
Cytokine Profiling among Children with Multisystem Inflammatory Syndrome versus Simple COVID-19 Infection: A Study from Northwest Saudi Arabia

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Biochemical Analysis
2.3.1. Basic Investigations
2.3.2. Serum Indices of Tissue Injury
2.3.3. Cytokine
2.4. Mid-Term Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
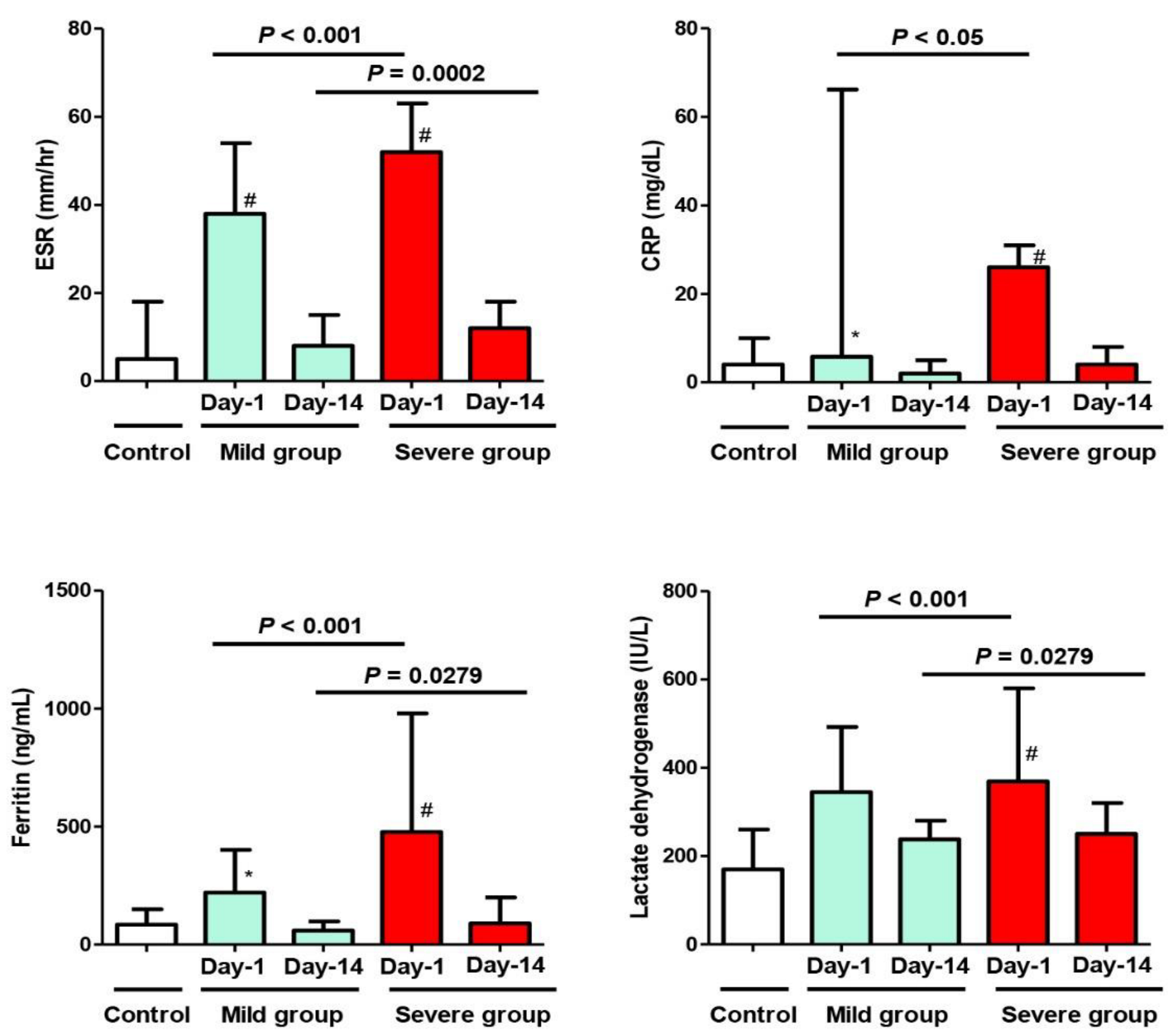
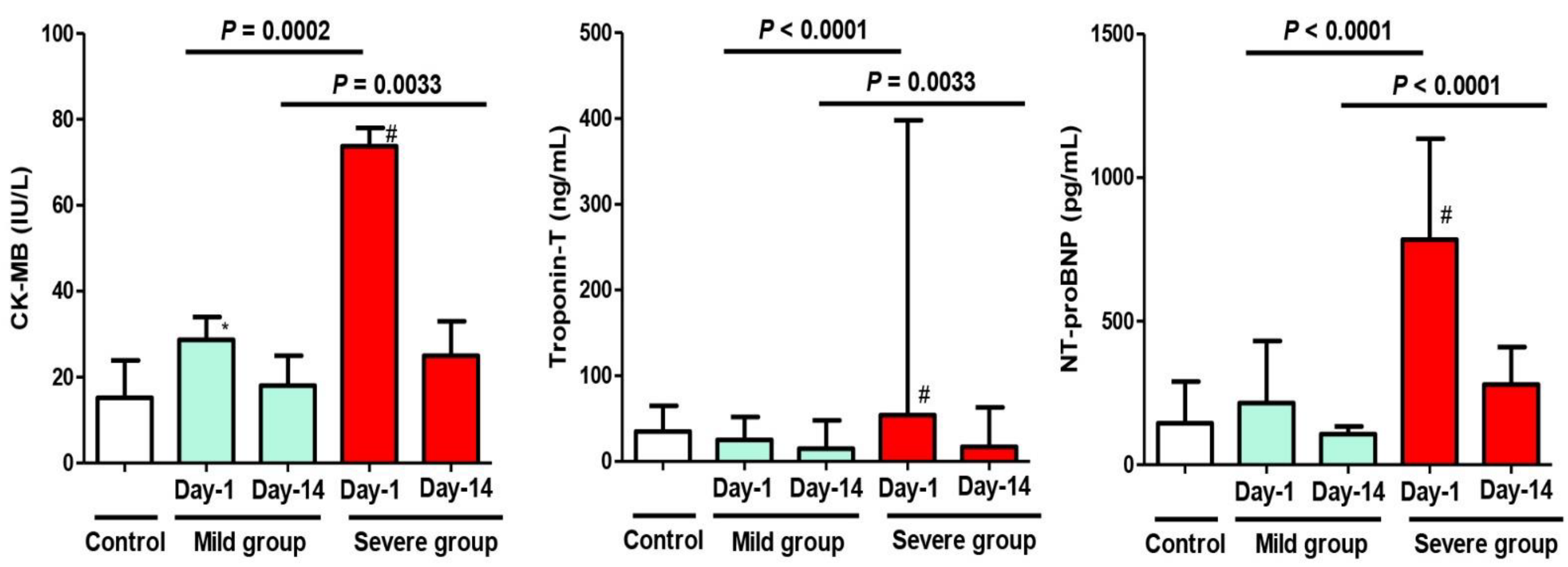
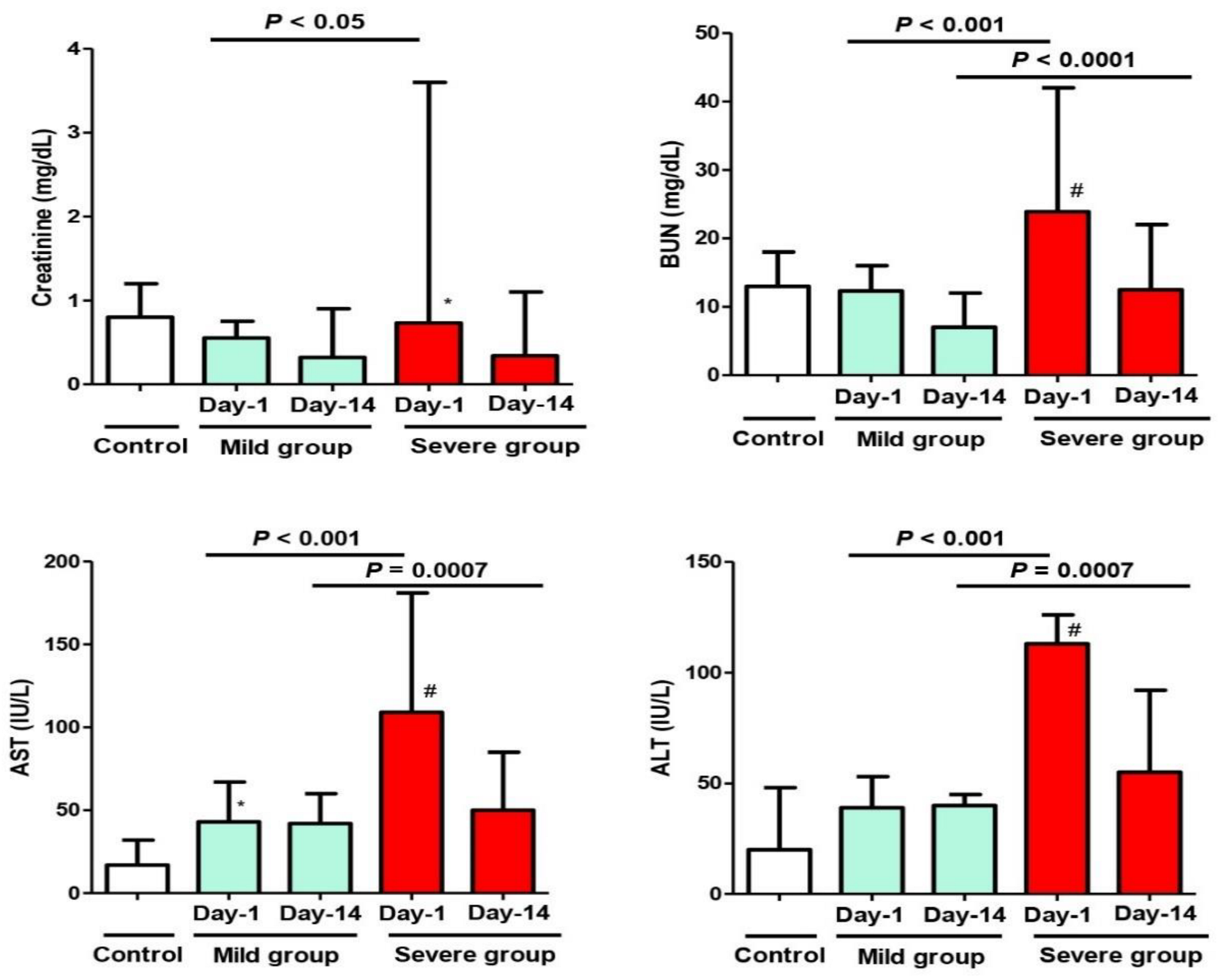
3.2. Laboratory Investigations
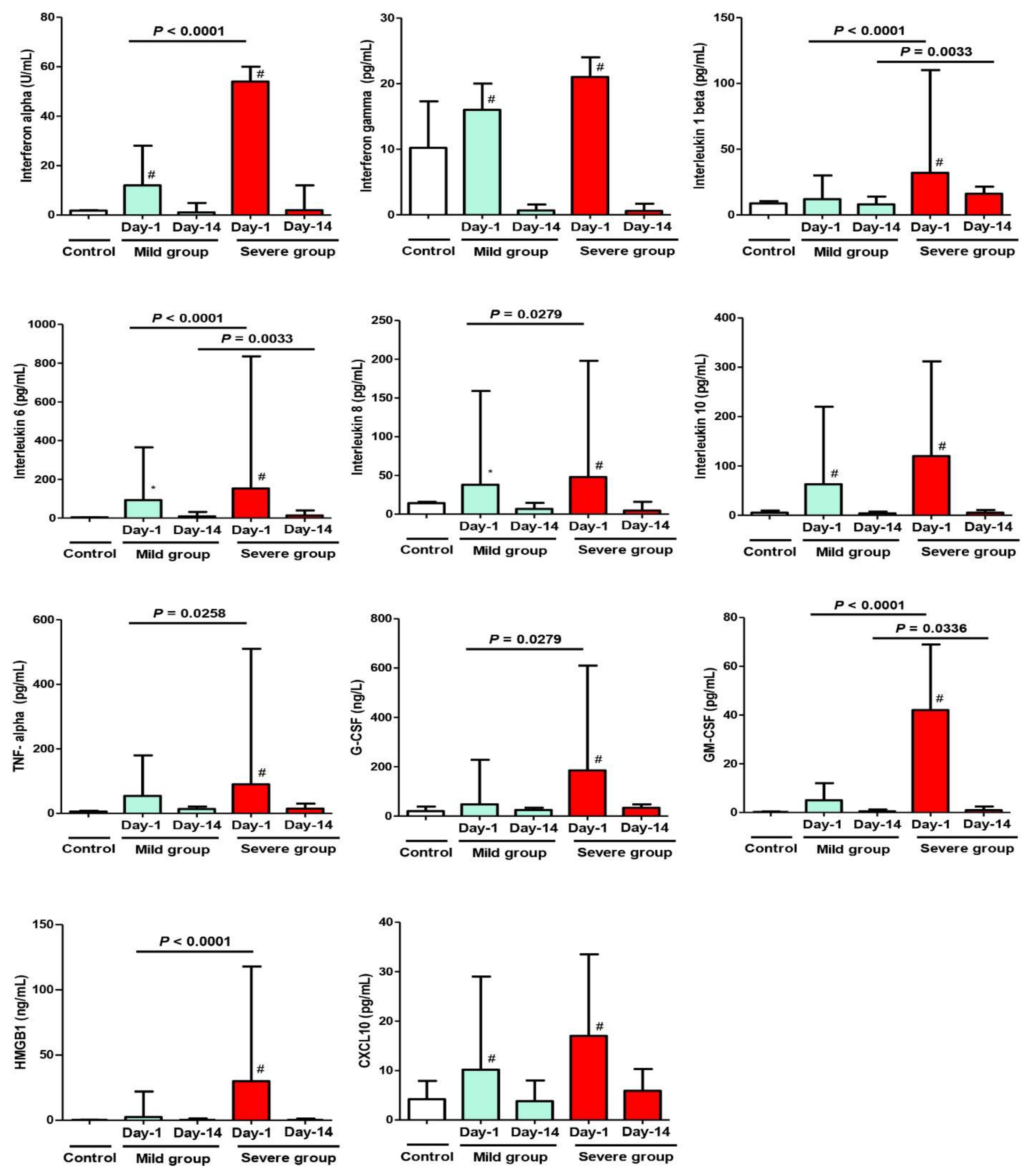
3.3. Cytokine Analysis
3.4. Follow-Up and Patients’ Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bourkhissi, L.; Fakiri, K.E.; Nassih, H.; Qadiry, R.E.; Bourrahouat, A.; Ait Sab, I.; Rada, N.; Draiss, G.; Bouskraoui, M. Laboratory abnormalities in children with novel Coronavirus Disease 2019. Clin. Med. Insights Pediatr. 2020, 14, 1179556520955177. [Google Scholar] [CrossRef] [PubMed]
- Polidoro, R.B.; Hagan, R.S.; de Santis Santiago, R.; Schmidt, N.W. Overview: Systemic inflammatory response derived from lung injury caused by SARS-CoV-2 Infection explains severe outcomes in COVID-19. Front. Immunol. 2020, 11, 1626. [Google Scholar] [CrossRef] [PubMed]
- Liao, M.; Liu, Y.; Yuan, J.; Wen, Y.; Xu, G.; Zhao, J.; Cheng, L.; Li, J.; Wang, X.; Wang, F.; et al. Single-cell landscape of bronchoalveolar immune cells in patients with COVID-19. Nat. Med. 2020, 26, 842–844. [Google Scholar] [CrossRef]
- Henry, B.M.; Lippi, G.; Plebani, M. Laboratory abnormalities in children with novel coronavirus disease 2019. Clin. Chem. Lab. Med. 2020, 58, 1135–1138. [Google Scholar] [CrossRef] [Green Version]
- Epidemiology Working Group for NCIP Epidemic Response; Chinese Center for Disease Control and Prevention. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar]
- European Centre for Disease Prevention and Control. Rapid Risk Assessment: Paediatric Inflammatory Multisystem Syndrome and SARS-CoV-2 Infection in Children. 2022. Available online: https://www.ecdc.europa.eu/en/news-events/webinar-multisystem-inflammatory-syndrome-children-mis-c (accessed on 5 March 2022).
- Royal College of Pediatrics and Child Health. Guidance: Pediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19—Guidance for Clinicians. 2020. Available online: https://www.rcpch.ac.uk/resources/paediatric-multisystem-inflammatory-syndrome-temporally-associated-COVID-19-pims-guidance (accessed on 5 November 2021).
- World Health Organization. Multisystem Inflammatory Syndrome in Children and Adolescents with COVID-19. 2020. Available online: https://www.who.int/publications/i/item/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-COVID-19 (accessed on 14 October 2021).
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 2020, 395, 1607–1608. [Google Scholar] [CrossRef]
- Cheung, E.W.; Zachariah, P.; Gorelik, M.; Boneparth, A.; Kernie, S.G.; Orange, J.S.; Milner, J.D. Multisystem inflammatory syndrome related to COVID-19 in previously healthy children and adolescents in New York city. JAMA 2020, 324, 294–296. [Google Scholar] [CrossRef]
- Jones, V.G.; Mills, M.; Suarez, D.; Hogan, C.A.; Yeh, D.; Segal, J.B.; Nguyen, E.L.; Barsh, G.R.; Maskatia, S.; Mathew, R. COVID-19 and Kawasaki Disease: Novel Virus and Novel Case. Hosp. Pediatr. 2020, 10, 537–540. [Google Scholar] [CrossRef]
- Toubiana, J.; Poirault, C.; Corsia, A.; Bajolle, F.; Fourgeaud, J.; Angoulvant, F.; Debray, A.; Basmaci, R.; Salvador, E.; Biscardi, S.; et al. Kawasaki-like multisystem inflammatory syndrome in children during the COVID-19 pandemic in Paris, France: Prospective observational study. BMJ 2020, 369, m2094. [Google Scholar] [CrossRef]
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.E.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. PIMS-TS Study Group and EUCLIDS and PERFORM Consortia. Clinical Characteristics of 58 Children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA 2020, 324, 259–269. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Belhadjer, Z.; Méot, M.; Bajolle, F.; Khraiche, D.; Legendre, A.; Abakka, S.; Auriau, J.; Grimaud, M.; Oualha, M.; Beghetti, M.; et al. Acute heart failure in multisystem inflammatory syndrome in children in the context of global SARS-CoV-2 pandemic. Circulation 2020, 142, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Hennon, T.R.; Yu, K.O.A.; Penque, M.D.; Abdul-Aziz, R.; Chang, A.C.; McGreevy, M.B.; Pastore, J.V.; Prout, A.J.; Schaefer, B.A.; Alibrahim, O.S.; et al. COVID-19 associated multisystem inflammatory syndrome in children (MIS-C) guidelines; revisiting the Western New York approach as the pandemic evolves. Prog. Pediatr. Cardiol. 2021, 62, 101407. [Google Scholar] [CrossRef] [PubMed]
- Yagnam, R.F.; Izquierdo, C.G.; Villena, M.R.; González, M.C.; Drago-T, M. Pediatric Multisystemic inflammatory syndrome temporarily associated with COVID-19: Clinical characteristics and management in a Pediatric Critical Care Unit. Andes. Pediatr. 2021, 92, 395–405. [Google Scholar]
- Belot, A.; Antona, D.; Renolleau, S.; Javouhey, E.; Hentgen, V.; Angoulvant, F.; Delacourt, C.; Iriart, X.; Ovaert, C.; Bader-Meunier, B.; et al. SARS-CoV-2-related paediatric inflammatory multisystem syndrome, an epidemiological study, France, 1 March to 17 May 2020. Eurosurveillance 2020, 25, 2001010. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, S.; Aydin, S.I.; Derespina, K.R.; Bansal, P.B.; Kowalsky, S.; Trachtman, R.; Gillen, J.K.; Perez, M.M.; Soshnick, S.H.; Conway, E.E., Jr.; et al. Multisystem inflammatory syndrome in children associated with severe acute respiratory syndrome Coronavirus 2 infection (MIS-C): A Multi-institutional study from New York City. J. Pediatr. 2020, 224, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Licciardi, F.; Pruccoli, G.; Denina, M.; Parodi, E.; Taglietto, M.; Rosati, S.; Montin, D. SARS-CoV-2-Induced Kawasaki-Like Hyperinflammatory syndrome: A novel COVID phenotype in children. Pediatrics 2020, 146, e20201711. [Google Scholar] [CrossRef]
- Carlin, R.F.; Fischer, A.M.; Pitkowsky, Z.; Abel, D.; Sewell, T.B.; Landau, E.G.; Caddle, S.; Robbins-Milne, L.; Boneparth, A.; Milner, J.D.; et al. Discriminating multisystem inflammatory syndrome in children requiring treatment from common febrile conditions in outpatient settings. J. Pediatr. 2021, 229, 26–32.e2. [Google Scholar] [CrossRef]
- Gupta, S.; Chopra, N.; Singh, A.; Gera, R.; Chellani, H.; Pandey, R.; Arora, B.S. Unusual clinical manifestations and outcome of multisystem inflammatory syndrome in children (MIS-C) in a tertiary care hospital of North India. J. Trop. Pediatr. 2021, 67, fmaa127. [Google Scholar] [CrossRef]
- Antúnez-Montes, O.Y.; Escamilla, M.I.; Figueroa-Uribe, A.F.; Arteaga-Menchaca, E.; Lavariega-Saráchaga, M.; Salcedo-Lozada, P.; Melchior, P.; de Oliveira, R.B.; Tirado Caballero, J.C.; Redondo, H.P.; et al. COVID-19 and multisystem inflammatory syndrome in Latin American children: A multinational study. Pediatr. Infect. Dis. J. 2021, 40, e1–e6. [Google Scholar] [CrossRef]
- Tang, J.; Randolph, A.G.; Novak, T.; Walker, T.C.; Loftis, L.L.; Zinter, M.S.; Irby, K.; Khurana, S. Systemic and lower respiratory tract immunity to SARS-CoV-2 Omicron and variants in pediatric severe COVID-19 and Mis-C. Vaccines 2022, 10, 270. [Google Scholar] [CrossRef] [PubMed]
- Hirabara, S.M.; Serdan, T.D.A.; Gorjao, R.; Masi, L.N.; Pithon-Curi, T.C.; Covas, D.T.; Curi, R.; Durigon, E.L. SARS-CoV-2 variants: Differences and potential of immune evasion. Front. Cell Infect. Microbiol. 2022, 11, 781429. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Figueroa, E.I.; Santos, R.; Simpson, S.; Garg, P. Incomplete Kawasaki disease in a child with COVID-19. Indian Pediatr. 2020, 57, 680–681. [Google Scholar] [CrossRef] [PubMed]
- Deza Leon, M.P.; Redzepi, A.; McGrath, E.; Abdel-Haq, N.; Shawaqfeh, A.; Sethuraman, U.; Tilford, B.; Chopra, T.; Arora, H.; Ang, J.; et al. COVID-19-associated pediatric multisystem inflammatory syndrome. J. Pediatric Infect. Dis. Soc. 2020, 9, 407–408. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.P.; Izquierdo, G.; Acuña, M.; Pavez, D.; Reyes, F.; Fritis, A.; González, R.; Rivacoba, C.; Contardo, V.; Tapia, L.I. Multisystem inflammatory syndrome in children (MIS-C): Report of the clinical and epidemiological characteristics of cases in Santiago de Chile during the SARS-CoV-2 pandemic. Int. J. Infect. Dis. 2020, 100, 75–81. [Google Scholar] [CrossRef]
- Kernan, K.F.; Carcillo, J.A. Hyperferritinemia and inflammation. Int. Immunol. 2017, 29, 401–409. [Google Scholar] [CrossRef]
- Sperotto, F.; Friedman, K.G.; Son, M.B.F.; VanderPluym, C.J.; Newburger, J.W.; Dionne, A. Cardiac manifestations in SARS-CoV-2-associated multisystem inflammatory syndrome in children: A comprehensive review and proposed clinical approach. Eur. J. Pediatr. 2021, 180, 307–322. [Google Scholar] [CrossRef]
- Theocharis, P.; Wong, J.; Pushparajah, K.; Mathur, S.K.; Simpson, J.M.; Pascall, E.; Cleary, A.; Stewart, K.; Adhvaryu, K.; Savis, A.; et al. Multimodality cardiac evaluation in children and young adults with multisystem inflammation associated with COVID-19. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 896–903. [Google Scholar] [CrossRef]
- Elshazli, R.M.; Toraih, E.A.; Elgaml, A.; El-Mowafy, M.; El-Mesery, M.; Amin, M.N.; Hussein, M.H.; Killackey, M.T.; Fawzy, M.S.; Kandil, E. Diagnostic and prognostic value of hematological and immunological markers in COVID-19 infection: A meta-analysis of 6320 patients. PLoS ONE 2020, 15, e0238160. [Google Scholar] [CrossRef]
- Feldstein, L.R.; Tenforde, M.W.; Friedman, K.G.; Newhams, M.; Rose, E.B.; Dapul, H.; Soma, V.L.; Maddux, A.B.; Mourani, P.M.; Bowens, C.; et al. Overcoming COVID-19 Investigators. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA 2021, 325, 1074–1087. [Google Scholar] [CrossRef]
- Lippi, G.; Lavie, C.J.; Sanchis-Gomar, F. Cardiac troponin I in patients with coronavirus disease 2019 (COVID-19): Evidence from a meta-analysis. Prog. Cardiovasc. Dis. 2020, 63, 390–391. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.; Hu, X.C.; Fan, M.X.; Chen, J.; Cheng, Q.R.; Li, Z.; Hu, Z.L.; Ge, X.H. Analysis of clinical characteristics of 66 pediatric patients with B.1.617.2 (Delta) variant of COVID-19. World J. Pediatr. 2022, 18, 343–349. [Google Scholar] [CrossRef]
- Matsubara, D.; Kauffman, H.L.; Wang, Y.; Calderon-Anyosa, R.; Nadaraj, S.; Elias, M.D.; White, T.J.; Torowicz, D.L.; Yubbu, P.; Giglia, T.M.; et al. Echocardiographic findings in pediatric multisystem inflammatory syndrome associated with COVID-19 in the United States. J. Am. Coll. Cardiol. 2020, 76, 1947–1961. [Google Scholar] [CrossRef] [PubMed]
- García-Salido, A.; de Carlos Vicente, J.C.; Belda Hofheinz, S.; Balcells Ramírez, J.; Slöcker Barrio, M.; Leóz Gordillo, I.; Hernández Yuste, A.; Guitart Pardellans, C.; Cuervas-Mons Tejedor, M.; Huidobro Labarga, B.; et al. Severe manifestations of SARS-CoV-2 in children and adolescents: From COVID-19 pneumonia to multisystem inflammatory syndrome: A multicenter study in pediatric intensive care units in Spain. Crit. Care 2020, 24, 666. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J.Y.; Oster, M.E.; Godfred-Cato, S.E.; Bryant, B.; Datta, S.D.; Campbell, A.P.; Leung, J.W.; Tsang, C.A.; Pierce, T.J.; Kennedy, J.L.; et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: A retrospective surveillance study. Lancet Child Adolesc. Health 2021, 5, 323–331. [Google Scholar] [CrossRef]
- Liu, X.; Shi, S.; Xiao, J.; Wang, H.; Chen, L.; Li, J.; Han, K. Prediction of the severity of the Coronavirus disease and its adverse clinical outcomes. Jpn. J. Infect. Dis. 2020, 73, 404–410. [Google Scholar] [CrossRef]
- Lucas, C.; Wong, P.; Klein, J.; Castro, T.B.R.; Silva, J.; Sundaram, M.; Ellingson, M.K.; Mao, T.; Oh, J.E.; Israelow, B.; et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature 2020, 584, 463–469. [Google Scholar] [CrossRef]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; Péré, H.; Charbit, B.; Bondet, V.; Chenevier-Gobeaux, C.; et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 2020, 369, 718–724. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control Group (Simple COVID-19) (n = 30) | Group A (Mild MIS-C) (n = 33) | Group B (Severe MIS-C) (n = 27) | p Value $ |
|---|---|---|---|---|
| Age (years) | 6.8 ± 4.1 | 7.2 ± 4.1 | 6.1 ± 4.8 | 0.6199 |
| Sex -Male -Female | 17 (56.6%) 13 (43.3%) | 15 (45.5%) 18 (54.5%) | 16 (59.3%) 11 (40.7%) | 0.1552 |
| Ethnicity -Saudi -Non-Saudi | 20 (66.7%) 10 (33.3%) | 20 (60.6%) 13 (39.4%) | 18 (66.7%) 9 (33.3%) | 0.3923 |
| Clinical presentations Fever Respiratory Gastrointestinal Rash Shock Conjunctivitis Lymphadenopathy | 25 (83.3%) 17 (56.6%) 16 (53.3%) 4 (13.3%) 0 (0%) 23 (76.6%) 2 (6.6%) | 33 (100%) 23 (69.7%) * 27 (81.8%) * 5 (15.2%) 0 (0%) 25 (75.8%) 3 (9.1%) | 27 (100%) 27 (100%) #,$ 21 (77.7%) * 4 (14.8%) 22 (81.5%) #,$ 23 (85.2%) 2 (7.4%) | 1.0000 0.0011 $ 0.7357 0.7928 <0.0001 $ 0.3143 0.7237 |
| Weight (kg) | 9.53 ± 3.1 | 10.52 ± 3.9 | 8.87 ± 2.9 | 0.0734 |
| Heart rate (beats/min) | 110.5 ± 9.23 | 113.43 ± 12.14 | 122.6 ± 15.93 #,$ | 0.05 $ |
| Respiratory rate (breaths/min) | 28.14 ± 9.8 | 34.23 ± 8.14 | 47.96 ± 11.58 #,$ | <0.0001 $ |
| Duration between SARS-CoV-2 infection and MIS-C diagnosis (days) | - | 6.1 ± 2.4 | 4.5 ± 1.7 | 0.002 $ |
| Length of hospital/± PICU stay (days) | - | 3.8 ± 1.3 (Range: 3–6) | 15.5 ± 2.8 (Range: 6–17.4) | <0.0001 $ |
| Hematology (median and IQR) | ||||
| Hemoglobin (gm/dL) (reference, 11.5–15.6) | 11.6 (9.2–13.3) | 10.6 (8.4–12.9) | 9.9 (8.6–10.9) # | 0.4666 |
| WBC count (109/L) (reference, 4.5–13.5) | 11.04 (5.2–13.1) | 14.4 (6.1–20.1) * | 18.3 (14.3– 20.2) #,$ | <0.01 $ |
| Lymphocytes (109/L) (reference, 2–10) | 1.2 (0.9–2.3) | 0.8 (0.6–1.7) * | 0.8 (0.7–0.9) # | 0.9941 |
| Platelet count (109/L) (reference, 140–450) | 155 (145–490) | 165 (112–247) # | 139 (114–246) # | 0.4666 |
| INR (seconds) (reference, ≤ 1.1) | 0.7 (0.4–1.0) | 0.8 (0.2–1.1) | 1.2 (0.9–1.3) #,$ | <0.001$ |
| Variable | Control Group (n = 30) Median (IQR) | Group A (Mild) (n = 33) Median (IQR) | Group B (Severe) (n = 27) Median (IQR) | p Value $ |
|---|---|---|---|---|
| Inflammatory Markers | ||||
| ESR (mm/hr) (reference, 1–20) | 5 (3–18) | 38 (20–54) * | 52 (38–63) #,$ | <0.001 $ |
| CRP (mg/dL) (reference, ≤5) | 4 (2–10) | 5.8 (3.14–36.15) * | 26 (13–31) # | <0.05 $ |
| Ferritin (ng/mL) (reference, ≤150) | 85 (70–150) | 220 (160–402) * | 477 (281–980) #,$ | <0.001 $ |
| Lactate dehydrogenase (IU/L) (reference, 120–260) | 170 (140–260) | 345 (265–492) | 369 (287–580) #,$ | <0.001 $ |
| Cardiac markers | ||||
| CK-MB (IU/L) (reference, ≤25) | 15.2 (5.8–23.9) | 28.7 (24.8–34) * | 73.7 (30.6–78) #,$ | 0.0002 $ |
| Troponin-T (ng/mL) (reference, 20–60) | 35 (25–65) | 25 (17–52) | 54 (35–398) #,$ | <0.0001 $ |
| NT-proBNP (pg/mL) (reference, <300) | 90 (145–290) | 154 (215–431) | 784 (631–1135) #,$ | <0.0001 $ |
| Biochemistry | ||||
| Creatinine (mg/dL) (reference, 0.6–1.1) | 0.8 (0.5–1.2) | 0.55 (0.42–0.75) | 0.73 (0.2–3.6) *,$ | <0.05 $ |
| BUN (mg/dL) (reference, 8–20) | 13 (9–18) | 12.3 (9–16) | 23.9 (20–42) #,$ | <0.001 $ |
| AST (IU/L) (reference, 10–37) | 17 (12–32) | 43 (28–67) * | 109 (76–181) #,$ | <0.001 $ |
| ALT (IU/L) (reference, 16–61) | 20 (15–48) | 39 (17–53) | 113 (46–126) #,$ | <0.001 $ |
| Variable | Group A (Mild) (n = 33) Median (IQR) | Group B (Severe) (n = 27) Median (IQR) | p Value # |
|---|---|---|---|
| Inflammatory Markers | |||
| ESR (mm/hr) (reference, 1–20) | 8 (6–15) | 12 (10–18) | 0.0002 # |
| CRP (mg/dL) (reference, ≤5) | 2 (1–5) | 4 (0–8) | 0.4666 |
| Ferritin (ng/mL) (reference, ≤150) | 60 (20–98) | 90 (30–200) | 0.0279 # |
| LDH (IU/L) (reference, 120–260) | 238 (170–280) | 250 (200–320) | 0.0279 # |
| Cardiac markers | |||
| CK-MB (IU/L) (reference, ≤25) | 18 (11–25) | 25 (15–33) | 0.0033 # |
| Troponin-T (ng/mL) (reference, 20–60) | 15 (9–48) | 17 (15–63) | 0.0033 # |
| NT-proBNP (pg/mL) (reference, <300) | 107 (60–134) | 280 (200–410) | <0.0001 # |
| Biochemistry | |||
| Creatinine (mg/dL) (reference, 0.6–1.1) | 0.32 (0.2–0.9) | 0.34 (0.2–1.1) | 0.0625 |
| BUN (mg/dL) (reference, 8–20) | 7 (4.5–12) | 12.5 (10–22) | <0.0001 # |
| AST (IU/L) (reference, 10–37) | 42 (27–60) | 50 (46–85) | 0.0007 # |
| ALT (IU/L) (reference, 16–61) | 40 (15–45) | 55 (36–92) | 0.0007 # |
| Variable | Control Group (n = 30) Median (IQR) | Group A (Mild) (n = 33) Median (IQR) | Group B (Severe) (n = 27) Median (IQR) | p Value $ |
|---|---|---|---|---|
| Interferon alpha (IFN-α) (reference, <2 U/mL) | 1.8 (0.5–2) | 12 (8–28) # | 54 (18–60) #,$ | <0.0001 $ |
| Interferon gamma (IFN-γ) (reference, 0.10–18.00 pg/mL) | 10.2 (1.9–17.3) | 16 (14–20) # | 21 (15–24) # | 0.9940 |
| Interleukin 1 beta (IL-1β) (reference, 0.5–12 pg/mL) | 8.7 (1.6–10.4) | 12 (5–30) | 32 (18–110) #,$ | <0.0001 $ |
| Interleukin 6 (IL-6) (reference, <5 pg/mL) | 3.8 (0.98–4.87) | 93 (44–365) * | 153 (69–835) #,$ | <0.0001 $ |
| Interleukin 8 (IL-8) (reference, 2.8–17.0 pg/mL) | 14.3 (4.7–15.9) | 38 (25–159) * | 48 (32–198) #,$ | 0.0279 $ |
| Interleukin 10 (IL-10) (reference, <10 pg/mL) | 5.2 (0.9–9.6) | 63 (43–220) # | 120 (40–312) # | 0.4666 |
| Tumor necrosis factor alpha (TNF-α) (reference, <8.5 pg/mL) | 5.9 (4.1–8.2) | 54 (42–180) | 90 (74–510) #,$ | 0.0258 $ |
| Granulocyte colony stimulating factor (G-CSF) (reference, 5–42 ng/L) | 19.8 (7.2–38.8) | 48 (15–228) | 185 (70–610) #,$ | 0.0279 $ |
| Granulocyte-macrophage colony-stimulating factor (GM-CSF) (reference, 0–0.39 pg/mL) | 0.2 (0.12–0.4) | 5 (0.4–12) | 42 (5–69) #,$ | <0.0001 $ |
| high-mobility group box 1 (HMGB1) (reference, 0.2–0.4 ng/mL) | 0.35 (0.15–0.39) | 2.5 (0.9–22) | 30 (15–118) #,$ | <0.0001 $ |
| Human C-X-C motif chemokine ligand 10 (CXCL10) (reference, <7.8 pg/mL) | 4.2 (1.9–7.9) | 10.2 (6–29) # | 17 (6.9–33.5) # | 0.0792 |
| Variable | Group A (Mild) (n = 33) Median (IQR) | Group B (Severe) (n = 27) Median (IQR) | p Value # |
|---|---|---|---|
| Interferon alpha (IFN-α) (reference, <2 U/mL) | 1.1 (0.8–4.9) | 2 (0.5–12) | 0.4666 |
| Interferon gamma (IFN-γ) (reference, 0.10–18.00 pg/mL) | 0.66 (0.11–1.57) | 0.58 (0.11–1.69) | 0.9791 |
| Interleukin 1 beta (IL-1β) (reference, 0.5–12 pg/mL) | 8 (5–14) | 16 (5–21.5) | 0.0033 # |
| Interleukin 6 (IL-6) (reference, <5 pg/mL) | 9 (8–32) | 13 (9–39) | 0.0033 # |
| Interleukin 8 (IL-8) (reference, 2.8–17.0 pg/mL) | 6.8 (2.5–14.6) | 4.7 (2–16) | 0.5194 |
| Interleukin 10 (IL-10) (reference, <10 pg/mL) | 3.82 (2.17–7.27) | 5.23 (3.31–10.64) | 0.425 |
| Tumor necrosis factor alpha (TNF-α) (reference, <8.5 pg/mL) | 13.5 (8.2–21.4) | 15 (8.1–30) | 0.5194 |
| Granulocyte colony stimulating factor (G-CSF) (reference, 5–42 ng/L) | 24.3 (7.9–34) | 33.5 (21.3–48) | 0.0508 |
| Granulocyte-macrophage colony-stimulating factor (GM-CSF) (reference, 0–0.39 pg/mL) | 0.45 (0.1–1.2) | 0.9 (0.3–2.5) | 0.0336 # |
| high-mobility group box 1 (HMGB1) (reference, 0.2–0.4 ng/mL) | 0.3 (0.1–1.4) | 0.3 (0.2–1.3) | 0.9935 |
| Human C-X-C motif chemokine ligand 10 (CXCL10) (reference, <7.8 pg/mL) | 3.8 (1.2–8) | 5.9 (4.7–10.3) | 0.9924 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abo-Haded, H.M.; Alshengeti, A.M.; Alawfi, A.D.; Khoshhal, S.Q.; Al-Harbi, K.M.; Allugmani, M.D.; El-Agamy, D.S. Cytokine Profiling among Children with Multisystem Inflammatory Syndrome versus Simple COVID-19 Infection: A Study from Northwest Saudi Arabia. Biology 2022, 11, 946. https://doi.org/10.3390/biology11070946
Abo-Haded HM, Alshengeti AM, Alawfi AD, Khoshhal SQ, Al-Harbi KM, Allugmani MD, El-Agamy DS. Cytokine Profiling among Children with Multisystem Inflammatory Syndrome versus Simple COVID-19 Infection: A Study from Northwest Saudi Arabia. Biology. 2022; 11(7):946. https://doi.org/10.3390/biology11070946
Chicago/Turabian StyleAbo-Haded, Hany M., Amer M. Alshengeti, Abdulsalam D. Alawfi, Saad Q. Khoshhal, Khalid M. Al-Harbi, Mohammad D. Allugmani, and Dina S. El-Agamy. 2022. "Cytokine Profiling among Children with Multisystem Inflammatory Syndrome versus Simple COVID-19 Infection: A Study from Northwest Saudi Arabia" Biology 11, no. 7: 946. https://doi.org/10.3390/biology11070946
APA StyleAbo-Haded, H. M., Alshengeti, A. M., Alawfi, A. D., Khoshhal, S. Q., Al-Harbi, K. M., Allugmani, M. D., & El-Agamy, D. S. (2022). Cytokine Profiling among Children with Multisystem Inflammatory Syndrome versus Simple COVID-19 Infection: A Study from Northwest Saudi Arabia. Biology, 11(7), 946. https://doi.org/10.3390/biology11070946