
Improving the Accuracy of Diagnosis for Multiple-System Atrophy Using Deep Learning-Based Method


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Data and Diagnosis
2.3. Items
2.4. Classification of MSA Subtypes
2.5. Extraction of Important Features Involved in Classification of MSA Subtypes
2.6. Statistics
3. Results
3.1. Patient Characteristics
3.2. Diagnostic Probability Using the Point-Wise Linear Model
3.3. Identifying Important Features Using the Pointwise Linear Model
3.3.1. Verification of the Prediction Performance for the Pointwise Linear Model
3.3.2. Extraction of Important Features Closely Associated with the Diagnosis for the MSA Subtypes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fanciulli, A.; Wenning, G.K. Multiple-System Atrophy. N. Engl. J. Med. 2015, 372, 249–263. [Google Scholar] [CrossRef] [PubMed]
- Gilman, S.; Low, P.A.; Quinn, N.; Albanese, A.; Ben-Shlomo, Y.; Fowler, C.J.; Kaufmann, H.; Klockgether, T.; Lang, A.E.; Lantos, P.L.; et al. Consensus statement on the diagnosis of multiple system atrophy. J. Neurol. Sci. 1999, 163, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Gilman, S.; Wenning, G.K.; Low, P.A.; Brooks, D.J.; Mathias, C.J.; Trojanowski, J.Q.; Wood, N.W.; Colosimo, C.; Dürr, A.; Fowler, C.J.; et al. Second consensus statement on the diagnosis of multiple system atrophy. Neurology 2008, 71, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Koga, S.; Aoki, N.; Uitti, R.J.; van Gerpen, J.A.; Cheshire, W.P.; Josephs, K.A.; Wszolek, Z.K.; Langston, J.W.; Dickson, D.W.; When, D.L.B. PD, and PSP masquerade as MSA: An autopsy study of 134 patients. Neurology 2015, 85, 404–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tăuţan, A.M.; Ionescu, B.; Santarnecchi, E. Artificial intelligence in neurodegenerative diseases: A review of available tools with a focus on machine learning techniques. Artif. Intell. Med. 2021, 117, 102081. [Google Scholar] [CrossRef] [PubMed]
- Duchesne, S.; Rolland, Y.; Vérin, M. Automated computer differential classification in Parkinsonian Syndromes via pattern analysis on MRI. Acad. Radiol. 2009, 16, 61–70. [Google Scholar] [CrossRef]
- Miki, Y.; Foti, S.C.; Asi, Y.T.; Tsushima, E.; Quinn, N.; Ling, H.; Holton, J.L. Improving diagnostic accuracy of multiple system atrophy: A clinicopathological study. Brain 2019, 142, 2813–2827. [Google Scholar] [CrossRef]
- Myszczynska, M.A.; Ojamies, P.N.; Lacoste, A.M.B.; Neil, D.; Saffari, A.; Mead, R.; Hautbergue, G.M.; Holbrook, J.D.; Ferraiuolo, L. Applications of machine learning to diagnosis and treatment of neurodegenerative diseases. Nat. Rev. Neurol. 2020, 16, 440–456. [Google Scholar] [CrossRef]
- Patel, U.K.; Anwar, A.; Saleem, S.; Malik, P.; Rasul, B.; Patel, K.; Yao, R.; Seshadri, A.; Yousufuddin, M.; Arumaithurai, K. Artificial intelligence as an emerging technology in the current care of neurological disorders. J. Neurol. 2021, 268, 1623–1642. [Google Scholar] [CrossRef]
- Richens, J.G.; Lee, C.M.; Johri, S. Improving the accuracy of medical diagnosis with causal machine learning. Nat. Commun. 2020, 11, 3923. [Google Scholar] [CrossRef]
- Xia, C.; Postuma, R.B. Diagnosing multiple system atrophy at the prodromal stage. Clin. Auton. Res. 2020, 30, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Tada, M.; Onodera, O.; Tada, M.; Ozawa, T.; Piao, Y.S.; Kakita, A.; Takahashi, H.; Nishizawa, M. Early development of autonomic dysfunction may predict poor prognosis in patients with multiple system atrophy. Arch. Neurol. 2007, 64, 256–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzolina, D.; Baldi, I.; Barbati, G.; Berchialla, P.; Bottigliengo, D.; Bucci, A.; Calza, S.; Dolce, P.; Edefonti, V.; Faragalli, A.; et al. Machine learning in clinical and epidemiological research: Isn’t it time for biostatisticians to work on it? Epidemiol. Biostat. Public Health 2019, 16, 1–3. [Google Scholar]
- Poon, A.I.F.; Sung, J.J.Y. Opening the black box of AI-Medicine. J. Gastroenterol. Hepatol. 2021, 36, 581–584. [Google Scholar] [CrossRef]
- Shibahara, T.; Wada, C.; Yamashita, Y.; Fujita, K.; Sato, M.; Okamoto, A.; Ono, Y. Deep learning generates custom-made logistic regression models for explaining how breast cancer subtypes are classified. bioRxiv 2021. [Google Scholar] [CrossRef]
- Kumagai, S.; Togashi, Y.; Kamada, T.; Sugiyama, E.; Nishinakamura, H.; Takeuchi, Y.; Vitaly, K.; Itahashi, K.; Maeda, Y.; Matsui, S.; et al. The PD-1 expression balance between effector and regulatory T cells predicts the clinical efficacy of PD-1 blockade therapies. Nat. Immunol. 2020, 21, 1346–1358. [Google Scholar] [CrossRef]
- Kanatani, Y.; Tomita, N.; Sato, Y.; Eto, A.; Omoe, H.; Mizushima, H. National Registry of Designated Intractable Diseases in Japan: Present Status and Future Prospects. Neurol. Med. Chir. 2017, 57, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Trouillas, P.; Takayanagi, T.; Hallett, M.; Currier, R.D.; Subramony, S.H.; Wessel, K.; Bryer, A.; Diener, H.C.; Massaquoi, S.; Gomez, C.M.; et al. International Cooperative Ataxia Rating Scale for pharmacological assessment of the cerebellar syndrome. The Ataxia Neuropharmacology Committee of the World Federation of Neurology. J. Neurol. Sci. 1997, 145, 205–211. [Google Scholar] [CrossRef]
- Fahn, S.; Elton, R. Members of the UPDRS Development Committee. The Unified Parkinson’s Disease Rating Scale. In Recent Developments in Parkinson’s Disease; Fahn, S., Marsden, C.D., Calne, D.B., Goldstein, M., Eds.; McMellam Health Care Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–163. [Google Scholar]
- Wenning, G.K.; Tison, F.; Seppi, K.; Sampaio, C.; Diem, A.; Yekhlef, F.; Ghorayeb, I.; Ory, F.; Galitzky, M.; Scaravilli, T.; et al. Multiple System Atrophy Study Group. Development and validation of the Unified Multiple System Atrophy Rating Scale (UMSARS). Mov. Disord. 2004, 19, 1391–1402. [Google Scholar] [CrossRef]
- Kasner, S.E. Clinical interpretation and use of stroke scales. Lancet Neurol. 2006, 5, 603–612. [Google Scholar] [CrossRef]
- Golas, S.B.; Shibahara, T.; Agboola, S.; Otaki, H.; Sato, J.; Nakae, T.; Hisamitsu, T.; Kojima, G.; Felsted, J.; Kakarmath, S.; et al. A machine learning model to predict the risk of 30-day readmissions in patients with heart failure: A retrospective analysis of electronic medical records data. BMC Med. Inform. Decis. Mak. 2018, 18, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koga, S.; Dickson, D.W. Recent advances in neuropathology, biomarkers and therapeutic approach of multiple system atrophy. J. Neurol. Neurosurg. Psychiatry 2018, 89, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Lemos, M.; Wenning, G.K.; Stefanova, N. Current experimental disease-modifying therapeutics for multiple system atrophy. J. Neural Transm. 2021, 128, 1529–1543. [Google Scholar] [CrossRef]
- Fereshtehnejad, S.M.; Zeighami, Y.; Dagher, A.; Postuma, R.B. Clinical criteria for subtyping Parkinson’s disease: Biomarkers and longitudinal progression. Brain 2017, 140, 1959–1976. [Google Scholar] [CrossRef] [PubMed]
- Rajula, H.S.R.; Verlato, G.; Manchia, M.; Antonucci, N.; Fanos, V. Comparison of Conventional Statistical Methods with Machine Learning in Medicine: Diagnosis, Drug Development, and Treatment. Medicina 2020, 56, 455. [Google Scholar] [CrossRef]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef] [Green Version]
- Glass, G.A.; Josephs, K.A.; Ahlskog, J.E. Respiratory insufficiency as the primary presenting symptom of multiple-system atrophy. Arch. Neurol. 2006, 63, 978–981. [Google Scholar] [CrossRef]
- Calandra-Buonaura, G.; Alfonsi, E.; Vignatelli, L.; Benarroch, E.E.; Giannini, G.; Iranzo, A.; Low, P.A.; Martinelli, P.; Provini, F.; Quinn, N.; et al. Dysphagia in multiple system atrophy consensus statement on diagnosis, prognosis and treatment. Parkinsonism Relat. Disord. 2021, 86, 124–132. [Google Scholar] [CrossRef]


{kind=link}
| Item | Option |
|---|---|
| Sex | 1. Male, 2. female |
| Age | |
| Symptoms at onset | 1. Ataxia |
| 2. Parkinsonism | |
| 3. Autonomic dysfunction | |
| Mode of onset | 1. Mild, 2. subacute, 3. acute |
| Progression | 1. Progressive, 2. arrested, 3. improved, 4. other |
| Neurological findings | 1. Walking capacity |
| 2. Gait abnormalities due to parkinsonism | |
| 3. Standing capacity, eyes open | |
| 4. Bent posture | |
| 5. Posture stability | |
| 6. Finger-to-nose test | |
| 7. Knee–tibia test | |
| 8. Tremor at rest | |
| 9. Rigidity | |
| 10. Finger taps | |
| 11. Rising from a chair | |
| Autonomic findings | 1. Head-up tilt test |
| 2. Syncope | |
| 3. Urinary disturbances | |
| 4. Urinary incontinence | |
| 5. Erectile dysfunction (male only) | |
| 6. Severe constipation | |
| Other neurological findings | 1. Dementia |
| 2. Hallucination (non-drug-induced) | |
| 3. Aphasia | |
| 4. Apraxia | |
| 5. Agnosia | |
| 6. Alien hand sign | |
| 7. Vertical supranuclear gaze palsy | |
| 8. Persistent Spontaneous Nystagmus | |
| 9. Dysphasia | |
| 10. Dysarthria | |
| 11. Respiratory failure | |
| 12.Tendon reflex | |
| 13. Babinski reflex | |
| 14. Other neurological findings | |
| Brain images with CT/MRI | 1. CT examination |
| 2. MRI examination | |
| 3. Cerebellar atrophy | |
| 4. Brain-stem atrophy | |
| 5. Hot-cross-bun sign | |
| 6. Striatal atrophy/signal abnormality | |
| 7. Enlargement of 3rd ventricle | |
| 8. Cerebral atrophy | |
| 9. Cerebral white-matter lesion | |
| ADL | 1. Eating |
| 2. Bathing | |
| 3. Hygiene | |
| 4. Dressing | |
| 5. Toileting | |
| 6. Walking (more than 50 m) | |
| 7. Climbing stairs | |
| Medication | 1. Taltirelin hydrate |
| 2. Protirelin tartrate hydrate | |
| 3. Levodopa | |
| 4. Dopamine receptor agonists | |
| 5. Amantadine hydrochloride | |
| 6. Anticholinergics | |
| 7. MAO-B inhibitors | |
| 8. Droxidopa | |
| Diagnosis | 1. SND 2. SDS 3. OPCA |
| Hyperparameter | Best Parameter |
|---|---|
| Number of epochs | 100 |
| Number of inner layers | 16 |
| Size of layers | 180 |
| Label smoothing | 0.055 |
| Learning rate | 1.83 × 10−4 |
| Momentum | 0.968 |
| Optimization | adam |
| Dropout rate of inner layers | 0.027 |
| Dropout rate of input layer | 0.171 |
| Regularization coefficient | 9.29 × 10−5 |
| Ratio of L1 regularization | 0.048 |
| (a) With Rank Order of Items | (b) Without Rank Order of Items | ||||
|---|---|---|---|---|---|
| Item | Options for Item | Category # | Number of Feature Variables = 58 | Category # | Number of Feature Variables = 126 |
| Sex | B | 1 | B | 1 | |
| Age | Q | 1 | Q | 1 | |
| Symptoms at onset | 1–3 | B | 3 | B | 3 |
| Mode of onset | O | 1 | C | 3 | |
| Progression | C | 4 | C | 4 | |
| Neurological findings | 1–11 | O | 11 | C | 62 |
| Autonomic findings | 1–6 | B | 6 | B | 6 |
| Other neurological findings | 1–11, 13 | B | 12 | B | 12 |
| 12 | C | 3 | C | 3 | |
| Brain images with CT/MRI | 1–9 | B | 9 | B | 9 |
| ADL | 1–7 | O | 7 | C | 22 |
| Medication | 1–8 | n/a | 0 | n/a | 0 |
| Item | Category | SND | SDS | OPCA | p–Value |
|---|---|---|---|---|---|
| 894 | 377 | 2106 | |||
| Sex | 1.21 | 0.41 | 0.92 | <0.001 | |
| Age | 67.4 ± 9.7 | 66.8 ± 10.6 | 64.8 ± 9.3 | <0.001 | |
| Symptoms at onset, n (%) | |||||
| Ataxia | Yes | 65 (7.3) | 61 (16.2) | 1907 (90.6) | <0.001 |
| Parkinsonism | Yes | 783 (87.6) | 61 (16.2) | 162 (7.7) | <0.001 |
| Autonomic dysfunction | Yes | 57 (6.4) | 275 (72.9) | 86 (4.1) | <0.001 |
| Mode of onset, n (%) | Mild | 835 (93.4) | 333 (88.3) * | 2017 (95.8) † | <0.001 |
| Subacute | 56 (6.3) | 39 (10.3) | 84 (4.0) * | ||
| Acute | 3 (0.3) | 5 (1.3) † | 5 (0.2) | ||
| Progression, n (%) | Progressive | 886 (99.1) | 369 (97.9) | 2087 (99.1) | 0.137 |
| Arrested | 8 (0.9) | 5 (1.3) | 11 (0.5) | ||
| Improved | 0 | 2 (0.5) | 4 (0.2) | ||
| Other | 0 | 1 (0.2) | 4 (0.2) | ||
| Neurological findings | Scale | ||||
| 1. Walking capacity | 1–9 | 5.7 ± 2.5 | 5.0 ± 2.7 | 4.8 ± 2.3 | <0.001 |
| 2. Gait abnormalities due to parkinsonism | 1–5 | 3.3 ± 1.1 | 2.4 ± 1.4 | 1.9 ± 1.3 | <0.001 |
| 3. Standing capacity, eyes open | 1–8 | 4.6 ± 2.3 | 4.2 ± 2.4 | 4.2 ± 2.0 | <0.001 |
| 4. Bent posture | 1–5 | 2.6 ± 1.0 | 1.8 ± 0.9 | 1.6 ± 0.9 | <0.001 |
| 5. Posture stability | 1–5 | 3.4 ± 1.2 | 2.7 ± 1.5 | 2.5 ± 1.5 | <0.001 |
| 6. Finger-to-nose test | 1–5 | 2.1 ± 1.1 | 2.1 ± 0.9 | 2.6 ± 0.8 | <0.001 |
| 7. Knee–tibia test | 1–5 | 2.2 ± 1.2 | 2.2 ± 1.1 | 2.9 ± 1.0 | <0.001 |
| 8. Tremor at rest | 1–5 | 1.7 ± 0.9 | 1.4 ± 0.7 | 1.3 ± 0.6 | <0.001 |
| 9. Rigidity | 1–5 | 3.0 ± 0.8 | 2.0 ± 0.9 | 1.7 ± 0.9 | <0.001 |
| 10. Finger taps | 1–5 | 2.9 ± 0.9 | 2.1 ± 0.9 | 2.0 ± 1.0 | <0.001 |
| 11. Rising from a chair | 1–5 | 3.5 ± 1.3 | 2.8 ± 1.5 | 2.9 ± 1.5 | <0.001 |
| Autonomic findings, n (%) | |||||
| 1. Head-up tilt test | Positive | 348 (38.9) | 310 (82.2) | 818 (38.8) | <0.001 |
| 2. Syncope | Yes | 166 (18.6) | 290 (76.9) | 269 (12.8) | <0.001 |
| 3. Urinary disturbances | Yes | 465 (52.0) | 300 (79.6) | 839 (39.8) | <0.001 |
| 4. Urinary incontinence | Yes | 335 (21.4) | 218 (57.8) | 517 (24.6) | <0.001 |
| 5. Erectile dysfunction (males only) | Yes | 191 (47.1) | 185 (69.2) | 366 (33.4) | <0.001 |
| 6. Severe constipation | Yes | 534 (59.7) | 259 (68.7) | 740 (35.1) | <0.001 |
| Other neurological findings | |||||
| 1. Dementia | Yes | 127 (14.2) | 52 (13.8) | 212 (10.1) | <0.001 |
| 2. Hallucination (non-drug-induced) | Yes | 37 (4.1) | 10 (2.7) | 24 (1.1) | <0.001 |
| 3. Aphasia | Yes | 9 (1.0) | 4 (1.1) | 18 (0.9) | 0.878 |
| 4. Apraxia | Yes | 16 (1.8) | 7 (1.9) | 17 (0.8) | 0.033 |
| 5. Agnosia | Yes | 9 (1.0) | 6 (1.6) | 16 (0.8) | 0.279 |
| 6. Alien hand sign | Yes | 1 (0.1) | 2 (0.5) | 3 (0.1) | 0.228 |
| 7. Vertical supranuclear gaze palsy | Yes | 66 (7.4) | 11 (2.9) | 69 (3.3) | <0.001 |
| 8. Persistent spontaneous nystagmus | Yes | 69 (7.7) | 24 (6.4) | 367 (17.4) | <0.001 |
| 9. Dysphasia | Yes | 318 (35.6) | 76 (20.2) | 489 (23.2) | <0.001 |
| 10. Dysarthria | Yes | 524 (58.6) | 194 (51.5) | 1670 (79.3) | <0.001 |
| 11. Respiratory failure | Yes | 175 (19.6) | 164 (43.5) | 331 (15.7) | <0.001 |
| 12. Tendon reflex | Increased | 363 (40.6) | 133 (35.3) * | 962 (45.7) † | <0.001 |
| Decreased | 81 (9.1) | 50 (13.3) † | 177 (8.4) | ||
| Normal | 450 (50.3) | 194 (51.5) | 967 (45.9) * | ||
| 13. Babinski reflex | Yes | 189 (21.1) | 78 (20.7) | 391 (18.6) | 0.489 |
| Brain images with CT/MRI, n (%) | |||||
| 1. Cerebellar atrophy | Yes | 367 (41.1) | 218 (57.8) | 1980 (94.0) | <0.001 |
| 2. Brain-stem atrophy | Yes | 323 (36.1) | 173 (45.9) | 1670 (79.3) | <0.001 |
| 3. Hot-cross-bun sign | Yes | 189 (21.1) | 81 (21.5) | 1008 (47.9) | <0.001 |
| 4. Striatal atrophy/signal abnormality | Yes | 525 (58.7) | 44 (11.7) | 111 (5.3) | <0.001 |
| 5. Enlargement of 3rd ventricle | Yes | 64 (7.2) | 29 (7.7) | 140 (6.7) | 0.674 |
| 6. Cerebral atrophy | Yes | 116 (13.0) | 52 (13.8) | 148 (7.0) | <0.001 |
| 7. Cerebral white-matter lesion | Yes | 47 (5.3) | 24 (6.4) | 70 (3.3) | <0.001 |
| ADL | Scale | ||||
| 1. Eating | 1–3 | 1.5 ± 0.7 | 1.4 ± 0.6 | 1.3 ± 0.5 | <0.001 |
| 2. Bathing | 1–3 | 2.0 ± 0.7 | 1.8 ± 0.8 | 1.6 ± 0.7 | <0.001 |
| 3. Hygiene | 1–3 | 1.8 ± 0.7 | 1.6 ± 0.7 | 1.4 ± 0.6 | <0.001 |
| 4. Dressing | 1–3 | 1.8 ± 0.7 | 1.6 ± 0.7 | 1.4 ± 0.7 | <0.001 |
| 5. Toileting | 1–3 | 1.7 ± 0.7 | 1.6 ± 0.7 | 1.4 ± 0.2 | <0.001 |
| 6. Walking (more than 50 m) | 1–4 | 2.3 ± 1.0 | 2.1 ± 1.0 | 1.9 ± 1.0 | <0.001 |
| 7. Climbing stairs | 1–3 | 2.3 ± 0.8 | 2.1 ± 0.8 | 2.0 ± 0.8 | <0.001 |
| Medication, n (%) | |||||
| 1. Taltirelin hydrate | 1. Not used | 786 (87.9) † | 316 (83.8) † | 1323 (62.8) * | <0.001 |
| 2. Used | 75 (8.4) * | 48 (12.7) * | 751 (35.7) † | ||
| 3. Unknown | 33 (3.7) † | 13 (3.5) | 32 (1.5) * | ||
| 2. Protirelin tartrate hydrate | 1. Not used | 824 (92.2) † | 347 (92.0) † | 1806 (85.8) * | <0.001 |
| 2. Used | 25 (2.8) * | 23 (6.1) * | 230 (10.9) † | ||
| 3. Unknown | 45 (5.0) † | 17 (4.5) † | 70 (3.3) * | ||
| 3. Levodopa | 1. Not used | 113 (12.6) * | 257 (68.2) † | 1752 (83.2) † | <0.001 |
| 2. Used | 775 (86.7) † | 109 (28.9) * | 288 (13.7) * | ||
| 3. Unknown | 6 (0.7) * | 11 (2.9) | 66 (3.1) † | ||
| 4. Dopamine receptor agonists | 1. Not used | 496 (55.5) * | 318 (84.3) | 1950 (92.6) † | <0.001 |
| 2. Used | 362 (40.5) † | 42 (11.1) * | 86 (4.1) * | ||
| 3. Unknown | 36 (4.0) | 17 (4.5) † | 70 (3.3) | ||
| 5. Amantadine hydrochloride | 1. Not used | 634 (70.9) * | 335 (88.9) | 1935 (91.9) † | <0.001 |
| 2. Used | 222 (24.8) † | 26 (6.9) * | 93 (4.4) * | ||
| 3. Unknown | 38 (4.3) | 16 (4.2) | 78 (3.7) | ||
| 6. Anticholinergic | 1. Not used | 775 (86.7) * | 341 (90.5) | 2000 (95.0) † | <0.001 |
| 2. Used | 79 (8.8) † | 17 (4.5) | 26 (1.2) * | ||
| 3. Unknown | 40 (4.5) | 19 (5.0) | 80 (3.8) | ||
| 7. MAO-B inhibitors | 1. Not used | 747 (83.6) * | 347 (92.0) | 2000 (95.0) † | <0.001 |
| 2. Used | 108 (12.1) † | 11 (2.9) | 26 (1.2) * | ||
| 3. Unknown | 39 (4.4) | 19 (5.0) | 80 (3.8) | ||
| 8. Droxidopa | 1. Not used | 693 (77.5) * | 223 (59.2) * | 1958 (93.0) † | <0.001 |
| 2. Used | 161 (18.0) † | 142 (37.7) † | 66 (3.1) * | ||
| 3. Unknown | 40 (4.5) † | 12 (3.2) | 82 (3.9) |
| SND (n = 10) | SDS (n = 10) | OPCA (n = 10) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Diagnostic Probability | Diagnostic Probability | Diagnostic Probability | |||||||||
| No. | SND | SDS | OPCA | No. | SND | SDS | OPCA | No. | SND | SDS | OPCA |
| 1 | 0.956 | 0.025 | 0.019 | 1 | 0.373 | 0.489 | 0.138 | 1 | 0.037 | 0.040 | 0.923 |
| 2 | 0.934 | 0.039 | 0.027 | 2 | 0.019 | 0.947 | 0.034 | 2 | 0.910 | 0.041 | 0.049 |
| 3 | 0.884 | 0.034 | 0.082 | 3 | 0.050 | 0.885 | 0.065 | 3 | 0.016 | 0.032 | 0.952 |
| 4 | 0.909 | 0.060 | 0.031 | 4 | 0.281 | 0.400 | 0.319 | 4 | 0.017 | 0.032 | 0.952 |
| 5 | 0.572 | 0.076 | 0.352 | 5 | 0.028 | 0.474 | 0.497 | 5 | 0.021 | 0.029 | 0.950 |
| 6 | 0.948 | 0.028 | 0.025 | 6 | 0.104 | 0.667 | 0.229 | 6 | 0.021 | 0.040 | 0.939 |
| 7 | 0.812 | 0.019 | 0.169 | 7 | 0.091 | 0.717 | 0.192 | 7 | 0.017 | 0.010 | 0.973 |
| 8 | 0.804 | 0.178 | 0.018 | 8 | 0.589 | 0.214 | 0.197 | 8 | 0.021 | 0.021 | 0.959 |
| 9 | 0.820 | 0.050 | 0.130 | 9 | 0.044 | 0.776 | 0.180 | 9 | 0.037 | 0.031 | 0.932 |
| 10 | 0.876 | 0.091 | 0.032 | 10 | 0.036 | 0.932 | 0.032 | 10 | 0.025 | 0.022 | 0.953 |
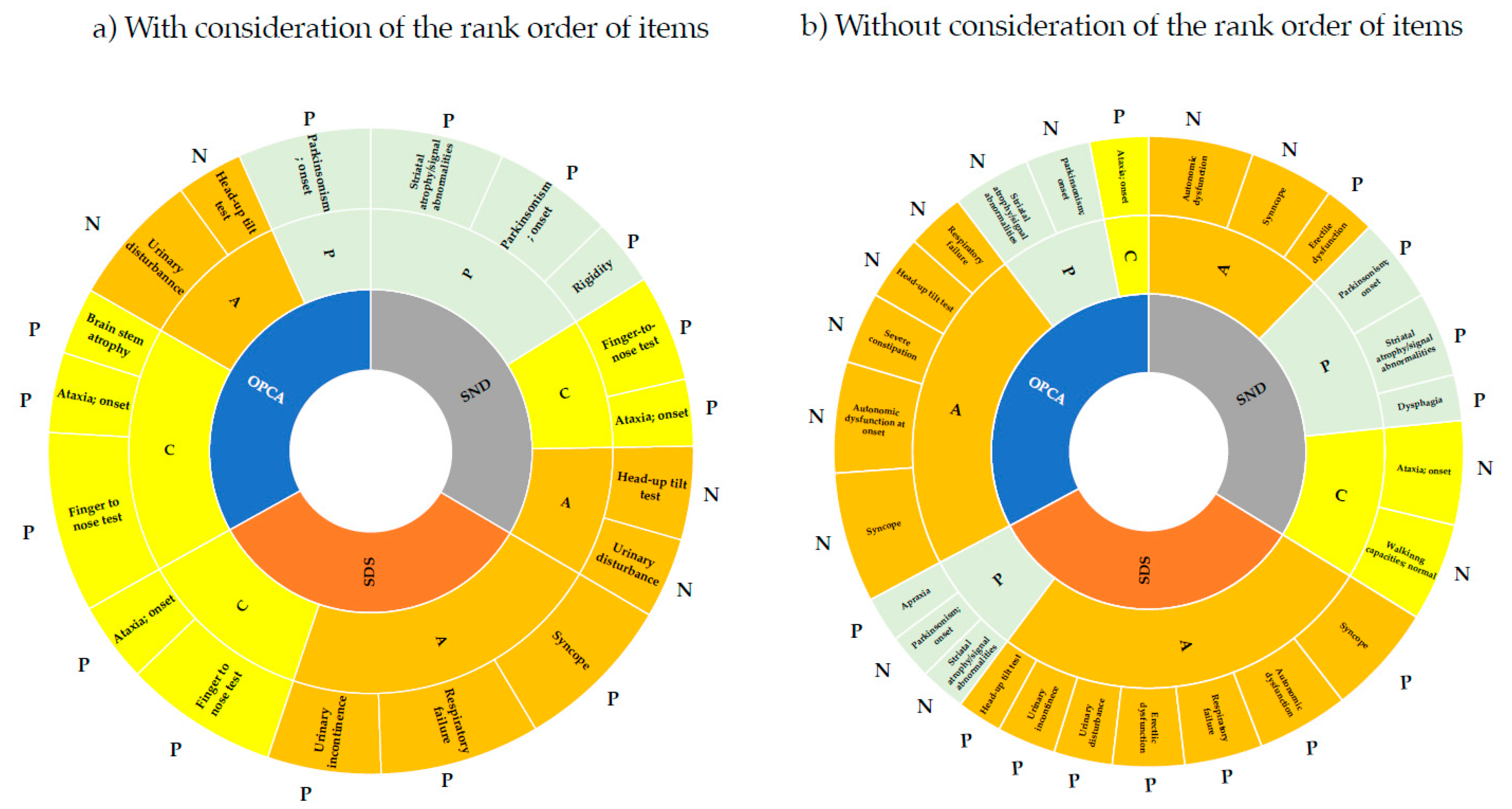
| (a) With Consideration of the Rank Order of Items | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Rank | SND | SDS | OPCA | ||||||
| Feature | Score | Weight | Feature | Score | Weight | Feature | Score | Weight | |
| 1 | Striatal atrophy/signal abnormalities | 0.798 | −0.143 | Respiratory failure | 0.796 | −0.122 | Finger-to-nose test | 0.910 | 0.060 |
| 2 | Parkinsonism onset | 0.705 | −0.288 | Syncope | 0.788 | −0.139 | Parkinsonism onset | 0.694 | −0.089 |
| 3 | Finger-to-nose test | 0.621 | 0.028 | Finger-to-nose test | 0.771 | 0.035 | Urinary disturbance | 0.517 | 0.104 |
| 4 | Head-up tilt test | 0.544 | 0.101 | Urinary incontinence | 0.562 | −0.074 | Ataxia onset | 0.395 | −0.458 |
| 5 | Urinary disturbance | 0.462 | 0.080 | Ataxia onset | 0.395 | −0.222 | Head-up tilt test | 0.350 | 0.067 |
| 6 | Ataxia onset | 0.395 | −0.183 | Brain-stem atrophy | 0.347 | −0.155 | |||
| 7 | Rigidity | 0.378 | 0.023 | ||||||
| (b) Without Consideration of the Rank Order of Items | |||||||||
| Rank | SND | SDS | OPCA | ||||||
| Feature | Score | Weight | Feature | Score | Weight | Feature | Score | Weight | |
| 1 | Autonomic dysfunction onset | 0.720 | 0.022 | Autonomic dysfunction onset | 0.865 | −0.254 | Striatal atrophy/signal abnormalities | 0.770 | 0.130 |
| 2 | Syncope | 0.639 | 0.173 | Striatal atrophy/signal abnormalities | 0.749 | 0.111 | Syncope | 0.720 | 0.155 |
| 3 | Parkinsonism onset | 0.628 | −0.125 | Parkinsonism onset | 0.704 | 0.214 | Parkinsonism onset | 0.644 | 0.204 |
| 4 | Striatal atrophy/signal abnormalities | 0.603 | −0.161 | Respiratory failure | 0.576 | −0.084 | Autonomic dysfunction onset | 0.606 | 0.071 |
| 5 | Erectile dysfunction | 0.378 | −0.020 | Head-up tilt test | 0.510 | −0.133 | Severe constipation | 0.414 | 0.064 |
| 6 | Ataxia onset | 0.375 | 0.173 | Syncope | 0.495 | −0.125 | Ataxia onset | 0.387 | −0.366 |
| 7 | Dysphagia | 0.343 | −0.025 | Erectile dysfunction | 0.444 | −0.056 | Head-up tilt test | 0.376 | 0.061 |
| 8 | Walking capacities, normal | 0.342 | −0.103 | Toileting, without assistance | 0.433 | −0.081 | Respiratory failure | 0.342 | 0.047 |
| 9 | Urinary incontinence | 0.372 | −0.053 | ||||||
| 10 | Apraxia | 0.368 | −0.030 | ||||||
| 11 | Urinary disturbance | 0.341 | −0.063 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanatani, Y.; Sato, Y.; Nemoto, S.; Ichikawa, M.; Onodera, O. Improving the Accuracy of Diagnosis for Multiple-System Atrophy Using Deep Learning-Based Method. Biology 2022, 11, 951. https://doi.org/10.3390/biology11070951
Kanatani Y, Sato Y, Nemoto S, Ichikawa M, Onodera O. Improving the Accuracy of Diagnosis for Multiple-System Atrophy Using Deep Learning-Based Method. Biology. 2022; 11(7):951. https://doi.org/10.3390/biology11070951
Chicago/Turabian StyleKanatani, Yasuhiro, Yoko Sato, Shota Nemoto, Manabu Ichikawa, and Osamu Onodera. 2022. "Improving the Accuracy of Diagnosis for Multiple-System Atrophy Using Deep Learning-Based Method" Biology 11, no. 7: 951. https://doi.org/10.3390/biology11070951
APA StyleKanatani, Y., Sato, Y., Nemoto, S., Ichikawa, M., & Onodera, O. (2022). Improving the Accuracy of Diagnosis for Multiple-System Atrophy Using Deep Learning-Based Method. Biology, 11(7), 951. https://doi.org/10.3390/biology11070951