Metabolically Healthy Obesity Is a Misnomer: Components of the Metabolic Syndrome Linearly Increase with BMI as a Function of Age and Gender

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Outcomes
2.3. Statistical Analysis
3. Results
3.1. Prevalence of Completely Metabolically Healthy Subjects as a Function of Gender and BMI Groups
3.2. Normometabolic Non-Obese (NO-NM) Subjects Have a More Favorable Cardiometabolic Profile Than Normometabolic-Obese (O-NM) Subjects
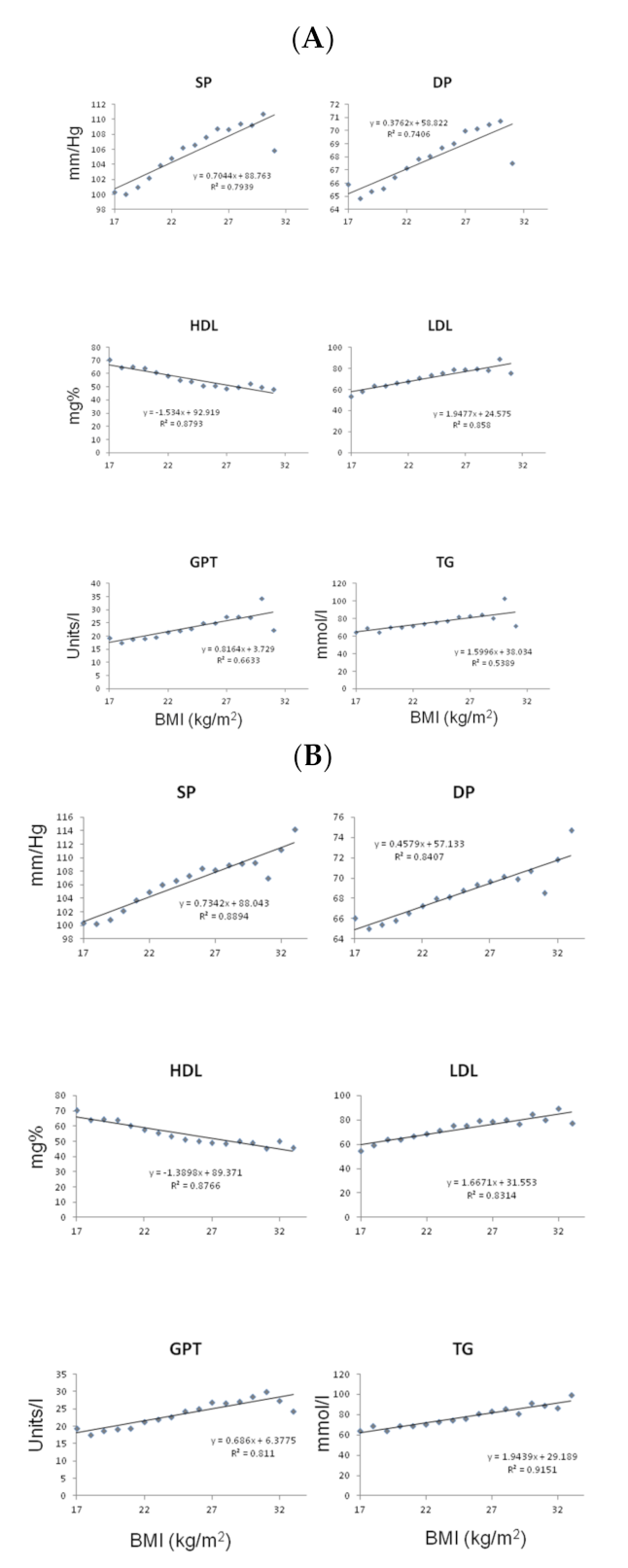
3.3. BMI Is Continuously Related to Metabolic Measures in Normometabolic Subjects
3.4. Young Women with and without Obesity Are Metabolically Protected Relative to Men
3.5. Metabolic Syndrome Components Are Prevalent in Normal BMI and Accumulate as a Function of Increasing BMI and Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidell, J.C. Obesity, insulin resistance and diabetes—A worldwide epidemic. Br. J. Nutr. 2000, 83 (Suppl. S1), S5–S8. [Google Scholar] [CrossRef] [Green Version]
- Limpijankit, T.; Vathesatogkit, P.; Matchariyakul, D.; Wiriyatanakorn, S.; Siriyotha, S.; Thakkinstian, A.; Sritara, P. Causal relationship of excess body weight on cardiovascular events through risk factors. Sci. Rep. 2022, 12, 5269. [Google Scholar] [CrossRef] [PubMed]
- McNeill, A.M.; Schmidt, M.I.; Rosamond, W.D.; East, H.E.; Girman, C.J.; Ballantyne, C.M.; Golden, S.H.; Heiss, G. The metabolic syndrome and 11-year risk of incident cardiovascular disease in the atherosclerosis risk in communities study. Diabetes Care 2005, 28, 385–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, P.W.F.; D’Agostino, R.B.; Parise, H.; Sullivan, L.; Meigs, J.B. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 2005, 112, 3066–3072. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.I.; Flegal, K.M.; Cowie, C.C.; Eberhardt, M.S.; Goldstein, D.E.; Little, R.R.; Wiedmeyer, H.M.; Byrd-Holt, D.D. Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults. The Third National Health and Nutrition Examination Survey, 1988–1994. Diabetes Care 1998, 21, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Mazloomzadeh, S.; Karami Zarandi, F.; Shoghli, A.; Dinmohammadi, H. Metabolic syndrome, its components and mortality: A population-based study. Med. J. Islam. Repub. Iran 2019, 33, 11. [Google Scholar] [CrossRef]
- Lonardo, A.; Mantovani, A.; Lugari, S.; Targher, G. Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity. Ann. Hepatol. 2020, 19, 359–366. [Google Scholar] [CrossRef]
- Aguilar-Salinas, C.A.; Garcia, E.G.; Robles, L.; Riano, D.; Ruiz-Gomez, D.G.; Garcia-Ulloa, A.C.; Melgarejo, M.A.; Zamora, M.; Guillen-Pineda, L.E.; Mehta, R.; et al. High adiponectin concentrations are associated with the metabolically healthy obese phenotype. J. Clin. Endocrinol. Metab. 2008, 93, 4075–4079. [Google Scholar] [CrossRef]
- Meigs, J.B.; Wilson, P.W.; Fox, C.S.; Vasan, R.S.; Nathan, D.M.; Sullivan, L.M.; D’Agostino, R.B. Body mass index, metabolic syndrome, and risk of type 2 diabetes or cardiovascular disease. J. Clin. Endocrinol. Metab. 2006, 91, 2906–2912. [Google Scholar] [CrossRef]
- Bluher, M. Metabolically Healthy Obesity. Endocr. Rev. 2020, 41, bnaa004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karelis, A.; Brochu, M.; Rabasa-Lhoret, R. Can we identify metabolically healthy but obese individuals (MHO)? Diabetes Metab. 2004, 30, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Lynch, L.A.; O’Connell, J.M.; Kwasnik, A.K.; Cawood, T.J.; O’Farrelly, C.; O’Shea, D.B. Are Natural Killer Cells Protecting the Metabolically Healthy Obese Patient? Obesity 2009, 17, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Wildman, R.P.; Muntner, P.; Reynolds, K.; McGinn, A.P.; Rajpathak, S.; Wylie-Rosett, J.; Sowers, M.R. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor—Prevalence and correlates of 2 phenotypes among the US population (NHANES 1999–2004). Arch. Intern. Med. 2008, 168, 1617–1624. [Google Scholar] [CrossRef] [Green Version]
- Korduner, J.; Bachus, E.; Jujic, A.; Magnusson, M.; Nilsson, P.M. Metabolically healthy obesity (MHO) in the Malmo diet cancer study—Epidemiology and prospective risks. Obes. Res. Clin. Pract. 2019, 13, 548–554. [Google Scholar] [CrossRef]
- Eckel, N.; Li, Y.; Kuxhaus, O.; Stefan, N.; Hu, F.B.; Schulze, M.B. Transition from metabolic healthy to unhealthy phenotypes and association with cardiovascular disease risk across BMI categories in 90 257 women (the Nurses’ Health Study): 30 year follow-up from a prospective cohort study. Lancet Diabetes Endocrinol. 2018, 6, 714–724. [Google Scholar] [CrossRef]
- Fisher, E.; Brzezinski, R.Y.; Ehrenwald, M.; Shapira, I.; Zeltser, D.; Berliner, S.; Marcus, Y.; Shefer, G.; Stern, N.; Rogowski, O.; et al. Increase of body mass index and waist circumference predicts development of metabolic syndrome criteria in apparently healthy individuals with 2 and 5 years follow-up. Int. J. Obes. 2019, 43, 800–807. [Google Scholar] [CrossRef]
- Kramer, C.K.; Zinman, B.; Retnakaran, R. Are metabolically healthy overweight and obesity benign conditions? A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 758–769. [Google Scholar] [CrossRef]
- Zheng, R.; Zhou, D.; Zhu, Y. The long-term prognosis of cardiovascular disease and all-cause mortality for metabolically healthy obesity: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 1024–1031. [Google Scholar] [CrossRef]
- Shenhar-Tsarfaty, S.; Yayon, N.; Waiskopf, N.; Shapira, I.; Toker, S.; Zaltser, D.; Berliner, S.; Ritov, Y.; Soreq, H. Fear and C-reactive protein cosynergize annual pulse increases in healthy adults. Proc. Natl. Acad. Sci. USA 2015, 112, E467–E471. [Google Scholar] [CrossRef] [Green Version]
- Physical Status: The Use and Interpretation of Anthropometry. Report of a WHO Expert Committee; WHO Technical Report Series 854; WHO: Geneva, Switzerland, 1995; pp. 1–452.
- Alberti, K.G.; Zimmet, P.; Shaw, J. IDF Epidemiology Task Force Consensus Group. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef] [PubMed]
- Nazare, J.A.; Smith, J.D.; Borel, A.L.; Haffner, S.M.; Balkau, B.; Ross, R.; Massien, C.; Almeras, N.; Despres, J.P. Ethnic influences on the relations between abdominal subcutaneous and visceral adiposity, liver fat, and cardiometabolic risk profile: The International Study of Prediction of Intra-Abdominal Adiposity and Its Relationship with Cardiometabolic Risk/Intra-Abdominal Adiposity. Am. J. Clin. Nutr. 2012, 96, 714–726. [Google Scholar] [PubMed] [Green Version]
- Lear, S.A.; Kohli, S.; Bondy, G.P.; Tchernof, A.; Sniderman, A.D. Ethnic Variation in Fat and Lean Body Mass and the Association with Insulin Resistance. J. Clin. Endocr. Metab. 2009, 94, 4696–4702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foy, C.G.; Hsu, F.C.; Haffner, S.M.; Norris, J.M.; Rotter, J.I.; Henkin, L.F.; Bryer-Ash, M.; Chen, Y.D.I.; Wagenknecht, L.E. Visceral fat and prevalence of hypertension among African Americans and Hispanic Americans: Findings from the IRAS family study. Am. J. Hypertens. 2008, 21, 910–916. [Google Scholar] [CrossRef]
- Zhou, Z.; Macpherson, J.; Gray, S.R.; Gill, J.M.R.; Welsh, P.; Celis-Morales, C.; Sattar, N.; Pell, J.P.; Ho, F.K. Are people with metabolically healthy obesity really healthy? A prospective cohort study of 381,363 UK Biobank participants. Diabetologia 2021, 64, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Mongraw-Chaffin, M.; Foster, M.C.; Anderson, C.A.M.; Burke, G.L.; Haq, N.; Kalyani, R.R.; Ouyang, P.; Sibley, C.T.; Tracy, R.; Woodward, M.; et al. Metabolically Healthy Obesity, Transition to Metabolic Syndrome, and Cardiovascular Risk. J. Am. Coll. Cardiol. 2018, 71, 1857–1865. [Google Scholar] [CrossRef]
- Bradshaw, P.T.; Monda, K.L.; Stevens, J. Metabolic Syndrome in Healthy Obese, Overweight, and Normal Weight Individuals: The Atherosclerosis Risk in Communities Study. Obesity 2013, 21, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, N.; Arora, S.; Kalra, S. Gender Disparities in People Living with Obesity—An Unchartered Territory. J. Midlife Health 2021, 12, 103–107. [Google Scholar]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Law, M.R.; Morris, J.K.; Wald, N.J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: Meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009, 338, b1665. [Google Scholar] [CrossRef] [Green Version]
- Keinan-Boker, L.; Noyman, N.; Chinich, A.; Green, M.S.; Nitzan-Kaluski, D. Overweight and obesity prevalence in Israel: Findings of the first national health and nutrition survey (MABAT). Isr. Med. Assoc. J. 2005, 7, 219–223. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normometabolic Obesity BMI ≥ 30 kg/m2 | Normometabolic Non-Obese Population BMI < 30 kg/m2 | |||||
|---|---|---|---|---|---|---|
| Female | Male | All | Female | Male | All | Average ± SD |
| 7 | 23 | 30 | 2123 | 3051 | 5174 | N IDF |
| 36 | 121 | 157 | 2632 | 3759 | 6391 | N ATP III |
| 39 ± 10 | 40 ± 10 | 40 ± 10 | 39 ± 10 * | 37 ± 10 | 38 ± 10 | Age (years) IDF |
| 43 ± 8 * | 40 ± 9 | 41 ± 9 | 40 ± 10 *,$ | 38 ± 10 $ | 39 ± 10 $ | Age (years) ATP III |
| 80 ± 7 * | 91 ± 6 | 89 ± 8 | 58 ± 7 * | 75 ± 8 | 68 ± 11 $ | Weight (kg) IDF |
| 77 ± 7 * | 92 ± 7 | 89 ± 9 | 60 ± 7 * | 76 ± 8 | 70 ± 11 | Weight (kg) ATP III |
| 31 ± 2 | 31 ± 2 | 31 ± 2 | 22 ± 2 *,$ | 24 ± 2 $ | 23 ± 2 $ | BMI (kg/m2) IDF |
| 31 ± 1 | 31 ± 1 | 31 ± 1 | 23 ± 2 *$ | 25 ± 2 $ | 24 ± 2 $ | BMI (kg/m2) ATP III |
| 74 ± 2 * | 91 ± 4 | 89 ± 8 | 72 ± 5 * | 86 ± 6 $ | 80 ± 9 | Waist Circumference (cm) IDF |
| 83 ± 4 * | 98 ± 3 | 94 ± 7 | 75 ± 6 *,$ | 88 ± 7 $ | 93 ± 9 | Waist Circumference (cm) ATP III |
| 115 ± 15 | 120 ± 6 | 119 ± 9 | 108 ± 10 * | 115 ± 9 | 113 ± 10 $ | SBP IDF |
| 113 ± 10 | 118 ± 9 | 116 ± 9 | 108 ± 10 * | 116 ± 9 $ | 113 ± 10 $ | SBP ATP III |
| 73 ± 9 | 77 ± 5 | 76 ± 6 | 70 ± 6 * | 73 ± 6 | 72 ± 6 | DBP IDF |
| 73 ± 6 | 76 ± 6 | 75 ± 6 | 70 ± 6 * | 74 ± 6 $ | 72 ± 6 $ | DBP ATP III |
| 4.9 ± 0.5 * | 4.5 ± 0.5 | 4.6 ± 0.6 | 4.5 ± 0.5 * | 4.7 ± 0.5 $ | 4.9 ± 0.5 | Glucose (mmol/L) IDF |
| 4.8 ± 0.4 | 4.9 ± 0.4 | 4.9 ± 0.4 | 4.6 ± 0 *,$ | 4.8 ± 0.3 | 4.7 ± 0 $ | Glucose (mmol/L) ATP III |
| 0.8 ± 0.3 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.8 ± 0.3 * | 0.9 ± 0.3 $ | 0.9 ± 0.3 $ | Triglycerides (mmol/L) IDF |
| 0.9 ± 0.3 * | 1.1 ± 0.3 | 1.0 ± 0.3 | 0.8 ± 0 *,$ | 0.9 ± 0 $ | 0.9 ± 0 | Triglycerides (mmol/L) ATP III |
| 2 ± 0.7 | 2.4 ± 0.6 | 2.3 ± 0.6 | 1.8 ± 0.4 * | 1.4 ± 0.5 | 1.6 ± 0.5 | HDL (mmol/L IDF |
| 1.6 ± 0.3 * | 1.3 ± 0.2 | 1.4 ± 0.3 | 1.8 ± 0.3 * | 1.4 ± 0.1 | 1.6 ± 0.1 | HDL (mmol/L) ATP III |
| 1.7 ± 0.5 | 2.3 ± 0.6 | 2.2 ± 0.6 | 1.8 ± 0.7 * | 2 ± 0.7 $ | 1.9 ± 0.7 | LDL (mmol/L) IDF |
| 2.9 ± 0.6 * | 3.3 ± 0.7 | 3.2 ± 0.1 | 2.8 ± 0 * | 2.9 ± 0.1 $ | 2.9 ± 0.1 $ | LDL (mmol/L) ATP III |
| 43 ± 40 | 36 ± 41 | 38 ± 40 | 28 ± 24 * | 34 ± 27 | 32 ± 26 | GOT IDF |
| 20 ± 3 * | 27 ± 19 | 25 ± 17 | 21 ± 7 *,$ | 24 ± 9 $ | 23 ± 9 $ | GOT ATP III |
| 44 ± 40 | 35 ± 29 | 37 ± 32 | 26 ± 25 * | 35 ± 27 | 31 ± 26 | GPT IDF |
| 18 ± 5 * | 30 ± 18 | 28 ± 17 | 18 ± 8 *$ | 25 ± 12 $ | 22 ± 11 $ | GPT ATP III |
| 6.0 ± 5 | 3 ± 3 | 4 ± 4 | 2 ± 3 * | 2.0 ± 3 | 2 ± 3 $ | hsCRP IDF |
| 6 ± 6 * | 3 ± 4 | 4 ± 4 | 2 ± 3 * | 2 ± 3 | 2 ± 3 $ | hsCRP ATP III |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcus, Y.; Segev, E.; Shefer, G.; Eilam, D.; Shenkerman, G.; Buch, A.; Shenhar-Tsarfaty, S.; Zeltser, D.; Shapira, I.; Berliner, S.; et al. Metabolically Healthy Obesity Is a Misnomer: Components of the Metabolic Syndrome Linearly Increase with BMI as a Function of Age and Gender. Biology 2023, 12, 719. https://doi.org/10.3390/biology12050719
Marcus Y, Segev E, Shefer G, Eilam D, Shenkerman G, Buch A, Shenhar-Tsarfaty S, Zeltser D, Shapira I, Berliner S, et al. Metabolically Healthy Obesity Is a Misnomer: Components of the Metabolic Syndrome Linearly Increase with BMI as a Function of Age and Gender. Biology. 2023; 12(5):719. https://doi.org/10.3390/biology12050719
Chicago/Turabian StyleMarcus, Yonit, Elad Segev, Gabi Shefer, David Eilam, Galina Shenkerman, Assaf Buch, Shani Shenhar-Tsarfaty, David Zeltser, Itzhak Shapira, Shlomo Berliner, and et al. 2023. "Metabolically Healthy Obesity Is a Misnomer: Components of the Metabolic Syndrome Linearly Increase with BMI as a Function of Age and Gender" Biology 12, no. 5: 719. https://doi.org/10.3390/biology12050719
APA StyleMarcus, Y., Segev, E., Shefer, G., Eilam, D., Shenkerman, G., Buch, A., Shenhar-Tsarfaty, S., Zeltser, D., Shapira, I., Berliner, S., & Rogowski, O. (2023). Metabolically Healthy Obesity Is a Misnomer: Components of the Metabolic Syndrome Linearly Increase with BMI as a Function of Age and Gender. Biology, 12(5), 719. https://doi.org/10.3390/biology12050719