

Systems Thinking for Supply Chains: Identifying Bottlenecks Using Process Mapping of a Child Health Intervention in the Democratic Republic of the Congo (DRC)

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
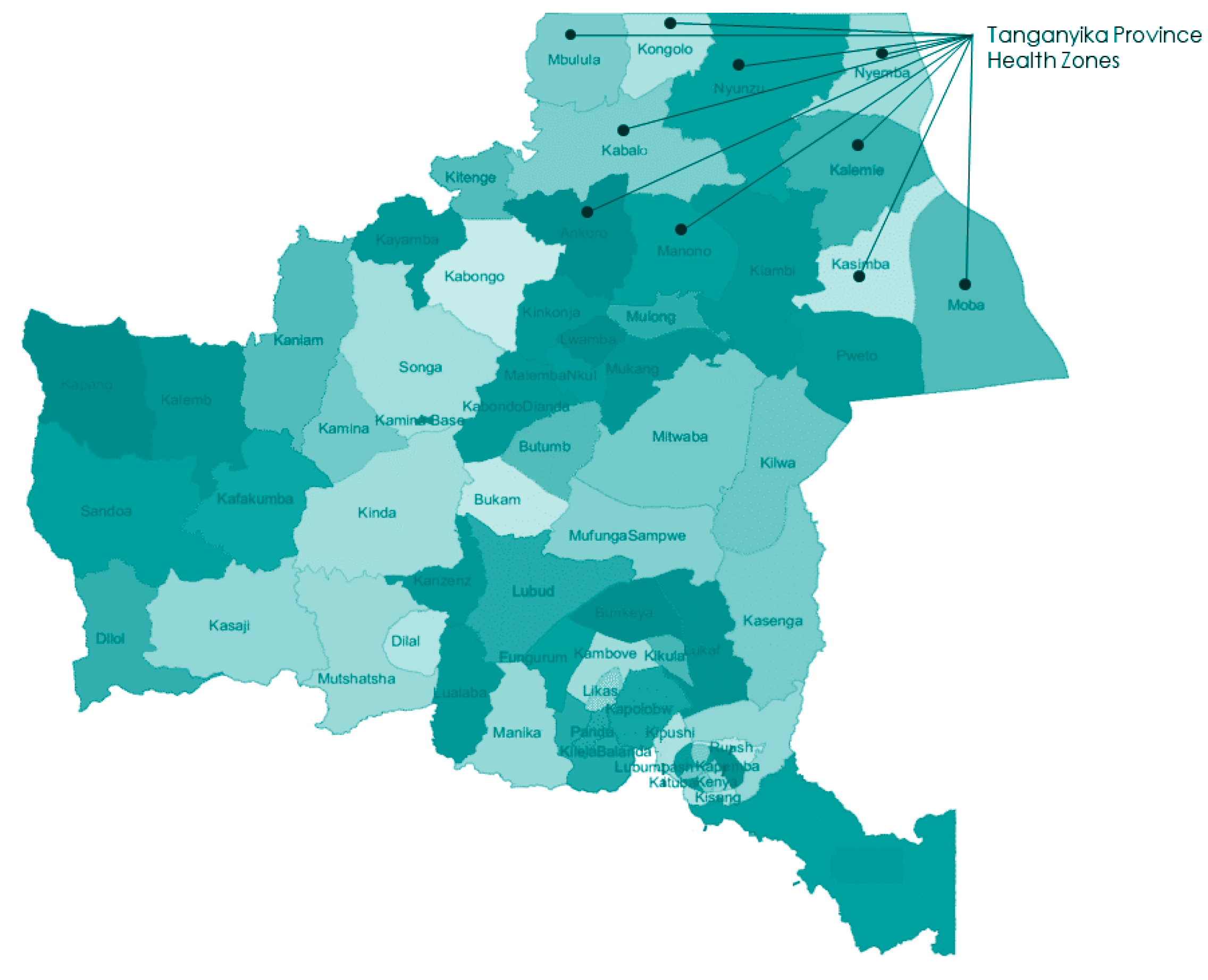
2.1. Study Setting
2.2. Study Design, Data Collection, and Analysis
3. Results
3.1. Process Mapping of Procurement and Distribution of iCCM Medical Products
3.1.1. Primary Actors, Administrative Organizations, and Their Roles in iCCM Supply Chain Processes
3.1.2. System Overview
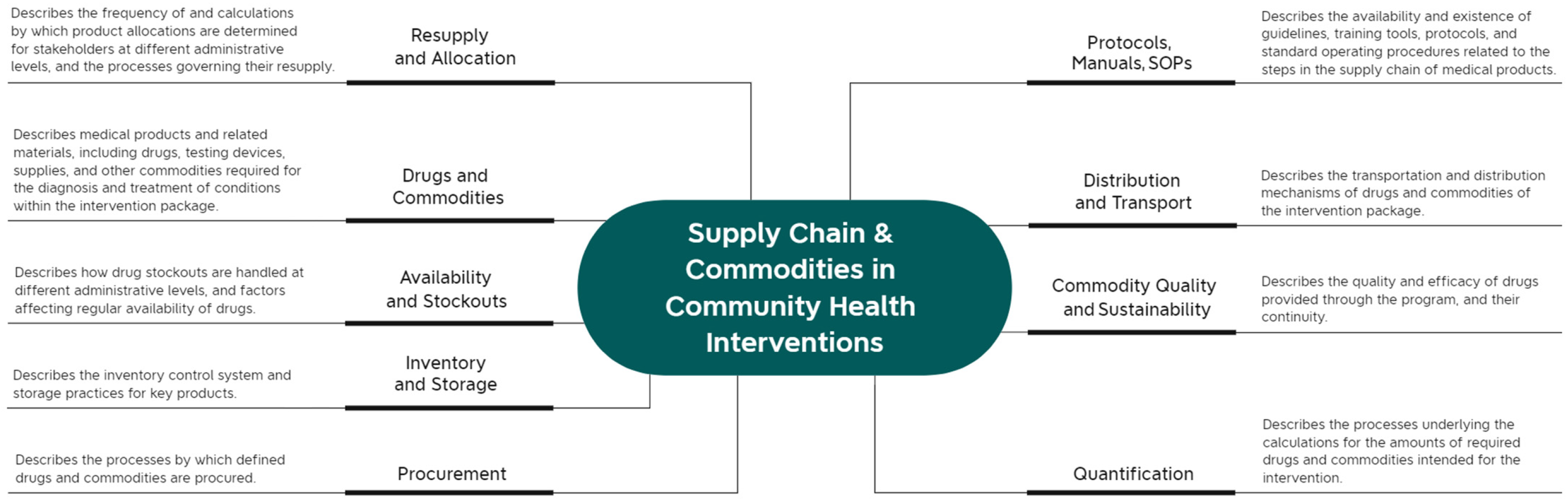
3.2. Supply Chain Thematic Areas
3.2.1. Drugs and Commodities, Quality, and Sustainability
3.2.2. Quantification and Allocation
3.2.3. Ordering and Procurement
3.2.4. Transmission, Distribution, and Reception
3.2.5. Inventory and Storage
3.2.6. Stockouts and Emergency Orders
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
| 1 | While all of the medicines listed in this study were technically included as items within the country’s national essential medicines list (2010) [16], only some formulations were listed as actually being available at or procured for health facilities or general hospitals. While rectal artesunate (100 mg suppositories) is included in WHO’s Model List of Essential Medicines [17] and Model List of Essential Medicines for Children as of 2017, it was not yet a part of DRC’s most recent Essential Drug List at the time of this study. Only from 2017 onwards was quality assured RAS was available on the market [18]. |
References
- Yadav, P. Health Product Supply Chains in Developing Countries: Diagnosis of the Root Causes of Underperformance and an Agenda for Reform. Health Syst. Reform 2015, 1, 142–154. [Google Scholar] [CrossRef] [PubMed]
- Dowling, P. Healthcare Supply Chains in Developing Countries: Situational Analysis; DELIVER PROJECT, Task Order 4; USAID: Arlington, VA, USA, 2011. [Google Scholar]
- Bennett, S.; Glandon, D.; Rasanathan, K. Governing multisectoral action for health in low-income and middle-income countries: Unpacking the problem and rising to the challenge. BMJ Glob. Health 2018, 3, e000880. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, S.; Salvatore, F.P.; De Pascale, G.; Faccilongo, N. Insights for the future of health system partnerships in low- and middle-income countries: A systematic literature review. BMC Health Serv Res. 2020, 20, 571. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Improving Health System Efficiency: Democratic Republic of the Congo: Improving Aid Coordination in the Health Sector; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/186673 (accessed on 8 December 2022).
- Senge, P.M. The Fifth Discipline: The Art and Practice of the Learning Organization; Doubleday/Currency: New York, NY, USA, 1990. [Google Scholar]
- Antonacci, G.; Reed, J.E.; Lennox, L.; Barlow, J. The use of process mapping in healthcare quality improvement projects. Health Serv. Manag. Res. 2018, 31, 74–84. [Google Scholar] [CrossRef] [PubMed]
- De Savigny, D.; Blanchet, K.; Adam, T. Applied Systems Thinking for Health Systems Research: A Methodological Handbook; McGraw-Hill: London, UK, 2017. [Google Scholar]
- Antonacci, G.; Lennox, L.; Barlow, J.; Evans, L.; Reed, J. Process mapping in healthcare: A systematic review. BMC Health Serv. Res. 2021, 21, 342. [Google Scholar] [CrossRef] [PubMed]
- NHS Institute for Innovation and Improvement. Improvement Leaders’ Guides; Series 1: Process mapping, analysis and redesign; Department of Health: London, UK, 2005. [Google Scholar]
- Karim, A.; de Savigny, D.; Awor, P.; Muñoz, D.C.; Mäusezahl, D.; Tshefu, A.K.; Ngaima, J.S.; Enebeli, U.; Isiguzo, C.; Nsona, H.; et al. The building blocks of community health systems: A systems framework for the design, implementation and evaluation of iCCM programs and community-based interventions. BMJ Glob. Health 2022, 7, e008493. [Google Scholar] [CrossRef]
- Karim, A.; de Savigny, D.; Ngaima, J.S.; Mäusezahl, D.; Cobos Muñoz, D.; Tshefu, A. Assessing Determinants of Programmatic Performance of Community Management of Malaria, Pneumonia, and Diarrhea in Children in Africa: Protocol and Data Collection for a Mixed Methods Evaluation of Integrated Community Case Management. JMIR Res. Protoc. 2022, 11, e33076. [Google Scholar] [CrossRef] [PubMed]
- Langston, A.; Wittcoff, A.; Ngoy, P.; O’Keefe, J.; Kozuki, N.; Taylor, H.; Lainez, Y.B.; Bacary, S. Testing a simplified tool and training package to improve integrated Community Case Management in Tanganyika Province, Democratic Republic of Congo: A quasi-experimental study. J. Glob. Health 2019, 9, 010810. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117–124. [Google Scholar] [CrossRef]
- Karim, A.; Cobos Munoz, D.; Mäusezahl, D.; de Savigny, D. A systems approach to assessing complexity in health interventions: An effectiveness decay model for integrated community case management. Glob. Health Action 2020, 13, 1794106. [Google Scholar] [CrossRef]
- Liste Nationale des Médicaments Essentiels; Révision Mars 2010; Ministre de la Santé de RDC: Kinshasa, Democratic Republic of the Congo, 2010.
- WHO Model List of Essential Medicines; World Health Organization: Geneva, Switzerland, 2017.
- Lengeler, C.; Burri, C.; Awor, P.; Athieno, P.; Kimera, J.; Tumukunde, G.; Angiro, I.; Tshefu, A.; Okitawutshu, J.; Kalenga, J.-C.; et al. Community access to rectal artesunate for malaria (CARAMAL): A large-scale observational implementation study in the Democratic Republic of the Congo, Nigeria and Uganda. PLOS Glob. Public Health 2022, 2, e0000464. [Google Scholar] [CrossRef]
- Chandani, Y.; Andersson, S.; Heaton, A.; Noel, M.; Shieshia, M.; Mwirotsi, A.; Krudwig, K.; Nsona, H.; Felling, B. Making products available among community health workers: Evidence for improving community health supply chains from Ethiopia, Malawi, and Rwanda. (Themed Issue: Current scientific evidence for integrated community case management (iCCM) in Africa: Finding. J. Glob. Health 2014, 4, 020405. [Google Scholar] [CrossRef]
- Rao, V.B.; Schellenberg, D.; Ghani, A.C. Overcoming health systems barriers to successful malaria treatment. Trends Parasitol. 2013, 29, 164–180. [Google Scholar] [CrossRef] [PubMed]
- Chandani, Y.; Noel, M.; Andersson, S.; Ombeva, A.; Shieshia, M.; Heaton, A.; Felling, B.; Mugeni, C. Improving community level supply chain performance using team-led, data driven solutions in Malawi and Rwanda. Am. J. Trop. Med. Hyg. 2013, 89, 327–328. [Google Scholar]
- Miller, N.P.; Zunong, N.; Al-Sorouri, T.A.A.; Alqadasi, Y.M.; Ashraf, S.; Siameja, C. Implementing integrated community case management during conflict in Yemen. (Research Theme: Community health in emergencies). J. Glob. Health 2020, 10, 020601. [Google Scholar] [CrossRef]
- Henriksson, D.K.; Fredriksson, M.; Waiswa, P.; Selling, K.; Peterson, S.S. Bottleneck analysis at district level to illustrate gaps within the district health system in Uganda. Glob. Health Action 2017, 10, 1327256. [Google Scholar] [CrossRef] [PubMed]
- USAID. Mozambique: Strengthening the Community Health Worker Supply Chain; Deliver Project. Final Report; USAID: Arlington, VA, USA, 2014. [Google Scholar]
- Global Fund; WHO; UNICEF. Integrated Community Case Management (iCCM) in Sub-Saharan Africa: Successes & Challenges with Access, Speed & Quality Thematic Review Report. 2018. Available online: https://www.childhealthtaskforce.org/resources/presentation/2019/thematic-review-iccm-success-challenges-access-speed-quality-e-shargie (accessed on 3 February 2024).
- Altaras, R.; Montague, M.; Graham, K.; Strachan, C.E.; Senyonjo, L.; King, R.; Counihan, H.; Mubiru, D.; Källander, K.; Meek, S.; et al. Integrated community case management in a peri-urban setting: A qualitative evaluation in Wakiso District, Uganda. BMC Health Serv. Res. 2017, 17, 785. [Google Scholar] [CrossRef] [PubMed]
- VillageReach. Exploring New Distribution Models for Vaccines and other Health Commodities Adapted to the on the Ground Realities of the Equateur and Tshuapa Provinces, Democratic Republic of Congo; VillageReach: Seattle, WA, USA, 2015. [Google Scholar]
- Javanparast, S.; Windle, A.; Freeman, T.; Baum, F. Community Health Worker Programs to Improve Healthcare Access and Equity: Are They Only Relevant to Low- and Middle-Income Countries? Int. J. Health Policy Manag. 2018, 7, 943–954. [Google Scholar] [CrossRef] [PubMed]
- John Snow, Inc. Quantification of Health Commodities: A Guide to Forecasting and Supply Planning for Procurement; John Snow, Inc.: Arlington, VA, USA, 2017. [Google Scholar]
- John Snow, Inc. Baseline Assessment for Cstock; John Snow, Inc.: Boston, MA, USA, 2018. [Google Scholar]
- Vledder, M.; Friedman, J.; Sjöblom, M.; Brown, T.; Yadav, P. Improving Supply Chain for Essential Drugs in Low-Income Countries: Results from a Large Scale Randomized Experiment in Zambia. Health Syst. Reform 2019, 5, 158–177. [Google Scholar] [CrossRef] [PubMed]
- Lufesi, N.N.; Andrew, M.; Aursnes, I. Deficient supplies of drugs for life threatening diseases in an African community. BMC Health Serv. Res. 2007, 7, 86. [Google Scholar] [CrossRef]
- John Snow, Inc. Information Systems for Supply Chain Management: The Case for Connecting Separate and Interoperable Technology Applications for Logistics Management Information System and Health Information Management Systems Data; John Snow, Inc.: Arlington, VA, USA, 2017. [Google Scholar]
- Sant Fruchtman, C.; Mbuyita, S.; Mwanyika-Sando, M.; Braun, M.; de Savigny, D.; Cobos Muñoz, D. The complexity of scaling up an mHealth intervention: The case of SMS for Life in Tanzania from a health systems integration perspective. BMC Health Serv. Res. 2021, 21, 343. [Google Scholar] [CrossRef]
- Pisa, M.; McCurdy, D. Improving Global Health Supply Chains through Traceability; CGD Policy Paper; Center for Global Development: Washington, DC, USA, 2019; Available online: https://www.cgdev.org/publication/improving-global-health-supply-chains-through-traceability (accessed on 9 December 2022).
- Zhu, P.; Jian, H.; Yue, J.; Xiaotong, L. A Blockchain Based Solution for Medication Anti-Counterfeiting and Traceability. IEEE Access 2020, 8, 184256–184272. [Google Scholar] [CrossRef]
- Lugada, E.; Komakech, H.; Ochola, I.; Mwebaze, S.; Olowo Oteba, M.; Okidi Ladwar, D. Health supply chain system in Uganda: Current issues, structure, performance, and implications for systems strengthening. J. Pharm. Policy Pract. 2022, 15, 14. [Google Scholar] [CrossRef]
- Schell, S.F.; Luke, D.A.; Schooley, M.W.; Elliott, M.B.; Herbers, S.H.; Mueller, N.B.; Bunger, A.C. Public health program capacity for sustainability: A new framework. Implement. Sci. 2013, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Denyer Willis, L.; Chandler, C. Quick fix for care, productivity, hygiene and inequality: Reframing the entrenched problem of antibiotic overuse. BMJ Glob. Health 2019, 4, e001590. [Google Scholar] [CrossRef]
- Hilton, C. Healthcare poverty-inequality and government quick fixes. BJPsych Bull. 2021, 45, 68. [Google Scholar] [CrossRef] [PubMed]
- Nanyonjo, A.; Counihan, H.; Siduda, S.G.; Belay, K.; Sebikaari, G.; Tibenderana, J. Institutionalization of integrated community case management into national health systems in low- and middle-income countries: A scoping review of the literature. Glob. Health Action 2019, 12, 1678283. [Google Scholar] [CrossRef]
- VillageReach. Outsourcing Transport to Improve Health at the Last Mile: A Case Study the Long Road to Health; VillageReach: Seattle, WA, USA, 2016. [Google Scholar]
- Olaniran, A.; Briggs, J.; Pradhan, A.; Bogue, E.; Schreiber, B.; Dini, H.S.; Hurkchand, H.; Ballard, M. Stock-outs of essential medicines among community health workers (CHWs) in low- and middle-income countries (LMICs): A systematic literature review of the extent, reasons, and consequences. Hum. Resour. Health 2022, 20, 58. [Google Scholar] [CrossRef] [PubMed]
- Briggs, J. Procurement and Supply Management for iCCM—Common Challenges. System for Improved Access to Pharmecuticals and Services; USAID: Nairobi, Kenya, 2016. [Google Scholar]
- Keane, E. Integrating Severe Acute Malnutrition into the Management of Childhood Diseases at Community Level in South Sudan Malaria Consortium Learning Paper Series. 2013. Available online: https://www.malariaconsortium.org/media (accessed on 10 December 2022).
- Wharton-Smith, A.; Counihan, H.; Strachan, C. Implementing Integrated Community Case Management: Stakeholder Experiences and Lessons Learned in Three African Countries. 2014. Available online: https://www.malariaconsortium.org/learningpapers. (accessed on 9 December 2022).
- World Health Organization and the UNICEF. Institutionalizing Integrated Community Case Management (iCCM) to End Preventable Child Deaths: A Technical Consultation and Country Action Planning, 22–26 July 2019, Addis Ababa; World Health Organization and the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2020. [Google Scholar]
- Chandani, Y.; Duffy, M.; Lamphere, B.; Noel, M.; Heaton, A.; Andersson, S. Quality improvement practices to institutionalize supply chain best practices for iCCM: Evidence from Rwanda and Malawi. Res. Soc. Adm. Pharm. 2017, 13, 1095–1109. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Source | No. Conducted/ Items Retrieved | Description of Participants or Items |
|---|---|---|
| Focus group discussions | 12 groups 101 participants | ReCos, supervisors, caregivers |
| Key informant interviews | 28 participants | Ministry and iCCM program staff at various administrative levels |
| Document review | 13 documents | iCCM and child health program policies, manuals, guidelines, and protocols; national and provincial supply chain policies and procedures |
| Commodity Requisition | Expected New Cases per ReCo |
|---|---|
| RDT | 40 cases per month |
| Paracetamol | 40 cases per month |
| Rectal artesunate | 0.5 cases per month |
| Amoxicillin | 10 cases per month |
| ORS | 10 cases per month |
| Gloves | 40 cases per month |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karim, A.; Burri, C.; Kila, J.S.N.; Bambwelo, N.; Bakukulu, J.T.; de Savigny, D. Systems Thinking for Supply Chains: Identifying Bottlenecks Using Process Mapping of a Child Health Intervention in the Democratic Republic of the Congo (DRC). Systems 2024, 12, 137. https://doi.org/10.3390/systems12040137
Karim A, Burri C, Kila JSN, Bambwelo N, Bakukulu JT, de Savigny D. Systems Thinking for Supply Chains: Identifying Bottlenecks Using Process Mapping of a Child Health Intervention in the Democratic Republic of the Congo (DRC). Systems. 2024; 12(4):137. https://doi.org/10.3390/systems12040137
Chicago/Turabian StyleKarim, Aliya, Christian Burri, Jean Serge Ngaima Kila, Nelson Bambwelo, Jean Tony Bakukulu, and Don de Savigny. 2024. "Systems Thinking for Supply Chains: Identifying Bottlenecks Using Process Mapping of a Child Health Intervention in the Democratic Republic of the Congo (DRC)" Systems 12, no. 4: 137. https://doi.org/10.3390/systems12040137
APA StyleKarim, A., Burri, C., Kila, J. S. N., Bambwelo, N., Bakukulu, J. T., & de Savigny, D. (2024). Systems Thinking for Supply Chains: Identifying Bottlenecks Using Process Mapping of a Child Health Intervention in the Democratic Republic of the Congo (DRC). Systems, 12(4), 137. https://doi.org/10.3390/systems12040137