
Tumor Microenvironment—A Short Review of Cellular and Interaction Diversity



Abstract
:Simple Summary
Abstract
1. Introduction
2. What Happens When Neoplastic Cells Begin to Grow?
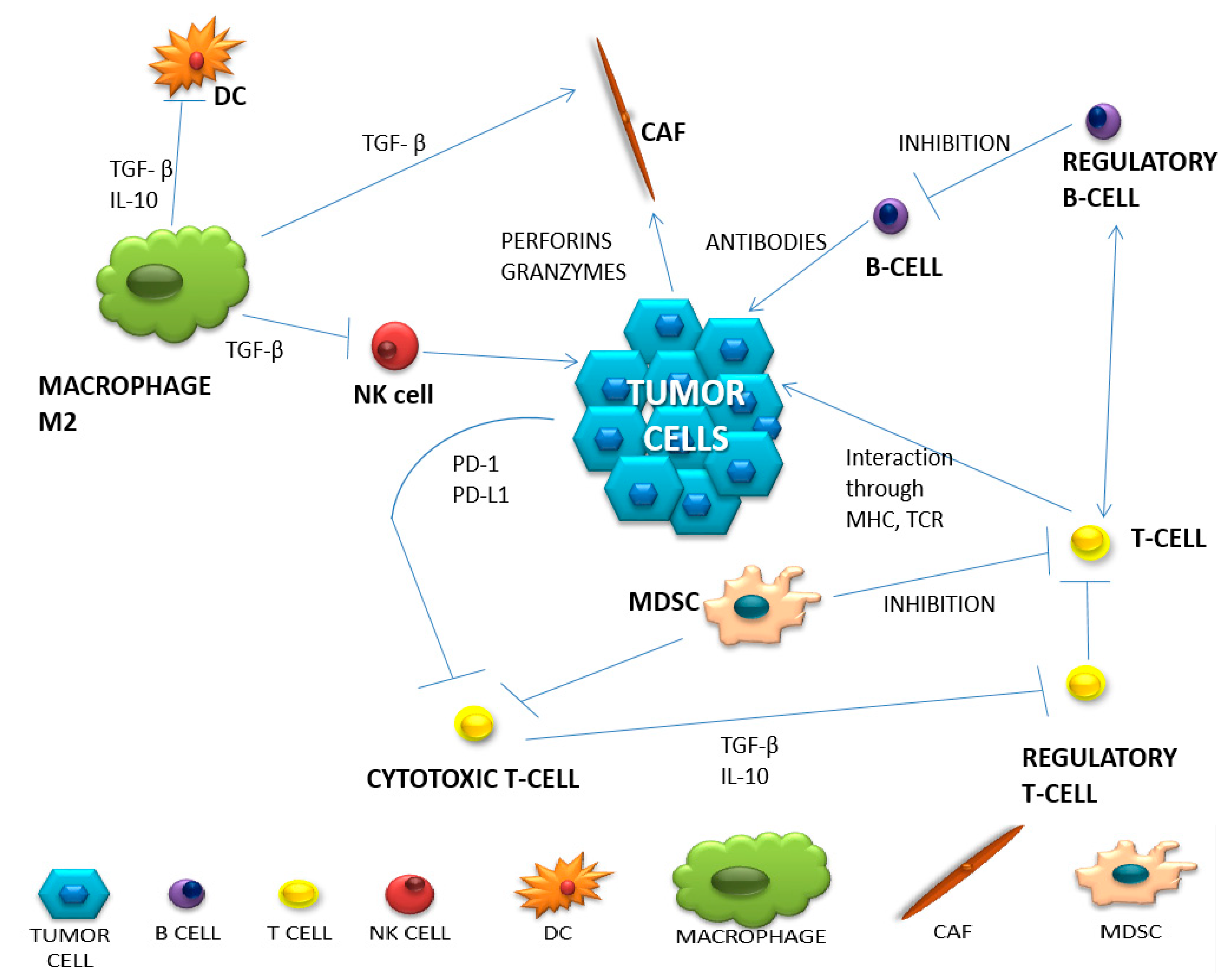
3. Diversity of Intercellular Interactions in the Tumor Microenvironment
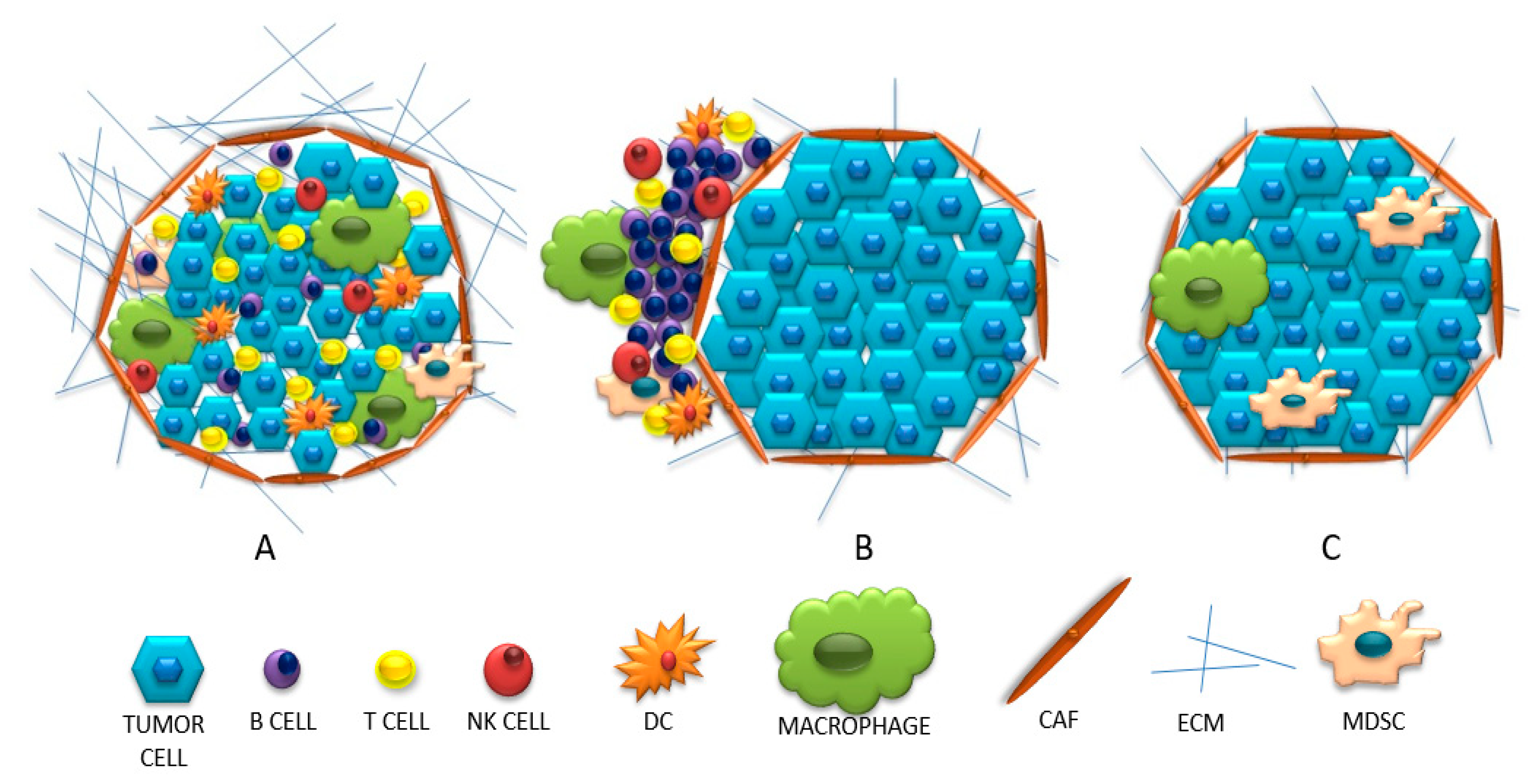
4. Three Categories of Tumor Microenvironments Based on Their Immunophenotype
5. The Tumor Microenvironment in Melanoma, Breast and Kidney Cancer
6. The Use of Cellular Interactions in the Treatment of Cancer
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, I.; Nabet, B.Y. Exosomes in the tumor microenvironment as mediators of cancer therapy resistance. Mol. Cancer 2019, 18, 32. [Google Scholar] [CrossRef] [PubMed]
- Hinshaw, D.C.; Shevde, L.A. The tumor microenvironment innately modulates cancer progression. Cancer Res. 2019, 79, 4557–4567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Rao, L.; Yu, G.; Cook, T.R.; Chen, X.; Huang, F. Supramolecular cancer nanotheranostics. Chem. Soc. Rev. 2021, 50, 2839–2891. [Google Scholar] [CrossRef]
- Zhou, J.; Yu, G.; Huang, F. Supramolecular chemotherapy based on host-guest molecular recognition: A novel strategy in the battle against cancer with a bright future. Chem. Soc. Rev. 2017, 46, 7021–7053. [Google Scholar] [CrossRef]
- Ding, Y.; Tong, Z.; Jin, L.; Ye, B.; Zhou, J.; Sun, Z.; Mao, Z. An NIR Discrete Metallacycle Constructed from Perylene Bisimide and Tetraphenylethylene Fluorophores for Imaging-Guided Cancer Radio-Chemotherapy. Adv. Mater. 2022, 34, 2106388. [Google Scholar] [CrossRef] [PubMed]
- Baghban, R.; Roshangar, L.; Jahanban-Esfahlan, R.; Seidi, K.; Ebrahimi-Kalan, A.; Jaymand, M.; Zare, P. Tumor microenvironment complexity and therapeutic implications at a glance. Cell Commun. Signal 2020, 18, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farc, O.; Cristea, V. An overview of the tumor microenvironment, from cells to complex networks (Review). Exp. Ther. Med. 2020, 21, 1–13. [Google Scholar] [CrossRef]
- Tamminga, M.; Hiltermann, T.J.N.; Schuuring, E.; Timens, W.; Fehrmann, R.S.N.; Groen, H.J.M. Immune microenvironment composition in non-small cell lung cancer and its association with survival. Clin. Transl. Immunol. 2020, 9, 1–13. [Google Scholar] [CrossRef]
- Petrova, V.; Annicchiarico-Petruzzelli, M.; Melino, G.; Amelio, I. The hypoxic tumour microenvironment. Oncogenesis 2018, 7, 1–13. [Google Scholar] [CrossRef]
- De Guillebon, E.; Dardenne, A.; Saldmann, A.; Séguier, S.; Tran, T.; Paolini, L.; Tartour, E. Beyond the concept of cold and hot tumors for the development of novel predictive biomarkers and the rational design of immunotherapy combination. Int. J. Cancer 2020, 147, 1509–1518. [Google Scholar] [CrossRef]
- Wang, M.; Zhao, J.; Zhang, L.; Wei, F.; Lian, Y.; Wu, Y.; Guo, C. Role of tumor microenvironment in tumorigenesis. J. Cancer 2017, 8, 761–773. [Google Scholar] [CrossRef] [PubMed]
- Gołąb, J.; Jakóbisiak, M.; Lasek, W.; Stokłosa, T. Immunologia; PWN: Warsaw, 2017; pp. 1–5. [Google Scholar]
- Deng, S.; Clowers, M.J.; Velasco, W.V.; Ramos-Castaneda, M.; Moghaddam, S.J. Understanding the Complexity of the Tumor Microenvironment in K-ras Mutant Lung Cancer: Finding an Alternative Path to Prevention and Treatment. Front. Oncol. 2020, 9, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Pallegar Nikitha, K. CSL. Adipocytes in the Tumour Microenvironment. Adv. Exp. Med. Biol. 2020, 1224, 1–13. [Google Scholar]
- Iwahori, K. Cytotoxic CD8+ Lymphocytes in the Tumor Microenvironment. Adv. Exp. Med. Biol. 2018, 1224, 53–62. [Google Scholar]
- Lee, J.; Lozano-Ruiz, B.; Yang, F.M.; Fan, D.D.; Shen, L.; González-Navajas, J.M. The Multifaceted Role of Th1, Th9, and Th17 Cells in Immune Checkpoint Inhibition Therapy. Front. Immunol. 2021, 12, 625667. [Google Scholar] [CrossRef]
- Lei, X.; Lei, Y.; Li, J.K.; Du, W.X.; Li, R.G.; Yang, J.; Tan, H.B. Immune cells within the tumor microenvironment: Biological functions and roles in cancer immunotherapy. Cancer Lett. 2020, 470, 126–133. [Google Scholar] [CrossRef]
- Galli, F.; Aguilera, J.V.; Palermo, B.; Markovic, S.N.; Nisticò, P.; Signore, A. Relevance of immune cell and tumor microenvironment imaging in the new era of immunotherapy. J. Exp. Clin. Cancer Res. 2020, 39, 89. [Google Scholar] [CrossRef]
- Jeske, S.S.; Weissinger, S.E.; Veit, J.A.; Brunner, C.; Huber, U.; Theodoraki, M.N.; Doescher, J. Treatment-induced changes of lymphocyte subsets in patients with adenoid cystic carcinoma of the head and neck. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 1465–1473. [Google Scholar] [CrossRef]
- Massimo, A.; Jun-Li, L.; Sergei, G.; Sergei, N.; Michael, K. Prostate Cancer—NCCN Evidence Blocks. Version 2.2017. Am. Cancer Soc. 2017, 464, 302–305. [Google Scholar]
- Borros, A. Tumor microenvironment. Medicina 2020, 56, 1–21. [Google Scholar]
- Tsou, P.; Katayama, H.; Ostrin, E.J.; Hanash, S.M. The emerging role of b cells in tumor immunity. Cancer Res. 2016, 76, 5591–5601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qing, Z.; Jiacheng, B.; Xiaodong, Z.; Yongyan, C.; Hua, W.; Wenyong, W.; Zhengguang, W.; Wu, Q.; Peng, H.; Wei, H.; et al. Blockade of the checkpoint receptor TIGIT prevents NK cell exhaustion and elicits potent anti-tumor immunity. Nat. Immunol. 2018, 19, 723–732. [Google Scholar]
- Kim, J.; Bae, J.S. Tumor-associated macrophages and neutrophils in tumor microenvironment. Mediators Inflamm. 2016, 2016, 6058147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zilionis, R.; Engblom, C.; Pfirschke, C.; Savova, V.; Zemmour, D.; Saatcioglu, H.D.; Klein, A.M. Single cell transcriptomics of human and mouse lung cancers reveals conserved myeloid populations across individuals and species. Immunity 2019, 50, 1317–1334. [Google Scholar] [CrossRef]
- Verneau, J.; Sautés-Fridman, C.; Sun, C.M. Dendritic cells in the tumor microenvironment: Prognostic and theranostic impact. Semin. Immunol. 2020, 48, 101410. [Google Scholar] [CrossRef]
- Wu Lingyun, S.S.; Singh Rakesh, K. Neutrophils in the tumor microenvironment. Adv. Exp. Med. Biol. 2020, 1224, 41–52. [Google Scholar]
- Ishii, G.; Ochiai, A.; Neri, S. Phenotypic and functional heterogeneity of cancer-associated fibroblast within the tumor microenvironment. Adv. Drug Deliv. Rev. 2016, 99, 186–196. [Google Scholar] [CrossRef]
- Monteran, L.; Erez, N. The dark side of fibroblasts: Cancer-associated fibroblasts as mediators of immunosuppression in the tumor microenvironment. Front Immunol. 2019, 10, 1–15. [Google Scholar] [CrossRef] [Green Version]
- LeBleu, V.S.; Kalluri, R. A peek into cancer-associated fibroblasts: Origins, functions and translational impact. DMM Dis. Model Mech. 2018, 11, dmm029447. [Google Scholar] [CrossRef] [Green Version]
- Wu, Q.; Li, B.; Sun, S.; Sun, S. Unraveling Adipocytes and Cancer Links: Is There a Role for Senescence? Front. Cell Dev. Biol. 2020, 8, 1–7. [Google Scholar] [CrossRef]
- Wu, Q.; Li, B.; Li, Z.; Li, J.; Sun, S.; Sun, S. Cancer-associated adipocytes: Key players in breast cancer progression. J. Hematol. Oncol. 2019, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Li, B.; Li, J.; Sun, S.; Yuan, J.; Sun, S. Cancer-associated adipocytes as immunomodulators in cancer. Biomark. Res. 2021, 9, 2. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Patel, S.; Tcyganov, E.; Gabrilovich, D.I. The Nature of Myeloid-Derived Suppressor Cells in the Tumor Microenvironment. Trends Immunol. 2016, 37, 208–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, V.; Cheng, P.; Condamine, T.; Mony, S.; Languino, L.R.; McCaffrey, J.C.; Gabrilovich, D.I. CD45 Phosphatase Inhibits STAT3 Transcription Factor Activity in Myeloid Cells and Promotes Tumor-Associated Macrophage Differentiation. Physiol. Behav. 2017, 176, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Duan, Q.; Zhang, H.; Zheng, J.; Zhang, L. Turning Cold into Hot: Firing up the Tumor Microenvironment. Trends Cancer 2020, 6, 605–618. [Google Scholar] [CrossRef]
- van der Woude, L.L.; Gorris, M.A.J.; Halilovic, A.; Figdor, C.G.; de Vries, I.J.M. Migrating into the Tumor: A Roadmap for T Cells. Trends Cancer 2017, 3, 797–808. [Google Scholar] [CrossRef]
- Ros, X.R.; Vermeulen, L. Turning Cold Tumors Hot by Blocking TGF-β. Trends Cancer 2018, 4, 335–337. [Google Scholar] [CrossRef]
- Soysal, S.D.; Tzankov, A.; Muenst, S.E. Role of the Tumor Microenvironment in Breast Cancer. Pathobiology 2015, 82, 142–152. [Google Scholar] [CrossRef]
- Yang, S.; Liu, T.; Nan, H.; Wang, Y.; Chen, H.; Zhang, X.; Liang, G. Comprehensive analysis of prognostic immune-related genes in the tumor microenvironment of cutaneous melanoma. J. Cell Physiol. 2020, 235, 1025–1035. [Google Scholar] [CrossRef]
- Vuong, L.; Kotecha, R.R.; Voss, M.H.; Hakimi, A.A. Tumor microenvironment dynamics in clear-cell renal cell carcinoma. Cancer Discov. 2019, 9, 1349–1357. [Google Scholar] [CrossRef] [Green Version]
- Wojas-Krawczyk, K.; Krawczyk, P. Rozwój koncepcji przeciwnowotworowej immunoterapii. Onkol. W Prakt. Klin. 2015, 11, 69–75. [Google Scholar]
- Wojas-Krawczyk, K.; Kubiatowski, T. Imperfect predictors for lung cancer immunotherapy—A field for further research. Front Oncol. 2020, 10, 568174. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat. Rev. Cancer 2016, 16, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.-Y.; Garon, E.B. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Grzywnowicz, M.; Giannopoulos, K. W Układzie Immunologicznym Oraz Nowotworach. Acta Haematol. Pol. 2012, 43, 132–145. [Google Scholar] [CrossRef]
- Buchan, S.L.; Fallatah, M.; Thirdborough, S.M.; Taraban, V.Y.; Rogel, A.; Thomas, L.J.; Al-Shamkhani, A. Pd-1 blockade and cd27 stimulation activate distinct transcriptional programs that synergize for CD8þ T-cell–driven antitumor immunity. Clin. Cancer Res. 2018, 24, 2383–2394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, D.T.; Bac, N.D.; Nguyen, K.H.; Tien, N.L.B.; Van, T.V.; Nga, V.T.; Thimiri Govinda Raj, D.B. An update on anti-CD137 antibodies in immunotherapies for cancer. Int. J. Mol. Sci. 2019, 20, 1822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, K.; Wu, Y.H.; Song, Y.; Yu, B. Indoleamine 2, 3-dioxygenase 1 (IDO1) inhibitors in clinical trials for cancer immunotherapy. J. Hematol. Oncol. 2021, 14, 1822. [Google Scholar] [CrossRef]
- Carpenter, B.; Lebon, G. Human adenosine A2A receptor: Molecular mechanism of ligand binding and activation. Front Pharmacol. 2017, 8, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Cai, L.; Sun, Y.; Wang, K.; Guan, W.; Yue, J.; Li, J.; Wang, L. The Better Survival of MSI Subtype Is Associated With the Oxidative Stress Related Pathways in Gastric Cancer. Front Oncol. 2020, 10, 1–15. [Google Scholar] [CrossRef]
- Malhotra, P.; Anwar, M.; Nanda, N.; Kochhar, R.; Wig, J.D.; Vaiphei, K.; Mahmood, S. Alterations in K-ras, APC and p53-multiple genetic pathway in colorectal cancer among Indians. Tumor Biol. 2013, 34, 1901–1911. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cellular Components | Non-Cellular Components |
|---|---|
| T lymphocytes | Extra-cellular matrix (ECM) |
| B lymphocytes | IFN γ |
| Macrophages | Tumor necrosis factor (TNF) |
| Adipocytes | Growth factors (PDGF, EGF, NGF, TGFα, β) |
| Neutrophils | IL-1, IL-2, IL-3, IL-4, IL-5, IL-6, IL-12, IL-15, IL-18, IL-37, IL-23, IL-27, IL-7, IL-37, IL-31, IL-10 |
| Cancer associated fibroblasts (CAF) | Chemokines (MIP, CCL11, CCL5, MCP, IL-8, IL-16, CCL9) |
| Endothelial cells | Exosomes |
| Cancer cells | Apoptotic bodies |
| NK cells | |
| Dendritic cells (DC) |
| Cell Type | Natural Function | Function in Tumor Microenvironment | Produced Substances | |
|---|---|---|---|---|
| of Anti-Tumor Activity | of Pro-Tumor Activity | |||
| HELPER T CELLS | Th1-stimulates dendritic and NK cells. Attracts T lymphocytes. | Th1- blocked by IL-4, IL-10, TGF-β, Treg, Th2, M2 Th2-. Inhibition of Th1. Stimulation of M2 population of macrophages. | TNF-α, IL-12, IL-17,IL-18, IL-21, IL-27. | Th17 lymphocytes can transform into Treg lymphocytes. |
| REGULATORY T CELLS | Protection against autoimmunity from autoreactive T lymphocytes. | Stimulating immune tolerance. Immunosuppression. Inhibition of the immune response. | IL-10, TGF-β, adenosine, PGE2, IL-35. | TGF-β, IL-2, IL-10, IL-35. |
| CYTOTOXIC T CELLS | Cytotoxic. Stimulation of other immune cells to infiltrate the tumor. | Inhibition of the cytotoxic function by binding to PD-L1. | Perforins. Granzymes IL-2, TNF-α, IFN-γ. | ------ |
| MACROPHAGES | Destruction, phagocytosis of abnormal cells. Inducing inflammation. | TAM2: Protumor. Inhibition of the inflammatory process. | IFN-γ, IL-12, GM-CSF. | IL-10, TGF-β, EGF, FGF, VEGF, MMP CCL2, CCL5, CCL3, CCL8, CCL22. |
| NEUTROPHILS | Phagocytosis. ADCC. Stimulation of CD8 + lymphocytes, NK cells. | N1: Phagocytosis. Stimulation of apoptosis N2: Angiogenesis. Stimulation of the inflammatory process in the tumor. | TNF-α, IFN- γ. | TGF-β, MPO, MMP9, HGF, VEGF |
| B CELLS | Presenting antigens. Complement activation. Antibody production. | Supporting angiogenesis. -inhibition of anti-cancer activities. Stimulation of Treg. | IL-2. | IL-10, TGF-β. |
| CANCER ASSOCIATED FIBROBLASTS (CAF) | -------- | Secreting growth factors. Causing inflammation. | -------- | CXCL1, CXCL2, CXCL3, CXCL12, CCL2, CCL5, CCL17, IL-8, GM-CSF TGF-β, IL-6, exosomes, HGF, IGF, CTGF. |
| NATURAL KILLER CELLS (NK) | Cytotoxic. Immune supervision. Stimulation of T and DC lymphocytes. | -------- | IL-2, IL-6, 12, 15, IFN-γ, TNF-α, GM-CSF, CCL-5. | -------- |
| DENDRITIC CELLS (DC) | Presentation of antigens. Influences the differentiation of helper and regulatory lymphocytes. Cytotoxic function. | Presence on the surface of PD-L1, Impaired antigen presentation, maturation and tumor infiltration. | IL-6, IL-8, IL-12, IL-15. | -------- |
| CANCER ASSOCIATED ADIPOCYTES (CAA) | Production and storage of simple fats (triglycerides). | Secretion of adipokines. They cause changes in the metabolism of cancer cells and remodel the ECM. | -------- | Adipokines: leptin, hepatocyte growth factors IL-1β. |
| MYELOID-DERIVED SUPPRESSOR CELLS (MDSC) | -------- | Suppression of the immune response. | -------- | IL-4, CCL3, CCL4, CCL5, PGE2, NO. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bożyk, A.; Wojas-Krawczyk, K.; Krawczyk, P.; Milanowski, J. Tumor Microenvironment—A Short Review of Cellular and Interaction Diversity. Biology 2022, 11, 929. https://doi.org/10.3390/biology11060929
Bożyk A, Wojas-Krawczyk K, Krawczyk P, Milanowski J. Tumor Microenvironment—A Short Review of Cellular and Interaction Diversity. Biology. 2022; 11(6):929. https://doi.org/10.3390/biology11060929
Chicago/Turabian StyleBożyk, Aleksandra, Kamila Wojas-Krawczyk, Paweł Krawczyk, and Janusz Milanowski. 2022. "Tumor Microenvironment—A Short Review of Cellular and Interaction Diversity" Biology 11, no. 6: 929. https://doi.org/10.3390/biology11060929
APA StyleBożyk, A., Wojas-Krawczyk, K., Krawczyk, P., & Milanowski, J. (2022). Tumor Microenvironment—A Short Review of Cellular and Interaction Diversity. Biology, 11(6), 929. https://doi.org/10.3390/biology11060929