| Antibody | Manufacturer | Type of Antibody |
|---|---|---|
| Anti-Prox 1 | Sigma-Aldrich, Germany | human, polyclonal |
| Anti-VEGFR-3 | Sigma-Aldrich, Germany | human, monoclonal |
| Anti-LYVE1 | Sigma-Aldrich, Germany | human, polyclonal |
| Anti-Collagen IV | Sigma-Aldrich, Germany | human, polyclonal |
| Anti-PDPN | Sigma-Aldrich, Germany | human, polyclonal |
| Antibody | Healthy Teeth X ± SD | Teeth with Caries X ± SD |
|---|---|---|
| Anti-PDPN | 0.75 ± 0.19 | 1.25 ± 0.19 |
| Anti-Collagen IV | 1.75 ± 0.19 | 1.25 ± 0.19 |
| Anti-Prox 1 | 1.25 ± 0.22 | 0.00 |
| Anti-VEGF Receptor-3 | 0.00 | 0.50 ± 0.22 |
| Anti-LYVE1 | 0.00 | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiśniewska, K.; Rybak, Z.; Szymonowicz, M.; Kuropka, P.; Kaleta-Kuratewicz, K.; Dobrzyński, M. Detection of Lymphatic Vessels in Dental Pulp. Biology 2022, 11, 635. https://doi.org/10.3390/biology11050635
Wiśniewska K, Rybak Z, Szymonowicz M, Kuropka P, Kaleta-Kuratewicz K, Dobrzyński M. Detection of Lymphatic Vessels in Dental Pulp. Biology. 2022; 11(5):635. https://doi.org/10.3390/biology11050635
Chicago/Turabian StyleWiśniewska, Kamila, Zbigniew Rybak, Maria Szymonowicz, Piotr Kuropka, Katarzyna Kaleta-Kuratewicz, and Maciej Dobrzyński. 2022. "Detection of Lymphatic Vessels in Dental Pulp" Biology 11, no. 5: 635. https://doi.org/10.3390/biology11050635
APA StyleWiśniewska, K., Rybak, Z., Szymonowicz, M., Kuropka, P., Kaleta-Kuratewicz, K., & Dobrzyński, M. (2022). Detection of Lymphatic Vessels in Dental Pulp. Biology, 11(5), 635. https://doi.org/10.3390/biology11050635