
Social Determinants of Health Influencing the New Zealand COVID-19 Response and Recovery: A Scoping Review and Causal Loop Diagram


Abstract
:1. Introduction
2. Materials and Methods
2.1. Defining the Research Questions
2.2. Identifying and Selecting Relevant Literature
2.3. Analyzing the Data
2.4. Summarizing through Causal Loop Diagram
3. Results
3.1. Characteristics of the Literature
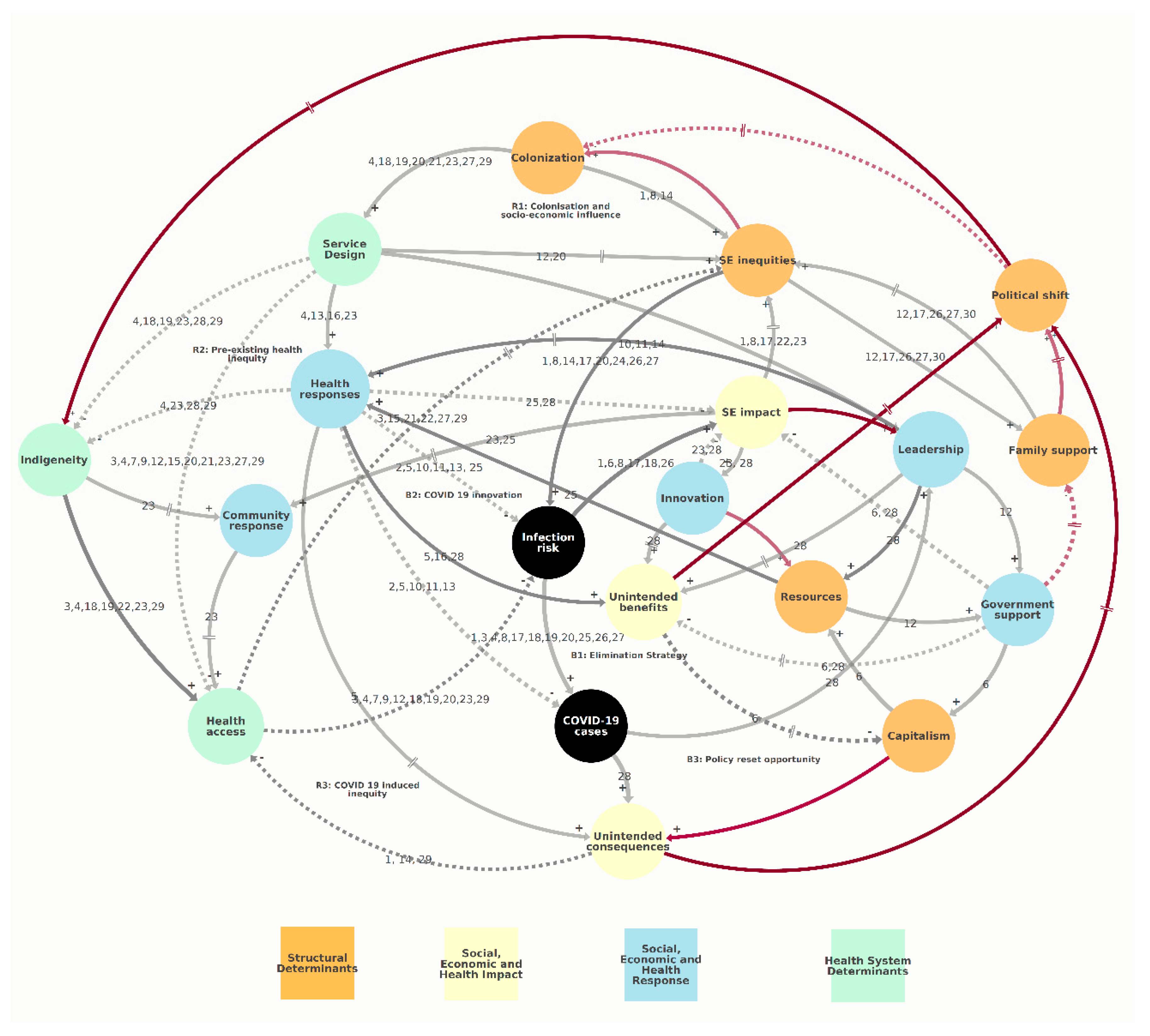
3.2. Causal Loop Diagram
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Benefits | Unintended benefits (e.g., policy reset opportunities) |
| Capitalism | Capitalism-based development |
| Cases | COVID-19 cases |
| Colonization | Colonization and structural racism |
| Community response | Collective community response |
| Consequences | Unintended consequences (e.g., biodiversity loss, mental health) |
| Family support | Families needing social support |
| Govt support | Government economic support |
| Health access | Equitable access to health services |
| Health response | COVID-19 health responses (e.g., lockdown, border shutdown) |
| Indigeneity | Indigenous knowledge utilization |
| Infection risk | Infection risk among at risk groups |
| Innovation | Job and service delivery innovation |
| Leadership | Pandemic decision-making and leadership |
| Resources | Resources for the health and social response |
| SE impact | Socio-economic impact |
| SE inequities | Socio-economic inequities |
| Service design | Design of health and social services based on colonial/western worldview |
References
- Jefferies, S.; French, N.; Gilkison, C.; Graham, G.; Hope, V.; Marshall, J.; McElnay, C.; McNeill, A.; Muellner, P.; Paine, S.; et al. COVID-19 in New Zealand and the impact of the national response: A descriptive epidemiological study. Lancet Public Health 2020, 5, e612–e623. [Google Scholar] [CrossRef]
- Solar, O.; Irwin, A. A Conceptual Framework for Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Hawe, P. The social determinants of health: How can a radical agenda be mainstreamed? Can. J. Public Health 2009, 100, 291–293. [Google Scholar] [CrossRef] [PubMed]
- National Health Committee. The Social, Cultural and Economic Determinants of Health in New Zealand: Action to Improve Health; National Health Committee: Wellington, New Zealand, 1998.
- Karanikolos, M.; Heino, P.; McKee, M.; Stuckler, D.; Legido-Quigley, H. Effects of the Global Financial Crisis on Health in High-Income Oecd Countries: A Narrative Review. Int. J. Health Serv. 2016, 46, 208–240. [Google Scholar] [CrossRef] [PubMed]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Fink, D.S.; Keyes, K.M.; Cerdá, M. Systems Science and the Social Determinants of Population Health. In Systems Science and Population Health; El-Sayed, A.M., Galea, S., Eds.; Oxford University Press: New York, NY, USA, 2017; pp. 140–149. [Google Scholar]
- Baker, M.G.; Barnard, L.T.; Kvalsvig, A.; Verrall, A.; Zhang, J.; Keall, M.; Wilson, N.; Wall, T.; Howden-Chapman, P. Increasing incidence of serious infectious diseases and inequalities in New Zealand: A national epidemiological study. Lancet 2012, 379, 1112–1119. [Google Scholar] [CrossRef]
- Health Quality and Safety Commission. A Window on the Quality of Aotearoa New Zealand’s Health Care 2019; Health Quality and Safety Commission: Wellington, New Zealand, 2019. [Google Scholar]
- Gurney, J.; Stanley, J.; McLeod, M.; Koea, J.; Jackson, C.; Sarfati, D. Disparities in Cancer-Specific Survival Between Māori and Non-Māori New Zealanders, 2007–2016. JCO Glob. Oncol. 2020, 6, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Waitangi Tribunal. Hauora: Report on Stage on of the Health Services and Outcomes Kaupapa Inquiry; Waitangi Tribunal: Wellington, New Zealand, 2019. [Google Scholar]
- Ministry of Health. Achieving Equity in Health Outcomes: Highlights of Selected Papers; Ministry of Health: Wellington, New Zealand, 2018.
- Ministry of Health. Health Loss in New Zealand 1990–2013: A Report from the New Zealand Burden of Diseases, Injuries and Risk Factors Study; Ministry of Health: Wellington, New Zealand, 2016.
- New Zealand Health and Disability System Review. Health and Disability System Review—Final Report Pūrongo Whakamutunga; Health and Disability System Review: Wellington, New Zealand, 2020.
- Steyn, N.; Binny, R.N.; Hannah, K.; Hendy, S.C.; James, A.; Kukutai, T.; Lustig, A.; McLeod, M.; Plank, M.J.; Ridings, K.; et al. Estimated Inequities in COVID-19 Infection Fatality Rates by Ethnicity for Aotearoa New Zealand. Medrxiv 2020. [Google Scholar] [CrossRef]
- Anderson, D.; Cominick, C.; Langley, E.; Painuthara, K.; Palmer, S. Rapid Evidence Review: The Immediate and Medium-Term Social and Psycho-Social Impacts of COVID-19 in New Zealand; Ministry of Social Development: Wellington, New Zealand, 2020.
- McMeeking, S.; Savage, C. Māori responses to Covid-19. Policy Q. 2020, 16, 36–41. [Google Scholar] [CrossRef]
- Azar, K.M.J.; Shen, Z.; Romanelli, R.J.; Lockhart, S.H.; Smits, K.; Robinson, S.; Brown, S.; Pressman, A.R. Disparities In Outcomes Among COVID-19 Patients In A Large Health Care System In California. Health Aff. (Millwood) 2020, 39, 1253–1262. [Google Scholar] [CrossRef]
- Furlong, Y.; Finnie, T. Culture counts: The diverse effects of culture and society on mental health amidst COVID-19 outbreak in Australia. Ir. J. Psychol. Med. 2020, 37, 1–6. [Google Scholar] [CrossRef]
- St Denis, X. Sociodemographic Determinants of Occupational Risks of Exposure to COVID-19 in Canada. Can. Rev. Soc. 2020, 57, 399–452. [Google Scholar] [CrossRef]
- Yashadhana, A.; Pollard-Wharton, N.; Zwi, A.B.; Biles, B. Indigenous Australians at increased risk of COVID-19 due to existing health and socioeconomic inequities. Lancet Reg. Health West. Pac. 2020, 1, 100007. [Google Scholar] [CrossRef]
- Abrams, E.M.; Szefler, S.J. COVID-19 and the impact of social determinants of health. Lancet Respir. Med. 2020, 8, 659–661. [Google Scholar] [CrossRef]
- Hawkins, D. Social Determinants of COVID-19 in Massachusetts, United States: An Ecological Study. J. Prev. Med. Public Health 2020, 53, 220–227. [Google Scholar] [CrossRef]
- Kvalsvig, A.; Baker, M.G. How Aotearoa New Zealand rapidly revised its Covid-19 response strategy: Lessons for the next pandemic plan. J. R. Soc. N. Z. 2021, 51, S143–S166. [Google Scholar] [CrossRef]
- Te Hiringa Hauora/Health Promotion Agency. Post-Lockdown Survey—The Impact on Health Risk Behaviours; Health Promotion Agency: Wellington, New Zealand, 2020. [Google Scholar]
- Barber, P.; Tanielu, R.; Ika, A. State of the Nation 2021; Salvation Army Social Policy and Parliamentary Unit: Wellington, New Zealand, 2021. [Google Scholar]
- Humpage, L.; Neuwelt-Kearns, C. Income Support in the Wake of COVID-19: Survey; The University of Auckland, Child Poverty Action Group, Acukland Action Against Poverty, First Union: Auckland, New Zealand, 2020. [Google Scholar]
- Huang, Q.S.; Wood, T.; Jelley, L.; Jennings, T.; Jefferies, S.; Daniells, K.; Nesdale, A.; Dowell, T.; Turner, N.; Campbell-Stokes, P.; et al. Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat. Commun. 2021, 12, 1–7. [Google Scholar] [CrossRef]
- Manuirirangi, K.; Jarman, J. The Taranaki COVID-19 repsonse from a Maori perspective: Lessons for mainstream health providers in Aotearoa New Zealand. N. Z. Med. J. 2021, 134, 122–124. [Google Scholar] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Sterman, J. Business Dynamics: Systems Thinking and Modeling for a Complex World; Irwin/McGraw-Hill: Boston, MA, USA, 2000; Volume 19. [Google Scholar]
- Wolstenholme, E.F.; Coyle, R.G. The Development of System Dynamics as a Methodology for System Description and Qualitative Analysis. J. Oper. Res. Soc. 1983, 34, 569–581. [Google Scholar] [CrossRef]
- Coyle, G. Qualitative modelling in system dynamics. In A Keynote Address to the Conference of the System Dynamics Society; System Dynamics Society: Wellington, New Zealand, 1999. [Google Scholar]
- Muttalib, F.; Ballard, E.; Langton, J.; Malone, S.; Fonseca, Y.; Hansmann, A.; Remy, K.; Hovmand, P.; Doctor, A. Application of systems dynamics and group model building to identify barriers and facilitators to acute care delivery in a resource limited setting. BMC Health Serv. Res. 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Al-Busaidi, I.S.; Martin, M. Provision of primary care in managed isolation and quarantine facilities during the COVID-19 pandemic: Lessons learned from Christchurch, New Zealand. N. Z. Med. J. 2020, 133, 130–132. [Google Scholar]
- Arnold, R.H.; Tideman, P.A.; Devlin, G.P.; Carroll, G.E.; Elder, A.; Lowe, H.; Macdonald, P.S.; Bannon, P.G.; Juergens, C.; McGuire, M.; et al. Rural and Remote Cardiology During the COVID-19 Pandemic: Cardiac Society of Australia and New Zealand (CSANZ) Consensus Statement. Heart Lung Circ. 2020, 29, e88–e93. [Google Scholar] [CrossRef]
- Bandyopadhyay, G.; Meltzer, A. Let us unite against COVID-19—A New Zealand perspective. Ir. J. Psychol. Med. 2020, 37, 218–221. [Google Scholar] [CrossRef]
- Boston, J. Transforming the economy: Why a ‘green recovery’ from Covid-19 is vital. Policy Q. 2020, 16, 61–66. [Google Scholar] [CrossRef]
- Carr, A. COVID-19, indigenous peoples and tourism: A view from New Zealand. Tour. Geogr. 2020, 22, 491–502. [Google Scholar] [CrossRef]
- Ministry of Education. Education Report: COVID-19 Response-Distance Learning Package; Ministry of Education: Wellington, New Zealand, 2020.
- Fletcher, M. Government’s income support responses to the Covid-19 pandemic. Policy Q. 2020, 16, 73–78. [Google Scholar] [CrossRef]
- Foley, D.A.; Kirk, M.; Jepp, C.; Brophy-Williams, S.; Tong, S.Y.C.; Davis, J.S.; Blyth, C.C.; O’Brien, M.P.; Bowen, A.C.; Yeoh, D.K. COVID-19 and paediatric health services: A survey of paediatric physicians in Australia and New Zealand. J. Paediatr. Child Health 2020, 56, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Galea-Singer, S.; Newcombe, D.; Farnsworth-Grodd, V.; Sheridan, J.; Adams, P.; Walker, N. Challenges of virtual talking therapies for substance misuse in New Zealand during the COVID-19 pandemic: An opinion piece. N. Z. Med. J. 2020, 133, 104–111. [Google Scholar]
- Hamill, J.K.; Sawyer, M.C. Reduction of childhood trauma during the COVID-19 Level 4 lockdown in New Zealand. ANZ J. Surg. 2020, 90, 1242–1243. [Google Scholar] [CrossRef]
- Kokaua, S. Giving Metua Va’ine Moana Opportunities to ‘Create Something Big’; Ministry of Women: Wellington, New Zealand, 2020.
- SocialLink. The Impact of COVID-19 on New Zealand Communities and the Social Sector: A Summary of Issues from Survey Findings; SocialLink: Wellington, New Zealand, 2020. [Google Scholar]
- Wilson, N.; Boyd, M.; Kvalsvig, A.; Chambers, T.; Baker, M. Public health aspects of the Covid-19 response and opportunities for the post-pandemic era. Policy Q. 2020, 16, 20–24. [Google Scholar] [CrossRef]
- Crotty, F.; Watson, R.; Lim, W.K. Nursing homes: The titanic of cruise ships—Will residential aged care facilities survive the coronavirus disease 2019 pandemic? Intern. Med. J. 2020, 50, 1033–1036. [Google Scholar] [CrossRef]
- Béland, D.; Marier, P. COVID-19 and Long-Term Care Policy for Older People in Canada. J. Aging Soc. Policy 2020, 32, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Laster Pirtle, W.N. Racial Capitalism: A Fundamental Cause of Novel Coronavirus (COVID-19) Pandemic Inequities in the United States. Health Educ. Behav. 2020, 47, 504–508. [Google Scholar] [CrossRef]
- Laurencin, C.T.; McClinton, A. The COVID-19 Pandemic: A Call to Action to Identify and Address Racial and Ethnic Disparities. J. Racial Ethn. Health Disparities 2020, 7, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Levin, J. The Faith Community and the SARS-CoV-2 Outbreak: Part of the Problem or Part of the Solution? J. Relig. Health 2020, 59, 2215–2228. [Google Scholar] [CrossRef] [PubMed]
- Doogan, C.; Buntine, W.; Linger, H.; Brunt, S. Public Perceptions and Attitudes Towards COVID-19 Non-Pharmaceutical Interventions Across Six Countries: A Topic Modeling Analysis of Twitter Data. J. Med. Internet Res. 2020, 22, e21419. [Google Scholar] [CrossRef]
- Fitzgerald, D.A.; Wong, G.W.K. COVID-19: A tale of two pandemics across the Asia Pacific region. Paediatr. Respir. Rev. 2020, 35, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Júnior, J.G.; Moreira, M.M.; Pinheiro, W.R.; de Amorim, L.M.; Lima, C.K.T.; da Silva, C.G.L.; Neto, M.L.R. The mental health of those whose rights have been taken away: An essay on the mental health of indigenous peoples in the face of the 2019 Coronavirus (2019-nCoV) outbreak. Psychiatry Res. 2020, 289, 113094. [Google Scholar] [CrossRef]
- Bradley, D.T.; Mansouri, M.A.; Kee, F.; Garcia, L.M.T. A systems approach to preventing and responding to COVID-19. EClinicalMedicine 2020, 21, 100325. [Google Scholar] [CrossRef] [Green Version]
- Carey, G.; Malbon, E.; Carey, N.; Joyce, A.; Crammond, B.; Carey, A. Systems science and systems thinking for public health: A systematic review of the field. BMJ Open 2015, 5, e009002. [Google Scholar] [CrossRef] [PubMed]
- Sahin, O.; Salim, H.; Suprum, E.; Richards, R.; MacAskill, S.; Heilgeist, S.; Rutherford, S.; Stewart, R.A.; Beal, C.D. Developing a Preliminary Causal Loop Diagram for Understanding the Wicked Complexity of the COVID-19 Pandemic. Systems 2020, 8, 20. [Google Scholar] [CrossRef]
- Jalali, M.S.; Sharafi-Avarzaman, Z.; Rahmandad, H.; Ammerman, A.S. Social influence in childhood obesity interventions: A systematic review. Obes. Rev. 2016, 17, 820–832. [Google Scholar] [CrossRef]
- Cockerham, W.C. Health Lifestyle Theory and the Convergence of Agency and Structure. J. Health Soc. Behav. 2005, 46, 51–67. [Google Scholar] [CrossRef] [Green Version]
- Bump, J.B.; Baum, F.; Sakornsin, M.; Yates, R.; Hofman, K. Political economy of covid-19: Extractive, regressive, competitive. BMJ 2021, 372, n73. [Google Scholar] [CrossRef]
- Welfare Expert Advisory Group. Whakamana Tangata: Restoring Dignity to Social Security in New Zealand; Welfare Expert Advisory Group: Wellington, New Zealand, 2019. [Google Scholar]
- Tokalau, T. Covid-19: Not Prioritising Caccine Rollout Plan by Ethnicity is Unfair, Experts Say. 2021. Available online: https://www.stuff.co.nz/pou-tiaki/124519579/covid19-not-prioritising-vaccine-rollout-plan-by-ethnicity-is-unfair-experts-say (accessed on 10 May 2020).
- Meadows, D.H.; Wright, D.E. Thinking in Systems: A Primer; Chelsea Green: White River Junction, VT, USA, 2008.
- Johnston, L.M.; Matteson, C.L.; Finegood, D.T. Systems Science and Obesity Policy: A Novel Framework for Analyzing and Rethinking Population-Level Planning. Am. J. Public Health 2014, 104, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Carey, G.; Crammond, B. Systems change for the social determinants of health. BMC Public Health 2015, 15, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senge, P.; Hamilton, H.; Kania, J. The dawn of system leadership. Standford Soc. Innov. Rev. 2015, 13, 27–33. [Google Scholar]
- Matheson, A.; Watene, K.; Vujnovich, G.; Mackey, T. Collective Impact: Shining the Light on Community Post Covid-19. 2020. Available online: https://thespinoff.co.nz/partner/te-punaha-matatini/27-08-2020/collective-impact-shining-the-light-on-community-post-covid-19/ (accessed on 10 May 2021).
- Loane, J.; Percival, T.; Laban, W.; Lambie, I. All-of-community by all-of-government: Reaching Pacific peopel in Aotearoa New Zealand during the COVID-19 pandemic. N. Z. Med. J. 2021, 134, 96–103. [Google Scholar]


{kind=link}
| ID | Paper | Focus Country | Social Determinants of Health | Model Variables and Connections |
|---|---|---|---|---|
| 1 | Abrams et al. | US | Poverty, homelessness, housing, ethnicity, smoking, pre-existing health conditions, physical distancing, COVID-19 morbidity, socio-economic impact | Colonization—SE inequities; SE inequities—Infection risk—Cases—SE impact—SE inequities; Consequences—Health access |
| 2 | Al-Bausaidi et al. | New Zealand | NZ lockdown, quarantine requirements, pre-existing health conditions, digital divide, primary care services, access to medicines | Health response—Cases; Health response—Infection risk |
| 3 | Arnold et al. | Australia and New Zealand | Age, indigenous people, rural, pre-existing conditions, COVID-19 morbidity, primary care services, resource management | Health access—Infection risk—Cases; Health access—SE inequities; Service design—Health access |
| 4 | Azar et al. | US | Racism, health service user experience, health seeking behavior, COVID-19 infection, COVID-19 hospitalization rate | Colonization—Services design—Health response/Indigeneity/Health access—Infection risk—Cases |
| 5 | Bandyopadhyay et al. | New Zealand | NZ pandemic response; mental stress; community cohesion; | Health responses—Benefits/Consequences/Cases |
| 6 | Boston | New Zealand | Linear economy; ecological crisis; policy reset opportunity; circular economy; NZ/global pandemic responses; fiscal recovery packages | Infection risk—SE impact; Govt support—SE impact/Capitalism/Benefits—Capitalism |
| 7 | Beland et al. | Canada | Canada federal & provincial health system; underfunding/low priority; aged care facilities; staffing, processes; age; COVID-19 morbidity | Service design—Health access—Infection risk |
| 8 | Carr | New Zealand | Tourism; indigenous businesses, racism, colonization, socio-economic status/impact, travel restrictions | Colonization—SE inequities—Infection risk—SE impact—SE inequities; Infection risk—Cases |
| 9 | Crotty et al. | Australia | Australia health care system; policy and funding settings; aged care facilities; staffing, processes; older age. vulnerable people; high morbidity | Service design—Health access—Infection risk |
| 10 | Doogan et al. | Global | Political leadership; information & communication; country pandemic response measures; compliance rate; emotional appeal | Leadership—Health response—Cases/Infection risk |
| 11 | Fitzgerald et al. | Global | Young age; morbidity; preparedness; centralized response; compliance rate; virus containment; prevention measures | Leadership—Health response—Cases/Infection risk |
| 12 | Fletcher | New Zealand | Poverty; welfare policies; inequalities; access; COVID-19 risk | SE inequities—Family support—SE inequities; Service design—SE inequities/Health access—Infection risk |
| 13 | Foley et al. | Australia and New Zealand | Young age; health needs; pediatric physicians; information; leadership; health system capacity/resilience; preparedness for pandemics | Service design—Health response—Infection risk/Cases |
| 14 | Furlong et al. | Australia | Structural, historical racism and colonization; Asian population discrimination; social capital and harmony; indigenous people; culture; economic and social disadvantage; co-existing health conditions; rural location; tobacco consumption; mental health resilience | Colonization—SE inequities—Infection risk; Leadership—Health response; Consequences—Health access |
| 15 | Galea-Singer et al. | New Zealand | Physical distancing; substance misuse therapy; virtual therapy clinics; research gaps | Service design—Health access—SE inequities |
| 16 | Hamill et al. | New Zealand | WHO declaration; global response; NZ response; lockdown and travel restriction; accidents and trauma rate among children | Health response—Benefits |
| 17 | Hawkins | US | Poverty; racism; vulnerability; occupational status; essential worker; job security and entitlements, at risk groups; poverty cycle | SE inequities—Family support—SE inequities; SE inequities—Infection risk—SE impact—SE inequities; Infection risk—Cases |
| 18 | Junior et al. | Global | Rural location; socio-economic condition, colonization and historical trauma; Western intervention; access to mental health services; information; health workers limited availability; indigenous mental health status and access to services; reinforcing vulnerability | Colonization—Service design—indigeneity—Health access—Infection risk—SE Impact/Cases |
| 19 | Kokaua | New Zealand | Race/ethnicity; vulnerability; COVID-19 advocacy; society development; systemic bias; cultural measures; inequity in health sector | Colonization—Service design—indigeneity—Health access—Infection risk—Cases |
| 20 | Laster Pirtle | US | Structural racism; historical trauma; socio-economic disadvantage; racial capitalism; health inequity; COVID-19 risk and vulnerability | Colonization—Service design—Health access/SE inequities—Infection risk—Cases |
| 21 | Laurencin et al. | US | Historical racism, poverty, crowded housing, limited data, misinformation; pre-existing social & health inequity; limited access; design of health system; disproportionate impact on disadvantaged groups | Colonization—Service design—Health access—SE inequities |
| 22 | Levin | US | Faith and religion context; scientific divide; trust; misinformation; COVID cases; faith based medical centers; collaboration and coordination with religious agencies | Indigeneity—Health access—SE inequities—SE impact |
| 23 | McMeeking et al. | New Zealand | Structural racism; historical inequity; underlying health conditions; Māori collective and cultural capital; government response; Māori empowerment and ownership; trust; access to services and information; at risk population; socio-economic status | Colonization—Service design—Indigeneity/Health access/Health response—Indigeneity—Community response/Health access—Infection risk; SE impact—SE inequities; SE impact—Innovation—SE impact; SE impact—Community response—Health access |
| 24 | Ministry of Education | New Zealand | Essential workers, low-income bracket; sick leave and flexibility at work; vulnerable age; ability to work from home; gender and essential work; socio-economic impact | SE inequities—Infection risk |
| 25 | SocialLink | New Zealand | Lockdown and travel restrictions; social services disruption; extra workload; increased travel expenses; effect on fundraising; Impact on livelihood and mental health; violence against women and children; | Health response—Resources/Infection risk/SE impact—Community response |
| 26 | St-Denis | Canada | Age; gender; essential work status; education status; poverty status; risk of COVID, reinforcing socio-economic condition | SE inequities—Family support—SE inequities; SE inequities—Infection risk—SE impact/Cases |
| 27 | Steyn et al. | New Zealand | Age; race/ethnicity; socio-economic status; structural racism; crowded living spaces; access to health services; rural location; at risk group; COVID cases | SE inequities—Family support—SE inequities; SE inequities—Infection risk—Cases; Colonization—Service design—Health access—SE inequities |
| 28 | Wilson et al. | New Zealand | Design of health system and infrastructure; health system gaps, preparedness; pre-existing inequities; health protection workforce; pandemic response strategies; precautionary principles; unintended benefits; socio-economic impact; infection rate; green reset opportunities; reduction in related harms | Service design—Indigeneity/Health response—Indigeneity; Health response—SE impact; Health response—Benefits; Leadership—Benefits/Resources; Cases—Leadership/Consequences; Govt support—SE impact/Benefits |
| 29 | Yashadhana et al. | Australia | Structural racism; health status, inequities; access to and design of health services; socio-economic status; trust; utilisation; funding of indigenous services; at risk group; COVID-19 cases | Colonization—Service design—Health access/Indigeneity/Health response—Indigeneity—Health access—SE impact/Infection risk; Consequences—Health access |
| 30 | Anderson et al. | New Zealand | Pre-existing social conditions; violence; poverty; young age; pandemic responses; child development; employment status; pre-existing social conditions | SE inequities—Family support—SE inequities; |
| ID | Name | Type | Causal Loop/s in the Model |
|---|---|---|---|
| R1 | Colonization and socio-economic influence | Reinforcing loops | Colonization → Service design → SE inequities (→ Family support) → Colonization |
| R2 | Pre-existing health inequity | Reinforcing loops | Colonization → Service design (→− Indigeneity →) →− Health access →− SE inequities → Colonization |
| R3 | COVID-19 induced inequity | Reinforcing loops | Health access (→− SE inequities →) →− Infection risk (→ SE impact → SE inequities) → COVID-19 cases→ Unintended consequences →− Health access |
| B1 | Elimination Strategy | Balancing loops | COVID-19 cases → Leadership → Health response (→− Infection risk →) →− COVID-19 cases SE Impact → Leadership → Resources (→ Health responses →− Infection risk → SE impact) → Government support →− SE impact |
| B2 | COVID-19 innovation | Balancing loops | Health access (→− SE inequities →) →−Infection risk → SE impact (→ Innovation →−) → Community response → Health access |
| B3 | Policy reset opportunity | Balancing loops | Infection risk → SE impact → Leadership (→ Resources) → Health response → Unintended benefits → Political shift → Indigeneity → Health access (→− SE inequities →) →− Infection risk Infection risk → SE impact → Leadership (→ Resources) → Health response → Unintended benefits →− Capitalism→ Unintended consequences→− Health access (→− SE inequities →) →− Infection risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, S.; Walton, M.; Manning, S. Social Determinants of Health Influencing the New Zealand COVID-19 Response and Recovery: A Scoping Review and Causal Loop Diagram. Systems 2021, 9, 52. https://doi.org/10.3390/systems9030052
Sharma S, Walton M, Manning S. Social Determinants of Health Influencing the New Zealand COVID-19 Response and Recovery: A Scoping Review and Causal Loop Diagram. Systems. 2021; 9(3):52. https://doi.org/10.3390/systems9030052
Chicago/Turabian StyleSharma, Sudesh, Mat Walton, and Suzanne Manning. 2021. "Social Determinants of Health Influencing the New Zealand COVID-19 Response and Recovery: A Scoping Review and Causal Loop Diagram" Systems 9, no. 3: 52. https://doi.org/10.3390/systems9030052
APA StyleSharma, S., Walton, M., & Manning, S. (2021). Social Determinants of Health Influencing the New Zealand COVID-19 Response and Recovery: A Scoping Review and Causal Loop Diagram. Systems, 9(3), 52. https://doi.org/10.3390/systems9030052