


Effectiveness of Respiratory Muscles Training by Voluntary Isocapnic Hyperpnea Versus Inspiratory Threshold Loading on Intercostales and Vastus Lateralis Muscles Deoxygenation Induced by Exercise in Physically Active Adults

 ,
,  , ,
, ,  , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Protocol
2.3. Baseline and Post-Training Evaluations
2.4. Cardiopulmonary Exercise Testing (CPET)
2.5. Muscle Oxygen Saturation (SmO2)
2.6. Respiratory Muscle Training Protocol (RMT)
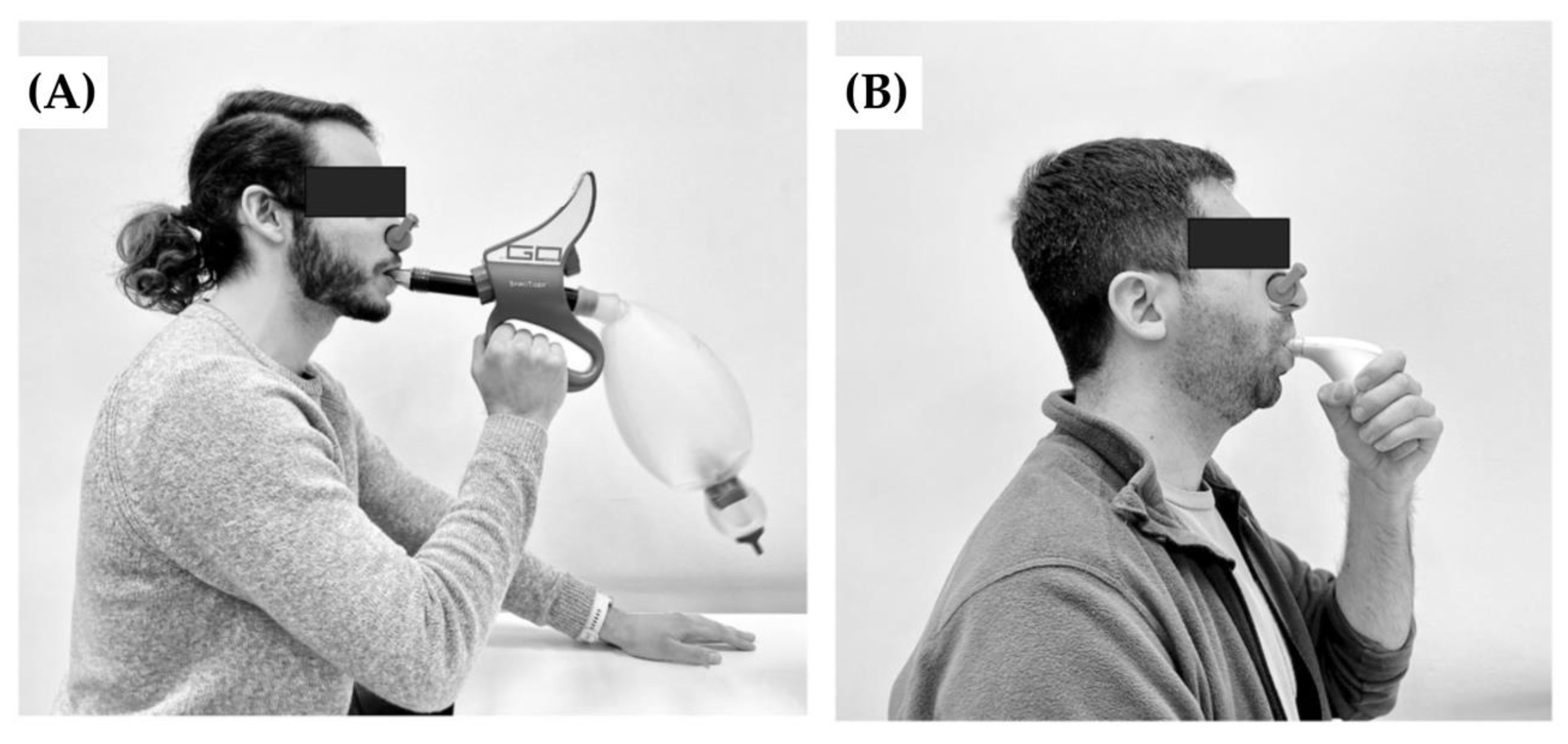
2.6.1. Voluntary Isocapnic Hyperpnea Training (VIH)
2.6.2. Inspiratory Threshold Loading Training (ITL)
2.7. Data Analysis
2.8. Statistical Analysis
3. Results
3.1. Muscle Oxygen Saturation Levels
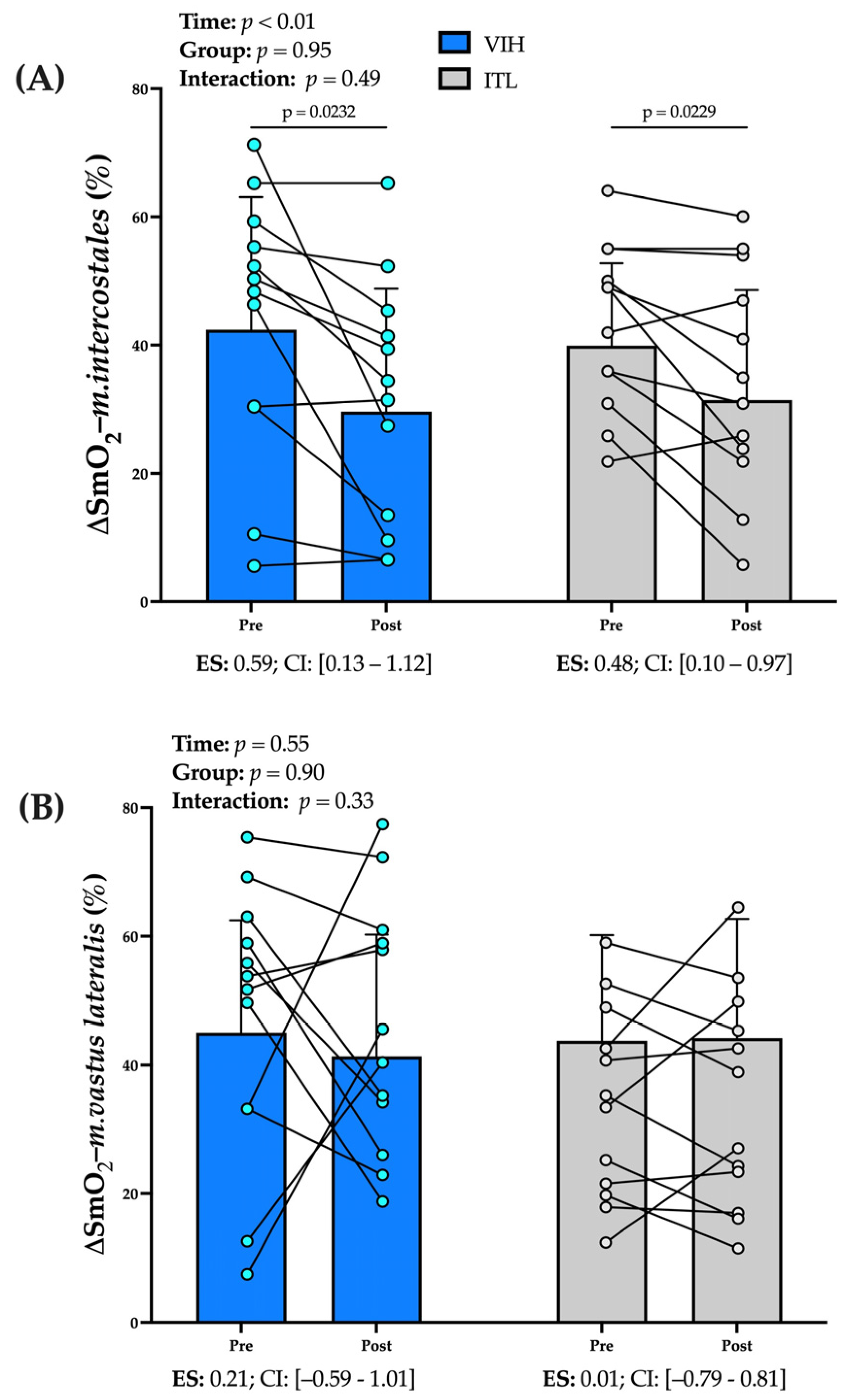
3.1.1. Deoxygenation of m. intercostales (∆SmO2-m. intercostales, %)
3.1.2. Deoxygenation of m. vastus lateralis (∆SmO2-m. vastus lateralis, %):
3.2. Total hemoglobin
3.3. SmO2 Ratio (∆SmO2-m. intercostales·∆SmO2-m. vastus lateralis−1)
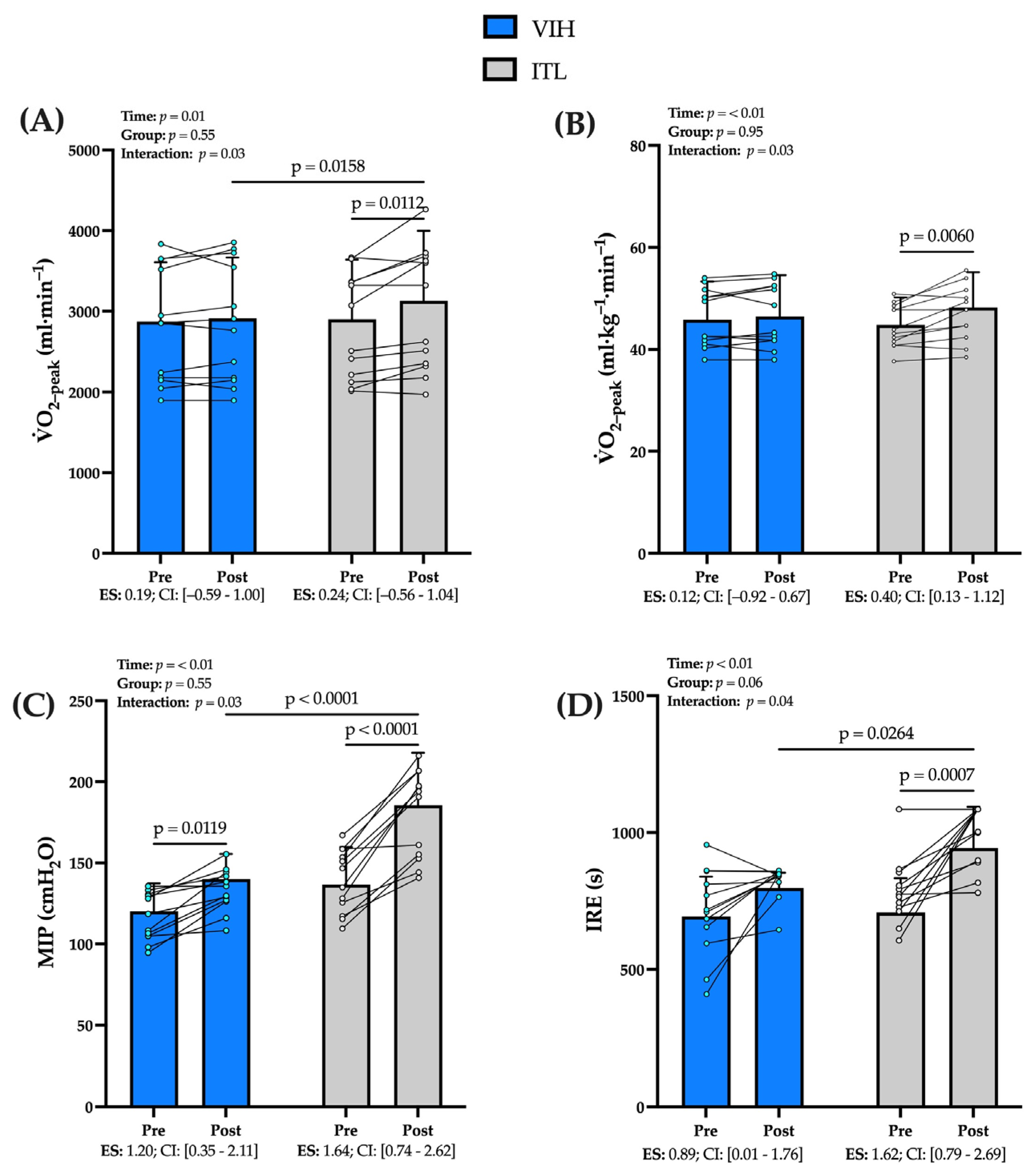
3.4. Cardiopulmonary Exercise Testing (CPET)
3.5. Performance of Respiratory Muscle
3.6. Deoxygenation Relative to Lung Ventilation and Peak Workload-to-Weight
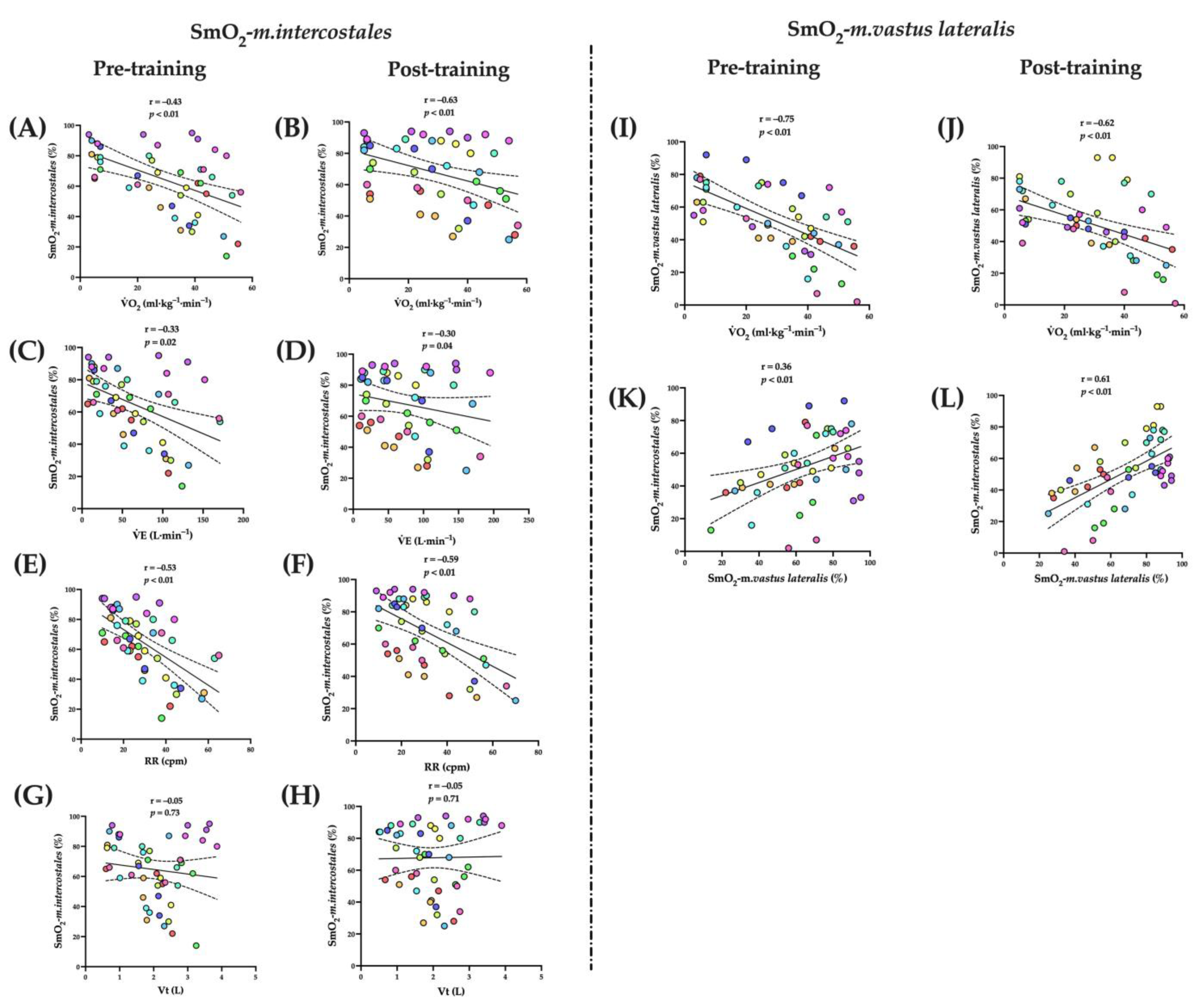
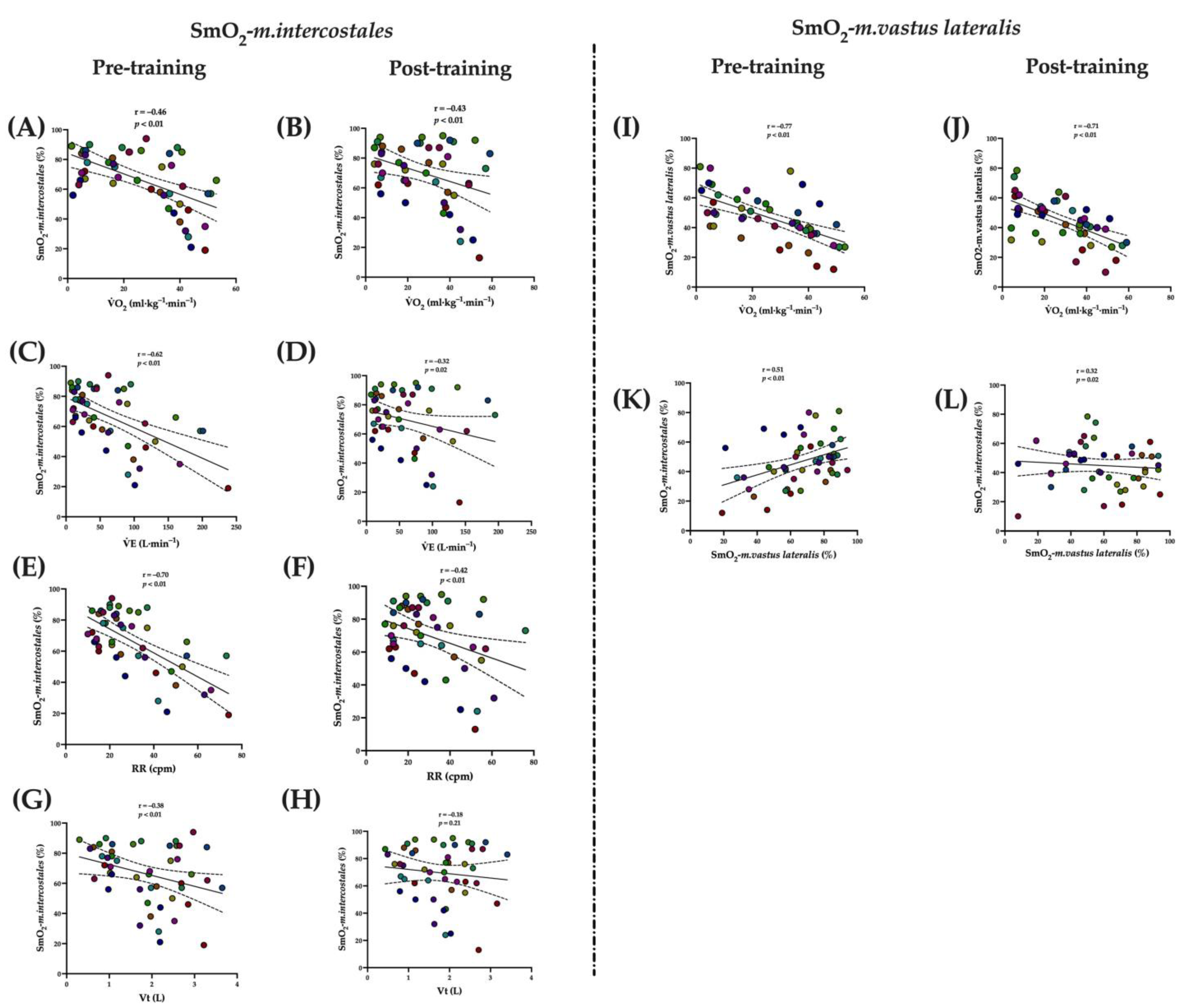
3.7. Correlations
3.7.1. Voluntary Isocapnic Hyperpnea Training (VIH)
3.7.2. Inspiratory Thresholds Loading Training (ITL)
4. Discussion
4.1. Effect of RMT in ∆SmO2-m. intercostales and ∆SmO2-m. Vastus Lateralis
4.2. Effect of RMT in Physical Performance
4.3. Effect of RMT in Respiratory Muscle Performance
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sheel, A.; Romer, L. Ventilation and respiratory mechanics. Compr. Physiol. 2012, 2, 1093–1142. [Google Scholar] [CrossRef] [PubMed]
- Romer, L.; Polkey, M. Exercise-induced respiratory muscle fatigue: Implications for performance. J. Appl. Physiol. 2008, 104, 879–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, J.; Kipp, S.; Sheel, A. Respiratory muscles during exercise: Mechanics, energetics, and fatigue. Curr. Opin. Physiol. 2019, 10, 102–109. [Google Scholar] [CrossRef]
- Romer, L.; Lovering, A.; Haverkamp, H.; Pegelow, D.; Dempsey, J. Effect of inspiratory muscle work on peripheral fatigue of locomotor muscles in healthy humans. J. Physiol. 2006, 571, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Boushel, R. Muscle metaboreflex control of the circulation during exercise. Acta Physiol. 2010, 199, 367–383. [Google Scholar] [CrossRef] [PubMed]
- McNulty, C.; Moody, W.; Wagenmakers, A.; Fisher, J. Effect of muscle metaboreflex activation on central hemodynamics and cardiac function in humans. Appl. Physiol. Nutr. Metab. 2014, 39, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Kaur, J.; Machado, T.; Alvarez, A.; Krishnan, A.; Hanna, H.; Altamimi, Y.; Senador, D.; Spranger, M.; O’Leary, D. Muscle metaboreflex activation during dynamic exercise vasoconstricts ischemic active skeletal muscle. Am. J. Physiol. Circ. Physiol. 2015, 309, H2145–H2151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.; Alexander, A.; Hammer, S.; Didier, K.; Kurti, S.; Broxterman, R.; Barstow, T.; Harms, C. Cardiovascular consequences of the inspiratory muscle metaboreflex: Effects of age and sex. Am. J. Physiol.-Heart Circ. Physiol. 2017, 312, H1013–H1020. [Google Scholar] [CrossRef] [Green Version]
- Witt, J.; Guenette, J.; Rupert, J.; McKenzie, D.; Sheel, A. Inspiratory muscle training attenuates the human respiratory muscle metaboreflex. J. Physiol. 2007, 584, 1019–1028. [Google Scholar] [CrossRef]
- Callegaro, C.; Ribeiro, J.; Tan, C.; Taylor, J. Attenuated inspiratory muscle metaboreflex in endurance-trained individuals. Respir. Physiol. Neurobiol. 2011, 177, 24–29. [Google Scholar] [CrossRef]
- Turner, L.; Tecklenburg-Lund, S.; Chapman, R.; Stager, J.; Wilhite, D.; Mickleborough, T. Inspiratory muscle training lowers the oxygen cost of voluntary hyperpnea. J. Appl. Physiol. 2012, 112, 127–134. [Google Scholar] [CrossRef] [PubMed]
- McConnell, A.; Lomax, M. The influence of inspiratory muscle work history and specific inspiratory muscle training upon human limb muscle fatigue. J. Physiol. 2006, 577, 445–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McConnell, A.; Romer, L. Respiratory muscle training in healthy humans: Resolving the controversy. Int. J. Sports Med. 2004, 25, 284–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leddy, J.; Limprasertkul, A.; Patel, S.; Modlich, F.; Buyea, C.; Pendergast, D.; Lundgren, C. Isocapnic hyperpnea training improves performance in competitive male runners. Eur. J. Appl. Physiol. 2007, 99, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Lázaro, D.; Gallego-Gallego, D.; Corchete, L.; Fernández Zoppino, D.; González-Bernal, J.; García Gómez, B.; Mielgo-Ayuso, J. Inspiratory muscle training program using the powerbreath®: Does it have ergogenic potential for respiratory and/or athletic performance? a systematic review with meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 6703. [Google Scholar] [CrossRef] [PubMed]
- Walterspacher, S.; Pietsch, F.; Walker, D.; Röcker, K.; Kabitz, H. Activation of respiratory muscles during respiratory muscle training. Respir. Physiol. Neurobiol. 2018, 247, 126–132. [Google Scholar] [CrossRef]
- Boushel, R.; Piantadosi, C. Near-infrared spectroscopy for monitoring muscle oxygenation. Acta Physiol. Scand. 2000, 168, 615–622. [Google Scholar] [CrossRef] [Green Version]
- Contreras-Briceño, F.; Espinosa-Ramirez, M.; Hevia, G.; Llambias, D.; Carrasco, M.; Cerda, F.; López-Fuenzalida, A.; García, P.; Gabrielli, L.; Viscor, G. Reliability of NIRS portable device for measuring intercostal muscles oxygenation during exercise. J. Sports Sci. 2019, 37, 2653–2659. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Ramírez, M.; Moya-Gallardo, E.; Araya-Román, F.; Riquelme-Sánchez, S.; Rodriguez-García, G.; Reid, W.D.; Viscor, G.; Araneda, O.; Gabrielli, L.; Contreras-Briceño, F. Sex-differences in the oxygenation levels of intercostal and vastus lateralis muscles during incremental exercise. Front. Physiol. 2021, 12, 738063. [Google Scholar] [CrossRef]
- Barstow, T. Understanding near infrared spectroscopy and its application to skeletal muscle research. J. Appl. Physiol. 2019, 126, 1360–1376. [Google Scholar] [CrossRef]
- Perrey, S.; Ferrari, M. Muscle oximetry in sports science: A systematic review. Sport. Med. 2018, 48, 597–616. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Briceño, F.; Espinosa-Ramírez, M.; Moya-Gallardo, E.; Fuentes-Kloss, R.; Gabrielli, L.; Araneda, O.; Viscor, G. Intercostal muscles oxygenation and breathing pattern during exercise in competitive marathon runners. Int. J. Environ. Res. Public Health 2021, 18, 8287. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Briceño, F.; Espinosa-Ramirez, M.; Keim-Bagnara, V.; Carreño-Román, M.; Rodríguez-Villagra, R.; Villegas-Belmar, F.; Viscor, G.; Gabrielli, L.; Andía, M.; Araneda, O.; et al. Determination of the respiratory compensation point by detecting changes in intercostal muscles oxygenation by using Near-Infrared Spectroscopy. Life 2022, 12, 444. [Google Scholar] [CrossRef] [PubMed]
- Bretonneau, Q.; Bisschop, C.; Mons, V.; Pichon, A. Intercostal muscle oxygenation and expiratory loaded breathing at rest: Respiratory pattern effect. Respir. Physiol. Neurobiol. 2022, 304, 103925. [Google Scholar] [CrossRef] [PubMed]
- Melo, L.; Rodrigues, A.; Cabral, E.; Tanaka, T.; Goligher, E.; Brochard, L.; Reid, W.D. Prefrontal cortex activation during incremental inspiratory loading in healthy participants. Respir. Physiol. Neurobiol. 2022, 296, 103827. [Google Scholar] [CrossRef] [PubMed]
- Harriss, D.; Macsween, A.; Atkinson, G. Standards for ethics in sport and exercise science research: 2018 update. Int. J. Sports Med. 2017, 38, 1126–1131. [Google Scholar] [CrossRef] [Green Version]
- Martorell, M.; Labraña, A.M.; Ramírez-Alarcón, K.; Díaz-Martínez, X.; Garrido-Méndez, A.; Rodríguez-Rodríguez, F.; Cigarroa, I.; Vásquez, J.; Concha, Y.; Martínez-Sanguinetti, M.A.; et al. Comparison between self-reported and device measured physical activity according to nutritional status. Rev. Med. Chil. 2020, 148, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Gibson, G.; Whitelaw, W.; Siafakas, N.; Supinski, G.; Fitting, J.; Bellemare, F.; Loring, S.; Troyer, A.; Grassino, A. ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef]
- Knudson, R.; Lebowitz, M.; Holberg, C.; Burrows, B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am. Rev. Respir. Dis. 1983, 127, 725–734. [Google Scholar] [CrossRef]
- Hyatt, R.; Black, L. Maximal respiratory pressures: Normal values and relationship to age and sex. Am. Rev. Respir. Dis. 1969, 99, 696–702. [Google Scholar] [CrossRef]
- Cahalin, L.; Arena, R. Novel methods of inspiratory muscle training via the Test of Incremental Respiratory Endurance (TIRE). Exerc. Sport Sci. Rev. 2015, 43, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Day, J.; Rossiter, H.; Coats, E.; Skasick, A.; Whipp, B. The maximally attainable VO2 during exercise in humans: The peak vs. maximum issue. J. Appl. Physiol. 2003, 95, 1901–1907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work. Environ. Health 1990, 16, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Austin, K.; Daigle, K.; Patterson, P.; Cowman, J.; Chelland, S.; Haymes, E. Reliability of near-infrared spectroscopy for determining muscle oxygen saturation during exercise. Res. Q. Exerc. Sport 2005, 76, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Grassi, B.; Quaresima, V. Near-infrared spectroscopy and skeletal muscle oxidative function in vivo in health and disease: A review from an exercise physiology perspective. J. Biomed. Opt. 2016, 21, 91313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McManus, C.; Collison, J.; Cooper, C. Performance comparison of the MOXY and PortaMon near-infrared spectroscopy muscle oximeters at rest and during exercise. J. Biomed. Opt. 2018, 23, 01. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.; Sharpe, G.; Brown, P. Inspiratory muscle training improves cycling time-trial performance and anaerobic work capacity but not critical power. Eur. J. Appl. Physiol. 2007, 101, 761–770. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd. ed; Hillsdale, N.J.: Lawrence Erlbaum Associates; Routledge: London, UK, 1988; ISBN 0805802835. [Google Scholar]
- Vogiatzis, I.; Athanasopoulos, D.; Habazettl, H.; Kuebler, W.; Wagner, H.; Roussos, C.; Wagner, P.; Zakynthinos, S. Intercostal muscle blood flow limitation in athletes during maximal exercise. J. Physiol. 2009, 587, 3665–3677. [Google Scholar] [CrossRef]
- Athanasopoulos, D.; Louvaris, Z.; Cherouveim, E.; Andrianopoulos, V.; Roussos, C.; Zakynthinos, S.; Vogiatzis, I. Expiratory muscle loading increases intercostal muscle blood flow during leg exercise in healthy humans. J. Appl. Physiol. 2010, 109, 388–395. [Google Scholar] [CrossRef] [Green Version]
- Alvares, T.; Oliveira, G.; Soares, R.; Murias, J. Near-infrared spectroscopy-derived total haemoglobin as an indicator of changes in muscle blood flow during exercise-induced hyperaemia. J. Sports Sci. 2020, 38, 751–758. [Google Scholar] [CrossRef]
- Bailey, S.; Romer, L.; Kelly, J.; Wilkerson, D.; DiMenna, F.; Jones, A. Inspiratory muscle training enhances pulmonary O2 uptake kinetics and high-intensity exercise tolerance in humans. J. Appl. Physiol. 2010, 109, 457–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marostegan, A.B.; Gobatto, C.A.; Rasteiro, F.M.; Hartz, C.S.; Moreno, M.A.; Manchado-Gobatto, F.B. Effects of different inspiratory muscle warm-up loads on mechanical, physiological and muscle oxygenation responses during high-intensity running and recovery. Sci. Rep. 2022, 12, 11223. [Google Scholar] [CrossRef]
- Walker, D.; Walterspacher, S.; Schlager, D.; Ertl, T.; Roecker, K.; Windisch, W.; Kabitz, H. Characteristics of diaphragmatic fatigue during exhaustive exercise until task failure. Respir. Physiol. Neurobiol. 2011, 176, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Illi, S.; Held, U.; Frank, I.; Spengler, C. Effect of respiratory muscle training on exercise performance in healthy individuals: A systematic review and meta-analysis. Sport. Med. 2012, 42, 707–724. [Google Scholar] [CrossRef] [PubMed]
- Uemura, H.; Lundgren, C.; Ray, A.; Pendergast, D. Effects of different types of respiratory muscle training on exercise performance in runners. Mil. Med. 2012, 177, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Van Hollebeke, M.; Gosselink, R.; Langer, D. Training specificity of inspiratory muscle training methods: A randomized trial. Front. Physiol. 2020, 11, 1551. [Google Scholar] [CrossRef] [PubMed]
- Ramsook, A.; Molgat-Seon, Y.; Schaeffer, M.; Wilkie, S.; Camp, P.; Reid, W.D.; Romer, L.; Guenette, J. Effects of inspiratory muscle training on respiratory muscle electromyography and dyspnea during exercise in healthy men. J. Appl. Physiol. 2017, 122, 1267–1275. [Google Scholar] [CrossRef] [Green Version]
- Salazar-Martínez, E.; de Matos, T.; Arrans, P.; Santalla, A. Ventilatory efficiency response is unaffected by fitness level, ergometer type, age or body mass index in male athletes. Biol. Sport 2018, 35, 393–398. [Google Scholar] [CrossRef]
- Richardson, R.; Poole, D.; Knight, D.; Kurdak, S.; Hogan, M.; Grassi, B.; Johnson, E.; Kendrick, K.; Erickson, B.; Wagner, P. High muscle blood flow in man: Is maximal O2 extraction compromised? J. Appl. Physiol. 1993, 75, 1911–1916. [Google Scholar] [CrossRef]
- Feldmann, A.; Schmitz, R.; Erlacher, D. Near-infrared spectroscopy-derived muscle oxygen saturation on a 0% to 100% scale: Reliability and validity of the Moxy monitor. J. Biomed. Opt. 2019, 24, 115001. [Google Scholar] [CrossRef]
- HajGhanbari, B.; Yamabayashi, C.; Bruna, T.B.; Coelho, J.D.; Freedman, K.D.; Morton, T.A.; Palmer, S.A.; Toy, M.A.; Walsh, C.; William Sheel, A.; et al. Effect of Respiratory Muscle Training on Performance in Athletes: A Systematic Review with Meta-Analyses. Strength Cond. 2008, 22, 903–909. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VIH (n = 12) | ITL (n = 12) | p-Value | [95% CI] | |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Sex (men/women) | 6/6 | 6/6 | - | - |
| Age (years) | 22 ± 1 | 21 ± 1 | 0.45 | [−1.2–0.6] |
| Height (cm) | 169 ± 7 | 169 ± 11 | 0.90 | [−7.6–6.7] |
| Weight (kg) | 62 ± 9 | 64 ± 12 | 0.63 | [−6.3–10.2] |
| BMI (kg⋅m−2) | 21.6 ± 1.6 | 22.3 ± 2.6 | 0.33 | [−0.8–2.1] |
| Physical activity (min·week−1) | ||||
| Light | 81 ± 21 | 83 ± 27 | 0.86 | [−18.6–22.1] |
| Moderate | 223 ± 29 | 236 ± 24 | 0.23 | [−9.4–36.1] |
| Vigorous | 83 ± 25 | 82 ± 26 | 0.90 | [−22.6–20.1] |
| Total | 387 ± 44 | 401 ± 33 | 0.39 | [−19.3–46.9] |
| FVC (L) | 4.9 ± 0.7 | 4.8 ± 1.8 | 0.74 | [−0.8–0.6] |
| FEV1 (L) | 4.1 ± 0.5 | 4.0 ± 1.5 | 0.78 | [−0.6–0.5] |
| FEV1⋅FVC−1 (%) | 82.6 ± 4.6 | 83.3 ± 5.2 | 0.71 | [−3.1–4.5] |
| MIP (cm H2O) | 120 ± 17 | 138 ± 24 | 0.06 | [−0.7–33.8] |
| IRE (s) | 694 ± 146 | 707 ± 127 | 0.81 | [−102–129] |
| CPET pre-RMT | ||||
| O2-peak (mL·kg−1·min−1) | 46 ± 8 | 45 ± 6 | 0.71 | [−6.5–4.5] |
| Heart rate-peak (bpm) | 182 ± 8 | 181 ± 9 | 0.94 | [−7.3–6.8] |
| Workload-peak (watts) | 215 ± 46 | 218 ± 58 | 0.90 | [−41–46] |
| Time to exhaustion (s) | 822 ± 189 | 843 ± 223 | 0.80 | [−153–196] |
| Respiratory rate-peak (cpm) | 48 ± 10 | 55 ± 13 | 0.15 | [−2.6–15.9] |
| Tidal volume-peak (L) | 2.6 ± 0.6 | 2.6 ± 1.4 | 0.84 | [−0.6–0.5] |
| Lung ventilation-peak (L·min−1) | 123 ± 28 | 142 ± 51 | 0.29 | [−16–52] |
| ∆SmO2-m. intercostales (%) | 42 ± 21 | 40 ± 14 | 0.73 | [−17–12] |
| ∆tHb-m. intercostales (g·dL−1) | 0.2 ± 0.2 | 0.2 ± 0.5 | 0.80 | [−0.4–0.3] |
| ∆SmO2-m. vastus lateralis (%) | 45 ± 18 | 44 ± 17 | 0.85 | [−16–13] |
| ∆tHb-m. vastus lateralis (g·dL−1) | 0.2 ± 0.2 | 0.2 ± 0.3 | 0.64 | [−0.3–0.2] |
| Variable | Training Groups | Two-Way ANOVA Results (p-Values) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| VIH | ITL | Factor | Interaction | Multiple Comparison | ||||||||||
| Pre (Mean ± SD) | Post (Mean ± SD) | Effect Size | Pre (Mean ± SD) | Post (Mean ± SD) | Effect Size | Time | Effect Size | Groups | Effect Size | Time × Group | Effect Size | VIH-pre vs. VIH-post / ITL-pre vs. ITL-post | VIH-pre vs. ILT-pre / VIH-post vs. ILT-post | |
| CPET test | ||||||||||||||
| O2-peak (mL·kg−1·min−1) | 46 ± 8 | 47 ± 8 | 0.12 | 45 ± 6 | 48 ± 8 | 0.40 | <0.01 ** | 0.56 | 0.95 | 0.04 | 0.02 * | 0.37 | 0.82/<0.01 ** | 0.58/0.16 |
| O2-peak(mL·min−1) | 2874 ± 732 | 2721 ± 754 | 0.19 | 2902 ± 739 | 3104 ± 897 | 0.24 | 0.01 * | 0.51 | 0.55 | 0.46 | 0.03* | 0.34 | 0.89/0.01 * | 0.95/0.01 * |
| Peak workload (watts) | 215 ± 46 | 224 ± 49 | 0.18 | 216 ± 58 | 220 ± 57 | 0.07 | 0.09 | 0.26 | 0.96 | 0.00 | 0.29 | 0.10 | - | - |
| Peak workload-to-weight | 3.4 ± 0.5 | 3.6 ± 0.5 | 0.38 | 3.4 ± 1.2 | 3.4 ± 1.2 | 0.03 | 0.06 | 0.29 | 0.53 | 0.47 | 0.30 | 0.08 | - | - |
| Time to exhaustion (s) | 822 ± 189 | 858 ± 198 | 0.17 | 844 ± 223 | 853 ± 222 | 0.04 | 0.09 | 0.57 | 0.90 | 0.14 | 0.05 | 0.30 | - | - |
| Heart rate-peak (bpm) | 182 ± 8 | 188 ± 7 | 0.77 | 181 ± 9 | 184 ± 11 | 0.29 | 0.09 | 0.23 | 0.46 | 0.07 | 0.43 | 0.06 | - | - |
| ∆Heart rate (bpm) | 96 ± 8 | 106 ± 13 | 0.89 | 99 ± 19 | 107 ± 14 | 0.46 | <0.01 ** | 0.65 | 0.67 | 0.06 | 0.68 | 0.02 | 0.01 */0.04 * | - |
| Respiratory rate-peak (cpm) | 48 ± 10 | 53 ± 9 | 0.37 | 55 ± 13 | 53 ± 11 | 0.13 | 0.53 | 0.03 | 0.36 | 0.23 | 0.17 | 0.16 | - | - |
| ∆Respiratory rate (cpm) | 33 ± 9 | 38 ± 11 | 0.48 | 39 ± 13 | 38 ± 11 | 0.08 | 0.46 | 0.06 | 0.42 | 0.18 | 0.25 | 0.12 | - | - |
| Tidal volume-peak (L) | 2.6 ± 0.6 | 2.5 ± 0.7 | 0.14 | 2.6 ± 1.4 | 2.3 ± 1.2 | 0.21 | <0.01 ** | 0.44 | 0.67 | 0.24 | 0.34 | 0.08 | 0.39/0.03 * | - |
| ∆Tidal volume (L) | 1.7 ± 0.7 | 1.5 ± 0.6 | 0.29 | 1.8 ± 1.4 | 1.4 ± 1.2 | 0.29 | 0.02 * | 0.32 | 0.94 | 0.00 | 0.40 | 0.06 | 0.76/0.18 | - |
| Lung ventilation-peak (L·min−1) | 124 ± 28 | 130 ± 37 | 0.17 | 142 ± 51 | 125 ± 39 | 0.36 | 0.37 | 0.08 | 0.61 | 0.12 | 0.05 | 0.29 | - | - |
| ∆Lung ventilation (L·min−1) | 110 ± 30 | 114 ± 36 | 0.12 | 130 ± 50 | 112 ± 38 | 0.39 | 0.31 | 0.11 | 0.47 | 0.19 | 0.07 | 0.27 | - | - |
| Ventilatory efficiency | 26 ± 3 | 26 ± 3 | 0.16 | 26 ± 5 | 25 ± 4 | 0.30 | 0.02 * | 0.41 | 0.97 | 0.00 | 0.01 * | 0.41 | 0.99/0.03 * | 0.76/0.84 |
| Spirometry test | ||||||||||||||
| FEV1 (L) | 4.1 ± 0.5 | 4.2 ± 0.5 | 0.26 | 4.0 ± 1.5 | 3.9 ± 1.5 | 0.06 | 0.08 | 0.26 | 0.42 | 0.47 | 0.92 | 0.00 | - | - |
| FVC (L) | 4.9 ± 0.7 | 4.9 ± 0.8 | 0.03 | 4.8 ± 1.8 | 4.6 ± 1.8 | 0.12 | 0.03 * | 0.25 | 0.90 | 0.00 | 0.93 | 0.00 | 0.37/0.45 | - |
| FEV1⋅ FVC−1 (%) | 83 ± 5 | 86 ± 11 | 0.41 | 83 ± 5.1 | 85 ± 6 | 0.34 | 0.02 * | 0.35 | 0.88 | 0.01 | 0.41 | 0.06 | 0.08/0.57 | - |
| Respiratory muscle performance | ||||||||||||||
| MIP (cmH2O) | 120 ± 17 | 140 ± 15 | 1.20 | 137 ± 24 | 186 ± 33 | 1.64 | <0.01 ** | 0.90 | <0.01 ** | 0.88 | <0.01 ** | 0.61 | <0.01 **/< 0.01 ** | 0.02 */<0.01 ** |
| MIP regard to predicted (%) | 105 ± 14 | 124 ± 19 | 1.09 | 123 ± 20 | 166 ± 20 | 2.07 | <0.01 ** | 0.90 | <0.01 *** | 0.90 | <0.01 ** | 0.60 | <0.01 **/<0.01 *** | <0.01 **/<0.01 ** |
| IRE (S) | 694 ± 146 | 797 ± 56 | 0.89 | 707 ± 127 | 924 ± 120 | 1.69 | <0.01 ** | 0.76 | 0.06 | 0.41 | 0.04 * | 0.32 | 0.16/<0.01 *** | 0.98/0.01 * |
| Muscle oxygenation | ||||||||||||||
| SmO2-m. intercostales-peak (%) | 43 ± 23 | 52 ± 26 | 0.35 | 43 ± 17 | 52 ± 26 | 0.39 | <0.01 ** | 0.46 | 0.86 | 0.03 | 0.95 | 0.00 | 0.15/0.13 | - |
| ∆SmO2-m. intercostales (%) | 42 ± 21 | 30 ± 19 | 0.59 | 40 ± 14 | 32 ± 18 | 0.48 | <0.01 ** | 0.53 | 0.95 | 0.00 | 0.49 | 0.04 | 0.02 */0.02 * | - |
| SmO2-m. vastus lateralis-peak (%) | 37 ± 19 | 39 ± 21 | 0.09 | 34 ± 12 | 32 ± 11 | 0.17 | 0.52 | 0.02 | 0.88 | 0.00 | 0.18 | 0.02 | - | - |
| ∆SmO2-m. vastus lateralis (%) | 45 ± 18 | 41 ± 19 | 0.21 | 44 ± 17 | 44 ± 19 | 0.01 | 0.55 | 0.06 | 0.91 | 0.01 | 0.31 | 0.09 | - | - |
| tHb-m. intercostales-peak (g·dL−1) | 12.0 ± 0.3 | 12.1 ± 0.4 | 0.27 | 12.1 ± 1.3 | 12.2 ± 1.3 | 0.07 | 0.65 | 0.01 | 0.52 | 0.18 | 0.47 | 0.01 | - | - |
| ∆tHb-m. intercostales (g·dL−1) | 0.2 ± 0.2 | 0.1 ± 0.2 | 0.48 | 0.2 ± 1.3 | 0.2 ± 1.0 | 0.01 | 0.55 | 0.03 | 0.42 | 0.00 | 0.98 | 0.02 | - | - |
| tHb-m. vastus lateralis-peak (g·dL−1) | 12.1 ± 0.6 | 11.9 ± 0.6 | 0.32 | 12.0 ± 1.2 | 12.1 ± 1.1 | 0.08 | 0.28 | 0.15 | 0.71 | 0.13 | 0.02 * | 0.42 | 0.07/0.77 | 0.74/0.08 |
| ∆tHb-m. vastus lateralis (g·dL−1) | 0.2 ± 0.2 | 0.3 ± 0.2 | 0.48 | 0.2 ± 1.2 | 0.3 ± 0.9 | 0.09 | 0.42 | 0.10 | 0.77 | 0.05 | 0.52 | 0.04 | - | - |
| Related variables | ||||||||||||||
| ∆SmO2-m. intercostales · ∆VE−1 | 0.4 ± 0.2 | 0.3 ± 0.2 | 0.48 | 0.4 ± 0.9 | 0.3 ± 1.0 | 0.10 | <0.01 ** | 0.39 | 0.75 | 0.07 | 0.07 | 0.26 | 0.01 */0.99 | - |
| ∆SmO2-m. vastus lateralis · PtW−1 | 13 ± 4 | 11 ± 4 | 0.48 | 13 ± 5 | 13 ± 6 | 0.01 | 0.26 | 0.20 | 0.64 | 0.16 | 0.25 | 0.12 | - | - |
| Ratio SmO2 | 1.1 ± 0.7 | 0.8 ± 0.6 | 0.48 | 1.1 ± 1.4 | 0.9 ± 1.5 | 0.13 | 0.02 * | 0.28 | 0.79 | 0.03 | 0.49 | 0.05 | 0.14/0.70 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espinosa-Ramírez, M.; Riquelme, S.; Araya, F.; Rodríguez, G.; Figueroa-Martínez, F.; Gabrielli, L.; Viscor, G.; Reid, W.D.; Contreras-Briceño, F. Effectiveness of Respiratory Muscles Training by Voluntary Isocapnic Hyperpnea Versus Inspiratory Threshold Loading on Intercostales and Vastus Lateralis Muscles Deoxygenation Induced by Exercise in Physically Active Adults. Biology 2023, 12, 219. https://doi.org/10.3390/biology12020219
Espinosa-Ramírez M, Riquelme S, Araya F, Rodríguez G, Figueroa-Martínez F, Gabrielli L, Viscor G, Reid WD, Contreras-Briceño F. Effectiveness of Respiratory Muscles Training by Voluntary Isocapnic Hyperpnea Versus Inspiratory Threshold Loading on Intercostales and Vastus Lateralis Muscles Deoxygenation Induced by Exercise in Physically Active Adults. Biology. 2023; 12(2):219. https://doi.org/10.3390/biology12020219
Chicago/Turabian StyleEspinosa-Ramírez, Maximiliano, Santiago Riquelme, Felipe Araya, Guido Rodríguez, Fernanda Figueroa-Martínez, Luigi Gabrielli, Ginés Viscor, W. Darlene Reid, and Felipe Contreras-Briceño. 2023. "Effectiveness of Respiratory Muscles Training by Voluntary Isocapnic Hyperpnea Versus Inspiratory Threshold Loading on Intercostales and Vastus Lateralis Muscles Deoxygenation Induced by Exercise in Physically Active Adults" Biology 12, no. 2: 219. https://doi.org/10.3390/biology12020219
APA StyleEspinosa-Ramírez, M., Riquelme, S., Araya, F., Rodríguez, G., Figueroa-Martínez, F., Gabrielli, L., Viscor, G., Reid, W. D., & Contreras-Briceño, F. (2023). Effectiveness of Respiratory Muscles Training by Voluntary Isocapnic Hyperpnea Versus Inspiratory Threshold Loading on Intercostales and Vastus Lateralis Muscles Deoxygenation Induced by Exercise in Physically Active Adults. Biology, 12(2), 219. https://doi.org/10.3390/biology12020219