


Glucose-Lowering Effects of Imeglimin and Its Possible Beneficial Effects on Diabetic Complications

Abstract
:Simple Summary
Abstract
1. Introduction
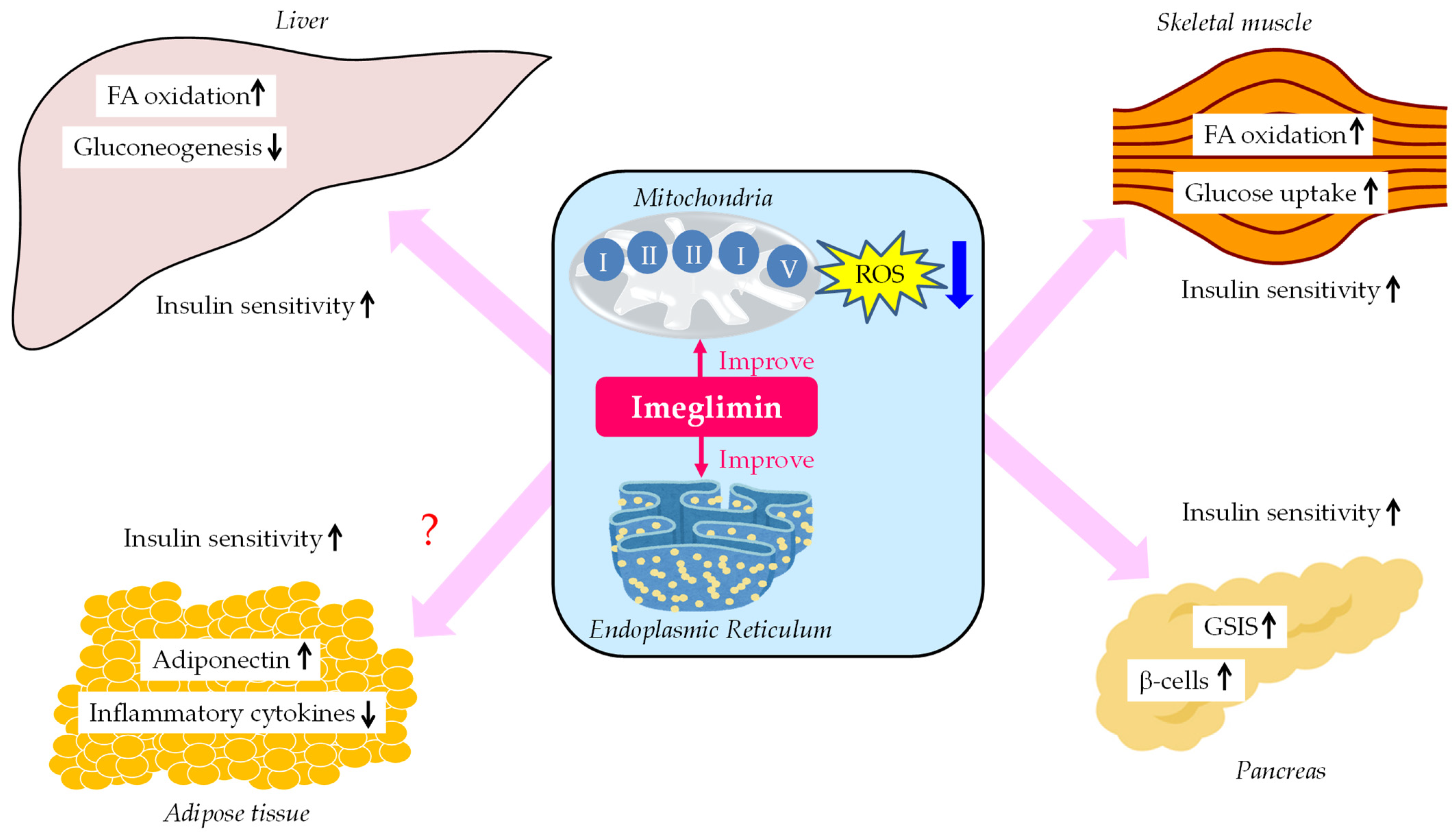
2. Glucose-Lowering Mechanisms of Imeglimin
2.1. An Improvement in Mitochondrial Function
2.2. An Improvement in Function of Endoplasmic Reticulum (ER)
2.3. An Inhibition of Hepatic Glucose Production
2.4. An Improvement in GSIS
2.5. An Improvement in β-Cell Function
2.6. An Enhancement of Glucose Uptake by the Skeletal Muscles
2.7. An Improvement in Oxidative Stress and Insulin Resistance
3. Glucose-Lowering Effects of Imeglimin in Clinical Trials
3.1. Effects of Imeglimin on HbA1c in Clinical Trials
3.2. Effects of Imeglimin on Fating Plasma Glucose (FPG), the Markers for Insulin Secretion and Insulin Resistance and Serum Lipids in Clinical Trials
3.3. Stimulatory Effect of Imeglimin on Incretin Secretion
4. A Safety Profile of Imeglimin
4.1. A Safety Profile Obtained from Clinical Trials Which Studied Imeglimin Monotherapy and Combination Therapy
4.2. Reported Treatment Emergent Adverse Events (TEAEs)
4.3. Electrophysiological Effects of Imeglimin on Cardiac Repolarization
4.4. The Drug–Drug Interaction between Imeglimin and an Inhibitor of Human Multidrug and Toxic Extrusion Transporters (MATE) and Organic Cation Transporters (OCT)
4.5. The Effect of Hepatic Impairment on the Pharmacokinetics (PK) of Imeglimin
4.6. The Effect of Renal Impairment on the PK of Imeglimin
4.7. Reduced Lactic Acidosis Risk with Imeglimin as Compared with Metformin
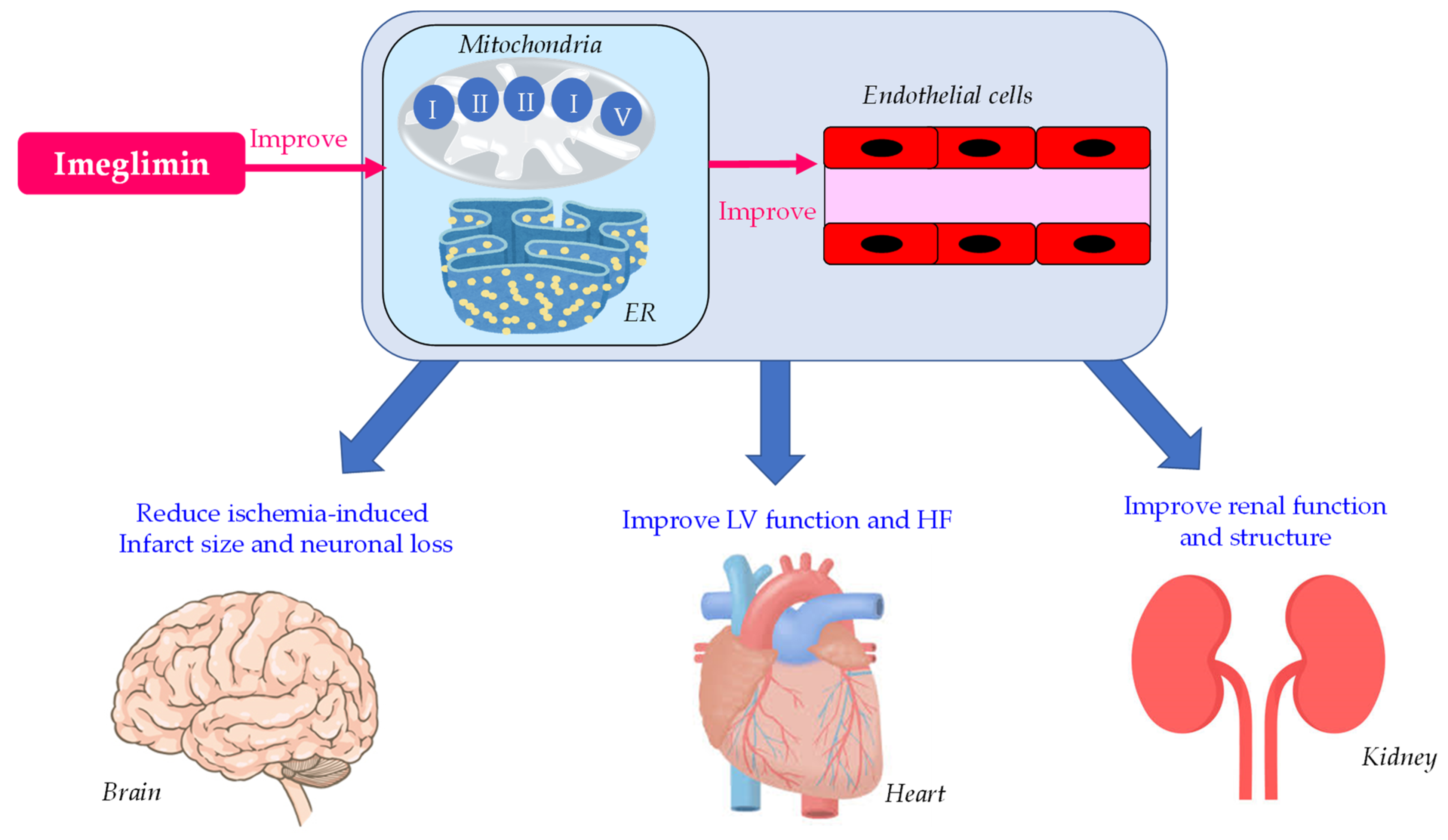
5. Effects of Imeglimin on Endothelial Dysfunction, Heart, Kidney and Brain
5.1. Effects of Imeglimin on Endothelial Dysfunction
5.2. Effects of Imeglimin on Left Ventricular (LV) Function
5.3. Effects of Imeglimin on Kidney Function and Structure
5.4. Effects of Imeglimin on Ischemia-Induced Brain Damage
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weksler-Zangen, S. Is Type 2 Diabetes a Primary Mitochondrial Disorder? Cells 2022, 11, 1617. [Google Scholar] [CrossRef]
- Aharon-Hananel, G.; Romero-Afrima, L.; Saada, A.; Mantzur, C.; Raz, I.; Weksler-Zangen, S. Cytochrome c Oxidase Activity as a Metabolic Regulator in Pancreatic Beta-Cells. Cells 2022, 11, 929. [Google Scholar] [CrossRef]
- Sha, W.; Hu, F.; Bu, S. Mitochondrial dysfunction and pancreatic islet beta-cell failure. Exp. Ther. Med. 2020, 20, 266. [Google Scholar] [CrossRef]
- Prasun, P. Role of mitochondria in pathogenesis of type 2 diabetes mellitus. J. Diabetes. Metab. Disord. 2020, 19, 2017–2022. [Google Scholar] [CrossRef]
- Esser, N.; Utzschneider, K.M.; Kahn, S.E. Early beta cell dysfunction vs insulin hypersecretion as the primary event in the pathogenesis of dysglycaemia. Diabetologia 2020, 63, 2007–2021. [Google Scholar] [CrossRef]
- Pinti, M.V.; Fink, G.K.; Hathaway, Q.; Durr, A.J.; Kunovac, A.; Hollander, J.M. Mitochondrial dysfunction in type 2 diabetes mellitus: An organ-based analysis. Am. J. Physiol. Metab. 2019, 316, E268–E285. [Google Scholar] [CrossRef]
- Fex, M.; Nicholas, L.M.; Vishnu, N.; Medina, A.; Sharoyko, V.V.; Nicholls, D.G.; Spegel, P.; Mulder, H. The pathogenetic role of beta-cell mitochondria in type 2 diabetes. J. Endocrinol. 2018, 236, R145–R159. [Google Scholar] [CrossRef]
- Mulder, H. Transcribing beta-cell mitochondria in health and disease. Mol. Metab. 2017, 6, 1040–1051. [Google Scholar] [CrossRef]
- Wiederkehr, A.; Wollheim, C.B. Mitochondrial signals drive insulin secretion in the pancreatic beta-cell. Mol. Cell. Endocrinol. 2012, 353, 123–137. [Google Scholar] [CrossRef]
- Nicholls, D.G. The Pancreatic beta-Cell: A Bioenergetic Perspective. Physiol. Rev. 2016, 96, 1385–1447. [Google Scholar] [CrossRef]
- Prentki, M.; Nolan, C.J. Islet beta cell failure in type 2 diabetes. J. Clin. Investig. 2006, 116, 1802–1812. [Google Scholar] [CrossRef]
- Dabravolski, S.; Orekhova, V.; Baig, M.; Bezsonov, E.; Starodubova, A.; Popkova, T.; Orekhov, A. The Role of Mitochondrial Mutations and Chronic Inflammation in Diabetes. Int. J. Mol. Sci. 2021, 22, 6733. [Google Scholar] [CrossRef] [PubMed]
- Henquin, J.C. Regulation of insulin secretion: A matter of phase control and amplitude modulation. Diabetologia 2009, 52, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Leenders, F.; Groen, N.; de Graaf, N.; Engelse, M.A.; Rabelink, T.J.; de Koning, E.J.P.; Carlotti, F. Oxidative Stress Leads to beta-Cell Dysfunction Through Loss of beta-Cell Identity. Front. Immunol. 2021, 12, 690379. [Google Scholar] [CrossRef] [PubMed]
- Gurgul-Convey, E.; Mehmeti, I.; Lortz, S.; Lenzen, S. Cytokine toxicity in insulin-producing cells is mediated by nitro-oxidative stress-induced hydroxyl radical formation in mitochondria. Klin. Wochenschr. 2011, 89, 785–798. [Google Scholar] [CrossRef] [PubMed]
- Lenzen, S. Oxidative stress: The vulnerable beta-cell. Biochem. Soc. Trans. 2008, 36, 343–347. [Google Scholar] [CrossRef]
- Ciccarelli, G.; Conte, S.; Cimmino, G.; Maiorano, P.; Morrione, A.; Giordano, A. Mitochondrial Dysfunction: The Hidden Player in the Pathogenesis of Atherosclerosis? Int. J. Mol. Sci. 2023, 24, 1086. [Google Scholar] [CrossRef]
- Cleveland, K.H.; Schnellmann, R.G. Pharmacological Targeting of Mitochondria in Diabetic Kidney Disease. Pharmacol. Rev. 2023, 75, 250–262. [Google Scholar] [CrossRef]
- Li, K.; Wan, B.; Li, S.; Chen, Z.; Jia, H.; Song, Y.; Zhang, J.; Ju, W.; Ma, H.; Wang, Y.F. Mitochondrial dysfunction in cardiovascular disease: Towards exercise regulation of mitochondrial function. Front. Physiol. 2023, 14, 1063556. [Google Scholar] [CrossRef]
- Ketenci, M.; Zablocki, D.; Sadoshima, J. Mitochondrial Quality Control Mechanisms during Diabetic Cardiomyopathy. JMA J. 2022, 5, 407–415. [Google Scholar]
- Novgorodov, S.A.; Gudz, T.I. Ceramide and mitochondria in ischemic brain injury. Int. J. Biochem. Mol. Biol. 2011, 2, 347–361. [Google Scholar]
- Vial, G.; Chauvin, M.A.; Bendridi, N.; Durand, A.; Meugnier, E.; Madec, A.M.; Bernoud-Hubac, N.; de Barros, J.-P.P.; Fontaine, É.; Acquaviva, C.; et al. Imeglimin normalizes glucose tolerance and insulin sensitivity and improves mitochondrial function in liver of a high-fat, high-sucrose diet mice model. Diabetes 2015, 64, 2254–2264. [Google Scholar] [CrossRef] [PubMed]
- Fauzi, M.; Murakami, T.; Yabe, D.; Inagaki, N. Current understanding of imeglimin action on pancreatic β-cells: Involvement of mitochondria and endoplasmic reticulum homeostasis. J. Diabetes Investig. 2023, 14, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Vuylsteke, V.; Chastain, L.M.; Maggu, G.A.; Brown, C. Imeglimin: A Potential New Multi-Target Drug for Type 2 Diabetes. Drugs R D 2015, 15, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Anello, M.; Lupi, R.; Spampinato, D.; Piro, S.; Masini, M.; Boggi, U.; Del Prato, S.; Rabuazzo, A.M.; Purrello, F.; Marchetti, P. Functional and morphological alterations of mitochondria in pancreatic beta cells from type 2 diabetic patients. Diabetologia 2005, 48, 282–289. [Google Scholar] [CrossRef]
- Ma, Z.A.; Zhao, Z.; Turk, J. Mitochondrial dysfunction and beta-cell failure in type 2 diabetes mellitus. Exp. Diabetes Res. 2012, 2012, 703538. [Google Scholar] [CrossRef]
- Haythorne, E.; Rohm, M.; van de Bunt, M.; Brereton, M.F.; Tarasov, A.I.; Blacker, T.S.; Sachse, G.; Dos Santos, M.S.; Exposito, R.T.; Davis, S.; et al. Diabetes causes marked inhibition of mitochondrial metabolism in pancreatic β-cells. Nat. Commun. 2019, 10, 2474. [Google Scholar] [CrossRef]
- Lowell, B.B.; Shulman, G.I. Mitochondrial dysfunction and type 2 diabetes. Science 2005, 307, 384–387. [Google Scholar] [CrossRef]
- Kim, J.A.; Wei, Y.; Sowers, J.R. Role of mitochondrial dysfunction in insulin resistance. Circ. Res. 2008, 102, 401–414. [Google Scholar] [CrossRef]
- Gonzalez-Franquesa, A.; Patti, M.E. Insulin resistance and mitochondrial dysfunction. Adv. Exp. Med. Biol. 2017, 982, 465–520. [Google Scholar]
- Petersen, M.C.; Shulman, G.I. Mechanisms of insulin action and insulin resistance. Physiol. Rev. 2018, 98, 2133–2223. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, S.; Urano, F. The Role of ER Stress in Diabetes: Exploring Pathological Mechanisms Using Wolfram Syndrome. Int. J. Mol. Sci. 2022, 24, 230. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Inoue, R.; Togashi, Y.; Okuyama, T.; Satoh, A.; Kyohara, M.; Nishiyama, K.; Tsuno, T.; Miyashita, D.; Kin, T.; et al. Imeglimin Ameliorates β-Cell Apoptosis by Modulating the Endoplasmic Reticulum Homeostasis Pathway. Diabetes 2022, 71, 424–439. [Google Scholar] [CrossRef] [PubMed]
- Vial, G.; Lamarche, F.; Cottet-Rousselle, C.; Hallakou-Bozec, S.; Borel, A.L.; Fontaine, E. The mechanism by which imeglimin inhibits gluconeogenesis in rat liver cells. Endocrinol. Diabetes Metab. 2021, 4, e00211. [Google Scholar] [CrossRef]
- Fouqueray, P.; Leverve, X.; Fontaine, E.; Baquié, M.; Wollheim, C. Imeglimin—A new oral anti-diabetic that targets the three key defects of type 2 diabetes. J. Diabetes Metab. 2011, 2, 126. [Google Scholar] [CrossRef]
- Hallakou-Bozec, S.; Vial, G.; Kergoat, M.; Fouqueray, P.; Bolze, S.; Borel, A.L.; Fontaine, E.; Moller, D.E. Mechanism of action of Imeglimin: A novel therapeutic agent for type 2 diabetes. Diabetes Obes. Metab. 2021, 23, 664–673. [Google Scholar] [CrossRef]
- Garten, A.; Schuster, S.; Penke, M.; Gorski, T.; de Giorgis, T.; Kiess, W. Physiological and pathophysiological roles of NAMPT and NAD metabolism. Nat. Rev. Endocrinol. 2015, 11, 535–546. [Google Scholar] [CrossRef]
- Hallakou-Bozec, S.; Kergoat, M.; Fouqueray, P.; Bolze, S.; Moller, D.E. Imeglimin amplifies glucose-stimulated insulin release from diabetic islets via a distinct mechanism of action. PLoS ONE 2021, 16, e0241651. [Google Scholar] [CrossRef]
- Lablanche, S.; Tubbs, E.; Cottet-Rousselle, C.; Lamarche, F.; Moisan, A.; Persoons, V.; Pierre, Y.; Benhamou, P.Y.; Hallakou-Bozec, S.; Fontaine, E.; et al. Imeglimin protects INS-1 cells and human islets against high glucose–and high fructose–induced cell death by inhibiting the mitochondrial PTP opening. Diabetes 2018, 67 (Suppl. 1), 81. [Google Scholar] [CrossRef]
- Sanada, J.; Obata, A.; Fushimi, Y.; Kimura, T.; Shimoda, M.; Ikeda, T.; Nogami, Y.; Obata, Y.; Yamasaki, Y.; Nakanishi, S.; et al. Imeglimin exerts favorable effects on pancreatic β-cells by improving morphology in mitochondria and increasing the number of insulin granules. Sci. Rep. 2022, 12, 13220. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Farrokhi, F.R.; Butler, A.E.; Sahebkar, A. Insulin resistance: Review of the underlying molecular mechanisms. J. Cell. Physiol. 2019, 234, 8152–8161. [Google Scholar] [CrossRef] [PubMed]
- Rains, J.L.; Jain, S.K. Oxidative stress, insulin signaling, and diabetes. Free Radic. Biol. Med. 2011, 50, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Pacini, G.; Mari, A.; Fouqueray, P.; Bolze, S.; Roden, M. Imeglimin increases glucose-dependent insulin secretion and improves β-cell function in patients with type 2 diabetes. Diabetes Obes. Metab. 2015, 17, 541–545. [Google Scholar] [CrossRef]
- Pirags, V.; Lebovitz, H.; Fouqueray, P. Imeglimin, a novel glimin oral antidiabetic, exhibits a good efficacy and safety profile in type 2 diabetic patients. Diabetes Obes. Metab. 2012, 14, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Dubourg, J.; Ueki, K.; Grouin, J.M.; Fouqueray, P. Efficacy and safety of imeglimin in Japanese patients with type 2 diabetes: A 24-week, randomized, double-blind, placebo-controlled, dose-ranging phase 2b trial. Diabetes Obes. Metab. 2021, 23, 800–810. [Google Scholar] [CrossRef]
- Dubourg, J.; Fouqueray, P.; Thang, C.; Grouin, J.M.; Ueki, K. Efficacy and Safety of Imeglimin Monotherapy Versus Placebo in Japanese Patients With Type 2 Diabetes (TIMES 1): A Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Multicenter Phase 3 Trial. Diabetes Care 2021, 44, 952–959. [Google Scholar] [CrossRef]
- Dubourg, J.; Fouqueray, P.; Quinslot, D.; Grouin, J.M.; Kaku, K. Long-term safety and efficacy of imeglimin as monotherapy or in combination with existing antidiabetic agents in Japanese patients with type 2 diabetes (TIMES 2): A 52-week, open-label, multicentre phase 3 trial. Diabetes Obes. Metab. 2022, 24, 609–619. [Google Scholar] [CrossRef]
- Fouqueray, P.; Pirags, V.; Inzucchi, S.E.; Bailey, C.J.; Schernthaner, G.; Diamant, M.; Lebovitz, H.E. The efficacy and safety of imeglimin as add-on therapy in patients with type 2 diabetes inadequately controlled with metformin monotherapy. Diabetes Care 2013, 36, 565–568. [Google Scholar] [CrossRef]
- Fouqueray, P.; Pirags, V.; Diamant, M.; Schernthaner, G.; Lebovitz, H.E.; Inzucchi, S.E.; Bailey, C.J. The efficacy and safety of imeglimin as add-on therapy in patients with type 2 diabetes inadequately controlled with sitagliptin monotherapy. Diabetes Care 2014, 37, 1924–1930. [Google Scholar] [CrossRef]
- Reilhac, C.; Dubourg, J.; Thang, C.; Grouin, J.M.; Fouqueray, P.; Watada, H. Efficacy and safety of imeglimin add-on to insulin monotherapy in Japanese patients with type 2 diabetes (TIMES 3): A randomized, double-blind, placebo-controlled phase 3 trial with a 36-week open-label extension period. Diabetes Obes. Metab. 2022, 24, 838–848. [Google Scholar] [CrossRef]
- Shabrawy, A.M.E.; Elbana, K.A.; Abdelsalam, N.M. Proinsulin/insulin ratio as a predictor of insulin resistance and B-cell dysfunction in obese Egyptians. Diabetes Metab. Syndr. 2019, 13, 2094–2096. [Google Scholar] [CrossRef]
- Schölin, A.; Nyström, L.; Arnqvist, H.; Bolinder, J.; Björk, E.; Berne, C.; Karlsson, F.A.; Diabetes Incidence Study Group in Sweden (DISS). Proinsulin/C-peptide ratio, glucagon and remission in new-onset Type 1 diabetes mellitus in young adults. Diabet. Med. 2011, 28, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Evans-Molina, C.; Hatanaka, M.; Mirmira, R.G. Lost in translation: Endoplasmic reticulum stress and the decline of β-cell health in diabetes mellitus. Diabetes Obes. Metab. 2013, 15 (Suppl. 3), 159–169. [Google Scholar] [CrossRef] [PubMed]
- Sims, E.K.; Chaudhry, Z.; Watkins, R.; Syed, F.; Blum, J.; Ouyang, F.; Perkins, S.M.; Mirmira, R.G.; Sosenko, J.; Di Meglio, L.A.; et al. Elevations in the fasting serum proinsulin-to-C-peptide ratio precede the onset of type 1 diabetes. Diabetes Care 2016, 39, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Loopstra-Masters, R.C.; Haffner, S.M.; Lorenzo, C.; Wagenknecht, L.E.; Hanley, A.J. Proinsulin-to-C-peptide ratio versus proinsulin-to-insulin ratio in the prediction of incident diabetes: The Insulin Resistance Atherosclerosis Study (IRAS). Diabetologia 2011, 54, 3047–3054. [Google Scholar] [CrossRef]
- Song, Y.; Manson, J.E.; Tinker, L.; Howard, B.V.; Kuller, L.H.; Nathan, L.; Rifai, N.; Liu, S. Insulin Sensitivity and Insulin Secretion Determined by Homeostasis Model Assessment and Risk of Diabetes in a Multiethnic Cohort of Women: The Women’s Health Initiative Observational Study. Diabetes Care 2007, 30, 1747–1752. [Google Scholar] [CrossRef]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and Abuse of HOMA Modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef]
- Yingyue, Q.; Sugawara, K.; Takahashi, H.; Yokoi, N.; Ohbayashi, K.; Iwasaki, Y.; Seino, S.; Ogawa, W. Stimulatory effect of imeglimin on incretin secretion. J. Diabetes Investig. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Fouqueray, P.; Perrimond-Dauchy, S.; Bolze, S. Imeglimin Does Not Induce Clinically Relevant Pharmacokinetic Interactions When Combined with Either Metformin or Sitagliptin in Healthy Subjects. Clin. Pharmacokinet. 2020, 59, 1261–1271. [Google Scholar] [CrossRef]
- Dubourg, J.; Perrimond-Dauchy, S.; Felices, M.; Bolze, S.; Voiriot, P.; Fouqueray, P. Absence of QTc prolongation in a thorough QT study with imeglimin, a first in class oral agent for type 2 diabetes mellitus. Eur. J. Clin. Pharmacol. 2020, 76, 1393–1400. [Google Scholar] [CrossRef]
- Chevalier, C.; Perrimond-Dauchy, S.; Dubourg, J.; Fouqueray, P.; Bolze, S. Lack of Drug-Drug Interaction Between Cimetidine, a Renal Transporter Inhibitor, and Imeglimin, a Novel Oral Antidiabetic Drug, in Healthy Volunteers. Eur. J. Drug. Metab. Pharmacokinet. 2020, 45, 725–733. [Google Scholar] [CrossRef]
- Chevalier, C.; Dubourg, J.; Bolze, S.; Fouqueray, P. Pharmacokinetics of Imeglimin in Subjects with Moderate Hepatic Impairment. Clin. Pharmacokinet. 2021, 60, 485–490. [Google Scholar] [CrossRef]
- Kitamura, A.; Yumizaki, T.; Kondo, T.; Sekino, H.; Kakuyama, H. Pharmacokinetics and Safety of Imeglimin in Japanese Patients with Impaired Renal Function. J. Clin. Pharmacol. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Tomita, Y.; Hansson, E.; Mazuir, F.; Wellhagen, G.J.; Ooi, Q.X.; Mezzalana, E.; Kitamura, A.; Nemoto, D.; Bolze, S. Imeglimin population pharmacokinetics and dose adjustment predictions for renal impairment in Japanese and Western patients with type 2 diabetes. Clin. Transl. Sci. 2022, 15, 1014–1026. [Google Scholar] [CrossRef] [PubMed]
- Theurey, P.; Vial, G.; Fontaine, E.; Monternier, P.A.; Fouqueray, P.; Bolze, S.; Moller, D.E.; Hallakou-Bozec, S. Reduced lactic acidosis risk with Imeglimin: Comparison with Metformin. Physiol. Rep. 2022, 10, e15151. [Google Scholar] [CrossRef] [PubMed]
- Madiraju, A.K.; Erion, D.M.; Rahimi, Y.; Zhang, X.M.; Braddock, D.T.; Albright, R.A.; Prigaro, B.J. Metformin suppresses gluconeogenesis by inhibiting mitochondrial glycerophosphate dehydrogenase. Nature 2014, 510, 542–546. [Google Scholar] [CrossRef]
- Petersen, M.C.; Vatner, D.F.; Shulman, G.I. Regulation of hepatic glucose metabolism in health and disease. Nat. Rev. Endocrinol. 2017, 13, 572–587. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Ueno, H.; Konagata, A.; Taniguchi, N.; Kogo, F.; Nagatomo, Y.; Shimizu, K.; Yamaguchi, H.; Shimoda, K. Improving the Effects of Imeglimin on Endothelial Function: A Prospective, Single-Center, Observational Study. Diabetes Ther. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Detaille, D.; Vial, G.; Borel, A.L.; Cottet-Rouselle, C.; Hallakou-Bozec, S.; Bolze, S.; Fouqueray, P.; Fontaine, E. Imeglimin prevents human endothelial cell death by inhibiting mitochondrial permeability transition without inhibiting mitochondrial respiration. Cell Death Discov. 2016, 2, 15072. [Google Scholar] [CrossRef]
- Lachaux, M.; Soulié, M.; Hamzaoui, M.; Bailly, A.; Nicol, L.; Rémy-Jouet, I.; Renet, S.; Vendeville, C.; Gluais-Dagorn, P.; Hallakou-Bozec, S.; et al. Short-and long-term administration of imeglimin counters cardiorenal dysfunction in a rat model of metabolic syndrome. Endocrinol. Diabetes Metab. 2020, 3, e00128. [Google Scholar] [CrossRef]
- MacDonald, M.R.; Petrie, M.C.; Varyani, F.; Ostergren, J.; Michelson, E.L.; Young, J.B.; Solomon, S.D.; Granger, C.B.; Swedberg, K.; Yusuf, S.; et al. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: An analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur. Heart J. 2008, 29, 1377–1385. [Google Scholar] [CrossRef]
- Kristensen, S.L.; Mogensen, U.M.; Jhund, P.S.; Petrie, M.C.; Preiss, D.; Win, S.; Køber, L.; Granger, C.B.; Swedberg, K.; Yusuf, S.; et al. Clinical and echocardiographic characteristics and cardiovascular outcomes according to diabetes status in patients with heart failure and preserved ejection fraction: A report from the I-preserve trial (irbesartan in heart failure with preserved ejection fraction). Circulation 2017, 135, 724–735. [Google Scholar]
- Schiattarella, G.G.; Altamirano, F.; Tong, D.; French, K.M.; Villalobos, E.; Kim, S.Y.; Luo, X.; Jiang, N.; May, H.I.; Wang, Z.V.; et al. Nitrosative stress drives heart failure with preserved ejection fraction. Nature 2019, 568, 351–356. [Google Scholar] [CrossRef]
- Schiattarella, G.G.; Altamirano, F.; Kim, S.Y.; Tong, D.; Ferdous, A.; Piristine, H.; Dasgupta, S.; Wang, X.; French, K.M.; Villalobos, E.; et al. Xbp1s-FoxO1 axis governs lipid accumulation and contractile performance in heart failure with preserved ejection fraction. Nat. Commun. 2021, 12, 1684. [Google Scholar] [CrossRef] [PubMed]
- Kitakata, H.; Endo, J.; Hashimoto, S.; Mizuno, E.; Moriyama, H.; Shirakawa, K.; Goto, S.; Katsumata, Y.; Fukuda, K.; Sano, M.; et al. Imeglimin prevents heart failure with preserved ejection fraction by recovering the impaired unfolded protein response in mice subjected to cardiometabolic stress. Biochem. Biophys. Res. Commun. 2021, 572, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Barabutis, N. Unfolded Protein Response: A Regulator of the Endothelial Barrier. Endocr. Metab. Sci. 2021, 3, 100092. [Google Scholar] [CrossRef] [PubMed]
- Zhen, J.; Lu, H.; Wang, X.Q.; Vaziri, N.D.; Zhou, X.J. Upregulation of endothelial and inducible nitric oxide synthase expression by reactive oxygen species. Am. J. Hypertens. 2008, 21, 28–34. [Google Scholar] [CrossRef]
- Zemgulyte, G.; Umbrasas, D.; Cizas, P.; Jankeviciute, S.; Pampuscenko, K.; Grigaleviciute, R.; Rastenyte, D.; Borutaite, V. Imeglimin Is Neuroprotective Against Ischemic Brain Injury in Rats-a Study Evaluating Neuroinflammation and Mitochondrial Functions. Mol. Neurobiol. 2022, 59, 2977–2991. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Monotherapy | |||
|---|---|---|---|
| Daily Dose (mg) | Duration (Weeks) | Change in HbA1c (%) | References |
| 1000 | 8 | +0.38 | [44] |
| 3000 | 8 | −0.18 | [44] |
| 1000 | 24 | −0.09 | [45] |
| 2000 | 24 | −0.51 | [45] |
| 2000 | 24 | −0.72 | [46] |
| 3000 | 24 | −0.57 | [45] |
| 2000 | 52 | −0.46 | [47] |
| Combination therapy | |||
| 3000 + BG | 12 | −0.65 | [48] |
| 2000 + BG | 52 | −0.67 | [47] |
| 3000 + DPP4i | 12 | −0.6 | [49] |
| 2000 + DPP4i | 52 | −0.92 | [47] |
| 2000 + insulin | 16 | −0.63 | [50] |
| Monotherapy | Combination Therapy | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Daily Dose (mg) | 1000 | 3000 | 1000 | 2000 | 2000 | 3000 | 3000 | 3000 | 2000 |
| Duration (weeks) | 8 | 8 | 24 | 24 | 24 | 24 | 12 | 12 | 16 |
| Metformin | Sitagliptin | Insulin | |||||||
| References | [44] | [44] | [45] | [46] | [45] | [45] | [48] | [49] | [50] |
| FPG | ↑ | ↓ | → | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ |
| Proinsulin/insulin | ↓ | ↓ | → | ||||||
| Proinsulin/C-peptide | → | ↓ | → | ↓ | |||||
| HOMA-B | ↑ | ↑ | ↑ | ↑ | |||||
| HOMA-IR | → | → | → | → | → | ||||
| LDL-C | → | → | → | → | |||||
| HDL-C | → | → | → | → | |||||
| Triglyceride | → | → | → | → | → | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yanai, H.; Adachi, H.; Hakoshima, M.; Katsuyama, H. Glucose-Lowering Effects of Imeglimin and Its Possible Beneficial Effects on Diabetic Complications. Biology 2023, 12, 726. https://doi.org/10.3390/biology12050726
Yanai H, Adachi H, Hakoshima M, Katsuyama H. Glucose-Lowering Effects of Imeglimin and Its Possible Beneficial Effects on Diabetic Complications. Biology. 2023; 12(5):726. https://doi.org/10.3390/biology12050726
Chicago/Turabian StyleYanai, Hidekatsu, Hiroki Adachi, Mariko Hakoshima, and Hisayuki Katsuyama. 2023. "Glucose-Lowering Effects of Imeglimin and Its Possible Beneficial Effects on Diabetic Complications" Biology 12, no. 5: 726. https://doi.org/10.3390/biology12050726
APA StyleYanai, H., Adachi, H., Hakoshima, M., & Katsuyama, H. (2023). Glucose-Lowering Effects of Imeglimin and Its Possible Beneficial Effects on Diabetic Complications. Biology, 12(5), 726. https://doi.org/10.3390/biology12050726