Clinical Effectiveness of a Combination of Black Elder Berries, Violet Herb, and Calendula Flowers in Chronic Obstructive Pulmonary Disease: The Results of a Double-Blinded Placebo-Controlled Study

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
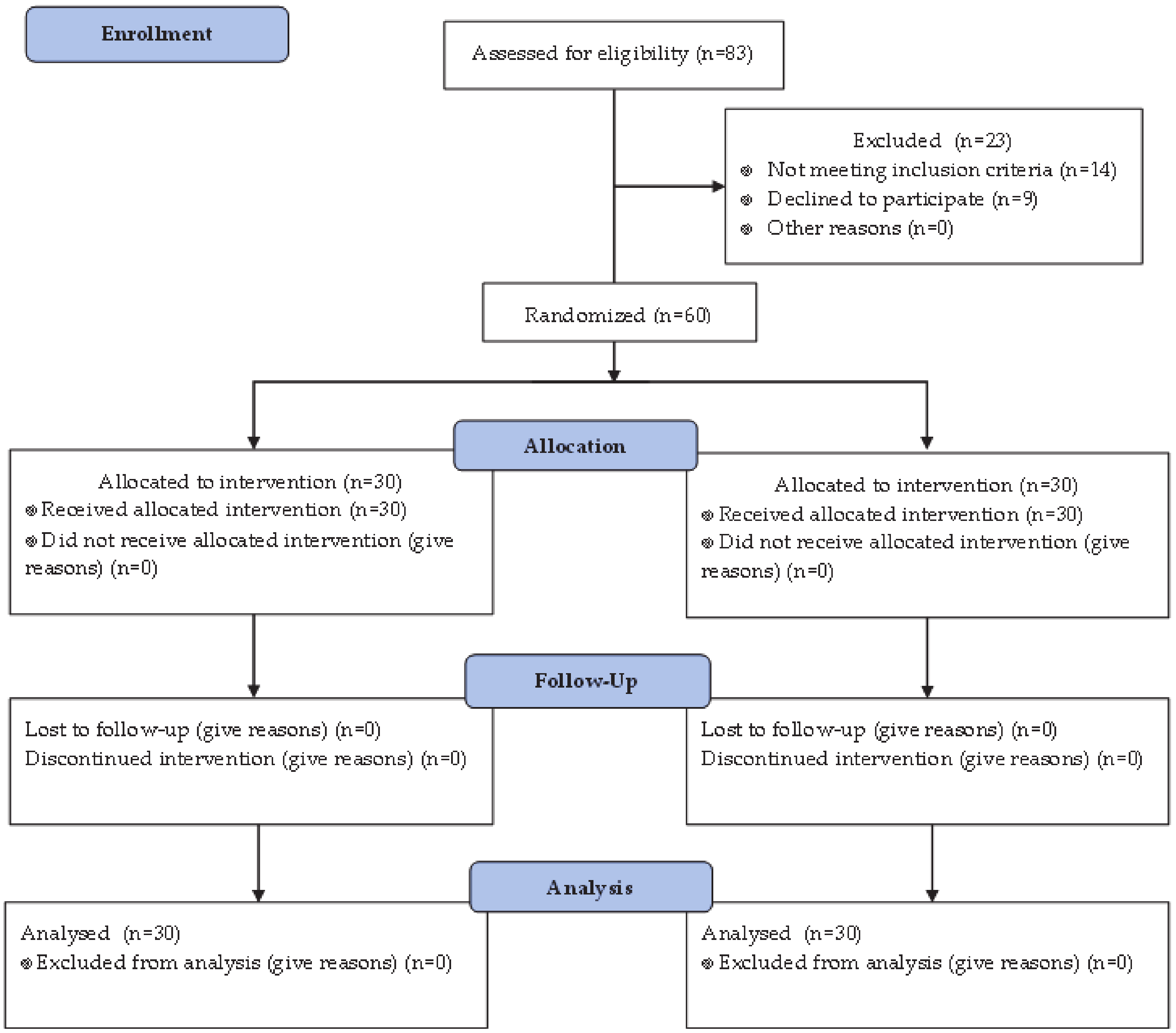
2.2. Study Design
2.3. Production and Dispensing of Preparations
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Belchamber, K.B.R.; Donnelly, L.E. Macrophage Dysfunction in Respiratory Disease. Results Probl. Cell Differ. 2017, 62, 299–313. [Google Scholar] [PubMed]
- Barnes, P.J. The cytokine network in COPD. Am. J. Respir. Cell Mol. Biol. 2009, 41, 631–638. [Google Scholar] [PubMed]
- Parolari, A.; Poggio, P.; Myasoedova, V.; Songia, P.; Bonalumi, G.; Pilozzi, A.; Pacini, D.; Alamanni, F.; Tremoli, E. Biomarkers in Coronary Artery Bypass Surgery: Ready for Prime Time and Outcome Prediction? Front. Cardiovasc. Med. 2015, 2, 39. [Google Scholar] [PubMed] [Green Version]
- Aaron, S.D.; Angel, J.B.; Lunau, M.; Wright, K.; Fex, C.; Le Saux, N.; Dales, R.E. Granulocyte inflammatory markers and airway infection during acute exacerbation of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 163, 349–355. [Google Scholar] [PubMed]
- Di Stefano, A.; Caramori, G.; Gnemmi, I.; Contoli, M.; Vicari, C.; Capelli, A.; Magno, F.; D’Anna, S.E.; Zanini, A.; Brun, P.; et al. T helper type 17-related cytokine expression is increased in the bronchial mucosa of stable chronic obstructive pulmonary disease patients. Clin. Exp. Immunol. 2009, 157, 316–324. [Google Scholar]
- Vitenberga, Z.; Pilmane, M.; Babjoniseva, A. The evaluation of inflammatory, anti-inflammatory and regulatory factors contributing to the pathogenesis of COPD in airways. Pathol. Res. Pract. 2019, 215, 97–105. [Google Scholar]
- Ambrocio-Ortiz, E.; Pérez-Rubio, G.; Abarca-Rojano, E.; Montaño, M.; Ramos, C.; Hernández-Zenteno, R.D.J.; Del Angel-Pablo, A.D.; Reséndiz-Hernández, J.M.; Ramírez-Venegas, A.; Falfán-Valencia, R. Influence of proinflammatory cytokine gene polymorphisms on the risk of COPD and the levels of plasma protein. Cytokine 2018, 111, 364–370. [Google Scholar]
- Strassheim, D.; Karoor, V.; Stenmark, K.; Verin, A.; Gerasimovskaya, E. A current view of G protein-coupled receptor-mediated signaling in pulmonary hypertension: Finding opportunities for therapeutic intervention. Vessel Plus 2018, 2, 21. [Google Scholar]
- Kirichenko, T.V.; Sobenin, I.A.; Nikolic, D.; Rizzo, M.; Orekhov, A.N. Anti-cytokine therapy for prevention of atherosclerosis. Phytomedicine 2016, 23, 1198–1210. [Google Scholar]
- Orekhov, A.N.; Sobenin, I.A.; Korneev, N.V.; Kirichenko, T.V.; Myasoedova, V.A.; Melnichenko, A.A.; Balcells, M.; Edelman, E.R.; Bobryshev, Y.V. Anti-atherosclerotic therapy based on botanicals. Recent Pat. Cardiovasc. Drug Discov. 2013, 8, 56–66. [Google Scholar]
- Leidy, N.K.; Schmier, J.K.; Jones, M.K.; Lloyd, J.; Rocchiccioli, K. Evaluating symptoms in chronic obstructive pulmonary disease: Validation of the Breathlessness, Cough and Sputum Scale. Respir. Med. 2003, 97 (Suppl. A), S59–S70. [Google Scholar] [CrossRef]
- Calvo, M.J.; Martínez, M.S.; Torres, W.; Chávez-Castillo, M.; Luzardo, E.; Villasmil, N.; Salazar, J.; Velasco, M.; Bermúdez, V. Omega-3 polyunsaturated fatty acids and cardiovascular health: A molecular view into structure and function. Vessel Plus 2017, 1, 116–128. [Google Scholar] [CrossRef] [Green Version]
- Marin, L.; Colombo, P.; Bebawy, M.; Young, P.M.; Traini, D. Chronic obstructive pulmonary disease: Patho-physiology, current methods of treatment and the potential for simvastatin in disease management. Expert Opin. Drug Deliv. 2011, 8, 1205–1220. [Google Scholar] [CrossRef] [PubMed]
- So, J.Y.; Dhungana, S.; Beros, J.J.; Criner, G.J. Statins in the treatment of COPD and asthma-where do we stand? Curr. Opin. Pharmacol. 2018, 40, 26–33. [Google Scholar] [CrossRef]
- Yıldızeli, Ş.O.; Balcan, B.; Eryüksel, E.; Ceyhan, B.B.; Karakurt, S.; Çelikel, T. Influence of Statin Therapy on Exacerbation Frequency in Patients with Chronic Obstructive Pulmonary Disease. Turk. Thorac. J. 2017, 18, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Sanja, M.; Jozsef, P.; Sanja, P.G.; Ivana, C.; Ivana, G.; Lana, G.; Gordana, S.; Renata, L.; Lepej Snjezana, Z. Cytokines and statin therapy in chronic obstructive pulmonary disease patients. Scand. J. Clin. Lab. Investig. 2018, 2, 533–538. [Google Scholar] [CrossRef]
- Rogliani, P.; Ora, J.; Di Daniele, N.; Lauro, D. Pleiotropic effects of hypoglycemic agents: Implications in asthma and COPD. Curr. Opin. Pharmacol. 2018, 40, 34–38. [Google Scholar] [CrossRef]
- Matera, M.G.; Page, C.; Rogliani, P.; Calzetta, L.; Cazzola, M. Therapeutic Monoclonal Antibodies for the Treatment of Chronic Obstructive Pulmonary Disease. Drugs 2016, 76, 1257–1270. [Google Scholar] [CrossRef]
- Rennard, S.I.; Fogarty, C.; Kelsen, S.; Long, W.; Ramsdell, J.; Allison, J.; Mahler, D.; Saadeh, C.; Siler, T.; Snell, P.; et al. The safety and efficacy of infliximab in moderate-to-severe chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2007, 175, 926–934. [Google Scholar] [CrossRef]
- Garth, J.; Barnes, J.W.; Krick, S. Targeting Cytokines as Evolving Treatment Strategies in Chronic Inflammatory Airway Diseases. Int. J. Mol. Sci. 2018, 19, 3402. [Google Scholar] [CrossRef] [Green Version]
- Sobenin, I.A.; Myasoedova, V.A.; Orekhov, A.N. Phytoestrogen-Rich Dietary Supplements in Anti-Atherosclerotic Therapy in Postmenopausal Women. Curr. Pharm. Des. 2016, 22, 152–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myasoedova, V.A.; Chistiakov, D.A.; Grechko, A.V.; Orekhov, A.N. Matrix Metalloproteinases in Pro-Atherosclerotic Arterial Remodeling. J. Mol. Cell Cardiol. 2018, 123, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Di Minno, A.; Zanobini, M.; Myasoedova, V.A.; Valerio, V.; Songia, P.; Saccocci, M.; Di Minno, M.N.D.; Tremoli, E.; Poggio, P. Could Circulating Fetuin A Be a Biomarker of Aortic Valve Stenosis? Int. J. Cardiol. 2017, 249, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Shin, N.R.; Kim, S.H.; Ko, J.W.; Park, S.H.; Lee, I.C.; Ryu, J.M.; Kim, J.C.; Shin, I.S. HemoHIM, a herbal preparation, alleviates airway inflammation caused by cigarette smoke and lipopolysaccharide. Lab. Anim. Res. 2017, 33, 40–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, C.M.; Oh, I.H.; Choe, B.K.; Yoon, T.Y.; Choi, J.M.; Hwang, J. Consuming Green Tea at Least Twice Each Day Is Associated with Reduced Odds of Chronic Obstructive Lung Disease in Middle-Aged and Older Korean Adults. J. Nutr. 2018, 148, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Chung, V.C.; Wu, X.; Ma, P.H.; Ho, R.S.; Poon, S.K.; Hui, D.S.; Wong, S.Y.; Wu, J.C. Chinese Herbal Medicine and Salmeterol and Fluticasone Propionate for Chronic Obstructive Pulmonary Disease: Systematic Review and Network Meta-Analysis. Medicine 2016, 95, e3702. [Google Scholar] [CrossRef]
- Wang, G.; Liu, B.; Cao, Y.; Du, Y.; Zhang, H.; Luo, Q.; Li, B.; Wu, J.; Lv, Y.; Sun, J.; et al. Effects of two Chinese herbal formulae for the treatment of moderate to severe stable chronic obstructive pulmonary disease: A multicenter, double-blind, randomized controlled trial. PLoS ONE 2014, 9, e103168. [Google Scholar] [CrossRef]
- Dr Duke’s Phytochemical and Ethnobotanical Database. Available online: https://phytochem.nal.usda.gov (accessed on 14 April 2020).


{kind=link}
| Indicators | Inflaminat | Placebo | p |
|---|---|---|---|
| Age, years | 54 ± 4 | 55 ± 3 | 0.785 |
| Number of exacerbations, per month | 0.15 ± 0.09 | 0.18 ± 0.10 | 0.163 |
| BCSS, points | 3.0 ± 0.6 | 3.0 ± 0.5 | 0.874 |
| FEV1/FVC, % | 66 ± 17 | 68 ± 25 | 0.608 |
| FEV1, % | 61 ± 12 | 62 ± 15 | 0.695 |
| ∆FEV1, % | 5 ± 4 | 6 ± 3 | 0.702 |
| Indicators | Group | 12 Month Before Inclusion | 0–3 Months of Follow-Up | 3–6 Months of Follow-Up |
|---|---|---|---|---|
| BCSS, points | Inflaminat | 3.0 ± 0.6 | 2.8 ± 0.6 | 1.9 ± 0.7 * |
| Placebo | 3.0 ± 0.5 | 2.8 ± 0.7 | 2.9 ± 0.6 | |
| Number of exacerbations, per month | Inflaminat | 0.15 ± 0.09 | 0.15 ± 0.08 | 0.12 ± 0.11 |
| Placebo | 0.18 ± 0.10 | 0.17 ± 0.10 | 0.19 ± 0.13 | |
| Hospitalizations due to COPD exacerbation, per month | Inflaminat | 0.07 ± 0.04 | 0.06 ± 0.07 | 0.07 ± 0.05 |
| Placebo | 0.08 ± 0.06 | 0.07 ± 0.04 | 0.08 ± 0.07 |
| Symptoms | Group | Baseline | 3 Months | 6 Months |
|---|---|---|---|---|
| Cough, points | Inflaminat | 2.9 ± 0.7 | 2.6 ± 0.5 | 1.2 ± 0.7 * |
| Placebo | 3.1 ± 0.6 | 2.9 ± 0.6 | 3.0 ± 0.7 | |
| Breathlessness, points | Inflaminat | 2.8 ± 0.5 | 2.9 ± 0.5 | 2.6 ± 0.6 |
| Placebo | 2.9 ± 0.5 | 2.7 ± 0.7 | 2.8 ± 0.6 | |
| Sputum production, points | Inflaminat | 3.2 ± 0.5 | 2.8 ± 0.7 | 1.8 ± 0.7 * |
| Placebo | 2.9 ± 0.5 | 2.8 ± 0.6 | 2.9 ± 0.6 |
| Indicators | Group | Baseline | 3 Months | 6 Months |
|---|---|---|---|---|
| FEV1/FVC, % | Inflaminat | 61 ± 13 | 63 ± 16 | 66 ± 18 |
| Placebo | 62 ± 15 | 62 ± 12 | 64 ± 15 | |
| FEV1, % | Inflaminat | 66 ± 18 | 68 ± 16 | 73 ± 17 * |
| Placebo | 68 ± 25 | 69 ± 22 | 71 ± 21 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kirichenko, T.V.; Sobenin, I.A.; Markina, Y.V.; Gerasimova, E.V.; Grechko, A.V.; Kashirskikh, D.A.; Romanenko, E.B.; Wu, W.-K.; Orekhov, A.N. Clinical Effectiveness of a Combination of Black Elder Berries, Violet Herb, and Calendula Flowers in Chronic Obstructive Pulmonary Disease: The Results of a Double-Blinded Placebo-Controlled Study. Biology 2020, 9, 83. https://doi.org/10.3390/biology9040083
Kirichenko TV, Sobenin IA, Markina YV, Gerasimova EV, Grechko AV, Kashirskikh DA, Romanenko EB, Wu W-K, Orekhov AN. Clinical Effectiveness of a Combination of Black Elder Berries, Violet Herb, and Calendula Flowers in Chronic Obstructive Pulmonary Disease: The Results of a Double-Blinded Placebo-Controlled Study. Biology. 2020; 9(4):83. https://doi.org/10.3390/biology9040083
Chicago/Turabian StyleKirichenko, Tatiana V., Igor A. Sobenin, Yuliya V. Markina, Elena V. Gerasimova, Andrey V. Grechko, Dmitry A. Kashirskikh, Elena B. Romanenko, Wei-Kai Wu, and Alexander N. Orekhov. 2020. "Clinical Effectiveness of a Combination of Black Elder Berries, Violet Herb, and Calendula Flowers in Chronic Obstructive Pulmonary Disease: The Results of a Double-Blinded Placebo-Controlled Study" Biology 9, no. 4: 83. https://doi.org/10.3390/biology9040083
APA StyleKirichenko, T. V., Sobenin, I. A., Markina, Y. V., Gerasimova, E. V., Grechko, A. V., Kashirskikh, D. A., Romanenko, E. B., Wu, W. -K., & Orekhov, A. N. (2020). Clinical Effectiveness of a Combination of Black Elder Berries, Violet Herb, and Calendula Flowers in Chronic Obstructive Pulmonary Disease: The Results of a Double-Blinded Placebo-Controlled Study. Biology, 9(4), 83. https://doi.org/10.3390/biology9040083