
Applicability of International Autoimmune Hepatitis Group (IAIHG) Scoring System for Autoimmune Hepatitis in Pediatrics
 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, P.J.; McFarlane, I.G. Meeting report: International autoimmune hepatitis group. Hepatology 1993, 18, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Kaya, M.; Angulo, P.; Lindor, K.D. Overlap of autoimmune hepatitis and primary sclerosing cholangitis: An evaluation of a modified scoring system. J. Hepatol. 2000, 33, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Omagari, K.; Masuda, J.I.; Kato, Y.; Nakata, K.; Kanematsu, T.; Kusumoto, Y.; Mori, I.; Furukawa, R.; Tanioka, H.; Tajima, H.; et al. Re-analysis of clinical features of 89 patients with autoimmune hepatitis using the revised scoring system proposed by the International Autoimmune Hepatitis Group. Intern. Med. 2000, 39, 1008–1012. [Google Scholar] [CrossRef]
- Alvarez, F.; Berg, P.A.; Bianchi, F.B.; Bianchi, L.; Burroughs, A.K.; Cancado, E.L.; Chapman, R.W.; Cooksley, W.G.E.; Czaja, A.J.; Desmet, V.J.; et al. International Autoimmune Hepatitis Group Report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar] [CrossRef]
- Ebbeson, R.; Schreiber, R. Diagnosing autoimmune hepatitis in children: Is the International Autoimmune Hepatitis Group scoring system useful? Clin. Gastroenterol. Hepatol. 2004, 2, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Arinaga-Hino, T.; Ohira, H.; Abe, K.; Torimura, T.; Zeniya, M.; Abe, M.; Yoshizawa, K.; Takaki, A.; Suzuki, Y.; et al. Non-alcoholic fatty liver disease in patients with autoimmune hepatitis. JGH Open. 2018, 2, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, A.; Tomar, R.; Reveille, J.; Solomon, D.H.; Homburger, H.A. Guidelines for clinical use of the antinuclear antibody test and tests for specific autoantibodies to nuclear antigens. American College of Pathologists. Arch. Pathol. Lab. Med. 2000, 124, 71–81. [Google Scholar] [CrossRef]
- Muratori, P.; Granito, A.; Pappas, G.; Muratori, L. Validation of simplified diagnostic criteria for autoimmune hepatitis in italian patients. Hepatology 2009, 49, 1782–1783. [Google Scholar] [CrossRef]
- Pathak, S.; Kamat, D. Autoimmune Hepatitis in Children. Pediatr. Ann. 2018, 47, e81–e86. [Google Scholar] [CrossRef]
- Mieli-Vergani, G.; Vergani, D.; Czaja, A.J.; Manns, M.P.; Krawitt, E.L.; Vierling, J.M.; Lohse, A.W.; Montano-Loza, A.J. Autoimmune hepatitis. Nat. Rev. Dis. Prim. 2018, 4, 18017. [Google Scholar] [CrossRef]
- Czaja, A.J.; Freese, D.K. Diagnosis and treatment of autoimmune hepatitis. Hepatology 2002, 36, 479–497. [Google Scholar] [CrossRef] [PubMed]
- Rockey, D.C.; Seeff, L.B.; Rochon, J.; Freston, J.; Chalasani, N.; Bonacini, M.; Fontana, R.J.; Hayashi, P.H.; US Drug-Induced Liver Injury Network. Causality assessment in drug-induced liver injury using a structured expert opinion process: Comparison to the Roussel-Uclaf causality assessment method. Hepatology 2010, 51, 2117–2126. [Google Scholar] [CrossRef] [PubMed]
- Lohse, A.W.; Mieli-Vergani, G. Autoimmune hepatitis. J. Hepatol. 2011, 55, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Granito, A.; Muratori, L.; Pappas, G.; Ferri, S.; Cassani, F.; Lenzi, M.; Bianchi, F.B.; Muratori, P. Clinical features of type 1 autoimmune hepatitis in elderly Italian patients. Aliment. Pharmacol. Ther. 2005, 21, 1273–1277. [Google Scholar] [CrossRef] [PubMed]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar] [CrossRef]
- Muratori, P.; Czaja, A.J.; Muratori, L.; Granito, A.; Guidi, M.; Ferri, S.; Volta, U.; Mantovani, W.; Pappas, G.; Cassani, F.; et al. Evidence of a genetic basis for the different geographic occurrences of liver/kidney microsomal antibody type 1 in hepatitis C. Dig. Dis. Sci. 2007, 52, 179–184. [Google Scholar] [CrossRef]
- Mieli-Vergani, G.; Vergani, D.; Baumann, U.; Czubkowski, P.; Debray, D.; Dezsofi, A.; Fischler, B.; Gupte, G.; Hierro, L.; Indolfi, G.; et al. Diagnosis and Management of Pediatric Autoimmune Liver Disease: ESPGHAN Hepatology Committee Position Statement. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 345–360. [Google Scholar] [CrossRef]
- Fallatah, H.I.; Akbar, H.O. Autoimmune liver disease—Are there spectra that we do not know? Comp. Hepatol. 2011, 12, 10. [Google Scholar] [CrossRef]
- Lala, V.; Zubair, M.; Minter, D.A. Liver Function Tests. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Montano-Loza, A.J.; Carpenter, H.A.; Czaja, A.J. Improving the end point of corticosteroid therapy in type 1 autoimmune hepatitis to reduce the frequency of relapse. Am. J. Gastroenterol. 2007, 102, 1005–1012. [Google Scholar] [CrossRef]
- Vuppalanchi, R.; Chalasani, N. 5–Laboratory tests in liver disease. In Practical Hepatic Pathology: A Diagnostic Approach; Sanders (Elsevier): Philadelphia, PA, USA, 2011; pp. 55–62. [Google Scholar]
- Danan, G.; Teschke, R. RUCAM in Drug and Herb Induced Liver Injury: The Update. Int. J. Mol. Sci. 2015, 17, 14. [Google Scholar] [CrossRef]
- Patton, H.; Lavine, J.E.; Van Natta, M.L.; Schwimmer, J.B.; Kleiner, D.; Molleston, J.; Nonalcoholic Steatohepatitis Clinical Research Network. Clinical Correlates of Histopathology in Pediatric Nonalcoholic Steatohepatitis. Gastroenterology 2008, 135, 1961–1971.e2. [Google Scholar] [CrossRef] [PubMed]
- Dalekos, G.N.; Gatselis, N.K.; Koukoulis, G.K. Non-alcoholic steatohepatitis or autoimmune hepatitis? Sometimes a closer look under the surface is needed. BMJ Case Rep. 2020, 13, e238400. [Google Scholar] [CrossRef]
- Yodoshi, T.; Orkin, S.; Arce-Clachar, A.C.; Bramlage, K.; Xanthakos, S.A.; Mouzaki, M.; Valentino, P.L. Significance of autoantibody seropositivity in children with obesity and non-alcoholic fatty liver disease. Pediatr. Obes. 2021, 16, e12696. [Google Scholar] [CrossRef] [PubMed]
- Hennes, E.M.; Zeniya, M.; Czaja, A.J.; Parés, A.; Dalekos, G.N.; Krawitt, E.L.; Bittencourt, P.L.; Porta, G.; Boberg, K.M.; Hofer, H.; et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008, 48, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Miao, Q.; Bian, Z.; Tang, R.; Zhang, H.; Wang, Q.; Huang, S.; Xiao, X.; Shen, L.; Qiu, D.; Krawitt, E.L.; et al. Emperipolesis mediated by CD8 T cells is a characteristic histopathologic feature of autoimmune hepatitis. Clin. Rev. Allergy Immunol. 2015, 48, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Harrington, C.; Krishnan, S.; Mack, C.L.; Cravedi, P.; Assis, D.N.; Levitsky, J. Noninvasive biomarkers for the diagnosis and management of autoimmune hepatitis. Hepatology 2022, 76, 1862–1879. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All Cases | AIH Cases | Control Cases |
|---|---|---|---|
| Total Cases, N | 61 | 32 | 29 |
| Age, Years, Median (IQR) | 13 (8–16) | 14 (8–15) | 12 (10–16) |
| Sex | |||
| Male, N (%) | 29 (48) | 12 (38) | 17 (59) |
| Female, N (%) | 32 (52) | 20 (63) | 12 (41) |
| Race | |||
| White, N (%) | 31 (51) | 19 (59) | 12 (41) |
| Black, N (%) | 12 (20) | 11 (34) | 1 (3) |
| Other/Unknown, N (%) | 18 (30) | 2 (6) | 16 (55) |
| Biomarker | AUROC (95% CI) | Standard Error | Optimized Cut-Off | Sensitivity | Specificity |
|---|---|---|---|---|---|
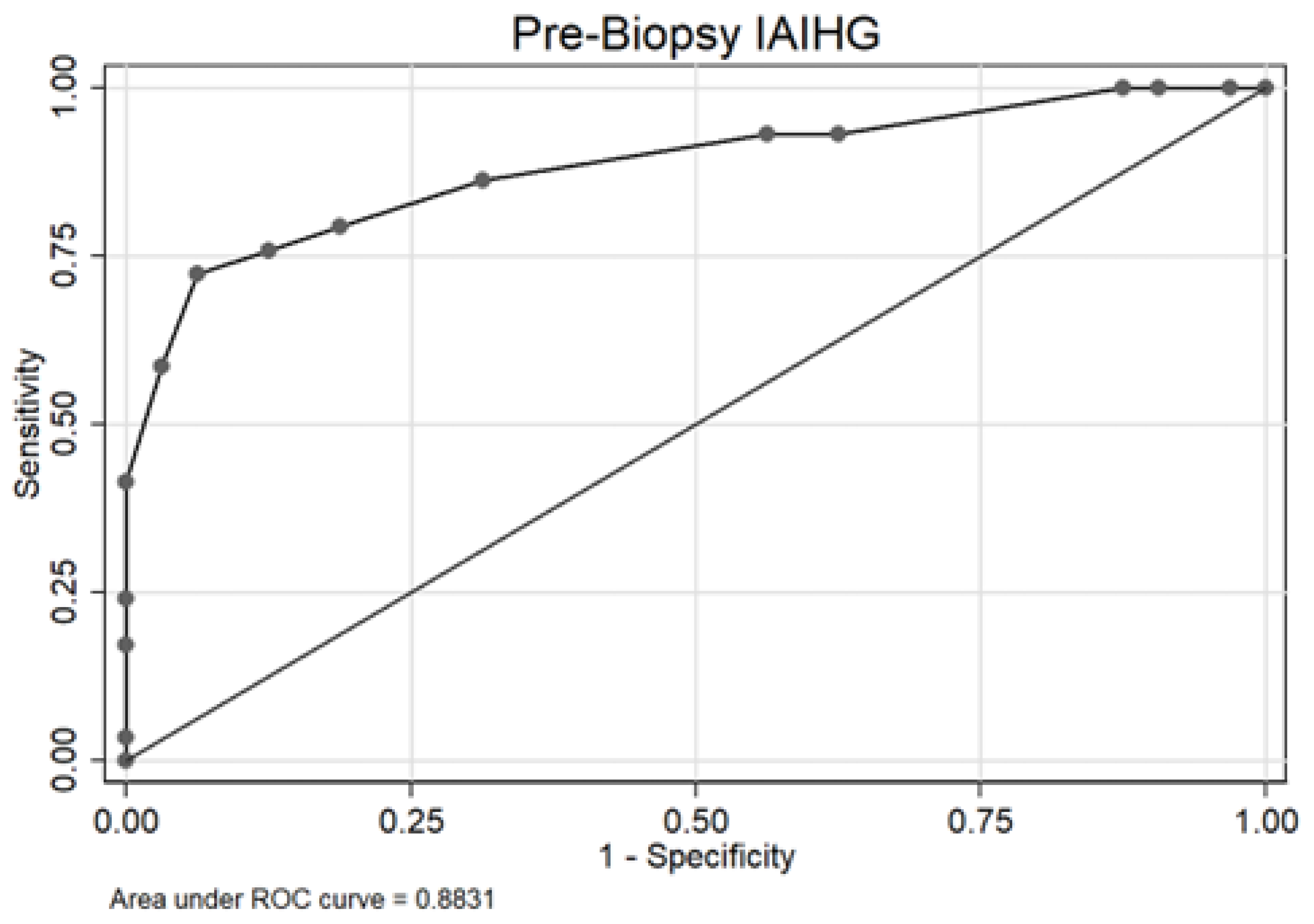
| Pre-liver biopsy IAIHG score | 0.88 (0.80–0.97) | 0.04 | ≥9 | 72% | 94% |
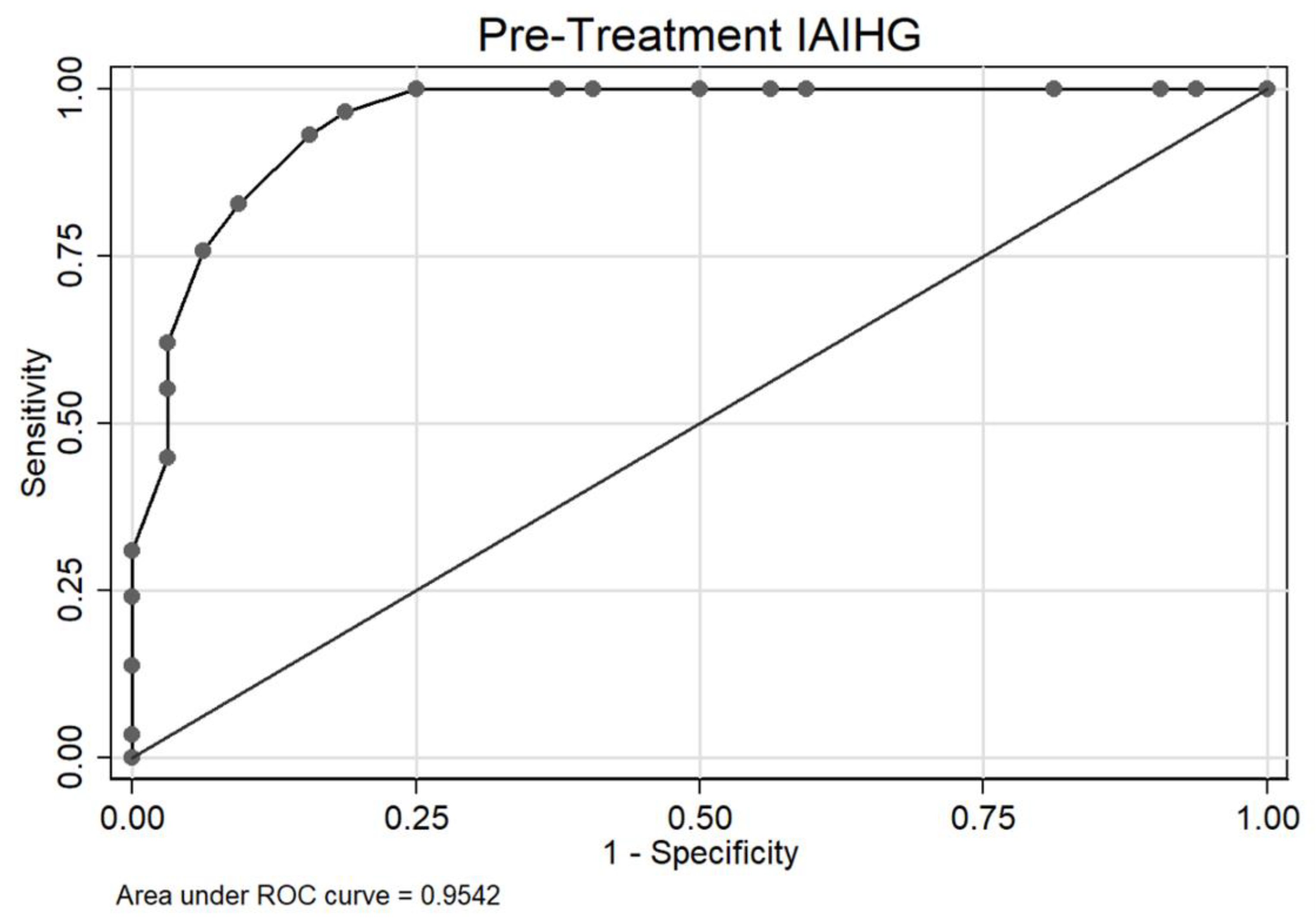
| Pre treatment IAIHG score with HLA | 0.95 (0.91–1.00) | 0.02 | ≥7 | 97% | 81% |
| Post treatment IAIHG score with HLA | N/A | N/A | N/A | N/A | N/A |
| Simplified AIH score | 0.91 (0.84–0.98) | 0.04 | ≥5 | 69% | 97% |
| Risk Factors | Odds Ratio (95% CI) | p-Value | |
|---|---|---|---|
| Demographics | |||
| Age (Year) | ≥12 (vs. <12) | 0.74 (0.26–2.06) | 0.562 |
| Sex | Female (vs. Male) | 2.10 (0.76–6.00) | 0.155 |
| Race | White (vs. Other) | 1.82 (0.66–5.13) | 0.248 |
| Black (vs. Other) | 7.89 (1.83–55.15) | 0.013 | |
| Asian/Unknown (vs. Other) | 0.07 (0.01–0.30) | 0.001 | |
| Biopsy | |||
| Consistent with AIH | Yes/No | 66.41 (11.44–100.00) | <0.001 |
| Biliary Changes | Yes/No | 1.72 (0.48–6.52) | 0.407 |
| Interface Hepatitis | Yes/No | 21.88 (3.82–100.00) | 0.004 |
| Predominant Plasma Cells | Yes/No | 39.38 (9.13–100.00) | <0.001 |
| Fibrosis | Yes/No | 0.72 (0.26–1.96) | 0.518 |
| Clinical | |||
| Autoimmune Disease in Family | Yes/No | 1.09 (0.39–3.00) | 0.873 |
| Recent Hepatotoxic Drug Use | Yes/No | 3.50 (0.68–26.19) | 0.158 |
| 6-Mercaptopurine Therapy | Yes/No | 8.31 (2.49–33.76) | 0.001 |
| Steroid Therapy | Yes/No | 100.00 (24.10–100.00) | <0.001 |
| Ulcerative Colitis | Yes/No | 1.67 (0.26–13.46) | 0.589 |
| Viral Hepatitis Screen | |||
| Hepatitis A Virus | Yes/No | 3.43 (0.40–72.25) | 0.302 |
| Hepatitis B Virus | Yes/No | N/A | N/A |
| Hepatitis C Virus | Yes/No | N/A | N/A |
| Hepatitis E Virus | Yes/No | N/A | 0.996 |
| Herpes Simplex Virus I/II | Yes/No | 1.33 (0.12–31.69) | 0.825 |
| Laboratory | |||
| ANA | Yes/No | 5.70 (1.88–19.02) | 0.003 |
| ASMA | Yes/No | 3.58 (1.17–12.09) | 0.031 |
| Anti-LKM-1 | Yes/No | N/A | 0.991 |
| AMA | Yes/No | 0.81 (0.03–21.25) | 0.882 |
| p-ANCA | Yes/No | 0.78 (0.08–7.86) | 0.822 |
| IgG (mg/dL) | >1600 (vs. ≤1600) | 16.00 (2.65–100.00) | 0.012 |
| AST (U/L) | >40 (vs. ≤40) | 4.13 (1.10–20.20) | 0.049 |
| ALT (U/L) | >56 (vs. ≤56) | 1.96 (0.59–7.24) | 0.285 |
| GGT (U/L) | >30 (vs. ≤30) | 4.41 (1.30–17.95) | 0.024 |
| Alkaline Phosphatase (U/L) | >140 (vs. ≤140) | 5.47 (1.50–26.53) | 0.017 |
| Total Bilirubin (mg/dL) | >1.2 (vs. ≤1.2) | 9.21 (2.75–37.67) | <0.001 |
| Direct Bilirubin (mg/dL) | >0.3 (vs. ≤0.3) | 7.34 (2.11–30.85) | 0.003 |
| Creatine Kinase (U/L) | >200 (vs. ≤200) | 2.34 (0.35–19.32) | 0.379 |
| C- Reactive Protein (mg/dL) | >0.8 (vs. ≤0.8) | 1.02 (0.27–3.87) | 0.975 |
| Hemoglobin (g/dL) | <12.0 (vs. ≥12.0) | 4.18 (1.47–12.68) | 0.009 |
| INR | >1.1 (vs. ≤1.1) | 4.06 (1.27–14.74) | 0.023 |
| Erythrocyte Sedimentation Rate (mm/h) | >20 (vs. ≤20) | 3.95 (0.97–20.47) | 0.070 |
| White Blood Count (/cu mm) | >11,000 (vs. ≤11,000) | 0.57 (0.14–2.14) | 0.416 |
| Platelet Count (K/cu mm) | <150 (vs. ≥150) | 8.09 (1.00–100.00) | 0.061 |
| BMI (kg/m2) | >24.9 (vs. ≤24.9) | 0.22 (0.07–0.65) | 0.009 |
| Biopsy Data | Sensitivity | Specificity |
|---|---|---|
| Consistent with AIH | 72% | 97% |
| Biliary changes | 24% | 84% |
| Interface hepatitis | 41% | 97% |
| Predominant plasma cells | 72% | 94% |
| Fibrosis | 45% | 47% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakulsaengprapha, V.; Wasuwanich, P.; Naraparaju, G.; Korotkaya, Y.; Thawillarp, S.; Oshima, K.; Karwowski, C.; Scheimann, A.O.; Karnsakul, W. Applicability of International Autoimmune Hepatitis Group (IAIHG) Scoring System for Autoimmune Hepatitis in Pediatrics. Biology 2023, 12, 479. https://doi.org/10.3390/biology12030479
Sakulsaengprapha V, Wasuwanich P, Naraparaju G, Korotkaya Y, Thawillarp S, Oshima K, Karwowski C, Scheimann AO, Karnsakul W. Applicability of International Autoimmune Hepatitis Group (IAIHG) Scoring System for Autoimmune Hepatitis in Pediatrics. Biology. 2023; 12(3):479. https://doi.org/10.3390/biology12030479
Chicago/Turabian StyleSakulsaengprapha, Vorada, Paul Wasuwanich, Gayathri Naraparaju, Yelena Korotkaya, Supharerk Thawillarp, Kiyoko Oshima, Christine Karwowski, Ann O. Scheimann, and Wikrom Karnsakul. 2023. "Applicability of International Autoimmune Hepatitis Group (IAIHG) Scoring System for Autoimmune Hepatitis in Pediatrics" Biology 12, no. 3: 479. https://doi.org/10.3390/biology12030479
APA StyleSakulsaengprapha, V., Wasuwanich, P., Naraparaju, G., Korotkaya, Y., Thawillarp, S., Oshima, K., Karwowski, C., Scheimann, A. O., & Karnsakul, W. (2023). Applicability of International Autoimmune Hepatitis Group (IAIHG) Scoring System for Autoimmune Hepatitis in Pediatrics. Biology, 12(3), 479. https://doi.org/10.3390/biology12030479