

Applying Integrative Systems Methodology: The Case of Health Care Organizations


Abstract
:1. Call for Cybersystemics
2. Methodological Framework
2.1. Concepts and Sources
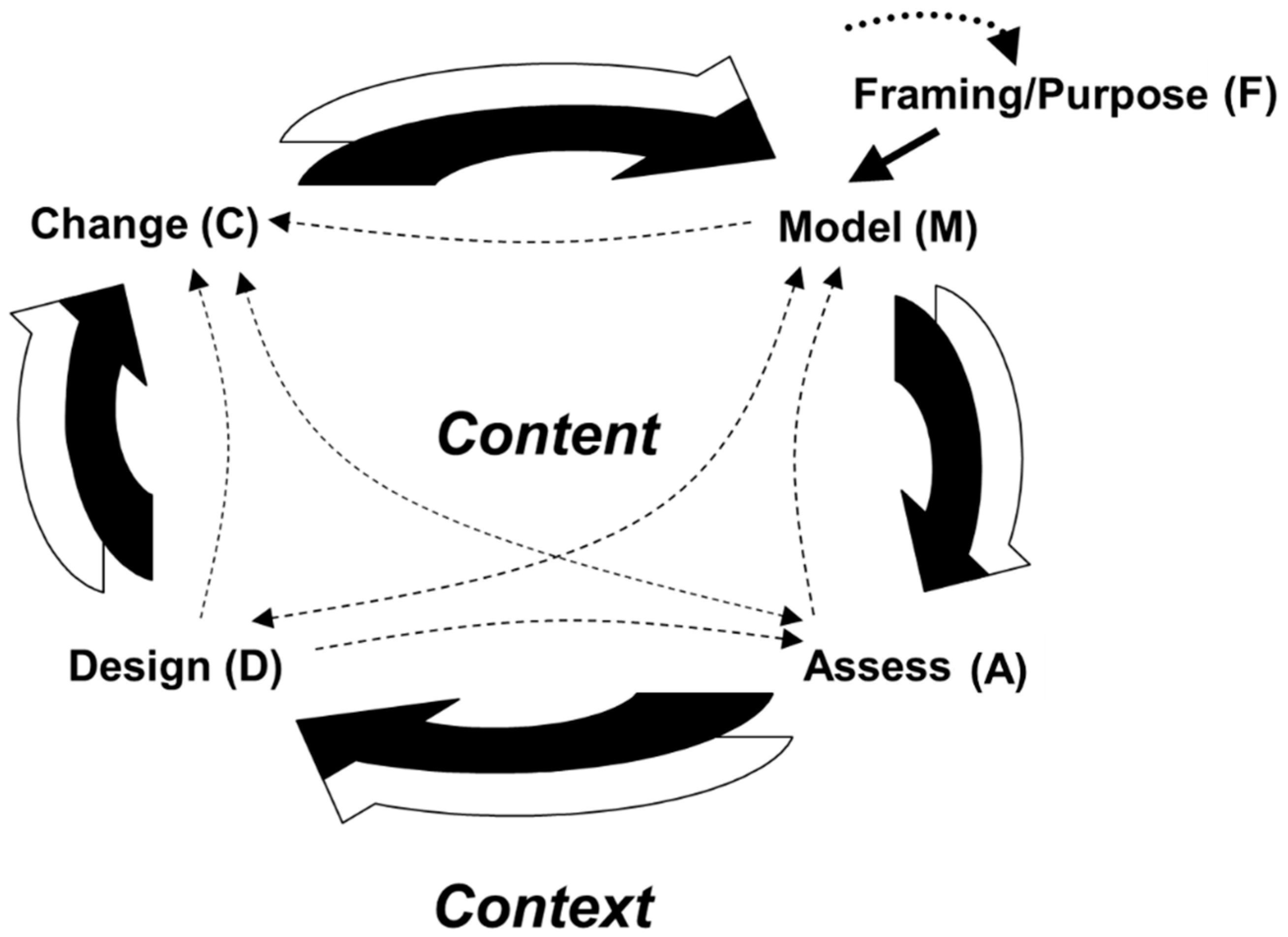
2.2. Integrative Systems Methodology
- -
- Modeling (formal or informal representation of the issue under study)
- -
- Assessment (diagnosis, evaluation of current situation)
- -
- Design (strategies, structures, etc., needed to solve the problem or improve the situation)
- -
- Change (of the system).

2.3. Epistemological Aspects
3. Case Study Part I–Framing (F)
3.1. Framing: Purpose and Overall Goals (F)
- (a)
- Guarantee of excellent oncological care in the context of the central hospital, using all the resources available within that powerful institution.
- (b)
- Provision of fast and high-level care for oncological patients all over the federal state, i.e., also outside the capital—in small towns and in the countryside, as far as possible “on the spot”.
- (c)
- An increasingly preventive orientation of oncological medicine in Carinthia.
3.2. Mapping the System at the Outset (M)
4. Case Study Part II–Content Level
4.1. Vision to Models (M)
4.2. Assessment/Diagnosis (A, D)
- Resistance of medical departments that should join the effort;
- Weak know-how and lack of interest among the peripheral hospitals;
- Deficits of knowledge among the independent physicians;
- Fear among doctors and nursing staff of increasing demands and uncertainties;
- Low motivation among staff;
- No formal authority among oncologists about parties that should be included;
- Scarce budgetary means;
- Limited personnel capacity in the central oncology unit;
- Low interest, among authorities, in preventive care.
- Winning the cooperation of medical departments at the Klagenfurt and peripheral hospitals;
- Multiply know how and enhance knowledge-building in the peripheral hospitals;
- Involve and link multiple resources;
- Create robust and nimble structures to enhance the viability of the oncological care system;
- Information management—make data and information available for the control of therapies and the creation of new therapy options;
- Balance decentralized and centralized care;
- Balance the efficiency of care operations and the effectiveness of care strategies.
4.3. Design and Change (D, C)
- (a)
- Psycho-hygiene: The staff in oncological care are subject to a stress load that tends to be greater than in other professions. Therefore, introducing psycho-hygienic measures was crucial, to sustain and foster the psychic health of people, adopting both preventive and restitutive measures.
- (b)
- Structure, information system and knowledge management: Structure is a powerful device that was considered crucial for strengthening the quality of care, coordination, and team cohesion. In addition, information systems and knowledge management were prominent in strengthening research.
- (c)
- Leadership: Ultimately everything in an organization is subject to the influence of leadership and hinges on its quality. Motivation as well as coordination and cohesion were identified as two main aspects to be strengthened by that driver. Coordination and cohesion then impinge strongly on cooperation. Equally crucial was a major effort to win the cooperation of all necessary parties.
5. Case Study Part III–Context Level
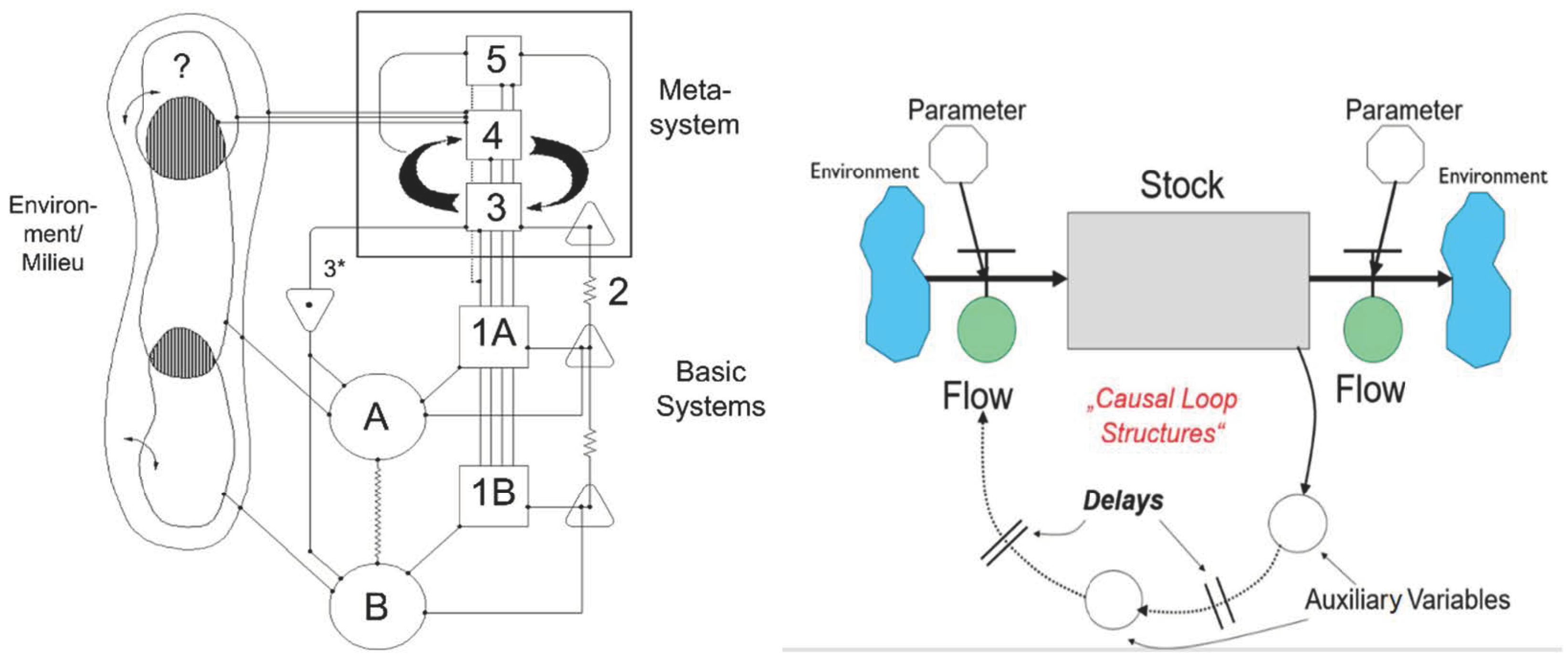
5.1. Master Structure (D)
- (1)
- Component 1. Management of a basic subsystem (an “operation”).
- (2)
- Component 2. Coordination of subsystems, attenuation of oscillations between them.
- (3)
- Component 3. Integrative management of a collective of subsystems.
- (4)
- Component 3*. Auditing and monitoring channel.
- (5)
- Component 4. Management for the long term, relationships with the overall environment.
- (6)
- Component 5. Normative management, corporate ethos.
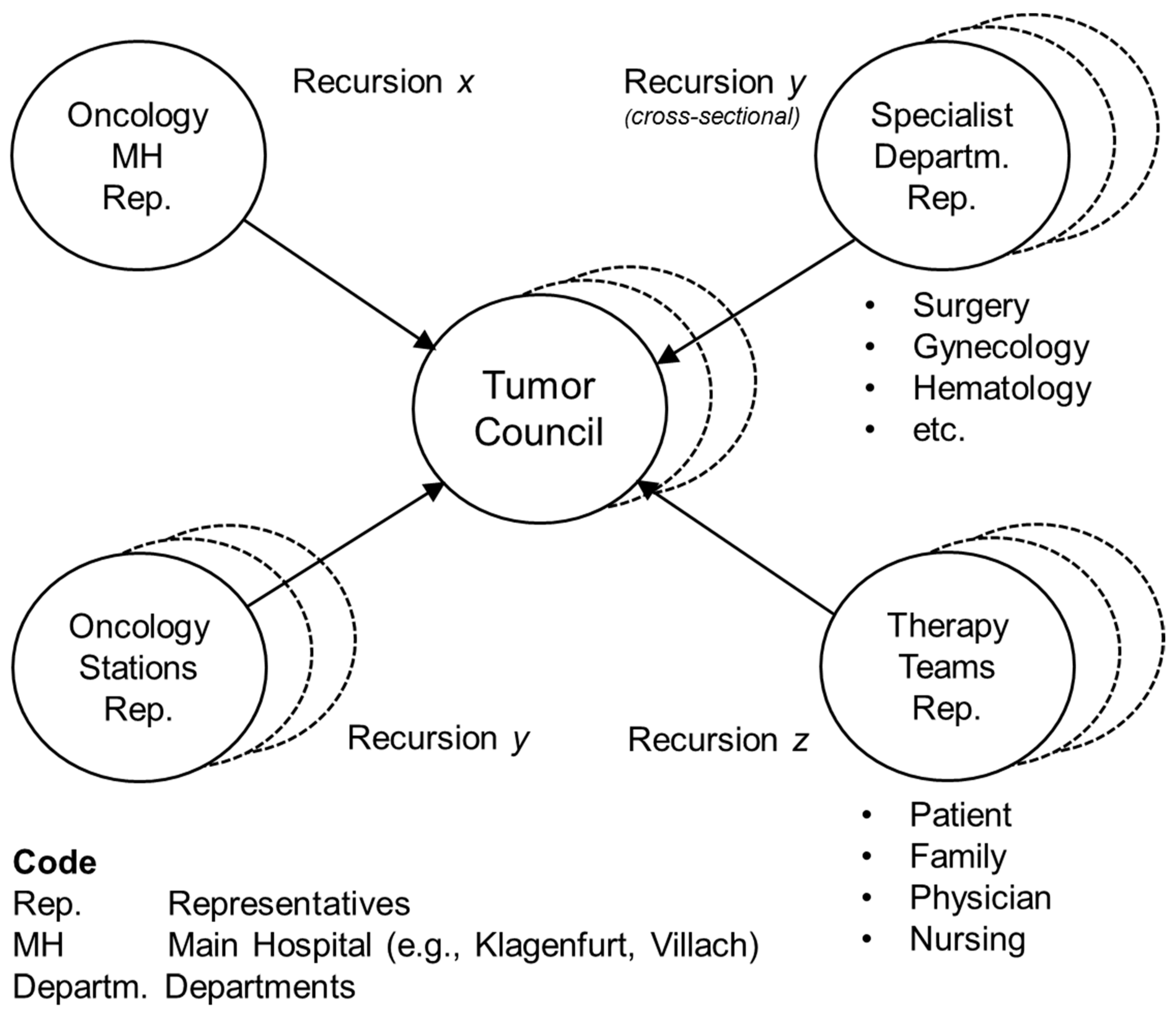
5.2. Team Organization (D)
6. Case Part IV–The Evolution of Oncology Carinthia (C)
7. Results
8. Conclusions
- (a)
- Ethos: The focus should be on the patient, with his or her family included. This means placing the patients and their quality of life at the center. Not only at the center, but also in command; the patient is the authority responsible for his or her health. For the doctors, nurses and other employees, a culture of the highest professional values, including unconditional commitment to patients, is the imperative to be adhered to. The principle of excellent care must pervade all activities. Goals must be high, and leaders need to energize the organization to attain them.
- (b)
- Systemic approach: Systemic thinking is a way of dealing competently with complex wholes. It enables systemic design for better organizations. The proposed thinking at the levels of both content and context forms a braid that enables a systemic process reaching from modelling to assessment to design to change. Unorthodox thinking, as our case showed, can produce management innovations that, although unwelcome at the beginning, go on to breed (unexpected) positive results and are adopted by the organization. To initiate and manage these innovations, powerful change agents are a sine qua non. Both an internal and external change agent were active, and in harmony. This may have been an important prerequisite for the successful performance of Oncology Carinthia [65].
- (c)
- Theory and practice: Practitioners are often theory averse. Therefore, we pursued another path, operating on a strong theoretical (and methodological) orientation, combining it with pragmatic, flexible implementation, and most important, with enduring dedication to the issues of health. This alternative path proved to be at the core of the success of Oncology Carinthia. The combination of theory-based and conceptually driven design, and reflexive, committed practice is mandatory for dealing effectively with complex organizational issues in a social system.
- (d)
- Methodology: We have tried to catalyze the dialectics of strategy and organization, proposing an integration of two system methodologies (SD and VSM) to facilitate dealing with the complex issues under study. These are not the only methodologies available, but they appear to be mature devices on which one can rely in the face of complexity. And they are complementary [45]. Much as with engineering, the chosen methods rely on the cyclic pair of reasoning and experimentation [66]. We have brought these methodologies together under the term Integrative Systems Methodology, a framework for systemic strategizing, i.e., for dealing with complexity in a long-term perspective.
- (e)
- Holistic organization design: The systemic approach provides highly effective heuristic devices and frameworks (e.g., VSM) for enhancing the viability and adaptiveness of organizations. Holistic design combines decentralization and centralization, as well as information flows from inside-out and outside-in, which is a better model than top-down and bottom-up. Structures can be nimble and robust at the same time, and a complex structure can be even more economical than a simplistic one. The systemic approach based on VSM, and other cybernetics-based structural models not discussed here. An example is Team Syntegrity, a systemic protocol for the interaction in large groups [67], and other cybersystemic models are remarkably effective in putting networks and virtual organizations in place, which absorb complexity pervasively. This proves to be the case here in an organization that is above all humanistic.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. System Dynamics and Organizational Cybernetics–Complementarity and Synergy (For a More Profound Treatment of the Topic, see: [45])

Appendix A.2. Combining Complementary Methodologies
References
- Ulrich, H. Die Unternehmung als Produktives Soziales System: Grundlagen der Allgemeinen Unternehmungslehre; Haupt: Bern, Switzerland, 1968. [Google Scholar]
- Beer, S. Diagnosing the System for Organizations; Wiley: Chichester, UK, 1985. [Google Scholar]
- Bleicher, K. Das Konzept. In Integriertes Management; Campus, Frankfurt a.M.: New York, NY, USA, 2004. [Google Scholar]
- Berlinski, D. On Systems Analysis; MIT Press: Cambridge, MA, USA, 1976. [Google Scholar]
- Hanssmann, F. Einführung in die Systemforschung. Methodik der modellgestützten Entscheidungsvorbereitung; Oldenbourg: München, Germany, 1993. [Google Scholar]
- Ackoff, R.L. Creating the Corporate Future: Plan or Be Planned for; Wiley: New York, NY, USA, 1981. [Google Scholar]
- Checkland, P.B.; Scholes, J. Soft Systems Methodology in Action; New edition; Wiley: Chichester, UK, 2000. [Google Scholar]
- Türke, R.-E. Governance. In Systemic Foundation and Framework; Physica: Heidelberg, Germany, 2008. [Google Scholar]
- Homer, J. Models that Matter; Grapeseed Press: Barrytown, NY, USA, 2012. [Google Scholar]
- Ison, R. Systems Practice: How to Act. In Situations of Uncertainty and Complexity in a Climate-Change World, 2nd ed.; Springer: London, UK, 2017. [Google Scholar]
- Schwaninger, M. Making Change Happen: Recollections of a Systems Professional. Kybernetes 2012, 41, 348–367. [Google Scholar] [CrossRef]
- Ulrich, W. Critical Heuristics of Social Planning: A New Approach to Practical Philosophy; Haupt: Bern, Switzerland, 1983. [Google Scholar]
- Von Foerster, H. Observing Systems; Intersystems Publications: Seaside, CA, USA, 1984. [Google Scholar]
- Espejo, R.; Schuhmann, W.; Schwaninger, M.; Bilello, U. Organizational Transformation and Learning. In A Cybernetic Approach to Management; Wiley: Chichester, UK, 1996. [Google Scholar]
- Hammond, D. The Science of Synthesis: Exploring the Social Implications of General Systems Theory; University Press of Colorado: Boulder, CO, USA, 2003. [Google Scholar]
- Jackson, M.C. Systems Approaches to Management; Kluwer Academic/Plenum: New York, NY, USA, 2000. [Google Scholar]
- Schwaninger, M.; Klocker, J. Holistic Systems Design: The Oncology Carinthia Study. In Social Systems Engineering; García-Díaz, C., Olaya, C., Eds.; Wiley: Chichester, UK, 2018. [Google Scholar]
- Schwaninger, M. Methodologies in Conflict: Achieving Synergies between System Dynamics and Organizational Cybernetics. Syst. Res. Behav. Sci. 2004, 21, 411–431. [Google Scholar] [CrossRef]
- Schwaninger, M. An Integrative Systems Methodology for Dealing with Complex Issues. In GABEK VI—Sozial Verantwortliche Entscheidungsprozesse; Zelger, J., Müller, J., Plangge, S., Eds.; StudienVerlag: Innsbruck, Austria, 2013; pp. 177–196. [Google Scholar]
- Ashby, W.R. An Introduction to Cybernetics; Chapman & Hall: London, UK, 1956. [Google Scholar]
- Beer, S. The Heart of Enterprise; Wiley: Chichester, UK, 1979. [Google Scholar]
- Gell-Mann, M. What is Complexity? Remarks on simplicity and complexity. Complexity 1995, 1, 16–19. [Google Scholar] [CrossRef]
- Mitchell, M. Complexity. In A Guided Tour; Oxford University Press: New York, NY, USA, 2009. [Google Scholar]
- Rescher, N. Complexity. In A Philosophical Overview; Transaction Publishers: New Brunswick, NJ, USA; London, UK, 1998. [Google Scholar]
- Checkland, P.B. Systems Thinking, Systems Practice; Wiley: Chichester, UK, 1981. [Google Scholar]
- Griffin, D.; Shaw, P.; Stacey, R. Speaking of Complexity in Management Theory and Practice. Organ. Chaos Complex. 1998, 5, 315–339. [Google Scholar] [CrossRef]
- Schwaninger, M. Intelligent Organizations: Powerful Models for Systemic Management, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Allen, P.; Maguire, S.; McKelvey, B. The SAGE Handbook of Complexity and Management; SAGE: London, UK, 2011. [Google Scholar]
- Stacey, R.D. Strategic Management and Organisational Dynamics the Challenge of Complexity to Ways of Thinking about Organisations; Financial Times Prentice Hall: Harlow, UK, 2011. [Google Scholar]
- Jackson, M.C. Critical Systems Thinking and the Management of Complexity; Wiley: Chichester, UK, 2019. [Google Scholar]
- Beer, S. The Brain of the Firm; Wiley: Chichester, UK, 1981. [Google Scholar]
- Weber, M.; Schwaninger, M. Transforming an Agricultural Trade Organization: A System-Dynamics-Based Intervention. Syst. Dyn. Rev. 2002, 18, 381–401. [Google Scholar] [CrossRef]
- Beer, S. The Viable System Model: Its Provenance, Development, Methodology and Pathology. J. Oper. Res. Soc. 1984, 35, 7–25. [Google Scholar] [CrossRef]
- Forrester, J.W. Industrial Dynamics; MIT Press: Cambridge, MA, USA, 1961. [Google Scholar]
- Forrester, J.W. Principles of Systems; Pegasus Communications: Waltham, MA, USA, 1968. [Google Scholar]
- Forrester, J.W. Counterintuitive Behavior of Social Systems. Technol. Rev. 1971, 73, 52–68. [Google Scholar]
- Sterman, J.D. Business Dynamics. In Systems Thinking and Modeling for a Complex World; Irwin/Mc Graw-Hill: Boston, MA, USA, 2000. [Google Scholar]
- Schwaninger, M. Integrative Systems Methodology: Heuristic for Requisite Variety. Int. Trans. Oper. Res. 1997, 4, 109–123. [Google Scholar] [CrossRef]
- Espejo, R. Management of Complexity in Problem Solving. In Organizational Fitness: Corporate Fitness through Management Cybernetics; Espejo, R., Schwaninger, M., Eds.; Campus Frankfurt: New York, NY, USA, 1993; pp. 67–92. [Google Scholar]
- Espejo, R.; Reyes, A. Organizational Systems. In Managing Complexity with the Viable System Model; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Pettigrew, A.M. The Awakening Giant: Continuity and Change in Imperial Chemical Industries; Blackwell: Oxford, UK, 1985. [Google Scholar]
- Gomez, P.; Probst, G.J.B. Vernetztes Denken im Management; Die Orientierung (89); Schweizerische Volksbank: Bern, Switzerland, 1987. [Google Scholar]
- Christopher, W.F. Holistic Management: Managing What Matters for Company Success; Wiley: Hoboken, NJ, USA, 2007. [Google Scholar]
- Espinosa, A. Sustainable Self-Governance in Businesses and Society: The Viable System Model in Action; Francis & Taylor, Routledge: London, UK, 2023. [Google Scholar]
- Schwaninger, M.; Pérez Ríos, J. System dynamics and cybernetics: A synergetic pair. Syst. Dyn. Rev. 2008, 24, 145–174. [Google Scholar] [CrossRef]
- Schwaninger, M.; Klocker, J. Systemic Development of Health organizations: An Integrative Systems Methodology. In Innovative Health Systems for the 21st Century; Qudrat-Ullah, H., Tsasis, P., Eds.; Springer International: Cham, Switzerland; Wiley: Chichester, UK, 2017. [Google Scholar]
- Schwaninger, M.; Klocker, J. Efficiency versus Effectiveness in Hospitals: A Dynamic Simulation Approach. In Outcome-Based Performance Management in the Public Sector; Borgonovi, E., Anessi Pessina, E., Bianchi, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Senge, P.M. The Fifth Discipline. In The Art and Practice of the Learning Organization; Century Business: London, UK, 1990. [Google Scholar]
- Richardson, G. Problems in Causal Loop Diagrams Revisited. Syst. Dyn. Rev. 1997, 13, 247–252. [Google Scholar] [CrossRef]
- Schwaninger, M.; Scheef, C. Testing the Viable System Model. Theoretical Claim versus Empirical Evidence. Cybern. Syst. 2016, 47, 544–569. [Google Scholar] [CrossRef]
- Crisan Tran, C.I. Beers Viable System Model und die Lebensfähigkeit von Jungunternehmen: Eine Empirische Untersuchung. Ph.D. Dissertation, University of St. Gallen, St. Gallen, Switzerland, 2006. No. 3201. [Google Scholar]
- Malik, F. Strategie des Managements Komplexer Systeme ein Beitrag zur Management-Kybernetik Evolutionärer Systeme; Haupt: Bern, Switzerland, 1989. [Google Scholar]
- Clemson, B. Cybernetics: A New Management Tool; Abacus: Turnbridge Wells, UK, 1984. [Google Scholar]
- Hoverstadt, P. The Fractal Organization. In Creating Sustainable Organizations with the Viable System Model; Wiley: Chichester, UK, 2008. [Google Scholar]
- Pérez Ríos, J. Design and Diagnosis for Sustainable Organizations: The Viable System Method; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Lassl, W. The Viability of Organizations; Springer: Berlin/Heidelberg, Germany, 2019/20; Volumes 1–3.
- Pfiffner, M. The Neurology of Business: Implementing the Viable System Model; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Erbsen, A. Krankheit im Zentrum Gestaltung von Krankheitsorientierten Spitalstrukturen aus Kybernetisch-Konstruktivistischer Sicht; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2012. [Google Scholar]
- Luhmann, N. Social Systems; Stanford University Press: Stanford, CA, USA, 1995. [Google Scholar]
- Lipnack, J.; Stamps, J. Virtual Teams, 2nd ed.; Wiley: New York, NY, USA, 2000. [Google Scholar]
- Nonaka, I.; Takeuchi, H. The Knowledge-Creating Company; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- McCulloch, W. Embodiments of Mind; MIT Press: Cambridge, MA, USA, 1965; new edition 1988. [Google Scholar]
- Boos, F.; Mitterer, G. Einführung in Das Systemische Management; Carl-Auer-Systeme Verlag: Heidelberg, Germany, 2014. [Google Scholar]
- Ziegler, A.; Lange, S.; Bender, R. Überlebenszeitanalyse: Der Log-Rang Test. Dtsch. Med. Wochenschr. 2007, 132, e39–e41. [Google Scholar] [CrossRef] [PubMed]
- Birkinshaw, J.; Hamel, G.; Mol, M.J. Management Innovation. Acad. Manag. Rev. 2008, 33, 825–845. [Google Scholar] [CrossRef]
- Golden, S.L. Compromised Exactness and the Rationality of Engineering. In Social Systems Engineering; Garcia-Díaz, C., Olaya, C., Eds.; Wiley: Chichester, UK, 2017. [Google Scholar]
- Beer, S. Beyond Dispute. In The Invention of Team Syntegrity; Wiley: Chichester, UK, 1994. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interest Groups | Goals | Key Factors |
|---|---|---|
| Patients & their Families | Be healthy Suffer little | Prevention Quality of life Quality of care |
| Champions of Oncological Care | Be excellent professionals Have an interesting job Realize their ideas Lead an effective team | Motivation Research & knowledge management Strong infrastructure Cooperation Effective coordination |
| Local Hospitals and Doctors | Qualify in oncology Become members of care network | Training Cooperation |
| Professional Staff | Have an interesting job Have a bearable job Become more qualified | Training Psychohygiene Cooperativeness of other units involved |
| State Authorities & Central Hospital Administration | Effectiveness of care system Efficiency of care system | Low incidence of cancer Cancer prevention Success of care High productivity Coordination |
| Public in General | Stay healthy | Social & ecological consciousness Quality of environment Healthy behavior |
| Recursion w: Oncology Carinthia | Recursion x: Oncology Regions (e.g., Oncology Klagenfurt) | Recursion y: Oncology Stations (e.g., Tumor Ambulance) | |
|---|---|---|---|
| Basic Units | Oncology Klagenfurt Oncology Villach Oncology Wolfsberg Oncology in 6 further hospitals | Oncological Ambulance, Oncology ward at internal station. n Local practitioners with oncological competence | N Teams (Interaction Systems, including patient & family, physician & nursing) n Local practitioners with oncological competence |
| Component 1: Local Management | Heads of basic units: Oncologists | Heads of station: oncologists or intemists | Patient & family |
| Component 2: Coordination | Standard therapies, tumor database, training, oncology circle, doctors’ letters, electronic messaging and conferences | Tumor database, tumor boards and councils, coordination sessions (Radiotherapy1Hematology/Pathology), standard therapies, training, doctors’ letters | Tumor councils, Standard therapy plans, daily station meeting, nursing guidelines, coffee break |
| Component 3: Executive Management | Lead Team OCS (2 oncologists, 1 internist-oncologist, 1 radiologist-oncologist) | Management team/local leaders (physicians & nursing staff; 9 persons) | Station leaders (physicians and nursing staff in charge) |
| Channel between Components 1 to 3 | Allocation of time and OCS staff, Management by Objectives, Definition/negotiation Std. Therapies | Allocation of time and personnel, design/negotiation of therapy plans | Assignments/requests, participation |
| Component 3*: Audit Channel | Visits to local oncology units, phone calls, messaging, Special studies, inquiries, Tests informal communication, cultural events | Medical visits, phone calls, messaging. informal communication | Medical visits, continualcontact1 conversations with patients. informal communication |
| Component 4: Organizational/ Development/ Strategic Management | OCS leaders team, therapy and prevention strategies, ongoing research, congresses and symposia, networks, strategy workshops | Development plan, future-oriented education, management team, leaders OCS | Station development plan, future-oriented education, leaders of station, leaders OCS, head internal station |
| Component 5: System Ethos/ Normative Management | Ethos OCS- Values, principles, vision and mission, mission, management framework OCS, leaders OCS | Values, principles, vision and mission, ethos OCS, management framework OCS, local management team, leaders OCS | mission, ethos OCS, leaders of station, leaders OCS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwaninger, M.; Klocker, J. Applying Integrative Systems Methodology: The Case of Health Care Organizations. Systems 2024, 12, 140. https://doi.org/10.3390/systems12040140
Schwaninger M, Klocker J. Applying Integrative Systems Methodology: The Case of Health Care Organizations. Systems. 2024; 12(4):140. https://doi.org/10.3390/systems12040140
Chicago/Turabian StyleSchwaninger, Markus, and Johann Klocker. 2024. "Applying Integrative Systems Methodology: The Case of Health Care Organizations" Systems 12, no. 4: 140. https://doi.org/10.3390/systems12040140
APA StyleSchwaninger, M., & Klocker, J. (2024). Applying Integrative Systems Methodology: The Case of Health Care Organizations. Systems, 12(4), 140. https://doi.org/10.3390/systems12040140