
An Extended Semantic Interoperability Model for Distributed Electronic Health Record Based on Fuzzy Ontology Semantics




Abstract
:1. Introduction
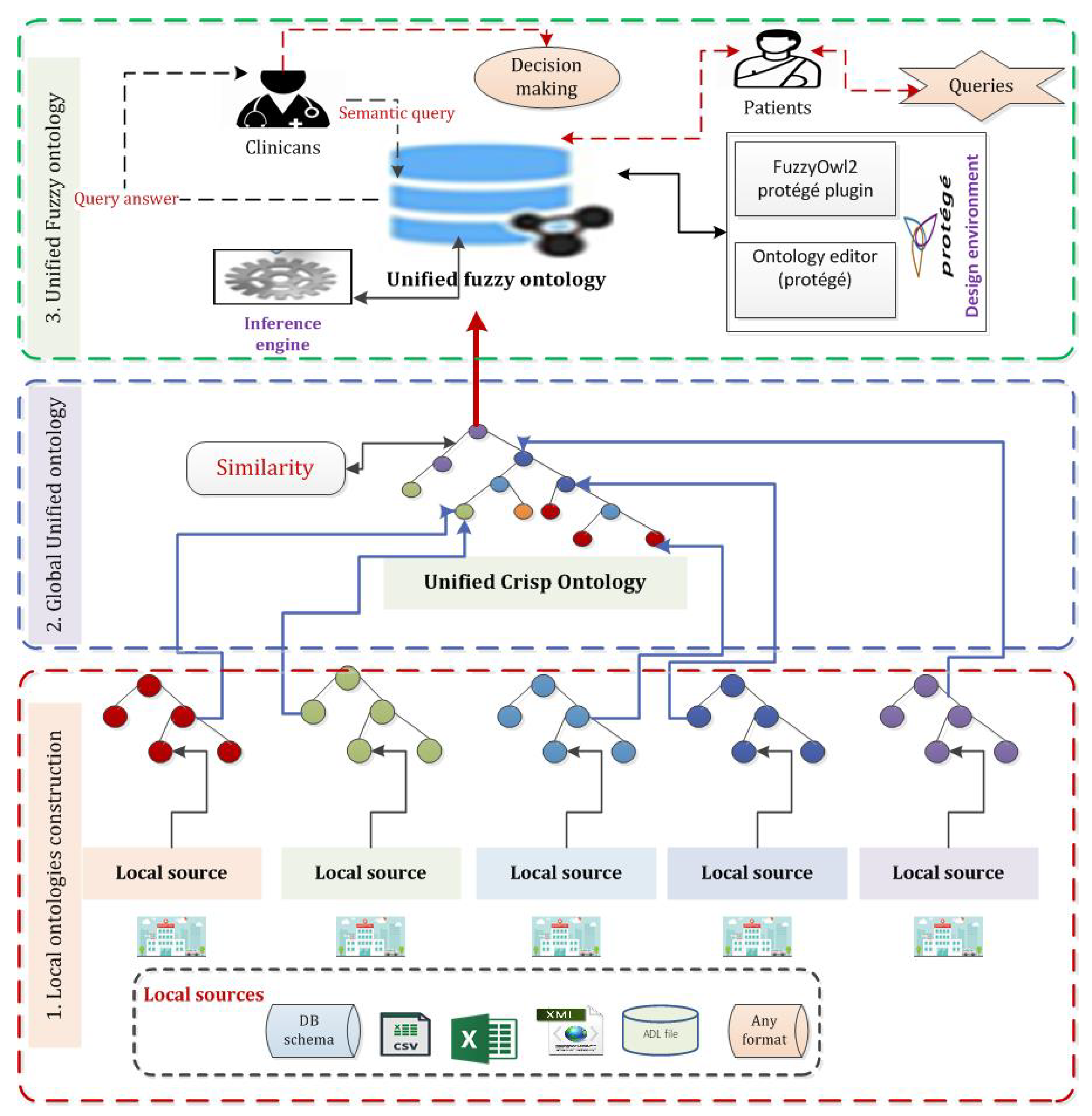
- Propose a framework that could integrate and collect all patient data from distributed and heterogeneous data sources in a centralized point based on using semantic web ontologies.
- Achieve syntax interoperability in distributed EHRs by aggregating data with heterogeneous structures. That aggregating and integration were done using the ontology semantic web concept.
- Achieve SI in distributed EHRs by fuzzing the united crisp ontology. We made unification between different heterogeneous formats using crisp ontology. FO could address semantic meaning for any inconsistent feature by using linguistic terms. For example, it is popular to utilize translation between people who are not from the same country and do not speak a similar language.
2. Related Work
2.1. Ontology-Based Interoperable Frameworks
2.2. Fuzzy-Based Ontology Systems
3. Materials and Methods
3.1. Fuzzy-Ontology Formulation
- Individual names a to domain elements aI ∈ I,
- Class names C to a set of domain elements CI ⊑ I,
- Role R to a set of pair of domain elements RI ⊑ I × I.
- ⊤I = I and ⊥I = ,
- (¬A) = I/AI,
- (C ⊓ D)I = CI∩ DI and (C ⊔ D)I = CI ∪ DI,
- (∀R.C)I = {a ∈ I ∣∀b.(a,b) ∈ RI ⟶ b ∈ CI},
- (∃R.⊤)I = {a ∈ I ∣∃b.(a,b) ∈ RI}.
- I ⊧ (t ≥ ) iff tI ≥ ,
- I ⊧ (trans R) iff ∀x,y∈ΔI, RI(x, y) ≥ supz∈ΔI RI(x, z) ⊕ RI (z, y),
- I ⊧ R1 ⊑ R2 iff ∀(x, z) ∈ I (z, y) ≤ (z, y),
- I(inv R1 R2) iff ∀(x, z) ∈ I (z, y) = (z, y).
3.2. Dataset Sources
3.2.1. Data Source #1: MIMIC-III CSV Format
3.2.2. Data Source #2: MIMIC-III MySQL Adapted Database
3.2.3. Data Source #3: Semantic openEHR Archetypes
3.3. The Proposed Architecture Model
| Algorithm 1: Fuzzy ontology preparation. |
 |
4. Results
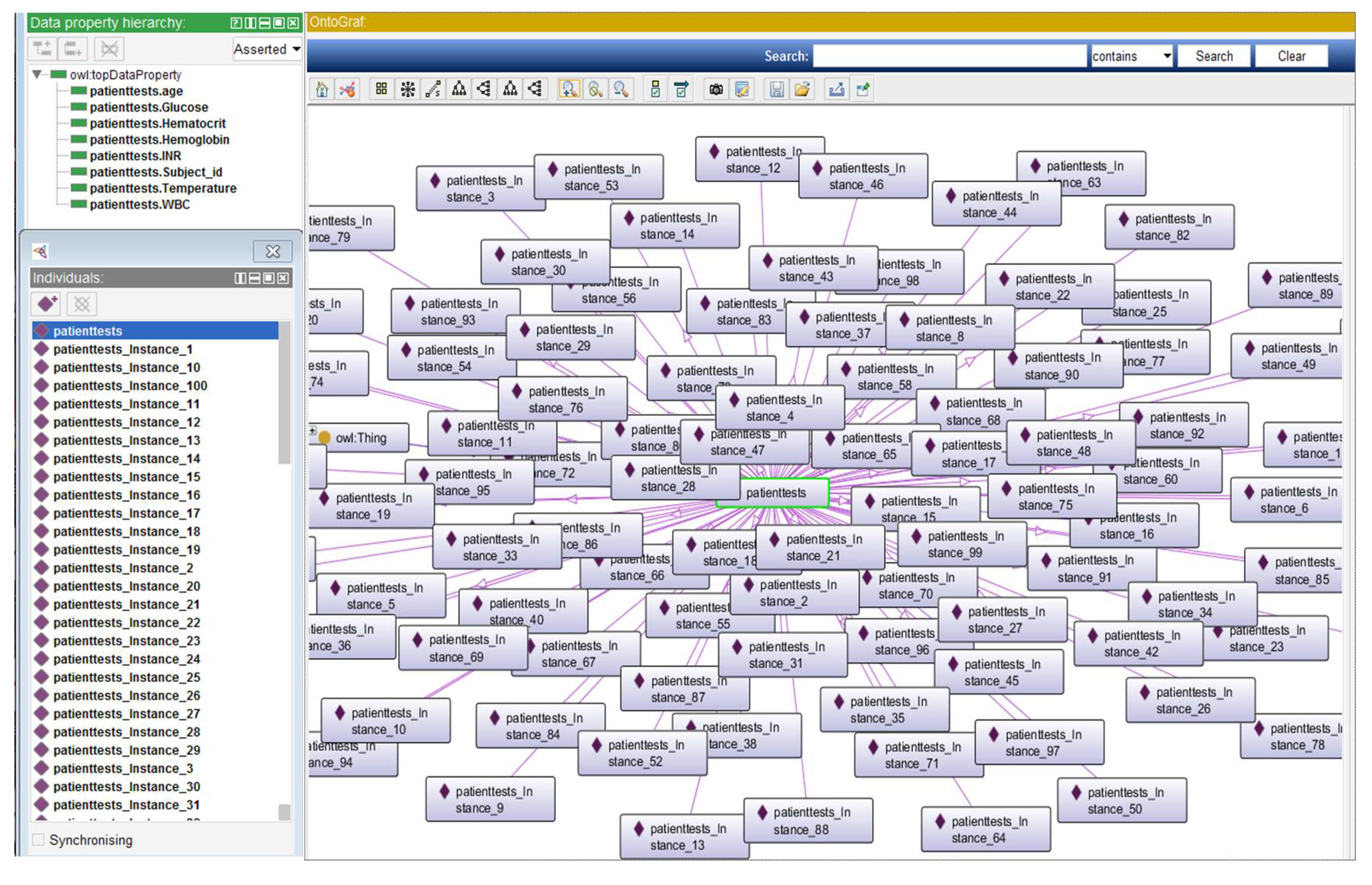
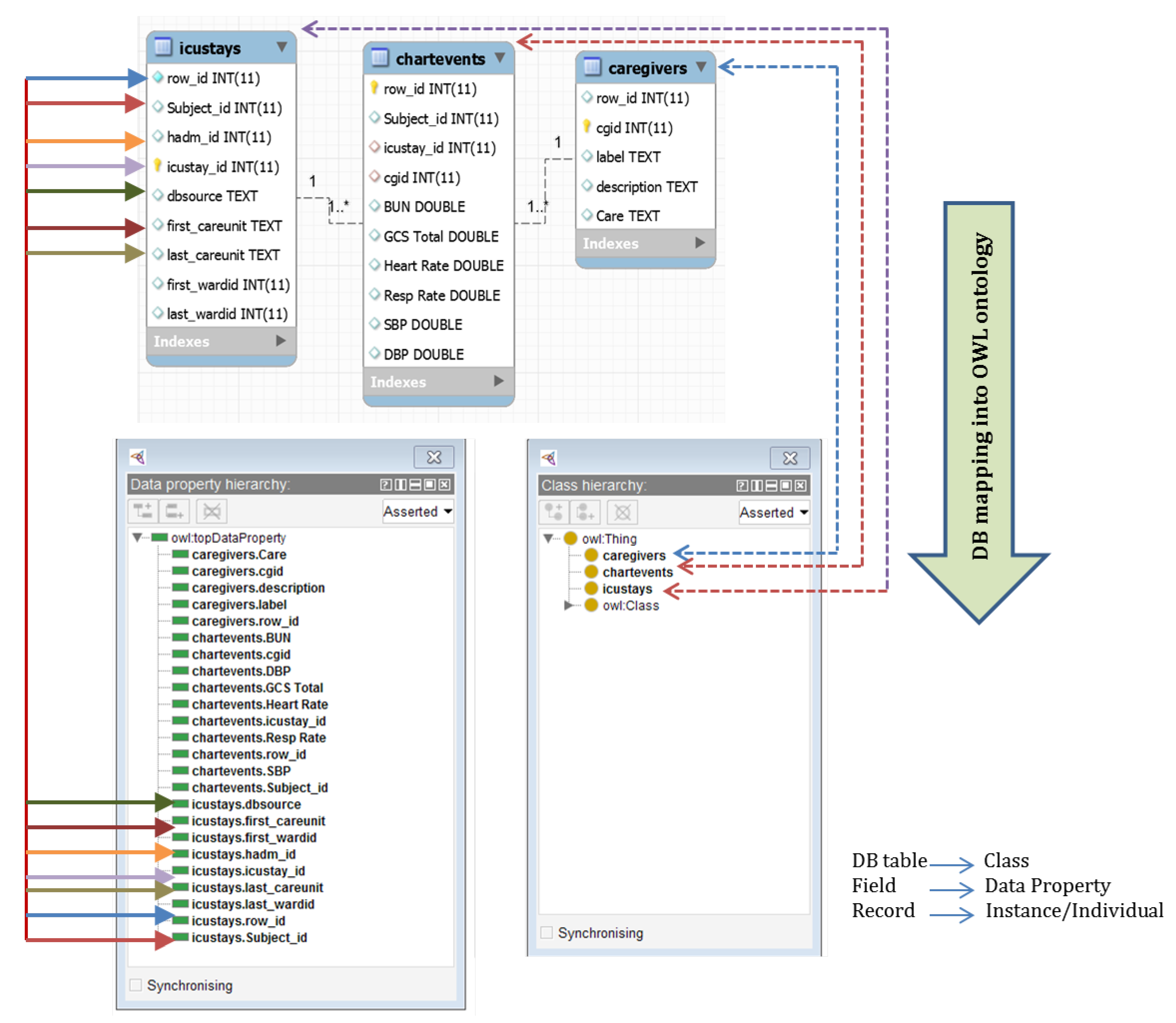
4.1. Local Ontologies Construction
- PatientTests ⊑ Thing ⊓ (∀ patienttests.Subject_id.Xsd:int),
- ⊓ (∀patienttests.age.Xsd:int),
- ⊓ (∃patienttests.Glucose.Xsd:long),
- ⊓ (∀patienttests.Hematocrit.Xsd:long),
- ⊓ (∃patienttests.Hemoglobin.Xsd:long),
- ⊓ (∃patienttests.Xsd:int),
- ⊓ (∀patienttests.Temperature.Xsd:long),
- ⊓ (∃patienttests.WBC.Xsd:long).
- caregivers ⊓ (∀caregivers.cgid.Xsd:int),
- ⊓ (∃caregivers.label.Xsd:string),
- ⊓ (∃caregivers.description.Xsd:string),
- ⊓ (∀caregivers.Care.Xsd:string).
- chartevents ⊓ (∀chartevents.cgid.Xsd:int),
- ⊓ (∀chartevents.hadm_id.Xsd:int),
- ⊓ (∀chartevents.icustay_id.Xsd:int),
- ⊓ (∀chartevents.itemid.Xsd:int),
- ⊓ (∀chartevents.subject_id.Xsd:int),
- ⊓ (∀chartevents.BUN.Xsd:double),
- ⊓ (∀chartevents.GCS Total.Xsd:double),
- ⊓ (∀chartevents.Hear Rate.Xsd:double),
- ⊓ (∀chartevents.SBP.Xsd:double),
- ⊓ (∀chartevents.DBP.Xsd:double).
- icustays ⊓ (∀icustays.hadm_id.Xsd:int),
- ⊓ (∀icustays.icustay_id.Xsd:int),
- ⊓ (∀icustays.subject_id.Xsd:int),
- ⊓ (∀icustays.outtime.Xsd:int),
- ⊓ (∀icustays.intime.Xsd:int),
- ⊓ (∀icustays.first_careunit.Xsd:int).
- ARCHETYPE ⊑ Thing (∀archetype_id.Xsd:string),
- ⊓ (∀archetype_node_id.Xsd:string),
- ⊓ (∀archetype_package_uri.Xsd:string),
- ⊓ (∀archetype_type.Xsd:string),
- ⊓ (∀parent_archetype.Xsd:string),
- ⊓ (∀Keywords.Xsd:string),
- ARCHETYPE DESCRIPTION ⊑ Thing,
- ARCHETYPE DESCRIPTION ITEM ⊑ Thing.
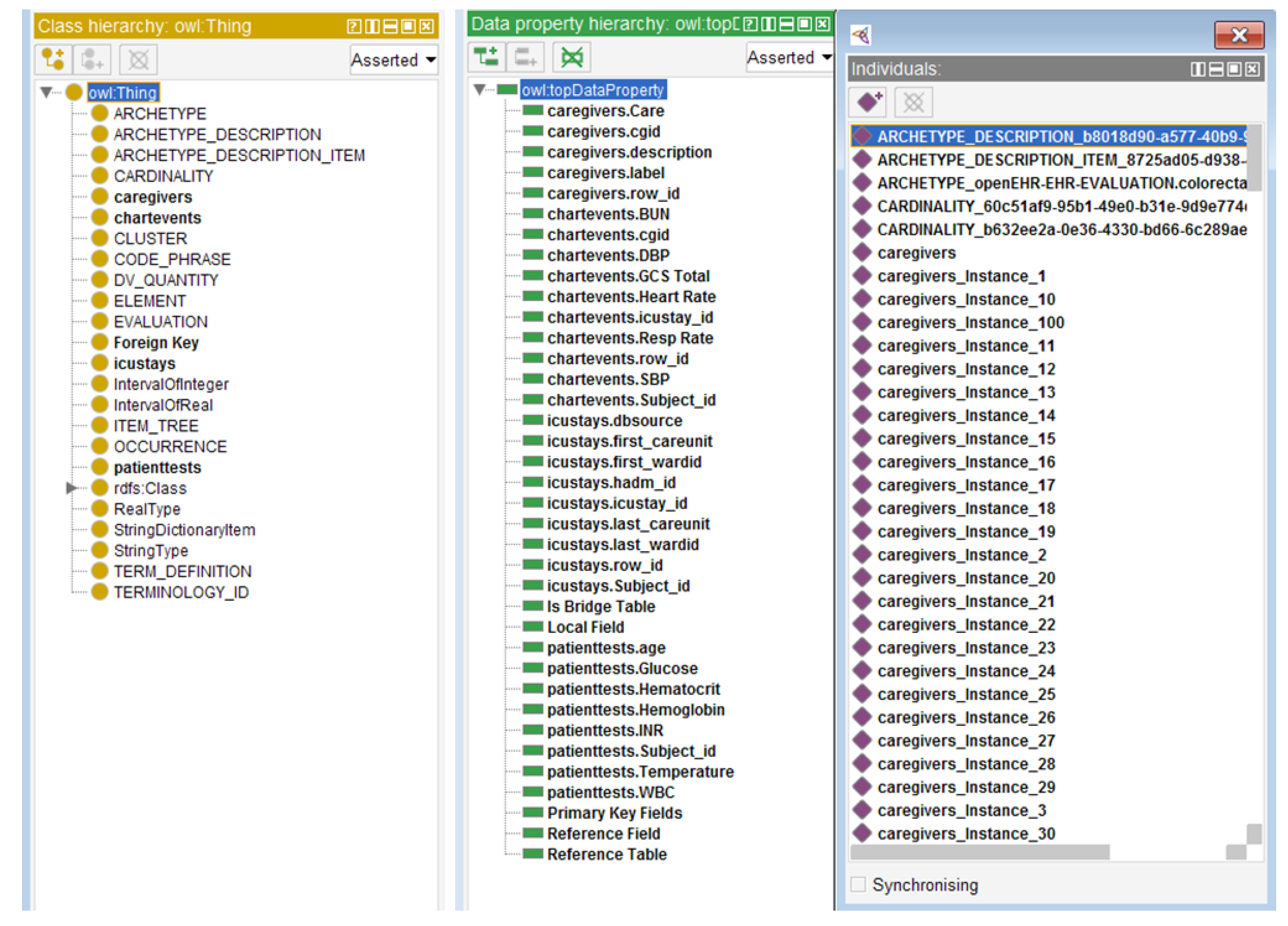
4.2. Integrated Crisp Ontology
4.3. Integrated Crisp Ontology Evaluation
4.4. Fuzzification of the Integrated Ontology
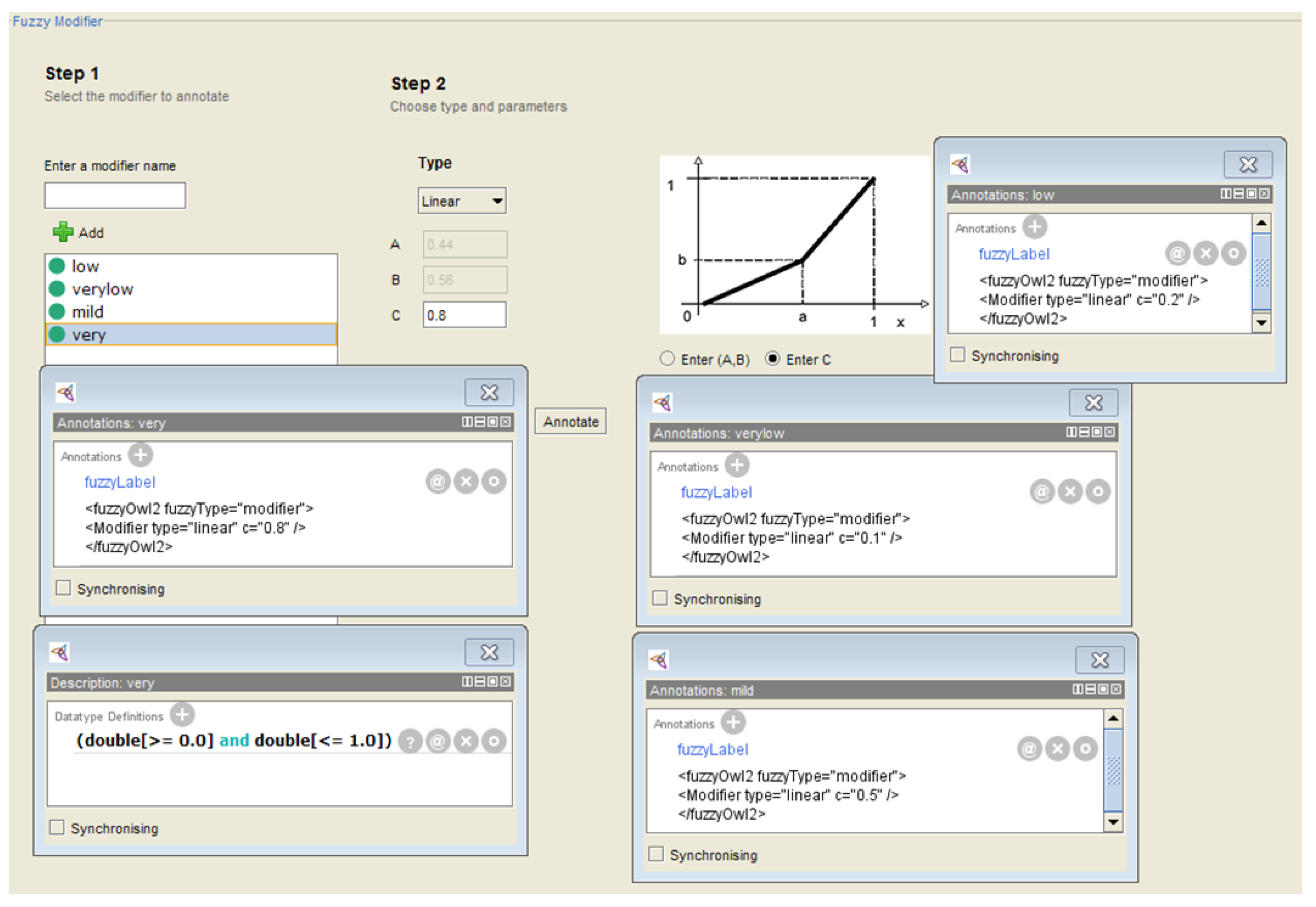
4.4.1. Definition of Fuzzy Data Types, Modifiers, and Concrete Domain
- –
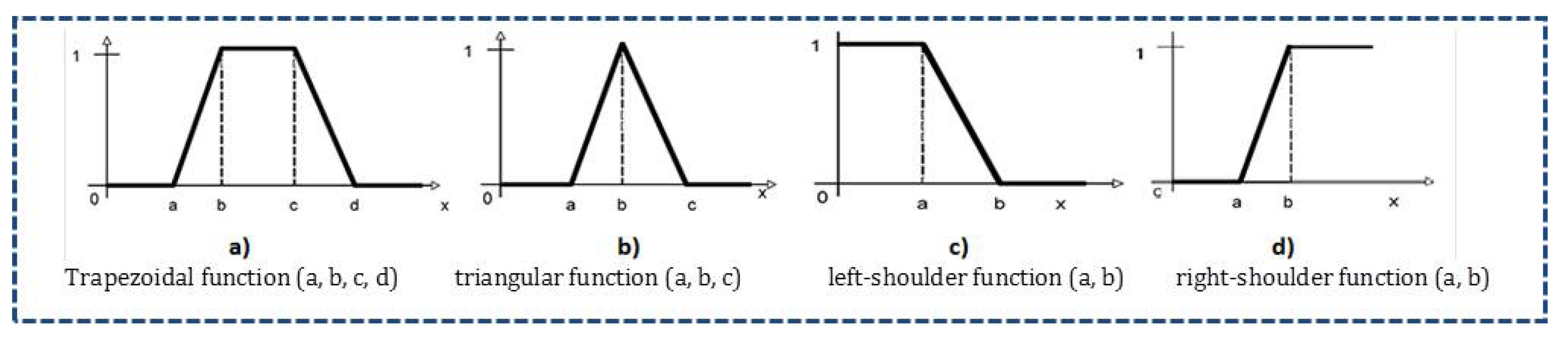
- Young (Trapezoidal (0, 10, 18, 35)), Middle-aged (Triangular (30, 40, 50)), Old (Right-shoulder (45, 90)) are linguistic variables used to represent Age (hasAge is a concrete role and indicates the Age of a patient). It has range of [0, 100]. Three fuzzy concrete roles were defined: hasyoung, hasmiddle-aged, and old.
- –
- Low.GCS (Triangular (3, 8, 10)), Moderate.GCS (Triangular (8, 12, 15)), Severe.GCS (Right-shoulder (12, 20)) are linguistic variables used to represent GCS total (hasGCStotal is a concrete role and indicates the GCStotal of a patient). It has range of [0, 25]. Three fuzzy concrete roles were defined: hasLow.GCS, hasModerate.GCS, and hasSevere.GCS.
- –
- Low.DBP (Left-shoulder (50, 70)), Normal.DBP (Trapezoidal (65, 70, 90, 110)), High.DBP (Right-shoulder (80, 110)) are used to represent DBP feature (hasDBP). It has range of [0.0, 200.0]. Three fuzzy concrete roles were defined: hasLow.DBP, hasNormal.DBP, and hasHigh.SBP.
- –
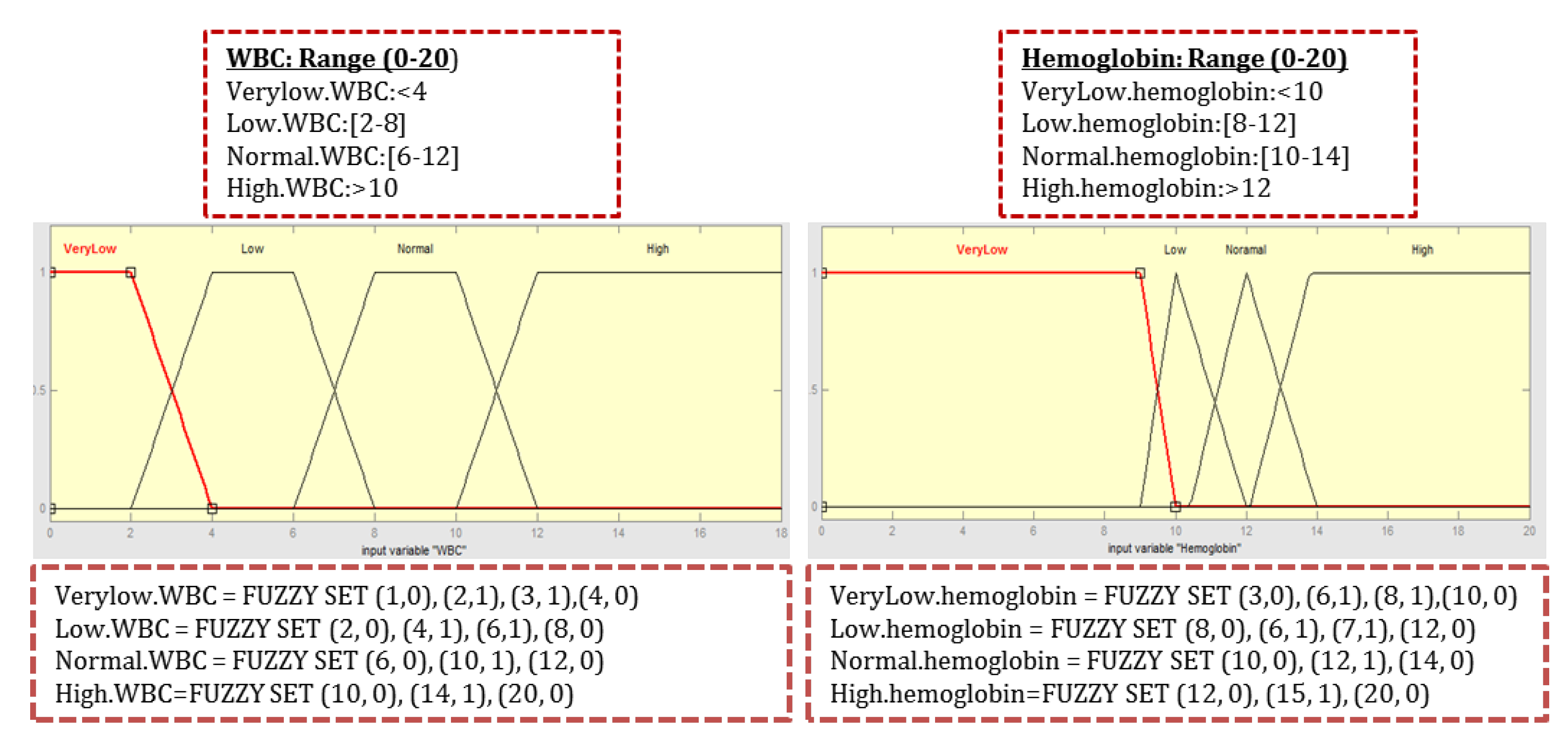
- VeryLow.hemoglobin (Left-shoulder (9, 10)), Low.hemoglobin (Triangular (8, 10, 12)), Normal.hemoglobin (Triangular (10, 13, 14)), (Right-shoulder (12, 16)) are linguistic variables used to represent Hemoglobin test variable (hasHMG). It has range of [0.0, 20.0]. Four fuzzy concrete roles were defined: hasVeryLow.hemoglobin, hasLow.hemoglobin, hasNormal.hemoglobin, and hasHigh.hemoglobin.
- –
- Low.SBP (Left-shoulder (70, 130)), Normal.SBP (Triangular (120, 140, 150)), High.SBP (Triangular (140, 160, 170)), Veryhigh.SBP (Right-shoulder (160, 190)) are used to represent SBP (hasSBP). It has range of [0.0, 240.0]. Four fuzzy concrete roles were defined: hasLow.SBP, hasNormal.SBP, hasHigh.SBP, and hasVeryhigh.SBP Fuzzy datatype annotation:<fuzzyOwl2 fuzzyType=“datatype”>,<Datatype type=“leftshoulder” a=“70” b=“130”/>,</fuzzyOwl2>.
- –
- Fuzzy concrete domain hasveryLow.Hemoglobin annotation:<fuzzyOwl2 fuzzyType=“role”><Role type=“modified” modifier=“verylow” base=“patienttests.Hemoglobin”/></fuzzyOwl2>
- –
- Fuzzy concrete domain hasLow.Hemoglobin annotation:<fuzzyOwl2 fuzzyType=“role”><Role type=“modified” modifier=“low” base=“patienttests.Hemoglobin”/></fuzzyOwl2>
- –
- Fuzzy concrete domain hasveryLow.WBC annotation:<fuzzyOwl2 fuzzyType=“role”><Role type=“modified” modifier=“verylow” base=“patienttests.WBC”/></fuzzyOwl2>
4.4.2. Integrated Fuzzy Ontology Validation
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baillieu, R.; Hoang, H.; Sripipatana, A.; Nair, S.; Lin, S.C. Impact of health information technology optimization on clinical quality performance in health centers: A national cross-sectional study. PLoS ONE 2020, 15, e0236019. [Google Scholar] [CrossRef] [PubMed]
- Jim Atherton, M. Development of the Electronic Health Record. Am. Med. Assoc. J. Ethics 2011, 13, 186–189. [Google Scholar]
- Handler, T.; Holtmeier, R.; Systems, B.; Metzger, J.; Consulting, F.; Overhage, M. HIMSS Electronic Health Record Definitional Model Electronic Health Record HIMSS Definitional Model. Health Inf. Manag. Syst. Soc. 2003, 2003, 1–8. [Google Scholar]
- Middleton, B.; Bloomrosen, M.; Dente, M.A.; Hashmat, B.; Koppel, R.; Overhage, J.M.; Payne, T.H.; Rosenbloom, S.T.; Weaver, C.; Zhang, J. Enhancing patient safety and quality of care by improving the usability of electronic health record systems: Recommendations from AMIA. J. Am. Med. Inform. Assoc. 2013, 20, e2–e8. [Google Scholar] [CrossRef]
- Olaronke, I.; Oluwaseun, O. Big Data in Healthcare: Prospects, Challenges and Resolutions. In Proceedings of the 2016 Future Technologies Conference (FTC), San Francisco, CA, USA, 6–7 December 2016; pp. 1152–1157. [Google Scholar]
- Groves, P.; Kayyali, B.; Knott, D.; Van Kuiken, S. Evaluation of the use and impact of the European Community Health Indicators ECHI by Member States Final report. Proces. Leng. Nat. 2013, 1, 168. [Google Scholar]
- Begoyan, A. An Overview of Interoperability Standards for Electronic Health Records; Society for Design and Process Science: Dallas, TX, USA, 2007. [Google Scholar]
- Bhartiya, S.; Mehrotra, D. Challenges and recommendations to healthcare data exchange in an interoperable environment. Electron. J. Health Inform. 2014, 8, 16. [Google Scholar]
- Framework Interoperability. European Interoperability Framework for Pan-European eGovernment Services; Publications Office of the European Union: Luxembourg, 2004. [Google Scholar]
- Adel, E.; El-Sappagh, S.; Barakat, S.; Elmogy, M. Distributed electronic health record based on semantic interoperability using fuzzy ontology: A survey. Int. J. Comput. Appl. 2018, 40, 223–241. [Google Scholar] [CrossRef]
- DICOM. Digital Imaging and Communications in Medicine. Available online: https://www.dicomstandard.org/ (accessed on 1 March 2021).
- ISO13606community. Available online: http://www.en13606.org/ (accessed on 3 August 2020).
- OpenEHR. Clinical Knowledge Manager (CKM). Available online: https://openehr.org/ckm/ (accessed on 3 April 2020).
- EuroRec. Available online: https://www.eurorec.org/ (accessed on 1 March 2021).
- Epsos. Available online: http://www.epsos.eu/ (accessed on 1 March 2021).
- Lewis, G.A.; Morris, E.; Simanta, S.; Wrage, L. Why Standards Are Not Enough to Guarantee End-to-End Interoperability. In Proceedings of the Seventh International Conference on Composition-Based Software Systems (ICCBSS 2008), Madrid, Spain, 25–29 February 2008; pp. 164–173. [Google Scholar]
- Blobel, B. Interoperable EHR systems—Challenges, standards and solutions. Eur. J. Biomed. Inform. 2018, 14, 10–19. [Google Scholar] [CrossRef]
- Martínez-Villaseñor, M.L.; Miralles-Pechuan, L.; González-Mendoza, M. Interoperability in Electronic Health Records through the Mediation of Ubiquitous User Model. In Proceedings of the International Conference on Ubiquitous Computing and Ambient Intelligence, Philadelphia, PA, USA, 7–10 November 2016; Springer: Cham, Switzerland, 2016; pp. 191–200. [Google Scholar]
- Images, G. Standardized Demographic Data Improve Patient Matching in Electronic Health Records; The Pew Charitable Trusts: Philadelphia, PA, USA, 2019. [Google Scholar]
- Adenuga, O.A.; Kekwaletswe, R.M.; Coleman, A. eHealth integration and interoperability issues: Towards a solution through enterprise architecture. Health Inf. Sci. Syst. 2015, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Blobel, B.; Kalra, D.; Koehn, M.; Lunn, K.; Pharow, P.; Ruotsalainen, P.; Schulz, S.; Smith, B. The role of ontologies for sustainable, semantically interoperable and trustworthy EHR solutions. Stud. Health Technol. Inform. 2009, 150, 953–957. [Google Scholar]
- Ren-chu, G.; Ding, D. A Framework of Information Service Platform in E-Government. J. Electron. Sci. Technol. 2004, 2, 152–155. [Google Scholar]
- Legaz-García, M.D.C.; Martínez-Costa, C.; Menárguez-Tortosa, M.; Fernández-Breis, J.T. A semantic web based framework for the interoperability and exploitation of clinical models and EHR data. Knowl. Based Syst. 2016, 105, 175–189. [Google Scholar] [CrossRef]
- Gruber, B.T. What Is an Ontology? Springer: Berlin, Germany, 2009; pp. 1–17. [Google Scholar]
- El-Sappagh, S.; Elmogy, M. A fuzzy ontology modeling for case base knowledge in diabetes mellitus domain. Eng. Sci. Technol. Int. J. 2017, 20, 1025–1040. [Google Scholar] [CrossRef]
- Bateman, J.A. The theoretical status of ontologies in natural language processing. arXiv 1997, arXiv:cmp-lg/9704010. [Google Scholar]
- Dolia, P.M. Integrating ontologies into multi-agent systems engineering (MaSE) for university teaching environment. J. Emerg. Technol. Web Intell. 2010, 2, 42–47. [Google Scholar] [CrossRef] [Green Version]
- Jasper, R.; Uschold, M. A Framework for Understanding and Classifying Ontology Applications. In Proceedings of the 12th International Workshop on Knowledge Acquisition, Modelling, and Management KAW, Banff, AB, Canada, 16–22 October 1999; Volume 99, pp. 16–21. [Google Scholar]
- Ortega, F.B. Managing Vagueness in Ontologies. Ph.D. Thesis, Universidad de Granada, Granada, Spain, 2008. [Google Scholar]
- Zadeh, L.A. From Search Engines to Question-Answering Systems the Need for New Tools. In Proceedings of the 12th IEEE International Conference on Fuzzy Systems, St. Louis, MO, USA, 25–28 May 2003; Volume 2, pp. 1107–1109. [Google Scholar]
- Djulbegovic, B.; Hozo, I.; Greenland, S. Uncertainty in clinical medicine. In Philosophy of Medicine; Elsevier: Amsterdam, The Netherlands, 2011; pp. 299–356. [Google Scholar]
- Bobillo, F.; Straccia, U. An OWL ontology for fuzzy OWL 2. In International Symposium on Methodologies for Intelligent Systems; Springer: Berlin/Heidelberg, Germany, 2009; pp. 151–160. [Google Scholar]
- Alexopoulos, P.; Wallace, M.; Kafentzis, K.; Askounis, D. Utilizing Imprecise Knowledge in Ontology-based CBR Systems by Means of Fuzzy Algebra. Int. J. Fuzzy Syst. 2010, 12, 1–13. [Google Scholar]
- Adel, E.; El-Sappagh, S.; Elmogy, M.; Barakat, S.; Kwak, K.S. A fuzzy ontological infrastructure for semantic interoperability in distributed electronic health record. Intell. Autom. Soft Comput. 2020, 26, 237–251. [Google Scholar] [CrossRef]
- Pan, J.Z.; Staab, S.; Aßmann, U.; Ebert, J.; Zhao, Y. Ontology-Driven Software Development; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Yang, H.; Li, W. An Ontology-Based Approach for Data Integration in Regionally Interoperable Healthcare Systems. In Proceedings of the 11th International Conference on Informatics and Semiotics in Organisations (ICISO 2009), Beijing, China, 11–12 April 2009; pp. 93–96. [Google Scholar]
- Kiourtis, A.; Mavrogiorgou, A.; Kyriazis, D. Aggregating Heterogeneous Health Data through An Ontological Common Health Language. In Proceedings of the 2017 10th International Conference on Developments in eSystems Engineering (DeSE), Paris, France, 14–16 June 2017; pp. 175–181. [Google Scholar]
- El Hajjamy, O.; Alaoui, L.; Bahaj, M. Integration of Heterogeneous Classical Data Sources in An Ontological Database. In International Conference on Big Data, Cloud and Applications; Springer: Cham, Switzerland, 2018; pp. 417–432. [Google Scholar]
- da Costa, C.A.; Wichman, M.H.; da Rosa Righi, R.; Yamin, A.C. Ontology-Based Model for Interoperability between Openehr and hl7 Health Applications. In Proceedings of the International Conference in Health Informatics and Medical Systems (HIMS19), Las Vegas, NV, USA, 29 July–1 August 2019. [Google Scholar]
- Roehrs, A.; da Costa, C.A.; da Rosa Righi, R.; Rigo, S.J.; Wichman, M.H. Toward a model for personal health record interoperability. IEEE J. Biomed. Health Inform. 2018, 23, 867–873. [Google Scholar] [CrossRef]
- Duncan, W.D.; Thyvalikakath, T.; Haendel, M.; Torniai, C.; Hernandez, P.; Song, M.; Acharya, A.; Caplan, D.J.; Schleyer, T.; Ruttenberg, A. Structuring, reuse and analysis of electronic dental data using the Oral Health and Disease Ontology. J. Biomed. Semant. 2020, 11, 1–19. [Google Scholar] [CrossRef]
- Calegari, S.; Sanchez, E. A Fuzzy Ontology-Approach to improve Semantic Information Retrieval. URSW 2007, 327, 1–6. [Google Scholar]
- Parry, D. A fuzzy ontology for medical document retrieval. ACM Int. Conf. Proc. Ser. 2004, 54, 121–126. [Google Scholar]
- Hudelot, C.; Atif, J.; Bloch, I. Fuzzy spatial relation ontology for image interpretation. Fuzzy Sets Syst. 2008, 159, 1929–1951. [Google Scholar] [CrossRef]
- Rodríguez, N.D.; Cuéllar, M.P.; Lilius, J.; Calvo-Flores, M.D. A fuzzy ontology for semantic modelling and recognition of human behaviour. Knowl. Based Syst. 2014, 66, 46–60. [Google Scholar] [CrossRef]
- Mylonas, P.; Athanasiadis, T.; Wallace, M.; Avrithis, Y.; Kollias, S. Semantic representation of multimedia content: Knowledge representation and semantic indexing. Multimed. Tools Appl. 2008, 39, 293–327. [Google Scholar] [CrossRef]
- Ali, F.; Islam, S.R.; Kwak, D.; Khan, P.; Ullah, N.; Yoo, S.j.; Kwak, K.S. Type-2 fuzzy ontology–aided recommendation systems for IoT–based healthcare. Comput. Commun. 2018, 119, 138–155. [Google Scholar] [CrossRef]
- Di Noia, T.; Mongiello, M.; Nocera, F.; Straccia, U. A fuzzy ontology-based approach for tool-supported decision making in architectural design. Knowl. Inf. Syst. 2019, 58, 83–112. [Google Scholar] [CrossRef]
- Ali, F.; Kwak, D.; Khan, P.; Islam, S.R.; Kim, K.H.; Kwak, K.S. Fuzzy ontology-based sentiment analysis of transportation and city feature reviews for safe traveling. Transp. Res. Part Emerg. Technol. 2017, 77, 33–48. [Google Scholar] [CrossRef] [Green Version]
- Viangteeravat, T.; Anyanwu, M.N.; Nagisetty, V.R.; Kuscu, E.; Sakauye, M.E.; Wu, D. Clinical data integration of distributed data sources using Health Level Seven (HL7) v3-RIM mapping. J. Clin. Bioinform. 2011, 1, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Myłka, A.; Myłka, A.; Kryza, B.; Kitowski, J. Integration of heterogeneous data sources in an ontological knowledge base. Comput. Inform. 2012, 31, 189–223. [Google Scholar]
- Gruber, T.R. Toward principles for the design of ontologies used for knowledge sharing? Int. J. Hum. Comput. Stud. 1995, 43, 907–928. [Google Scholar] [CrossRef]
- Politi, M.C.; Han, P.K.; Col, N.F. Communicating the uncertainty of harms and benefits of medical interventions. Med. Decis. Mak. 2007, 27, 681–695. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.H. Fuzzy Ontology Map—A fuzzy Extension of the Hard-Constraint Ontology. In Proceedings of the 2006 IEEE/WIC/ACM International Conference on Web Intelligence (WI 2006 Main Conference Proceedings) (WI’06), Hong Kong, China, 18–22 December 2006; pp. 506–509. [Google Scholar]
- Zadeh, L.A. From computing with numbers to computing with words. From manipulation of measurements to manipulation of perceptions. IEEE Trans. Circuits Syst. Fundam. Theory Appl. 1999, 46, 105–119. [Google Scholar] [CrossRef]
- Cox, E. The Fuzzy Systems Handbook: A Practitioner’s Guide to Building, Using, and Maintaining Fuzzy Systems; Academic Press Professional, Inc.: Rochester, NY, USA, 1994. [Google Scholar]
- Harman, G. Logic and reasoning. In Foundations: Logic, Language, and Mathematics; Springer: Cham, Switzerland, 1984; pp. 107–127. [Google Scholar]
- Baader, F.; Calvanese, D.; McGuinness, D.L.; Nardi, D.; Patel-Schneider, P.F. The Description Logic Handbook: Theory, Implementation and Applications. Kybernetes 2010, 32, 624. [Google Scholar]
- Cohen, W.W.; Laboratories, T.B.; Hill, M.; Borgida, A. Computing Least Common Subsumers in Description Logics. AAAI 1992, 1992, 754–760. [Google Scholar]
- Barwise, J. (Ed.) An Introduction to First-Order Logic. In Handbook of Mathematical Logic; Elsevier: Amsterdam, The Netherlands, 1977; Volume 90, pp. 5–46. [Google Scholar]
- Graves, A.; Mohamed, A.; Hinton, G. Speech Recognition with Deep Recurrent Neural Networks. In Proceedings of the 2013 IEEE International Conference on Acoustics, Speech and Signal Processing, Vancouver, BC, Canada, 26–31 May 2013; pp. 6645–6649. [Google Scholar]
- Hirschberg, J.; Manning, C.D. Advances in natural language processing. Science 2015, 349, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Mnih, V.; Kavukcuoglu, K.; Silver, D.; Graves, A.; Antonoglou, I.; Wierstra, D.; Riedmiller, M. Playing Atari with Deep Reinforcement Learning. arXiv 2013, arXiv:1312.5602. [Google Scholar]
- Baader, F.; Lutz, C. Description logic. In Studies in Logic and Practical Reasoning; Elsevier: Amsterdam, The Netherlands, 2007; Volume 3, pp. 757–819. [Google Scholar]
- Pellet. Available online: http://pellet.owldl.com/ (accessed on 17 April 2021).
- HermiT. HermiT OWL Reasoner. Available online: http://www.hermit-reasoner.com/ (accessed on 11 April 2021).
- KAON2. KAON2 -Ontology Management for the Semantic Web. Available online: http://kaon2.semanticweb.org (accessed on 3 April 2021).
- Manchester. FaCT++ Reasoner. Available online: http://owl.cs.manchester.ac.uk/tools/fact/ (accessed on 9 April 2021).
- RacerPro. Available online: https://franz.com/agraph/racer/ (accessed on 4 April 2021).
- Bobillo, F.; Straccia, U. Fuzzy ontology representation using OWL 2. Int. J. Approx. Reason. 2011, 52, 1073–1094. [Google Scholar] [CrossRef] [Green Version]
- Horrocks, I.; Kutz, O.; Sattler, U. The Even More Irresistible SROIQ. Kr 2006, 6, 57–67. [Google Scholar]
- Lutz, C. Description logics with concrete domains—A survey. J. IGPL 2003, 5, 535–567. [Google Scholar]
- Bobillo, F.; Straccia, U. The fuzzy ontology reasoner fuzzyDL. Knowl. Based Syst. 2016, 95, 12–34. [Google Scholar] [CrossRef]
- Bobillo, F.; Delgado, M.; Gómez-Romero, J. DeLorean: A reasoner for fuzzy OWL 2. Expert Syst. Appl. 2012, 39, 258–272. [Google Scholar] [CrossRef] [Green Version]
- LinkEHR. Available online: https://linkehr.veratech.es/ (accessed on 4 April 2021).
- Maldonado, J.A.; Moner, D.; Boscá, D.; Fernández-Breis, J.T.; Angulo, C.; Robles, M. LinkEHR-Ed: A multi-reference model archetype editor based on formal semantics. Int. J. Med. Inform. 2009, 78, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Dugas, M.; Neuhaus, P.; Meidt, A.; Doods, J.; Storck, M.; Bruland, P.; Varghese, J. Portal of medical data models: Information infrastructure for medical research and healthcare. Database 2016, 2016, bav121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noy, N.F.; Musen, M. PROMPT: Algorithm and Tool for Automated Ontology Merging and Alignment. In Proceedings of the Seventeenth National Conference on Artificial Intelligence (AAAI-2000), Austin, TX, USA, 30 July–3 August 2000. [Google Scholar]
- Severo, B.; Trojahn, C.; Vieira, R. VOAR: A Visual and Integrated Ontology Alignment Environment; European Language Resources Association: Reykjavik, Iceland, 2014; pp. 3671–3677. [Google Scholar]
- Calvanese, D.; De Giacomo, G.; Lenzerini, M. Ontology of Integration and Integration of Ontologies. Descr. Log. 2001, 49, 30. [Google Scholar]
- Adel, E.; Barakat, S.; Elmogy, M. Distributed Electronic Health Records Semantic Interoperability Based on a Fuzzy Ontology Architecture. In Proceedings of the 2019 14th International Conference on Computer Engineering and Systems (ICCES), Cairo, Egypt, 17–18 December 2019; pp. 362–367. [Google Scholar]
- Umberto, D.B.; Straccia, F.B. FuzzyOWL2. Available online: https://protegewiki.stanford.edu/wiki/FuzzyOWL2/ (accessed on 17 January 2021).
- DuCharme, B. Learning SPARQL: Querying and Updating with SPARQL 1.1; O’Reilly Media, Inc.: Sebastopol, CA, USA, 2013. [Google Scholar]
- O’Connor, M.J.; Das, A.K. SQWRL: A Query Language for OWL. In Proceedings of the 6th International Workshop on OWL: Experiences and Directions (OWLED 2009), Chantilly, VA, USA, 23–24 October 2009; Volume 529, pp. 42–44. [Google Scholar]
- Tommila, T.; Hirvonen, J.; Pakonen, A. Fuzzy Ontologies for Retrieval of Industrial Knowledge—A Case Study; VTT Technical Research Centre of Finland: Espoo, Finland, 2010. [Google Scholar]
- Alexopoulos, P.; Wallace, M.; Kafentzis, K.; Askounis, D. IKARUS-Onto: A methodology to develop fuzzy ontologies from crisp ones. Knowl. Inf. Syst. 2012, 32, 667–695. [Google Scholar] [CrossRef]
- Yardimci, A. Soft computing in medicine. Appl. Soft Comput. 2009, 9, 1029–1043. [Google Scholar] [CrossRef]
- Singh, A.; Juneja, D.; Sharma, A. A fuzzy integrated ontology model to manage uncertainty in semantic web: The fiom. Int. J. Comput. Sci. Eng. 2011, 3, 1057–1062. [Google Scholar]
- Adel, E.; El-Sappagh, S.; Barakat, S.; Elmogy, M. A unified fuzzy ontology for distributed electronic health record semantic interoperability. In U-Healthcare Monitoring Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 353–395. [Google Scholar]
- Häyrinen, K.; Saranto, K.; Nykänen, P. Definition, structure, content, use and impacts of electronic health records: A review of the research literature. Int. J. Med. Inform. 2008, 77, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.Q.; Denny, J.C. Extracting research-quality phenotypes from electronic health records to support precision medicine. Genome Med. 2015, 7, 1–14. [Google Scholar] [CrossRef] [Green Version]
- The Health Information Technology Policy Committee. Report to Congress: Challenges and Barriers to Interoperability; Technical Report for United States Government Publishing Office: Washington, DC, USA, December 2015.
- Virtanen, M.; Ustun, B.; Rodrigues, J.M.; Surjan, G.; Rector, A.; Stroetmann, V.N.; Stroetmann, K.A.; Lewalle, P.; Zanstra, P.E.; Kalra, D. Semantic Interoperability for Better Health and Safer Healthcare: Deployment and Research Roadmap for Europe; Publications Office of the European Union: Luxembourg, 2009; Volume 240, pp. 508–510. [Google Scholar]
- CMS. Centers for Medicare and Medicaid Services. Available online: https://www.cms.gov/ (accessed on 17 January 2021).
- Garde, S.; Knaup, P.; Hovenga, E.J.; Heard, S. Towards semantic interoperability for electronic health records. Methods Inf. Med. 2007, 46, 332–343. [Google Scholar]
- Berners-Lee, T.; Hendler, J.; Lassila, O. The Semantic Web. Sci. Am. 2001, 284, 34–43. [Google Scholar] [CrossRef]
- Sanchez, D.; Tettamanzi, A.G. Fuzzy quantification in fuzzy description logics. In Capturing Intelligence; Elsevier: Amsterdam, The Netherlands, 2006; Volume 1, pp. 135–159. [Google Scholar]
- Berges, I.; Bermúdez, J.; Illarramendi, A. Toward semantic interoperability of electronic health records. IEEE Trans. Inf. Technol. Biomed. 2011, 16, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, M.; Yu, F.; Andrus, C.H.; Bradner, S.; Rawn, J. A general framework for interoperability with applications to healthcare. Health Policy Technol. 2014, 3, 3–12. [Google Scholar] [CrossRef]
- El Azami, I.; Malki, M.O.C.; Tahon, C. Integrating hospital information systems in healthcare institutions: A mediation architecture. J. Med. Syst. 2012, 36, 3123–3134. [Google Scholar] [CrossRef]
- Shi, Y.; Liu, X.; Xu, Y.; Ji, Z. Semantic-Based Data Integration Model Applied to Heterogeneous Medical Information System. In Proceedings of the 2010 The 2nd International Conference on Computer and Automation Engineering (ICCAE), Singapore, 26–28 February 2010; Volume 2, pp. 624–628. [Google Scholar]
- Abhyankar, S.; Demner-Fushman, D.; Callaghan, F.M.; McDonald, C.J. Combining structured and unstructured data to identify a cohort of ICU patients who received dialysis. J. Am. Med. Inform. Assoc. 2014, 21, 801–807. [Google Scholar] [CrossRef] [Green Version]
- Solares, J.R.A.; Raimondi, F.E.D.; Zhu, Y.; Rahimian, F.; Canoy, D.; Tran, J.; Gomes, A.C.P.; Payberah, A.H.; Zottoli, M.; Nazarzadeh, M.; et al. Deep learning for electronic health records: A comparative review of multiple deep neural architectures. J. Biomed. Inform. 2020, 101, 103337. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Column Name | Datatype | Description |
|---|---|---|
| Subject_id | Integer | Defines a unique identifier for the patient. |
| Age (years) | Double | Defines calculated value for the age of the patient. It is calculated from the difference between DOD “date of death” and DOB “date of birth” from the PATIENTS table. |
| Glucose | Double | It measures Glucose in the blood; its values were identified by the following ITEMIDs: (50809, 50931, 51529). |
| Hematocrit | Double | It measures hematocrit in the blood; its ITEMSIDs are (51348, 51369, 51422, 51445, 50810, 51115, 51221, 51480). |
| Hemoglobin | Double | This field measures hemoglobin percentage in the blood. Its values were identified by the following ITEMIDs: (50814, 50852, 50855, 51222, 51223, 51224, 51225, 51226, 51227, 51285). |
| INR | Double | Its ITEMID is (51237). |
| Temperature | Double | It contains the temperature of the body. Its ITEMID is (50825). |
| Temperature | Double | Its ITEMID is (51237). |
| WBC | Double | It determines the number of white blood cells in the blood. Its values were identified by the following ITEMIDs: (51363, 51384, 51439, 51458, 51128, 51300, 51301, 51516, 51517, 51518). |
| Question | SPARQL Query | Result |
|---|---|---|
| Q1: Find the results of the main tests for a specific patient? | SELECT ?age ?Glucose ?HCT ?HMG ?WBC ?TMP ?SBP ?DBP ?GCS WHERE { ?person pats:patienttests.age ?age; pats:patienttests.Glucose ?Glucose; pats:patienttests.Hematocrit ?HCT; pats:patienttests.Hemoglobin ?HMG; pats:patienttests.WBC ?WBC; pats:patienttests.Temperature ?TMP; pats:chartevents.SBP ?SBP; pats:chartevents.DBP ?DBP; pats:chartevents.GCS Total ?GCS; pats:patienttests.Subject_id 3888. } | 1 result |
| Q2: Find the patients with SBD ≥ 140 or DBP ≥ 90? | SELECT ?subjectID WHERE { ?person pats:chartevents.Subject_id ?subjectID; pats:chartevents.SBP ?SBP; pats:chartevents.DBP ?DBP. FILTER ((?SBP ≥ 140) (?DBP ≥ 100))} | 2 results |
| Q3: Find the patients with hemoglobin ≤ 10? | SELECT ?subjectID WHERE { ?person pats:patienttests.Subject_id ?subjectID; pats:patienttests.Hemoglobin ?HMG. FILTER ((?HMG ≤ 10))} | 71 results |
| Q4: Count the young patients who entered ICU? | SELECT ?subjectID COUNT(?subjectID) AS ?TotalYoung WHERE { ?person pats:patienttests.Subject_id ?subjectID; pats:patienttests.age?age. FILTER ((?age ≤ 30))} | 1 result |
| Q5: Query to get all data for patients older than 70 years? | SELECT ?Glucose ?HCT ?HMG ?WBC ?TMP ?INR ?SBP ?DBP ?GCS ?BUN WHERE { ?person pats:patienttests.age ?age; pats:patienttests.Glucose ?Glucose; pats:patienttests.Hematocrit ?HCT; pats:patienttests.Hemoglobin ?HMG; pats:patienttests.WBC ?WBC; pats:patienttests.Temperature ?TMP; pats: patienttests.INR ?INR; pats:chartevents.SBP ?SBP; pats:chartevents.DBP ?DBP; pats: chartevents.BUN ?BUN; pats:chartevents.GCS Total ?GCS. FILTER ((?age > 70)) } | 50 results |
| Fuzzy Feature | MF Shape | MF Range | MF Fuzzy Parameters |
|---|---|---|---|
| Age (years) | Young | [≤30] | Trapezoidal (0, 10, 18, 35) |
| Range (0–100) | Middle-aged | [30–50] | Triangular (30, 40, 50) |
| Old | [≥45] | Right-shoulder (45, 90) | |
| Glucose | Low.glucose | [≤120] | Left-shoulder (50, 120) |
| (mg/dL) | Medium.glucose | [100–220] | Trapezoidal (100, 120, 200, 220) |
| Range (0–350) | High.glucose | [≥220] | Right-shoulder (200, 250) |
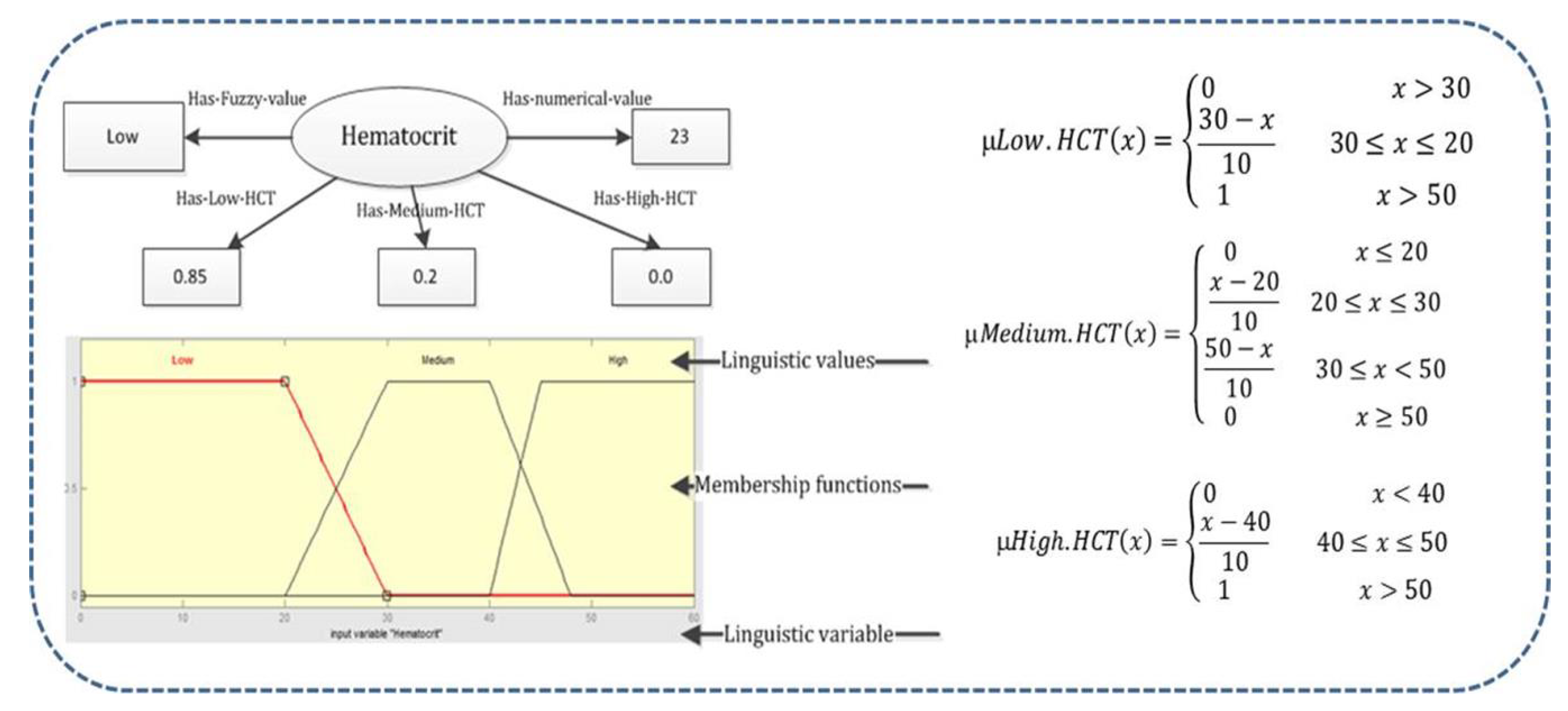
| Hematocrit | Low.HCT | [≤30] | Left-shoulder (20, 30) |
| (%) | Medium.HCT | [20–45] | Trapezoidal (20, 35, 40, 45) |
| Range (15–60) | High.HCT | [≥40] | Right-shoulder (40, 50) |
| Hemoglobin | VeryLow.hemoglobin | [≤10] | Left-shoulder (9, 10) |
| (mmolL) | Low.hemoglobin | [8–12] | Triangular (8, 10, 12) |
| Range (0–20) | Normal.hemoglobin | [10–14] | Triangular (10, 13, 14) |
| High.hemoglobin | [≥12] | Right-shoulder (12, 16) | |
| INR | Low.INR | [≤15] | Left-shoulder (0, 15) |
| Range (0–50) | Medium.INR | [13–27] | Trapezoidal (13,15, 25, 27) |
| High.INR | [≥25] | Right-shoulder (25, 45) | |
| Temperature | Low.Tmp | [≤36] | Left-shoulder (34, 36) |
| (°C) | Medium.Tmp | [35–37] | Triangular (35, 36, 37) |
| Range (34–42) | High.Tmp | [36–38] | Triangular (36, 37, 38) |
| veryHigh.TMP | [≥37] | Right-shoulder (37, 39) | |
| WBC | Verylow.WBC | [≤4] | Left-shoulder (2, 4) |
| (×103 cells/μL) | Low.WBC | [2–8] | Trapezoidal (2, 4, 6, 8) |
| Range (0–20) | Normal.WBC | [6–12] | Trapezoidal (6, 8, 10, 12) |
| High.WBC | [≥10] | Right-shoulder (10, 16) | |
| BUN | Low.BUN | [≤4] | Left-shoulder (4, 10) |
| (mg/dL) | Moderate.BUN | [8–22] | Trapezoidal (4, 10, 15, 22) |
| Range (0–40) | High.BUN | [≥10] | Right-shoulder (20, 25) |
| GCS Total | Low.GCS | [3–10] | Triangular (3, 8, 10) |
| Range (0–25) | Moderate.GCS | [8–15] | Triangular (8, 12, 15) |
| Severe.GCS | [12–20] | Right-shoulder (12, 20) | |
| Heart Rate | Low.HR | [≤100] | Left-shoulder (100, 120) |
| (beats/minute) | Medium.HR | [100–180] | Triangular (100, 150, 180) |
| Range (0–500) | High.HR | [≥150] | Right-shoulder (150, 200) |
| Resp Rate | Low.RR | [0–12] | Triangular (0, 8, 10) |
| (breaths/minute) | Medium.RR | [10–25] | Triangular (8, 15, 25) |
| Range (0–80) | High.RR | [23–60] | Triangular (20, 40, 60) |
| SBP | Low.SBP | [<130] | Left-shoulder (70, 130) |
| (mmHg) | Normal.SBP | [120–150] | Triangular (120, 140, 150) |
| Range (0–240) | High.SBP | [140–170] | Triangular (140, 160, 170) |
| Veryhigh.SBP | [≥170] | Triangular (140, 160, 170) | |
| DBP | Low.DBP | [≤70] | Left-shoulder (50, 70) |
| (mmHg) | Normal.DBP | [65,110] | Trapezoidal (65, 70, 90, 110) |
| Range (0–200) | High.DBP | [≥90] | Right-shoulder (80, 110) |
| Metrics | |
|---|---|
| Axioms | 8376 |
| Logical axioms | 5232 |
| Class count | 27 |
| Object property count | 3 |
| Data property count | 58 |
| Individuals count | 451 |
| Individuals count | 451 |
| Declarative axioms | 1216 |
| Annotation axioms | 113 |
| Data property assertion axioms | 3204 |
| Datatype property axioms | 138 |
| Fuzzy data types | 43 |
| Question | FuzzyDL Query | Result |
|---|---|---|
| Q1: Extract the old age patient with high blood pressure | hasAge only (patienttests.age.value only (hasOld value veryold)) and hasSBP some (chartevents.SBP.value some (hasSBP value hasVeryhigh.SBP)) and hasDBP some (chartevents.DBP.value some (hasDBP value hasHigh.DBP)) | 5 instances |
| Q2: Extract the young patients with very low hemoglobin score? | hasAge only (patienttests.age only (hasYoung value young)) and hasHMG some (patienttests.Hemoglobin some (hasHMG value hasVerylow.hemoglobin)) | 4 instances |
| Q3: Extract the patients with low hemoglobin and very low WBC score? | hasHMG some (patienttests.Hemoglobin some (hasHMG value hasVerylow.hemoglobin)) and hasWBC some (patienttests.WBC some (hasWBC value hasVerylow.WBC)) | 34 instances |
| Q4: Query to get all number of patients older than 70 years | hasAge only (patienttests.age.value only (hasOld value veryold)) | 55 instances |
| Q5: Find all the patients with high blood pressure? | hasSBP some (chartevents.SBP.value some (hasSBP value hasveryhigh.SBP)) and hasDBP some (chartevents.DBP.value some (hasDBP value hasHigh.DBP)) | 6 results |
| Dimension | Berges et al. [98] | da Costa et al. [39] | Gaynor et al. [99] | Mylka et al. [51] | El Azami et al. [100] | Shi et al. [101] | Proposed |
|---|---|---|---|---|---|---|---|
| EHRs formats | RDB, ADL | MIMIC-III, openEHR, and HL7 | EHRs standards | RDB, XML and LDAP | Different RDBs | any DBMS | DB, Excel, CSV, XML, and openEHR ADL |
| methodology | Ontologies-mapping | Ontologies + SWRL Rules | Interoperability matrix and Flow Graph | Ontology-based | Ontology-based Mediation | Mdiation ontology | Fuzzy-ontology |
| Standard | Yes | No | Yes | No | No | No | Yes |
| Interoperability level | Full (Syntactic and Semantic) | Syntactic | Syntactic | Semantic | Syntactic | Semantic | Full |
| Handling vague and imprecise problems | Yes | No | No | No | No | No | Yes |
| Implemented/theoretical framework | Implemented | Implemented | Theoretical | Implemented | Implemented | Theoretical | Implemented |
| Year | 2011 | 2019 | 2013 | 2012 | 2012 | 2010 | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adel, E.; El-Sappagh, S.; Barakat, S.; Hu, J.-W.; Elmogy, M. An Extended Semantic Interoperability Model for Distributed Electronic Health Record Based on Fuzzy Ontology Semantics. Electronics 2021, 10, 1733. https://doi.org/10.3390/electronics10141733
Adel E, El-Sappagh S, Barakat S, Hu J-W, Elmogy M. An Extended Semantic Interoperability Model for Distributed Electronic Health Record Based on Fuzzy Ontology Semantics. Electronics. 2021; 10(14):1733. https://doi.org/10.3390/electronics10141733
Chicago/Turabian StyleAdel, Ebtsam, Shaker El-Sappagh, Sherif Barakat, Jong-Wan Hu, and Mohammed Elmogy. 2021. "An Extended Semantic Interoperability Model for Distributed Electronic Health Record Based on Fuzzy Ontology Semantics" Electronics 10, no. 14: 1733. https://doi.org/10.3390/electronics10141733
APA StyleAdel, E., El-Sappagh, S., Barakat, S., Hu, J. -W., & Elmogy, M. (2021). An Extended Semantic Interoperability Model for Distributed Electronic Health Record Based on Fuzzy Ontology Semantics. Electronics, 10(14), 1733. https://doi.org/10.3390/electronics10141733